
Abstract
Introduction
Over 55 million people worldwide have dementia (WHO, 2023). An additional 19.7% are living with mild cognitive impairment (MCI), which can develop into clinical dementia (Bruscoli et al., 2004; Busse et al., 2006; Song et al., 2023). The economic consequences total a global cost of US$23,796 per person with dementia, half of which is subsidised by informal care (Wimo et al., 2023). The personal consequences are challenging. Psychologically, people with dementia can experience grief, sadness, and loss of self-esteem (Aminzadeh et al., 2007; Lee et al., 2014; Scott, 2022). Functionally, changes can result in greater dependency on others and reduced relationship quality across social networks, and this can negatively impact on quality of life (Jing et al., 2016; Moyle et al., 2011; Nakayama et al., 2017; Victor et al., 2021). Thus, maintaining and improving the quality of life of people living with dementia and MCI is a research priority (Department of Health, 2015; Parkin & Baker, 2021).
Digital interventions, which can be defined as ‘Interventions delivered via information and communication technologies’, might improve quality of life and be cost effective (Murray et al., 2016). Newer forms recognise the active role individuals with dementia can play in using technology, leading to more interactive interventions such as cognitive stimulation or training, reminiscence opportunities, and virtual reality (Cipriani et al., 2006; Hayhurst, 2018; Irazoki et al., 2020; Lazar et al., 2014). There is also significant investment in digital interventions for people living with dementia to diagnose, monitor and intervene (Long et al., 2023). The effectiveness of assistive technology devices and telecare to achieve this is well documented (Chien et al., 2011; Pappada et al., 2021; Van der Roest et al., 2017). Reviews have also explored the effectiveness of digital interventions for improving outcomes such as social interaction, and wellbeing across multiple settings (Anderson et al., 2022; Bradley et al., 2023). Understanding the effectiveness of digital interventions that require engagement from people with dementia has also begun to be explored (Holthe et al., 2018), however, so far, these have not focused on whether interventions improve quality of life.
Dequanter et al. (2021), reviewed the development and effectiveness of digital interventions to support the quality of life of people living with dementia between 2013–18. In their review, they map interventions on to van Bronswijk, Bouma, and Fozard (2002) technology application domains. This framework focuses on how technology can be applied to improve older adult’s quality of life. Whilst their findings provide promising evidence that digital interventions can improve the quality of life of people with dementia and their carers, it is useful to explore digital interventions using a dementia specific quality of life framework.
Also, Dequanter et al.’s (2021) review does not consider how people living with dementia experience using interventions. Popular frameworks for developing complex interventions emphasise that development should focus on effectiveness, context, and implementation, to understand for whom, how and in what context the intervention may be useful (Skivington et al., 2021). To achieve this, exploring experience as well as effectiveness is essential.
This review aimed to fill this gap by answering the questions: • What is the effectiveness of digital interventions which require interaction from people with dementia or MCI for improving their quality of life? • What are the experiences of people with dementia or MCI when using these digital interventions?
Findings from this review will be used to develop understandings of what domains of quality of life can be improved by digital interventions and how intervention delivery might be optimised.
Method
The reporting of this systematic review was guided by the standards of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Statement (Moher et al., 2009). The protocol was registered on PROSPERO (CRD42023388030) in February 2023.
Search strategy
Databases, MEDLINE [Ovid], PsycINFO, EMBASE, CINAHL and Web of Science were searched in February 2023 using MeSH terms and free text (supplemental material 1). Searches were supplemented by searches in Google Scholar and hand searching of reference lists. Additionally, RSS alerts were set for the specified search terms.
Eligibility criteria
Inclusion and exclusion criteria were defined using the PEO framework (Capili et al., 2020).
Types of studies
Quantitative, qualitative and mixed-methods peer reviewed literature, written in English, and published between January 2018 - February 2023 were included.
Types of participants
Samples where at least 50% of participants were community dwelling people diagnosed with dementia or MCI, or samples containing dementia carer dyads were included. These were only included if participants had been diagnosed with MCI or dementia using a validated criterion. Validated criteria included diagnoses according to the Petersen (2001) criteria, the ATN (Clifford et al., 2016), NINCDS-ADRDA (McKhann et al., 1984), or diagnoses made by healthcare professionals. Community dwelling was defined as individuals living at home or in someone else’s home, including sheltered or support accommodation. We excluded people living in nursing homes, residential facilities, acute or psychiatric hospitals, and those receiving end of life care.
Types of interventions
Digital interventions, defined as ‘interventions delivered via information and communication technologies’ (Murray et al., 2016) were included if the participant had interacted with them. Interaction was defined as the person with dementia taking some control over the use of the intervention, independently or with support. This meant participants were required to use the intervention beyond the set-up period, such as pressing buttons, speaking into the device, or using their body to communicate and interact with the technology in some manner.
Types of outcomes
Quantitative data measuring any quality-of-life domain using a validated scale, as either a primary or secondary outcome were included. Outcomes were grouped according to the domains of quality of life defined by Smith et al.’s., (2005) conceptual framework of health-related quality of life. This framework is a dementia specific quality of life framework developed with people living with dementia and includes five concepts: daily activities and looking after yourself, health and wellbeing, cognitive functioning, social relationships, and self-concept. Additionally, qualitative data related to participants' experiences with digital interventions were included.
Study selection
Duplicates were removed using EndNote and RAYYAN software packages. Titles and abstracts were screened independently by two authors (AD and HA) for eligibility. Full versions of potentially relevant articles were obtained and reviewed for eligibility independently by AD and HA. Discrepancies were discussed, and if unresolved considered by the full research team for a decision.
Data extraction
Data were extracted by one author (AD), and a second author (HA) independently extracted data from 7% of the articles to verify the accuracy of the extraction. There were no discrepancies, so remaining data were extracted by AD into bespoke tables based on the ‘Cochrane Collaboration Data Collection Tools’ (Li et al., 2023). Extracted data included: • Participants: age, gender, diagnosis, ethnicity, socio-demographic background, sample size, baseline cognitive status. • Methods: study location, publication date, study design, recruitment strategy, attrition, follow up, setting. • Interventions: intervention name, software, hardware, support given to use intervention, length and frequency of intervention, control group information. • Outcomes: primary and secondary quantitative outcomes, direct participant quotes, author interpretations, observations, reflexive notes, and thematic analysis themes.
Quality assessment
Study quality was assessed using appropriate Joanna Briggs Institute (JBI) quality assessment checklists. The Mixed Methods Appraisal Tool (MMAT) was used for mixed methods studies (Hong et al., 2018).
Article quality was graded by author AD with 7% also being independently graded by HA for accuracy checking. Checklist items were graded as ‘yes’, ‘no’, ‘can’t tell’, and ‘not applicable’. Discrepancies were minimal (12%). All articles were then re-evaluated for quality by AD based on HA’s comments with AD making the final decision.
Each article received a quality percentage score based on the number of checklist criteria they met using the formula
Traditionally in qualitative meta-syntheses, credibility of individual findings is graded based on the number of supporting illustrations using CONQUAL (Munn, 2014a). This categorises study findings as either supported or unsupported. Unsupported findings are usually excluded from analyses. The complexities of data integration means that mixed-method review guidance does not recommend grading and excluding qualitative findings based on credibility (Stern et al., 2020). Therefore, all findings from the qualitative articles are included, even if not supported by illustrations.
Methods of data synthesis
A convergent segregated approach was used to synthesise data in accordance with JBI guidance and methodological papers (Heyvaert et al., 2011; Hong et al., 2017; Stern et al., 2020). This involved synthesising quantitative and qualitative data separately and integrating them at the end to form a narrative.
