
Abstract
The present study addresses the perspectives of Israeli family caregivers and migrant care workers on behavioral problems of persons with dementia. We thematically analyzed interviews with 21 migrant home care workers and 17 family members. Three main themes reported by both family members and migrant home care workers were identified. The first theme concerned the main challenges associated with caring for a person with dementia. The second theme concerned the management of the care recipient’s behavioral problems. The last theme concerned the relationship between family members and the migrant home care worker in the context of the care provided to a family member with dementia. Our findings stress that the different stakeholders have quite similar perspectives concerning what the most challenging behaviors associated with dementia are as well as ways to address them. Moreover, both family members and migrant home care workers recognize the role of family members as mediators and as those who ensure adequate working relations of the migrant care workers and thus, are directly responsible for protecting the mental and physical wellbeing of the worker. Policy stakeholders and clinicians responsible for this caregiving arrangement should use these insights to better prepare family members and migrant home care workers for this caregiving context and the challenges it brings.
Introduction
Behavioral problems such as aggression, agitation, sleep impairment, behavioral apathy, hallucinations, and delusions are highly prevalent in the case of persons with dementia, affecting as many as 90% of all persons with this condition, especially in the later stages of the disease (Radue et al., 2019). These behavioral challenges, which are also understood as responses to external stimuli or unmet needs within the social environment, make the care for a person with dementia particularly challenging, resulting in high levels of burden and burnout among the carers (Tan et al., 2005). In the context of migrant live-in care arrangements, this also includes the negotiation of different cultural interpretations of and approaches towards dementia (Adebayo et al., 2020). The present study addresses the perspectives of Israeli family caregivers and migrant home care workers on the behavioral problems of persons with dementia.
Migrant home care workers
Research has shown that both older persons and their family members prefer to age in place (Wiles et al., 2011). Given the changing demographics and lifestyle, which have resulted in a longer life expectancy, fewer children, more diverse family arrangements, a tendency to live within the nuclear family, and the entrance of women into the workforce, the sole reliance on informal care has become more challenging. As a result, worldwide, migrant home care workers represent a relatively economic and readily available care arrangement, which supplements the informal care provided by family members (Cangiano, 2014; Eckenwiler, 2011).
The Israeli society is considered a society in transition between traditional values of family care to modern individualistic values (AboJabel & Ayalon, 2023; Lavee & Katz, 2003). As such, migrant home care is a common practice in Israel as it allows older persons to age at home, and supposedly releases family members from the provision of personal care. This migrant in the family model is common in many Mediterranean countries (Michel & Peng, 2012; Modanesi, 2018) as well as in Asian countries (Chou et al., 2015; Shah & Lerche, 2020), Europe (Hoens & Smetcoren, 2023), and North America (Bourgeault et al., 2010).
By the end of 2022, there were 58,605 documented migrant home care workers and an additional 13,298 undocumented migrant home care workers in Israel. The majority come from the Philippines, with notable representations from India, Nepal, and Eastern Europe (Population and Immigration Authority, 2022). Migrant home care workers are expected to live in the home of the care recipient and provide personal care, including limited responsibilities for maintaining the physical living environment of the older person.
There is a growing body of research on the triadic or even larger network of caregivers and care recipients which evolves in the context of migrant home care workers (Ayalon, 2022). Oftentimes, family members do not neglect their role as carers. Instead, with the entrance of the migrant home care worker, they are more likely to resort to instrumental care, including the management of the caregiving arrangement (Ayalon, 2009a). Migrant home care workers, on the other hand, tend to provide personal care in addition to emotional care, as they are the ones who provide daily care to the older person (Ayalon, 2009a). Research has shown that not only is the care being shared between family members and migrant home care workers, but also the well-being and subjective health perceptions are shared, so that greater involvement of the family member results in improved well-being and subjective health among migrant home care workers and vice versa (Ayalon & Green, 2013).
Dementia care
Dementia is a syndrome that can be caused by several diseases which over time destroy nerve cells and damage the brain, typically leading to deterioration in cognitive function (i.e. the ability to process thought) beyond what might be expected from the usual consequences of biological ageing. It is characterized by a progressive deterioration of cognitive function, with memory being the most notable change. Abstract reasoning and personality characteristics also change, especially in more advanced stages. Although many types of dementia exist, Alzheimer’s disease is the most common one, characterized by an average life expectancy of 8–10 years from the initial diagnosis and is accompanied by a gradual loss of faculties to the point of needing ongoing supervision and assistance in daily life (Knopman et al., 2021). In Israel, there were approximately 154,000 individuals who have some form of dementia as of 2019. This number is expected to increase substantially over time (Bentur & Sternberg, 2019).
Addressing behavioral problems of dementia is considered particularly challenging (Adebayo et al., 2020; Mulsant, 2014). An Israeli study has found that those migrant home care workers who provided care to an older person with dementia were more likely to express an intent to leave their job compared with those who cared for an older person without dementia (Ayalon, 2010). Likewise, family members also report high levels of stress in the face of behavioral problems (Kim et al., 2021). Knowledge of dementia and its accompanying challenging behaviors is considered one factor that possibly improves the care provided to older persons with dementia (Spector et al., 2012). Cultural beliefs and attitudes also result in differential care practices and the ability to cope with care challenges (Andruske & O'Connor, 2020; Assfaw et al., 2024; Brooke et al., 2018). Moreover, addressing the challenges posed by the behavioral problems of dementia often requires using individually tailored behavioral strategies designed to meet the specific needs of the person with dementia (Livingston et al., 2005).
The present study