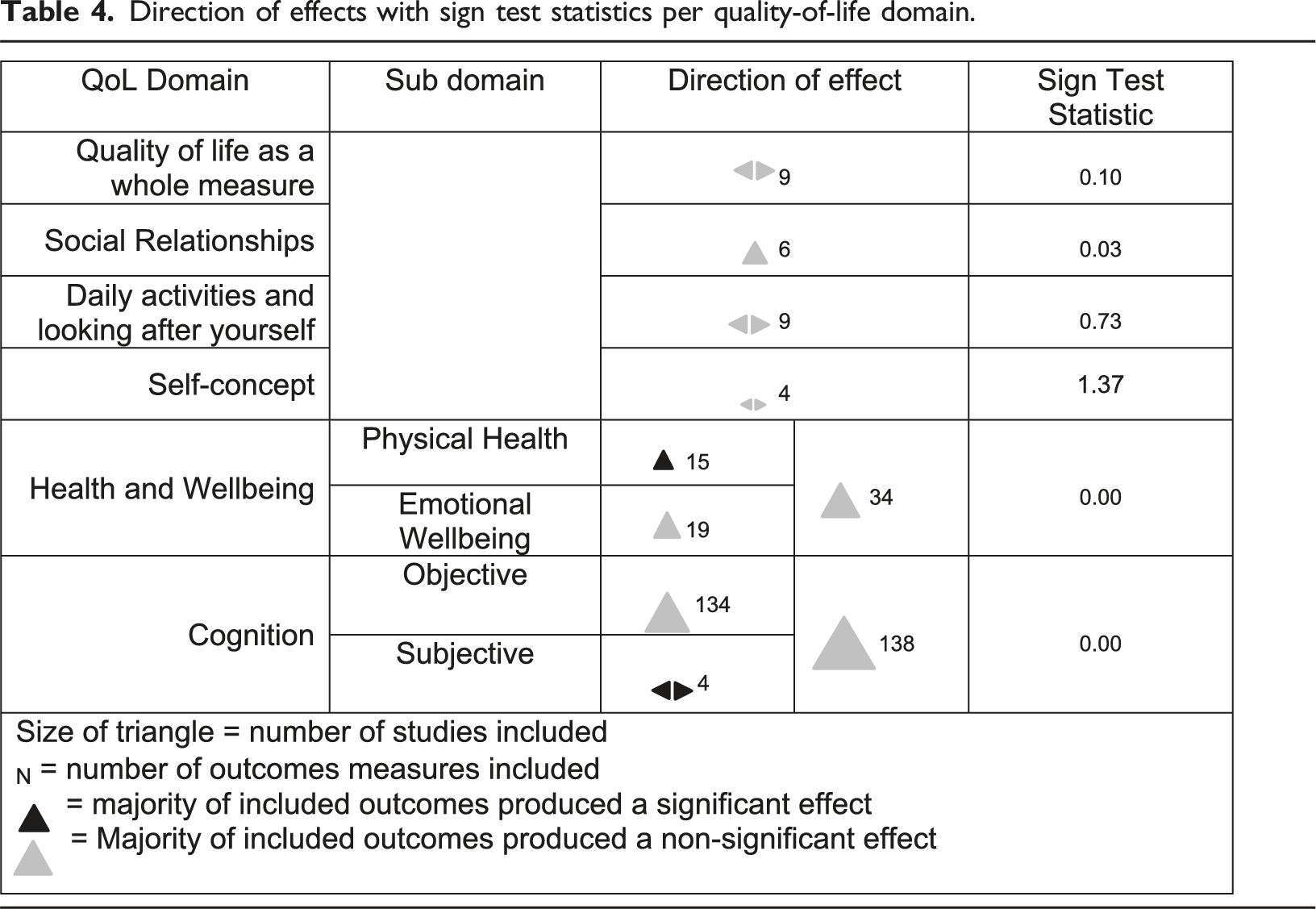
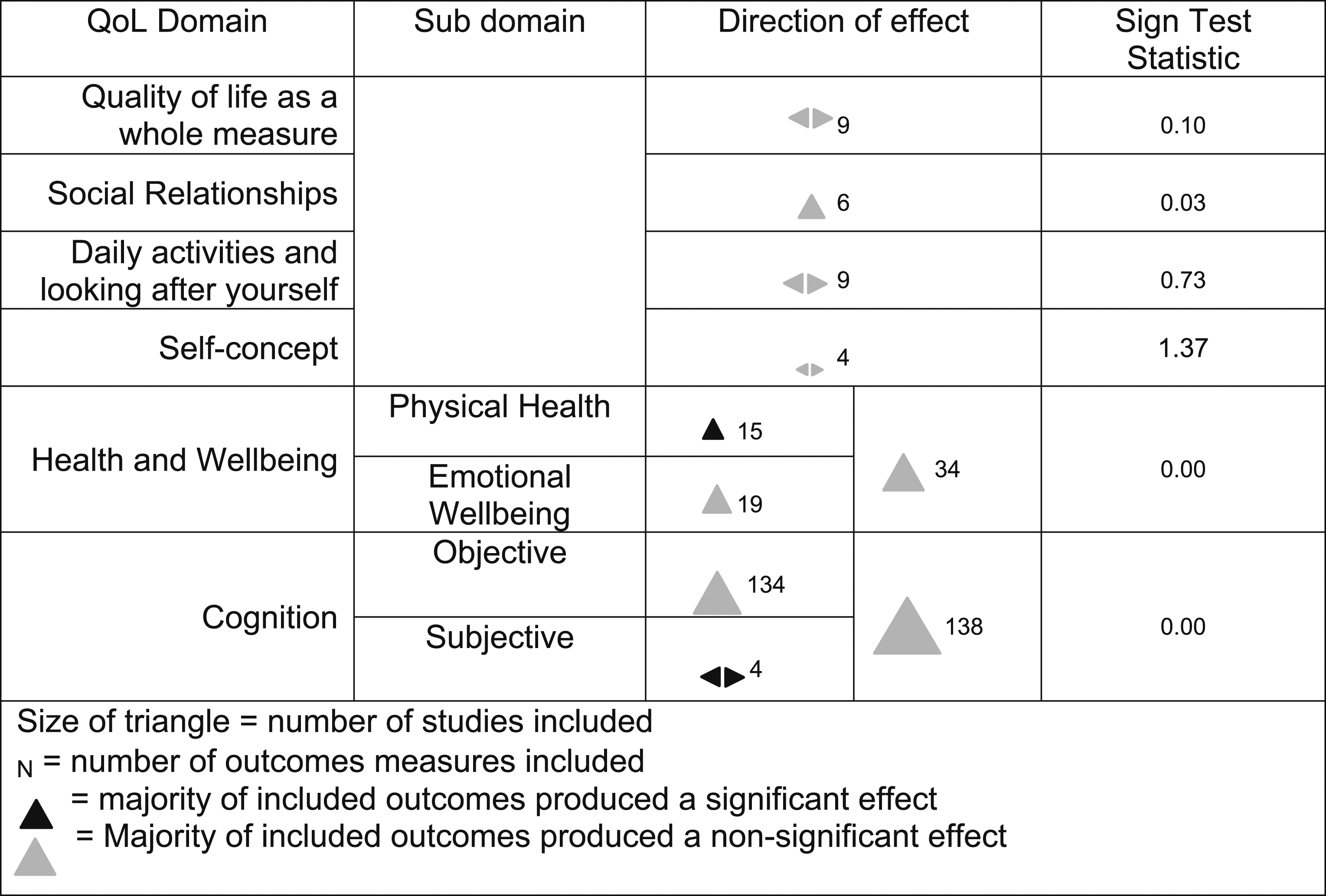
Quantitative data was narratively synthesised to determine effectiveness (Campbell et al., 2020). Articles were grouped by quality-of-life domain, determined by the outcome measures used. Several articles measured multiple quality of life domains and are therefore repeated within the synthesis. Vote counting based on direction of effects with sign test statistics were used to determine intervention effects using mean difference values, effect sizes and p statistics. This involved categorising each outcome as showing benefit or harm, regardless of effect size or statistical significance, creating a binary metric (McKenzie et al., 2023). The metrics were then grouped by quality-of-life domain and a sign test statistic was used to determine the presence of a positive effect (McKenzie et al., 2023). Sign test statistics that reached significance (p = ≤0.05) demonstrated that digital interventions positively influenced quality of life.
Qualitative data was synthesised using meta-aggregation (Lockwood et al., 2015). This involved extracting all findings produced by authors of the included articles, grouping these into categories, and grouping categories to form synthesised review findings. The aim of producing synthesised findings was to provide recommendations for optimising intervention delivery (Munn, Tufanaru, & Aromataris, 2014).
Both syntheses were then integrated together by juxtaposing and linking the findings to produce a third synthesis (Harden, 2010; Stern et al., 2020). This synthesis is presented in narrative recommendations on how digital interventions can benefit the quality of life of people living with dementia, and how delivery may be optimised.