In light of the challenges associated with providing care to a person with dementia, this study was set to examine the perspectives of family members and migrant home care workers concerning dementia care. In our inquiry, we specifically focused on their perception of dementia and its accompanying behavioral problems, strategies used, and how dementia and its accompanying challenges are addressed within the caregiving context, which consists of an older person with dementia, a migrant home care worker, and family members. Given past research, which has shown that the care of older persons with dementia is impacted by the cultural origin of the carer (Ahmad et al., 2020), the present study provides valuable information as it examines how people of different cultures and different care roles negotiate the understanding of dementia and its care within the caregiving context.
Methods
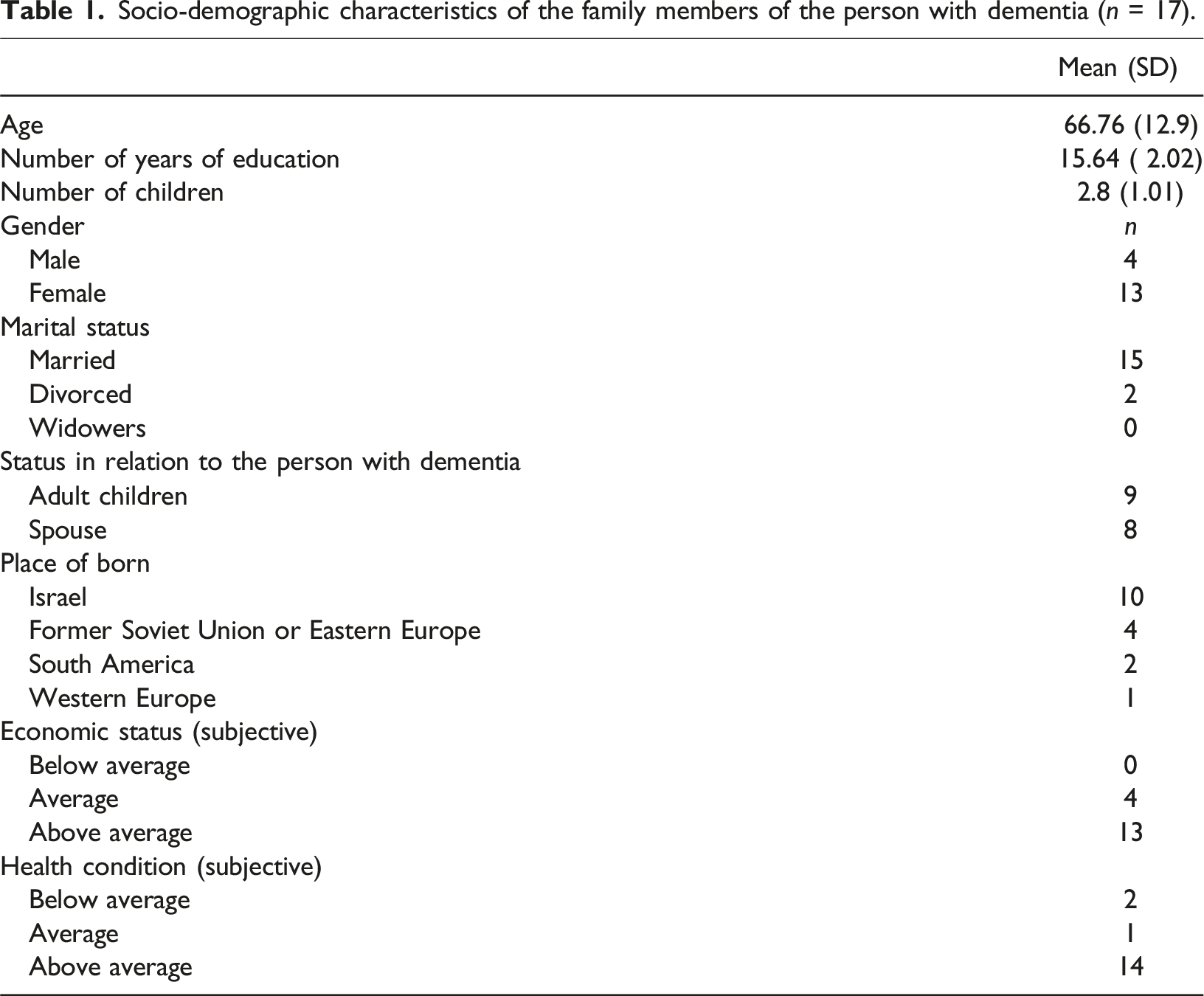
Socio-demographic characteristics of the family members of the person with dementia (n = 17).
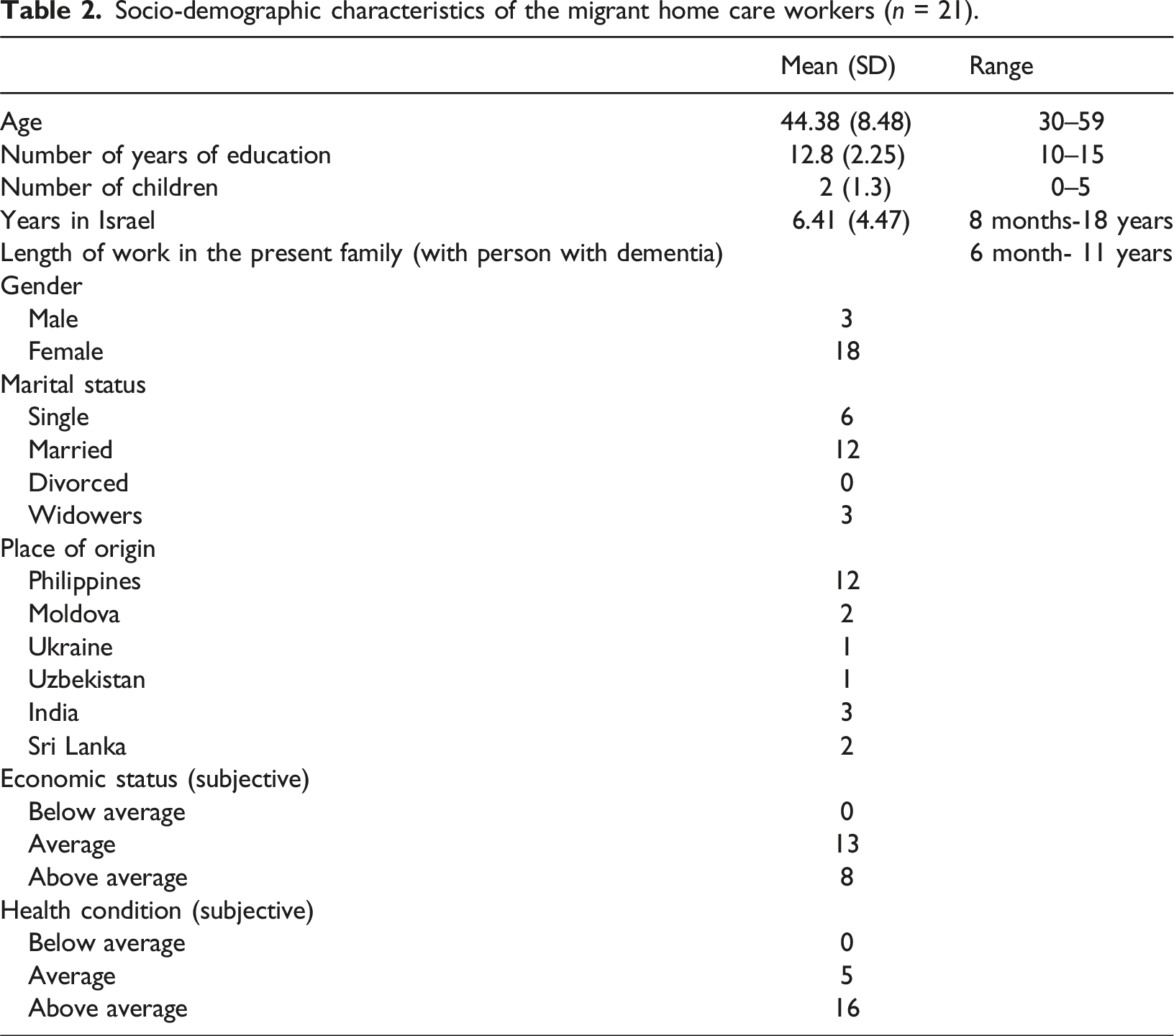
Socio-demographic characteristics of the migrant home care workers (n = 21).
Procedure
The majority of respondents were interviewed in their homes or another private location of their choice. Interviews were conducted separately with each participant. Interviews with family members were conducted in Hebrew, whereas interviews with home care workers were conducted in English, Hebrew, or Russian, based on their preference. All participants filled out a short questionnaire concerning socio-demographic information. The interview guides of family members and migrant home care workers were similar, with limited modifications. We started with a broad question, such as “How do you perceive dementia? A person with dementia?” Followed by more specific questions, such as “How do you define good care for a person with dementia?”, “What are the challenges in your work?”. For more information concerning the interview guide see Online Appendix. Interviews lasted between half an hour and an hour and a half. All interviews were recorded, transcribed and anonymized.
Analysis
We conducted thematic analysis (Braun & Clarke, 2012), starting by reading and re-reading each of the interviews in order to familiarize ourselves with the data. This was followed by thematic coding of each of the interviews, identifying broad, descriptive units of meaning. Subsequently, we grouped the descriptive themes into more interpretative themes to represent