Results
Included studies
6046 citations were retrieved from electronic databases and an additional 529 citations were retrieved from additional searches, resulting in a total of 6,575 publications. Of these, 73 articles met eligibility. 59 contained quantitative data related to quality-of-life outcomes, and 18 contained qualitative data related to experience (Figure 1) (Page et al., 2021). Study characteristics for all studies can be found in Table 1. PRISMA flowchart for study selection. Study characteristics of included studies. Abbreviated terms: PwD, Person with Dementia type unspecified; ADL; Daily activities and looking after yourself; ASCOT, Adult Social Care Outcomes Toolkit; MSPP, Maastricht Social Participation Profile; DQoL, Dementia Quality of Life Instrument; MMSE, Mini-Mental State Examination; GQOL-74, Generic Quality of Life Inventory-74; BDI, Becks Depression Inventory; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; MOCA, Montreal Cognitive Assessments; GDS, Geriatric Depression Scale; CAMCOG, Cambridge Cognition Examination; RBMT, Rivermead Behaviour Memory Test; TMT, Trails Making Test; DQOL, Dementia Quality of Life Measure; Euro-QoL-5D, European Quality of Life Five Dimension Five Level Scale; RCFT, Rey Complex Figure Test; AD-QoL, Alzheimer’s Disease-Related Quality of Life; DQOL, Dementia Quality of Life Instrument; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; NPI, Neuropsychiatric Inventory; QOL-AD, Quality of Life- Alzheimer Disease Scale; CDR, Clinical Dementia Rating; ACE-R, Addenbrookes Cognitive Examination-Revised; ACE-III, Addenbrookes Cognitive Examination; SDST, Symbol Digit substitution Test; WAIS, Wechsler Adult Intelligence Scale; PRMQ, Prospective and retrospective Memory Questionnaire.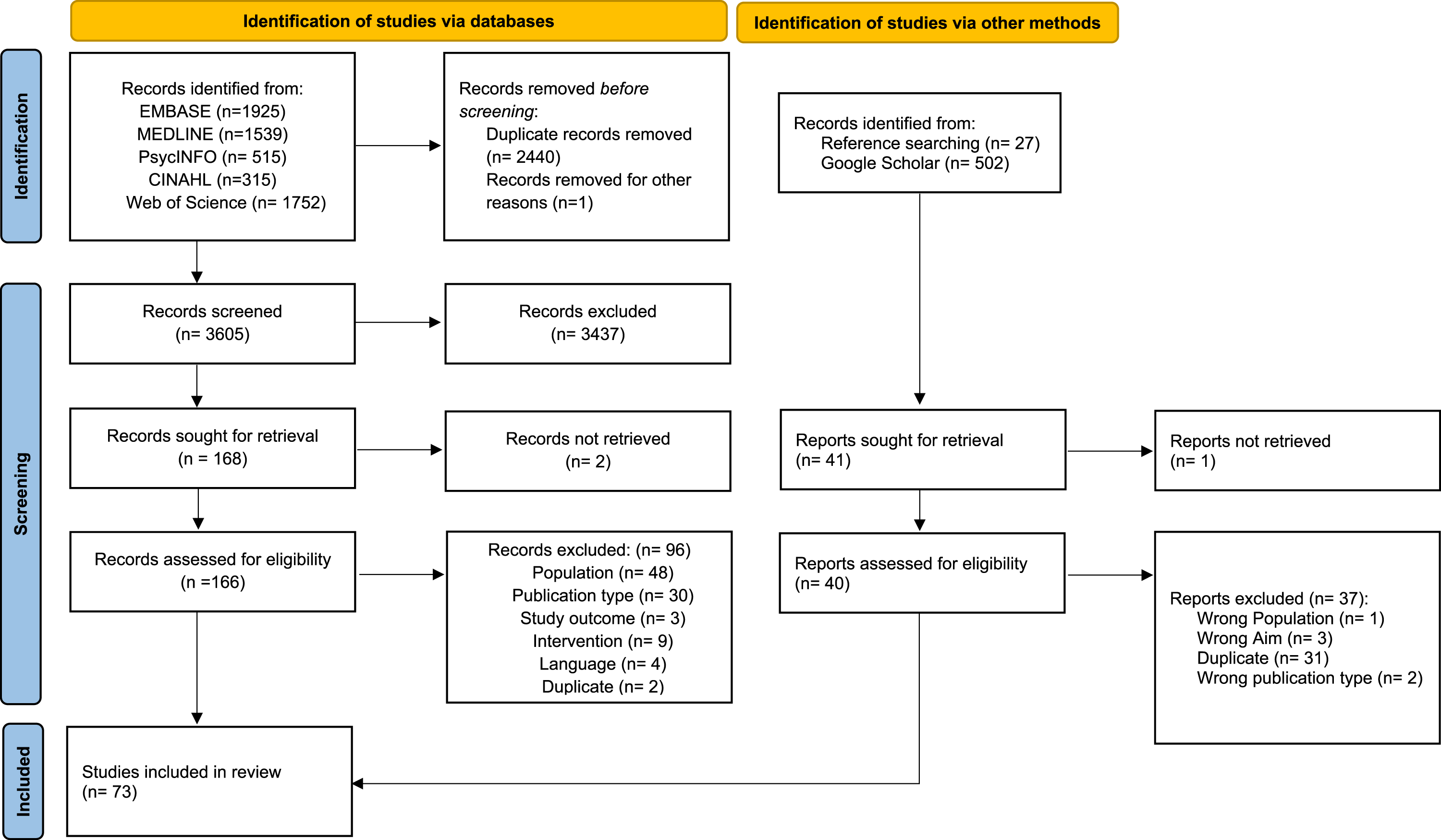

Quality of articles
Overall study quality varied. RCT’s were mostly of moderate quality (Park, 2022a; Park, Liao, et al., 2020; Park, Jung, & Lee, 2020; Poptsi et al., 2019; Schmitter-Edgecombe, 2022; Scullin et al., 2022; Shyu et al., 2022; Thapa et al., 2020; Torpil et al., 2021), twelve were of low quality (Amjad et al., 2019; Beentjes, Neal et al., 2020; Han et al., 2020; Jirayucharoensak et al., 2019; Knoefel et al., 2018; Li et al., 2019; Marin et al., 2022; Park 2020a; Phatak et al., 2021; Sautter et al., 2021; Singh et al., 2022; Yang et al., 2022). They commonly failed to provide sufficient detail of concealment, blinding, details of power calculations, or justifications of sample size. Non-randomised studies were mostly moderate quality (Bojan et al., 2021; Debring et al., 2021; Kim et al., 2021; Maeng et al., 2021; Petersen et al., 2020; Tsolaki et al., 2020; Zhang et al., 2019; Zhu et al., 2022), two were low quality (Burgos-Morelos et al., 2023; Chen et al., 2022). Commonly these lacked control groups, incomplete outcomes, lacked detail regarding the reliability of outcome measurement, showed no power calculations, or justifications for sample sizes. Mixed Methods designs were all high quality. Missing was a lack of description on the impact of confounding variables and descriptions related to risk of non-response biases. Case study designs were high quality, except for the case series design which was low in quality (Fasilis et al., 2018). This lacked clear descriptions of the participant information and reporting of site demographics. All qualitative studies were high quality except Øksnebjerg et al. (2019) which was low quality. This study failed to describe philosophical and methodological perspectives, had unclear analytical methods, and provided insufficient participant data to determine adequate representation of participants. They also did not locate the researcher theoretically or culturally in the study, a common flaw amongst 55% of the qualitative studies (Berrett et al., 2022; Critten & Kucirkova, 2019; Ryan et al., 2020; Øksnebjerg et al., 2019). The quality assessment checklist scores for all studies are presented in supplemental material 2.
Quantitative Synthesis
Study characteristics
Most articles were randomised control trials (n = 35, see Table 1). Study designs also included non-randomised control trials (Cinar & Sahiner, 2020; Kim et al., 2021; Maeng et al., 2021; Petersen et al., 2020; Tsolaki et al., 2020), within subject designs (Bojan et al., 2021; Burgos-Morelos et al., 2023; Chen et al., 2022; Debring et al., 2021; Laird et al., 2018; Taylor et al., 2020; Zajac-Lampaska et al., 2019; Zhang et al., 2019; Zhu et al., 2022), mixed methods (Kerkhof et al., 2022; König et al., 2022; Mattos et al., 2021; Sheehy et al., 2022), case studies (Edgar & Bargmann, 2021; Foloppe et al., 2018; Imbeault et al., 2018a, 2018b), case series (Fasilis et al., 2018), and a cost effectiveness design (Ferry et al., 2020). Twenty articles did not report their location. Of those that did, locations included Europe (Diaz Baquero et al., 2022; Beentjes, Neal, et al., 2020; Bojan et al., 2021; Debring et al., 2021; Fasilis et al., 2018; Ferry et al., 2020; Foloppe et al., 2018; Laird et al., 2018; Marin et al., 2022; Nousia et al., 2021; Petersen et al., 2020; Poptsi et al., 2019; Rai, Schneider, & Orrell, 2021; Rodella et al., 2022; Sautter et al., 2021; Tsolaki et al., 2020), Republic of Korea (Han et al., 2020; Kim et al., 2020, 2021; Lee et al., 2018; Maeng et al., 2021; Park, 2022a, 2022b; Park et al., 2020a, 2020b; Park, Jung, & Lee, 2020; Thapa et al., 2020; Yang et al., 2022), China (Li et al., 2019; Zhang et al., 2019; Zhu et al., 2022), United States of America (Duff et al., 2022; Edgar & Bargmann, 2021), Taiwan (Chen et al., 2022; Shyu et al., 2022), Pakistan (Amjad et al., 2019), Canada (Sheehy et al., 2022), Turkey (Cinar & Sihinar, 2020), and Thailand (Jirayucharoensak et al., 2019).
The duration of interventions ranged between <1 day to 4 years, with most providing interventions for 12 weeks (Beentjes, Neal, et al., 2020; Cavallo & Angilletta, 2019; Cinar & Sahiner, 2020; Debring et al., 2021; Duff et al., 2022; Ferry et al., 2020; Kerkhof et al., 2022; König et al., 2022; Laird et al., 2018; Manenti et al., 2020; Park, Liao, et al., 2020; Torpil et al., 2021; Tsolaki et al., 2020; Zhang et al., 2019). Most designs contained two groups such as digital intervention versus control, digital intervention versus non-digital intervention, or cognitively impaired versus healthy adults. Seven articles compared three or more different arms (Cheng et al., 2022; Cinar & Angilletta, 2019; Jirayucharoensak et al., 2019; Manenti et al., 2020; Poptsi et al., 2019; Tsolaki et al., 2020; Yang et al., 2022).
Sample sizes ranged from 1 to 272 participants, with a total 2793 participants providing quantitative data on quality-of-life outcomes. The diagnosis of participants consisted primarily of individuals with mild cognitive impairment (n = 1697). Other diagnoses included individuals with Alzheimer’s disease (n = 21), vascular dementia (n = 98), unspecified or combination of dementias (N = 416), mixed samples of mild cognitive impairment or dementia (n = 463), and probable Alzheimer’s disease (n = 98). Only 17 studies reported age range of participants which ranged from 50 to 101 years, with an average age of 74 years (Beentjes, Neal, et al., 2020; Chen et al., 2022; Debring et al., 2021; Edgar & Bargmann, 2021; Ferry et al., 2020; Flak et al., 2019; Foloppe et al., 2018; Imbeault et al., 2018a, 2018b; König et al., 2022; Laird et al., 2018; Marin et al., 2022; Mattos et al., 2021; Poptsi et al., 2019; Sheehy et al., 2022; Torpil et al., 2021; Zajac-Lamparska et al., 2019). Ethnicity was only reported in nine studies, however, both western and eastern ethnicities were represented (Edgar & Bargmann, 2021; Li et al., 2019; Marin et al., 2022; Nousia et al., 2021; Park, 2022a, 2022b; Rai, Schneider, & Orrell, 2021; Schmitter-Edgecombe et al., 2022; Scullin et al., 2022).