a more coherent summary of the interviews. Analysis was conducted separately for family members and migrant home care workers, going back and forth between and within interviews. To present a coherent storyline, we omitted themes that addressed systemic challenges associated with the care arrangement. We also omitted themes related to challenges associated with the care arrangement which were not directly related to dementia care and the management of behavioral problems. These themes are discussed elsewhere.
To improve the trustworthiness of the study (Elo et al., 2014), we rely on two sources of information, family members and migrant home care workers. Incorporating two sources of information allows us to apply methodological triangulation, enhancing the depth and breadth of our analysis. This triangulation is not intended to validate findings directly through mere agreement between sources but rather to enrich our understanding of the care arrangement by highlighting common and different views. The inclusion of multiple perspectives ensures a more comprehensive exploration of the phenomenon, capturing a fuller range of experiences and interpretations that might be missed by relying on a single perspective. We also relied on two individuals who coded the data independently. Both have many years of experience conducting qualitative research. We maintained an audit trail documenting all stages of the analysis and providing a thick description of the interviews to ensure that the readers will be able to determine the suitability of the themes identified.
Findings
The themes identified in interviews with family members (n = 17) and migrant home care workers (n = 21), accompanied by direct excerpts.

The second theme concerned the management of the care recipient’s behavioral problems. Both family members and migrant home care workers stated that attributing behavioral problems to the disease, rather than to the person with the dementia, is helpful as a means to view the situation more empathically. Family members also reported a technique termed “going with the flow” to accept problematic behaviors rather than attempting to correct or challenge them: “If she (care recipient) says, I want to stand up, I can’t say no. She will be angry with me. This is the dementia” (Daughter, age 65).
Caring with love and patience like a family member, including being responsive and attentive to the care recipient, were reported as strategies employed by migrant home care workers:
Unlike family members, migrant home care workers mentioned that repetitively communicating the same information or instructions to individuals with dementia could be useful. They believe this approach helps in managing behavioral problems and serves as a preventive measure against the manifestation of challenging behaviors such as yelling, screaming, and hitting. Last, migrant home care workers also reported willingness to suffer through the situation as a means to deal with the challenges of providing care for a person with dementia: “Yes, you need “to absorb” things; you need to suffer… I don’t know how to say it; just not refer to it… it’s hard work, of course, it’s not… mentally, it’s hard work. I think you need patience; you need to suffer.” (A migrant worker from Moldova, female, age 50)
The last theme concerned the relationship between family members and the migrant home care worker in the context of the care provided to an older person with dementia. Both family members and migrant care workers discussed their mutual relationships in this setting as essential to ensuring adequate care for the older care recipient. Family members acknowledged cultural differences and expressed a need to mediate them to ensure appropriate care by the migrant home care worker. For example, they mentioned language proficiency as being crucial for effective communication. They also discussed gaps in dementia knowledge, and different understandings and perceptions of familial relationships, emotional expressions, customs, and holidays in Israeli society. In addition, they noted differences in dietary practices and behaviors, including the principles of kashrut in religious Jewish culture and general eating habits and etiquette: “There are very large gaps in culture, very large gaps in understanding things, in many things, yes”( Son, age 55).
These disparities can hinder communication and mutual understanding between all involved parties, potentially diminishing the effectiveness of care and interaction with individuals with dementia. To address these challenges, some family members advocated for “educating” migrant care workers about the host society’s culture to bridge these gaps and enhance their caregiving efficiency. Additionally, good communication and good relationships, including paying extra money and “cutting corners,” were identified by family members as means to ensure that the migrant home care worker is satisfied and, as a result, provides satisfactory care to their loved one with dementia. Trusting the migrant home care worker was also identified as an essential ingredient in this context: “We can relieve her so she can get some fresh air, go out to recharge her batteries. I try to come once a week. My sister also tries to visit. We really make an effort and tell her: ‘Go out, take some time for yourself.’ We are interested in her well-being, (…) we need to give her a good feeling, show her that she is important, that we appreciate her work. She really works hard, and I know it’s tough. It’s about showing appreciation, giving her a kind word, strengthening her, and telling her that what she does is great and that she is good.” (Daughter, age 49)
Like family members, migrant home care workers acknowledged the importance of maintaining adequate relations with the family, stressing the importance of gaining the family’s trust, respect, and protection in the face of older persons with dementia: “If you (family members) love them (caregivers)- they will love you more. Give them humanity and proper treatment. We are also humans, and we need proper treatment; we are foreign here, so give us just respect and proper treatment. That’s it.” (Migrant worker from the Philippines, female, age 52).
The need to acquire knowledge about the older person and the role of family members as mediators of this knowledge was also acknowledged. Migrant home care workers also reported the need to take care of their own mental and physical well-being.
Discussion
With the increasing life expectancy and the direct association between advanced age and dementia, dementia and its behavioral problems are expected to pose an ongoing, growing challenge to society at large, as well as to older persons with dementia, their family members, and their migrant home care workers (Radue et al., 2019; Tan et al., 2005). There is a growing realization that at least some of the care provided to older persons, including the way carers interpret and address dementia and its behavioral problems, is culture specific (Ahmad et al., 2020; Andruske & O’Connor, 2020; Brooke et al., 2018). This was clearly evident in the present study as family members and migrant home care workers attributed some of the challenges, they have faced to the cultural gaps which challenge the relationship between the different stakeholders. As such, it is particularly important to examine the perspectives of carers from different cultures who gather forces in the care of older persons with dementia. The present study provides a unique outlook on the caregiving context, by examining perspectives of family members and migrant home care workers who provide care to an older person with dementia.