Digital interventions were categorised by their hardware and software. Virtual reality software was present in 21 interventions. These included cognitive training and stimulation (Amjad et al., 2019; Flak et al., 2019; Foloppe et al., 2018; Kim et al., 2021; Maeng et al., 2021; Manenti et al., 2020; Park, Yun, et al., 2020; Park, Liao, et al., 2020; Park, 2022a; Thapa et al., 2020; Torpil et al., 2021; Yang et al., 2022; Zajac-Lamparska et al., 2019; Zhu et al., 2022), leisure and relaxation (Fasilis et al., 2018; Flynn et al., 2022; Cheng et al., 2022; Sheehy et al., 2022; Singh et al., 2022), and for physical exergames (Micarelli et al., 2019; Park, Jung, & Lee, 2020). Computerised software was present in 45 studies which included web pages, applications, smart devices, and computer programs. These consisted of cognitive training or stimulation interventions (n = 23, see Table 1), interventions for improving activities of daily living (Beentjes, Kerkhof, et al., 2020; Beentjes, Neal, et al., 2020; Berret et al., 2022; Imbeault et al., 2018a, 2018b; Kerkhof et al., 2022; König et al., 2022; Schmitter-Edgecombe et al., 2022; Scullin et al., 2022; Smith et al., 2020; Øksnebjerg et al., 2019), physical exergames or exercises (Cinar & Sahiner, 2020; Jirayucharoensak et al., 2019; Petersen et al., 2020; Taylor et al., 2020; Tsolaki et al., 2020; van Stanten et al., 2020), reminiscence opportunities (Bielsten et al., 2020; Critten & Kucirkova, 2019; Ferry et al., 2020; Laird et al., 2018; Ryan et al., 2020), leisure activities (Berenbaum et al., 2020; Hicks et al., 2019), and a communication aid (Debring et al., 2021). Also present was a dementia specific computer (Sautter et al., 2021), and a website providing cognitive behavioural therapy for insomnia (Mattos et al., 2021). Several interventions were explored in multiple studies. These included FindMyApps, an application to assist people to download dementia friendly tablet apps (Beentjes, Kerkhof, et al., 2020; Beentjes, Neal, et al., 2020; Kerkhof et al., 2022), BrainHQ©, a computerised cognitive training website (Duff et al., 2022; Knoefel et al., 2018; Phatak et al., 2021; Tsolaki et al., 2020), iCST, an application for cognitive stimulation (Rai et al., 2021a, 2021b, 2021c), InspireD, a reminiscence application (Laird et al., 2018; Ryan et al., 2020), and Constant Therapy®, a computerised cognitive training website (Edgar & Bargmann, 2021; Marin et al., 2022).
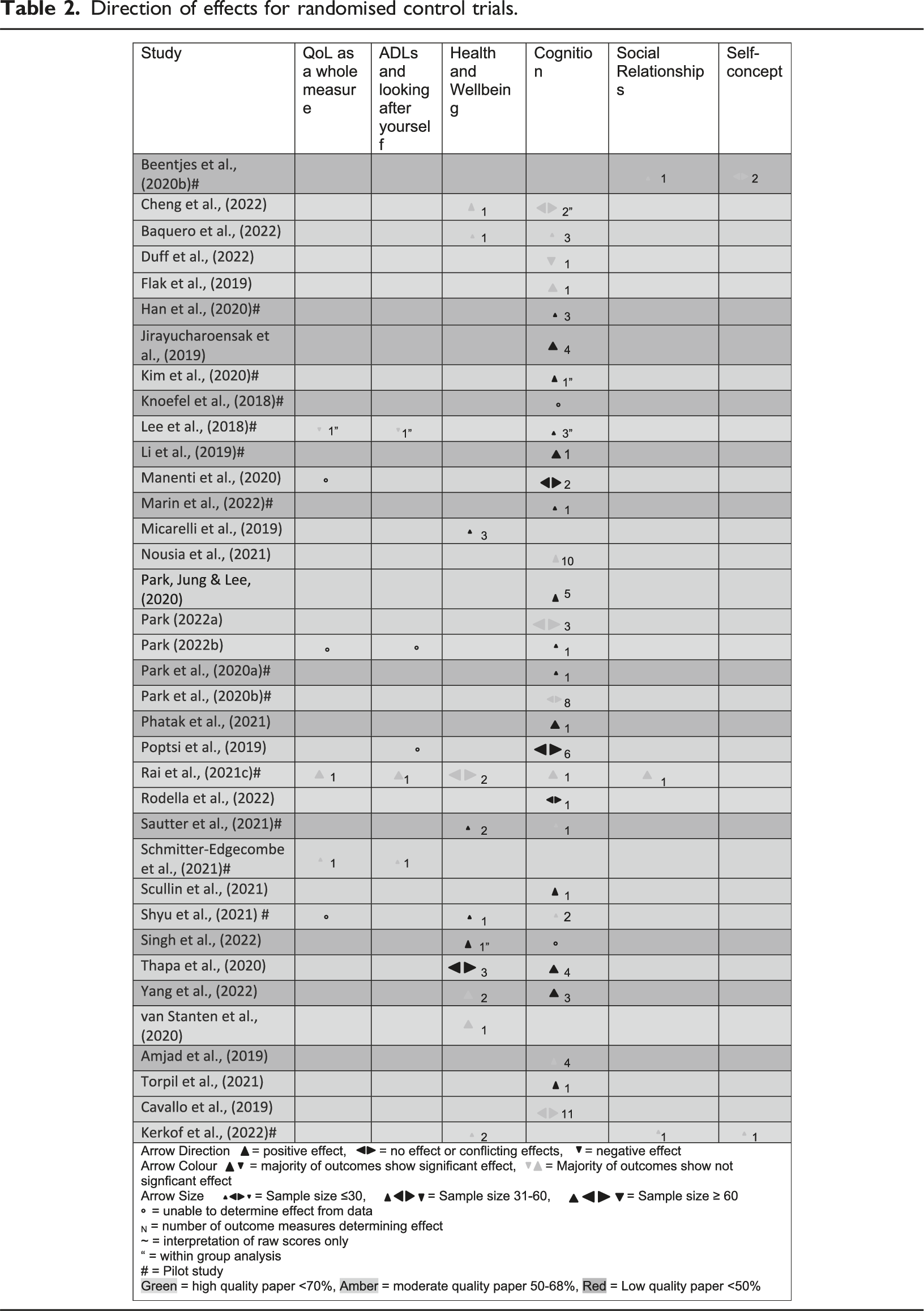
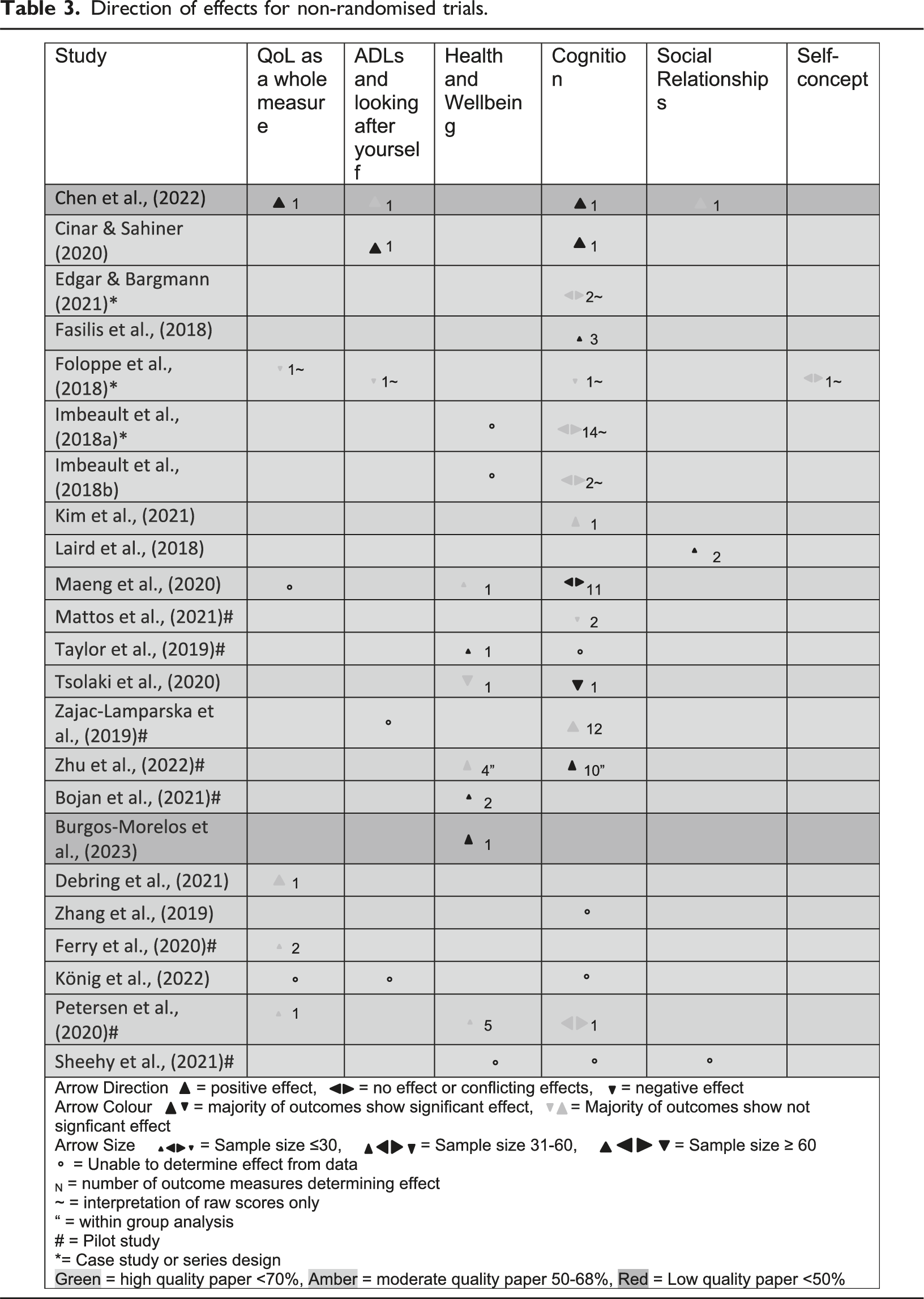
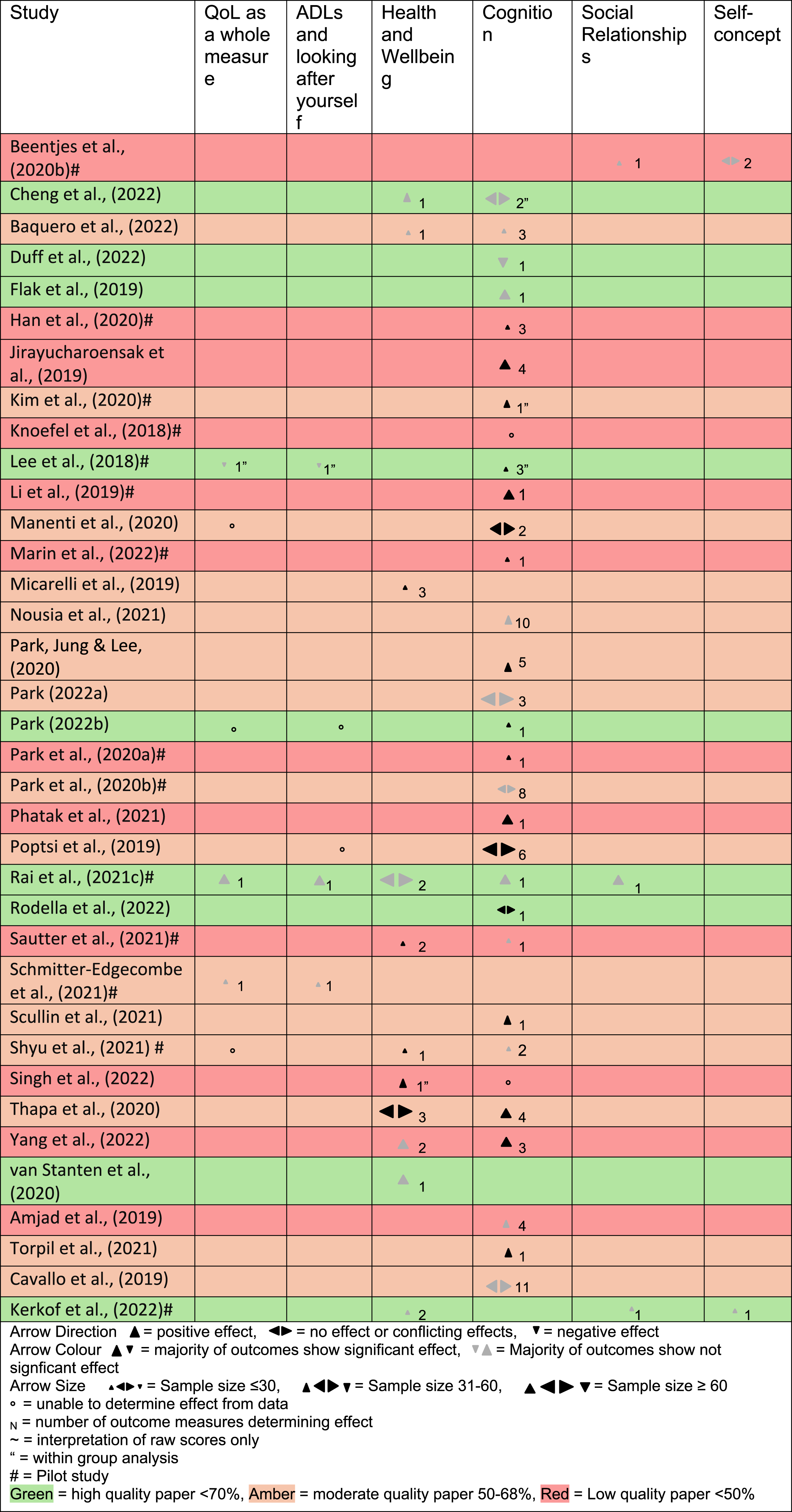
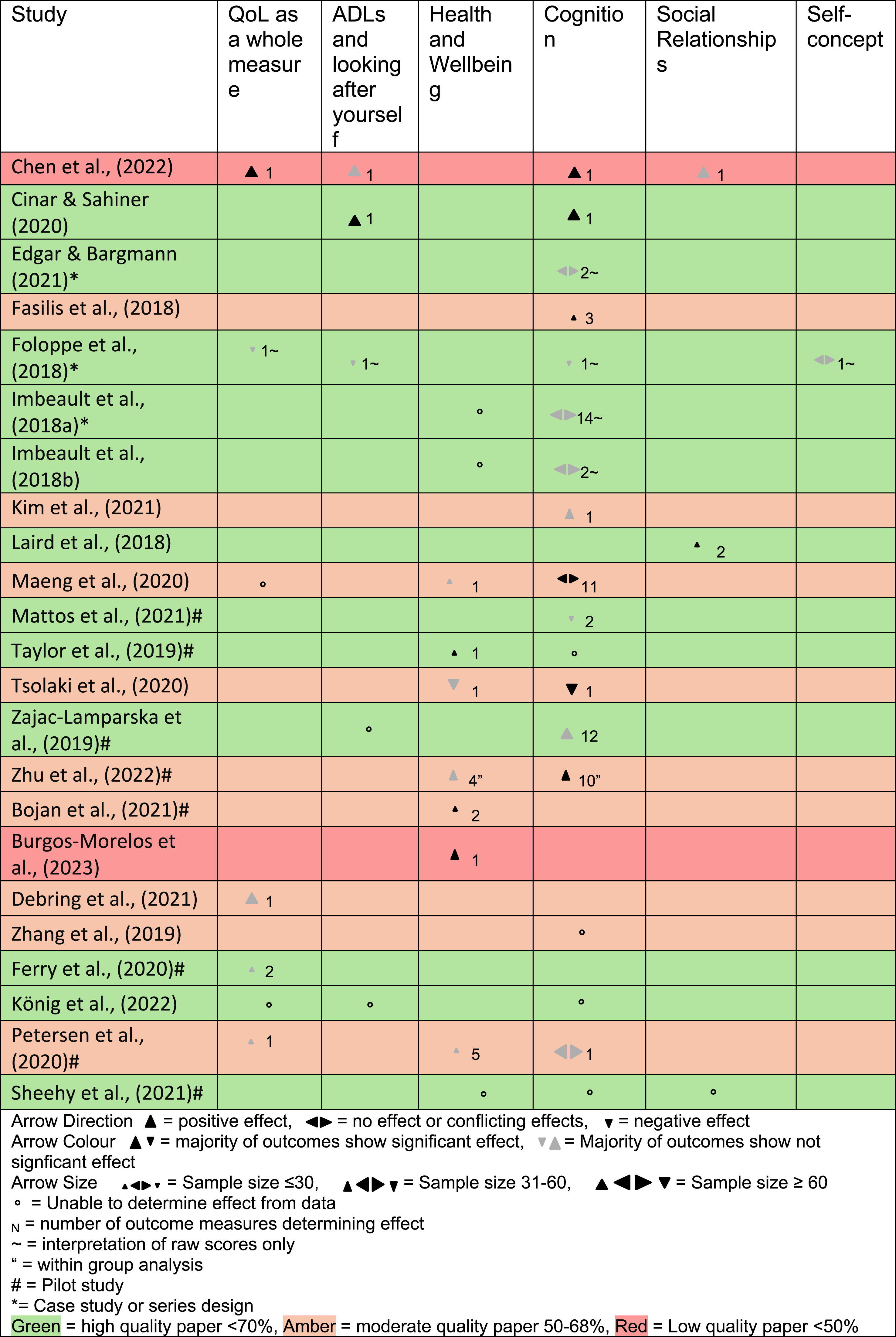
Seventeen articles explored quality of life as a whole measure additional to exploring individual quality-of-life domains (Beentjes, Neal, et al., 2020; Chen et al., 2022; Foloppe et al., 2018; Han et al., 2020; Kerkhof et al., 2022; Kim et al., 2021; König et al., 2022; Maeng et al., 2021; Manenti et al., 2020; Petersen et al., 2020; Rai, Schneider, & Orrell, 2021; Rodella et al., 2022; Schmitter-Edgecombe et al., 2022; Scullin et al., 2022; Shyu et al., 2022; van Stanten et al., 2020), two explored quality-of-life as a whole measure without exploring individual domains (Debring et al., 2021; Ferry et al., 2020). Figure 2 shows the combination of quality-of-life domains explored within articles, and the number of digital methods used by interventions to explore each domain. Cognition was the most explored domain with mostly virtual reality interventions. Twenty articles only explored cognition, thirteen explored cognition and health and wellbeing, five cognition and daily activities and looking after yourself, and five explored all three of these domains. Self-concept and social relationships were least explored, and outcomes related to these appeared in five and seven articles respectively. Measures used to explore quality of life varied (see Table 1). Tables 2 and 3 show the number of outcome measures used in each study and the direction of outcome effects for each quality-of-life domain per study. Venn diagram highlighting the combinations of quality-of-life domains measured in studies, and which digital platforms were used. Direction of effects for randomised control trials. Direction of effects for non-randomised trials.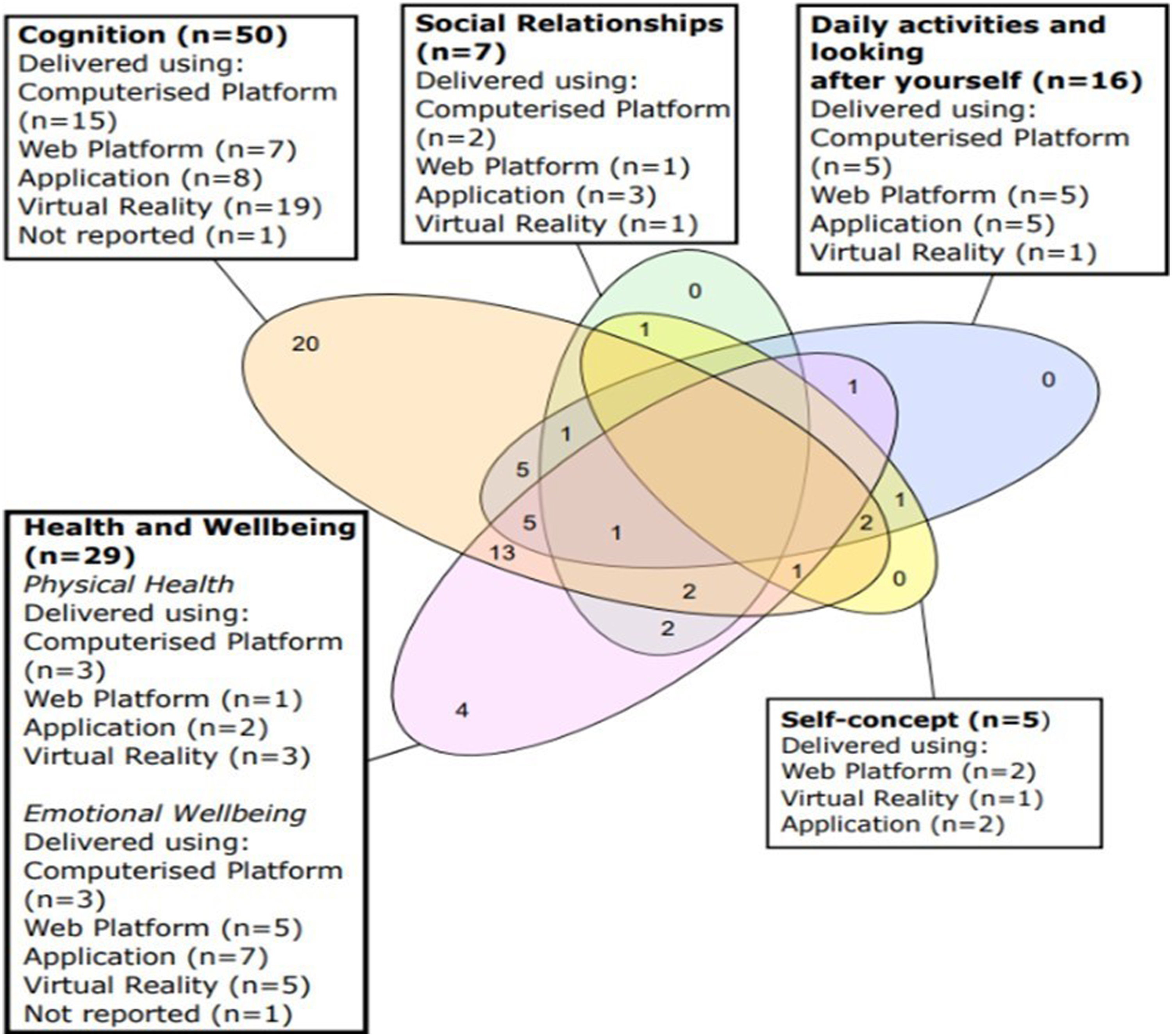
Effectiveness of digital interventions
Direction of effects with sign test statistics per quality-of-life domain.