Our findings suggest that both family members and migrant home care workers report similar challenges associated with the care of a person with dementia. These challenges are consistent with the literature (Kim et al., 2021; Tan et al., 2005) and include verbal and physical aggression, repetitive questions, and disruptions in the sleep-wake cycle. Our findings reveal, however, that migrant home care workers are more likely to directly confront these challenges as those providing direct care. Hence, their interviews included rich examples of experiences they have had, rather than a discussion of incidents they observed. This is because migrant care workers are the ones who provide daily care and have the most frequent and intense interactions with the care recipients (Ayalon, 2009a). This also could be attributed to the fact that migrant carers as newcomers to the home, are more likely to be perceived as a threat by the older care recipient and thus, are more likely to be exposed to behavioral challenges presented by the older care recipient. Additionally, the aspect of cultural difference or ‘otherness’ of migrant care workers may contribute to fear or agitation on the part of the person with dementia, further complicating their reaction to the caregiver’s presence.
Although there is a growing body of literature concerning the role that culture plays in dementia care (Adebayo et al., 2020; Ahmad et al., 2020; Brooke et al., 2018), our analysis has identified several similarities between Israeli family members and the migrant home care workers, which suggest an overall culture of care. Specifically, both family members and migrant home care workers stressed the need to acknowledge the nature of dementia and its accompanying behavioral problems as being responsible for the older care recipient’s behaviors, rather than the older care recipient’s personality characteristics. However, mainly family members stressed the need to “go with the flow” and not to argue when they were presented with verbal abuse or repetitive communication of the older care recipient. Interestingly, migrant home care workers described the care needed to alleviate and address behavioral problems as being “family-like” and characterized by love and patience. Hence, they viewed family relations as ideal and acknowledged their role as family-like members. This accompanies a growing body of literature that discusses the role of migrant home care workers in the family as fictive kin (Baldassar et al., 2017; Lovelock & Martin, 2016). It also corresponds with the notion of care as a universal need, which should be performed out of empathy and respect, regardless of cultural values and attitudes.
Whereas family members stressed the need to “go with the flow,” migrant home care workers emphasized the need to repeat the same commands or information over and over. Although at first glance, these might seem like contradictory approaches, they, in fact, are in agreement as repeating the same information is one approach to “go with the flow” and avoid arguments with the care recipient. As both migrant home care workers and family members reported repetitive questions as a disturbing behavior, it is not a coincidence that migrant home care workers, who have the most contact with the older care recipients, have developed specific techniques to address repetitive questions.
Migrant home care workers also reported a requirement to “keep suffering” as a desired approach to caring for a person with dementia. Past research has stressed the emotional labor done by service workers (Leidner, 1999), including migrant home care workers, who provide emotional care in addition to personal care (Ayalon, 2009a). In this study, we stress the impact of providing such emotional care on one’s wellbeing. As migrant home care workers are at the forefront when it comes to patient care, it is no coincidence that they are the ones most affected by the provision of such care.
An important finding of the present study concerns the perspectives of family members and migrant home care workers regarding the caregiving context. Both family members and migrant home care workers acknowledged their interdependence, with family members being identified as essential mediators in the care of an older person with dementia. Family members emphasized the cultural differences between themselves and the migrant home care workers, highlighting their role in mediating knowledge about dementia as well as specific information about the older care recipient’s needs and preferences. A similar finding was identified in past research conducted in Israel (Ayalon, 2009a). The problem is that this position assumes that family members inherently possess superior or more accurate knowledge about dementia. This assumption opens up a broader discussion on the necessity of culturally sensitive care within live-in caregiving contexts. It underscores the importance of raising awareness about the diverse understandings of dementia across cultures and the imperative to navigate these differences collaboratively.
Family members also acknowledged the importance of maintaining good relationships with the migrant home care workers, making compromises at times and, on other occasions, providing the worker with additional financial incentives to ensure their stay. At the same time, family members also stressed the importance of ensuring open communication and trust between parties to improve the care of the older person with dementia. Past research has shown that family members often go an extra step by providing migrant home care workers with gifts, extra money and time off in order to ensure their loyalty to the family, especially under conditions of high demand and low supply of migrant care workers (Ayalon, 2009b). When the older person experiences dementia, his or her working conditions are even more challenging and as such, extra attention and adequate relationships become essential.