Cognition
Fifty articles explored cognition, data were included from 43 studies using cognition as the primary outcome or did not specify that it was not the primary outcome (see Tables 2 and 3). One hundred and thirty-eight outcome effects were identified across cognitive domains; however, most did not reach statistical significance. When measured immediately after the intervention period statistically significant positive effects were found in 22 studies (see Tables 2 and 3), and a statistically significant effect favouring the active control group was identified in a study of auditory memory (Duff et al., 2022). This control was an unvalidated digital cognitive training intervention which was compared to a validated version BrainHQ©. In studies with later follow up measures (Diaz Baquero et al., 2022; Cavallo & Angilletta, 2019; Cheng et al., 2022; Duff et al., 2022; Li et al., 2019; Manenti et al., 2020), positive effects remained but were not statistically significant in two studies (Li et al., 2019; Manenti et al., 2020), and negative effects were no longer evident in one study (Duff et al., 2022). Sustained significant effects were found in two RCTs of high and moderate quality (Cavallo & Angilletta, 2019; Cheng et al., 2022). Participants with Parkinson’s disease and MCI received remote transcranial magnetic stimulation (rTMS) alongside virtual reality cognitive training. They showed sustained improvement in delayed memory three months post intervention compared to those receiving rTMS alone, and sustained improvement in delayed memory and total RBANS scores compared to those receiving neither intervention (Cheng et al., 2022). Participants with early-stage Alzheimer’s who received computerised cognitive training using Branier© showed significant improvement in scores on the digit span test, two syllable word test, story recall and delayed recall, and the Brixton test 12 months post intervention compared to individuals receiving unstructured computer use; however, improvements declined compared to immediately after completing the intervention (Cavallo & Angilletta, 2019). The evidence contributing to this synthesis was mostly moderate quality (23%–87%) and mainly RCTs (see supplemental material). Ten studies, including nine of the RCTs, were low quality, lacking details of blinding and concealment, justification of sample size, and clarity regarding reliability of outcome measures (Amjad et al., 2019; Chen et al., 2022; Han et al., 2020; Jirayucharoensak et al., 2019; Li et al., 2019; Marin et al., 2022; Park, Yun, et al., 2020; Phatak et al., 2021; Sautter et al., 2021; Yang et al., 2022). Therefore, the certainty of whether digital interventions can improve cognition is low.
Health and wellbeing
Twenty-nine articles explored health and wellbeing, data were included from 18 using it as the primary outcome or not specifying that it was not the primary outcome (see Tables 2 and 3). Thirty-four outcome effects were identified, and positive effects were found across measures of emotional wellbeing, physical activity, and health. Large effect sizes favouring digital interventions were reported between groups in two studies using the Geriatric Depression Scale (Sautter et al., 2021) and the Pleasant Activities List (Kerkhof et al., 2022); and a small effect size was found using within group analysis on measures of walking abilities (Thapa et al., 2020). However, these didn’t reach statistical significance. Significant improvements immediately post intervention were found using within group analyses in four studies (Bojan et al., 2021; Petersen et al., 2020; Singh et al., 2022; Zhu et al., 2022) and between groups in four studies (Micarelli et al., 2019; Sautter et al., 2021; Shyu et al., 2022; Thapa et al., 2020) using measures of depression, positive and negative affect, stress, mindfulness awareness, walking ability, dexterity, grip strength, dizziness handicap, and balance confidence. 27% of RCT evidence contributing to this synthesis was of low quality (Sautter et al., 2021; Singh et al., 2022; Yang et al., 2022) and causal certainty is low. Quality was low due to unclear blinding, no group concealment, differences between groups at baseline and because groups were not treated identically. Additionally, a significant effect favouring the physical training control group was found on depressive symptoms in one non-randomised control trial of moderate quality (Tsolaki et al., 2020). This intervention was not digital, and therefore questions are raised as to whether a digital method of delivery is more effective than in person. Given the low quality of this evidence and conflicting findings, the certainty regarding whether digital interventions improve health and wellbeing is low.
Social relationships
Seven studies explored social relationships, data were included from five measuring social relationships as the primary outcome or not specifying that it was not the primary outcome (see Tables 2 and 3). Six outcome effects were identified showing positive effects in mutuality (positive quality of relationship between carer and care recipient), and social participation. Most did not reach statistical significance, except two using the Personal and Social Performance Scale, Quality of Carer Patient Relationship scale, and Mutuality scale (Chen et al., 2022; Laird et al., 2018). Both used within group analysis measured pre and post intervention, neither had a control group or further follow up, thus the certainty regarding whether digital interventions caused this effect and whether this was sustained is low. Although the quality of studies contributing to this synthesis was mostly high (Kerkhof et al., 2022; Laird et al., 2018; Rai, Schneider, & Orrell, 2021) two were low quality (Beentjes, Neal, et al., 2020; Chen et al., 2022). Most were non-randomised control designs (80%), and only one compared the intervention to a no treatment control group (Rai, Schneider, & Orrell, 2021). Quality was commonly reduced due to lack of detail on randomisation, concealment, blinding processes, and difficulty determining whether both groups were treated identically. Thus, it is difficult to determine whether improvements were the result of digital interventions, or confounding variables and therefore the certainty of this finding is low.
Qualitative synthesis
Study characteristics
Study designs consisted of mixed methods (Beentjes, Kerkhof, et al., 2020; Beishon et al., 2021; Berenbaum et al., 2020; Bogza et al., 2020; Kerkhof et al., 2022; König et al., 2022; Mattos et al., 2021; Rai et al., 2021a, 2021b; Sheehy et al., 2022) and qualitative papers (Berrett et al., 2022; Bielsten et al., 2020; Critten & Kucirkova, 2019; Flynn et al., 2022; Hicks et al., 2019; Ryan et al., 2020; Smith et al., 2020; Øksnebjerg et al., 2019). Five articles described their methods as aligning with participatory action research (Beentjes, Neal, et al., 2020; Berenbaum et al., 2020; Critten & Kucirkova, 2019; Flynn et al., 2022; Hicks and Innes, 2019). Four articles did not report their location (Beishon et al., 2021; Flynn et al., 2022; Mattos et al., 2021; Smith et al., 2020), the rest were in Europe (Beentjes, Kerkhof, et al., 2020; Bielsten et al., 2020; Critten & Kucirkova, 2019; Hicks et al., 2019; Kerkhof et al., 2022; König et al., 2022; Rai, Griffiths, et al., 2021; Ryan et al., 2020; Øksnebjerg et al., 2019), Israel (Berenbaum et al., 2020), Australia (Berrett et al., 2022), and Canada (Sheehy et al., 2022). The duration of interventions ranged between <1 day to 18 months, with most lasting 12 weeks.
Evidence from 295 participants was included in the qualitative synthesis comprising of data from individuals with unspecified, or combined dementia diagnoses (n = 184), mild cognitive impairment (n = 44), and individuals with dementia or mild cognitive impairment (n = 67). In some cases, family members supporting the person living with dementia to use the digital intervention were included in the synthesis when interviewed with the person living with dementia. The participants ages were reported in 13 studies, ranging between 41–97 years, the mean age was 74 years (Beentjes, Kerkhof, et al., 2020; Beilsten et al., 2021; Berenbaum et al., 2020; Bogza et al., 2020; Critten & Kucirkova, 2019; Flynn et al., 2022; Hicks et al., 2019; König et al., 2022; Mattos et al., 2021; Ryan et al., 2020; Sheehy et al., 2022; Smith et al., 2020; Øksnebjerg et al., 2019). Seven studies documented ethnicity, representing eastern and western ethnicities (Beishon et al., 2021; Berenbaum et al., 2020; Bogza et al., 2020; Hicks et al., 2019; Rai et al., 2021a, 2021b; Øksnebjerg et al., 2019).