As in past research (Ayalon, 2009a), migrant home care workers as well addressed the importance of family members in ensuring their ability to provide adequate care to the older care recipient. They stressed the importance of family-like relations not only towards the older person with dementia, but also in relation to the family members. In fact, migrant home care workers stated that to provide “family-like” care to the older care recipient, they expect, a “family-like” approach from his or her family members. Specifically, they expected a respectful attitude, and trust as well as physical protection from abuse. Just like family members, they too viewed the role of family members as mediators of knowledge not only concerning what dementia and its behavioral problems are but also concerning the older care recipient.
Finally, migrant home care workers stressed the importance of taking care of their own mental and physical health. This includes taking some time off, but also having adequate sleep at night and a safe environment. It is important to note that although family members certainly acknowledged the importance of ensuring the migrant home care workers’ satisfaction with the care arrangement, and stressed the issue of monetary compensation, they hardly mentioned the need to provide adequate working conditions to the migrant home care worker. This discrepancy should be stressed when preparing family members to this caregiving arrangement to ensure that they are well-aware of the challenges faced by migrant home care workers and of the need to improve their working and living conditions to ensure their stay. At the same time, this expectation introduces complexities as the migrant home care workers are not actual family members, leading to fluctuating roles and expectations. These blurred boundaries between professional and familial roles may create challenges, as the dynamics of care provision can become complicated by the varying interpretations and implementations of what constitutes “family-like” care and interaction. Such a scenario underscores the need for clear communication and boundary-setting to manage expectations and responsibilities, ensuring that the caregiving arrangement benefits all parties involved, especially the care recipient.
Despite its strengths, the study has several limitations that should be considered. First, we did not include interviews with older persons in this study because of the challenges of interviewing older persons with advanced dementia. Our attempts to interview older care recipients and obtain their perspectives have been largely futile. We also do not have the exact data concerning the stage of dementia diagnosis, other than what was reported by family members. In addition, although the study possibly sheds light on the role of culture in determining attitudes towards dementia and ways to address it, we were unable to thoroughly examine it as the migrant home care workers came from several different countries and cultural contexts. Moreover, the Israeli family members interviewed also do not constitute a homogenous group as there are variations in education, socioeconomic status, and country of origin in this group as well, which potentially result in differential care provided to older persons. Hence, it is more accurate to view the findings as emerging from two different care roles, rather than different cultural origins. More comprehensive research is needed to determine the extent to which our findings reflect the impact of distinct care roles versus diverse cultural backgrounds. Use of scales that directly measure burden and relationship between the different stakeholders, as well as the reliance on videotaped material to better capture the interactions between the different stakeholders will enhance future understanding of the topic.
Despite its limitations, the study has multiple strengths that should be acknowledged. The reliance on the viewpoints of both family members and migrant home care workers is a first step in ensuring coordinated care, given the need to rely on both family members and migrant care workers in the care of older persons with dementia. Our findings stress that the different stakeholders have quite similar perspectives concerning what the most challenging behaviors associated with dementia are as well as ways to address them. Moreover, both family members and migrant home care workers recognize the role of family members as mediators and as those who ensure adequate working relations of the migrant care workers and thus, are directly responsible for protecting the mental and physical wellbeing of the worker. Our findings also highlight the importance of viewing this caregiving arrangement within the context of “family-like” care. The idea that migrant home care workers can offer more personalized and effective care by viewing the care recipient as part of the family holds merit. However, this approach necessitates reciprocal familial treatment of the migrant home care worker by the family members. Moreover, it is essential to relate to this concept with caution because an inherent tension exists between the roles of a care provider and a ‘quasi-family' member, compounded by underlying commercial interests. Specifically, to provide adequate care to an older care recipient with dementia, migrant home care workers should view them as family members. However, to do so, they expect to receive a similar approach from family members. Policy stakeholders and clinicians responsible for this caregiving arrangement should use these insights to better prepare family members and migrant home care workers for this caregiving context and the challenges it brings.
Supplemental Material
Supplemental Material - Caring for an older person with dementia: Behavioral problems in the eyes of family caregivers and migrant home care workers
Supplemental Material for Caring for an older person with dementia: Behavioral problems in the eyes of family caregivers and migrant home care workers by Liat Ayalon and Natali Ulitsa, Anna-Eva Nebowsky and Mark Schweda, Milena von Kutzleben in Dementia
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Volkswagen foundation (11-76251-2684/2021 ZN 3864).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
Author Biograpphies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.