Digital interventions were categorised by their software and hardware. Several studies used various ‘off the shelf’ devices (Berrett et al., 2022; Hicks et al., 2019; Øksnebjerg et al., 2019; Smith et al., 2020). Two digital interventions were described within multiple studies: FindMyApps (Beentjes, Kerkhof, et al., 2020; Kerkhof et al., 2022), an application to assist people to download dementia friendly tablet apps, and iCST (Rai et al., 2021a, 2021b), an individual cognitive stimulation application. Other digital interventions were categorised as computerised cognitive training (Beishon et al., 2021; Berenbaum et al., 2020), virtual reality games (Sheehy et al., 2022) and virtual reality experiences (Flynn et al., 2022), assistive technologies (König et al., 2022), reminiscence apps (Critten & Kucirkova, 2019), self-management apps (Bielsten et al., 2020), a web-based decision-making tool (Bogza et al., 2020), and online cognitive behavioural therapy for insomnia (Mattos et al., 2021).
In general, data were from interviews, focus groups, and observations, and analysed using thematic analysis (61%) to produce themes summarising participants experiences supplemented by participant quotes. All articles gathered data from carers and people living with dementia except one observational study (Smith et al., 2020) which only gathered data from people living with dementia. Most (61%) used dyadic interviews or focus groups, two conducted separate interviews but combined data during analyses (Flynn et al., 2022; Ryan et al., 2020). It was unclear how data were collected in three articles; however, carer and participant data were analysed together (Beentjes, Kerkhof, et al., 2020; Berenbaum et al., 2020; Konig et al., 2022).
Experiences of using digital interventions
Meta-aggregation of qualitative findings.
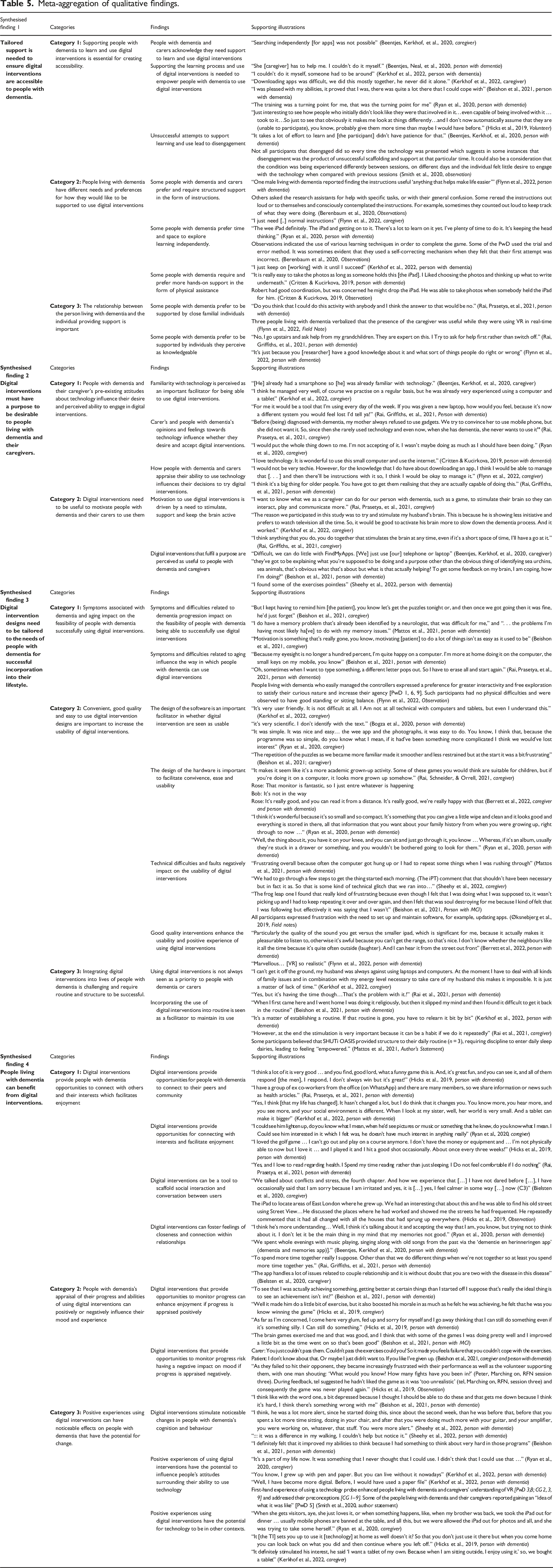
Synthesised finding 1: Tailored support is needed to ensure digital interventions are accessible to people living with dementia
People living with dementia and their caregivers acknowledge that support to learn and use digital interventions is crucial to empower them (Beentjes, Kerkhof, et al., 2020; Beishon et al., 2021; Hicks et al., 2019; Kerkhof et al., 2022; Ryan et al., 2020), and if not supported, this can lead to disengagement (Beentjes, Neal, et al., 2020; Smith et al., 2020). Support must be tailored to the needs and preferences of people living with dementia, who differ in how they would like to be supported, and who they would like to be supported by. Some prefer to be supported by family (Flynn et al., 2022; Rai et al., 2012b), and others by individuals they feel are knowledgeable about technology (Flynn et al., 2022; Rai et al., 2012a). The level of support ranged from independent exploration (Berehaum et al., 2020; Kerkhof et al., 2022; Ryan et al., 2020), providing instructions (Berenhaum et al., 2020; Flynn et al., 2022), to verbal or physical assistance such as holding devices, or physically guiding participants around devices (Critten & Kucirkova, 2019).
Synthesised finding 2: Digital interventions must have a purpose to be desirable to people living with dementia and their caregivers
People living with dementia and their caregivers have pre-existing attitudes towards technology which influence the desirability of using digital interventions. Lack of familiarity with technology (Beentjes, Kerkhof, et al., 2020; Kerkhof et al., 2022; Rai, Griffiths, et al., 2021), negative opinions (Critten & Kucirkova, 2019; Rai, Prasetya, et al., 2021; Ryan et al., 2020) and low skill appraisal (Flynn et al., 2022; Rai, Griffiths, et al., 2021) make digital interventions less desirable. To improve desirability, digital interventions need a purpose to be seen as useful (Beentjes, Kerkhof, et al., 2020; Beishon et al., 2021; Sheehy et al., 2022). Caregivers' desires to stimulate, support, and keep the brain active are powerful purposes for initiating use of digital interventions (Kerkhof et al., 2022; Rai et al., 2021a, 2021b). However, people with dementia also need to find the intervention useful for it to be maintained (Beentjes, Neal, et al., 2020; Beishon et al., 2021; Sheehy et al., 2022).
Synthesised finding 3: Digital intervention designs must be tailored to the needs of people living with dementia for successful incorporation into their lifestyle
Symptoms such as apathy and memory difficulties, associated with dementia progression make individuals less likely to, or less able to use digital interventions (Beishon et al., 2021; Mattos et al., 2021). Deterioration of eyesight and physical abilities, associated with normal aging also make digital interventions more difficult to use (Beishon et al., 2021; Flynn et al., 2022; Rai, Prasetya, et al., 2021). There appeared two ways of mitigating these difficulties.
Firstly, designs prioritising simplicity (Beishon et al., 2021; Bogza et al., 2020; Kerkhof et al., 2022; Ryan et al., 2020) and convenience were deemed more usable, and less stigmatising (Berrett et al., 2022; Rai, Griffiths, et al., 2021; Ryan et al., 2020). Additionally, good quality enhanced intervention appeal (Berrett et al., 2022; Flynn et al., 2022). Those that require multiple updates are deemed less usable because they produce technical difficulties making participants frustrated and disengaged (Beishon et al., 2021; Mattos et al., 2021; Sheehy et al., 2022; Øksnebjerg et al., 2019). Difficulties are mitigated when intervention use is successfully incorporated into the routines of people living with dementia (Beishon et al., 2021; Kerkhof et al., 2022; Mattos et al., 2021; Rai, Griffiths, et al., 2021). This is acknowledged as challenging and not always a priority (Kerkhof et al., 2022; Rai, Prasetya, et al., 2021).
Synthesised finding 4: People living with dementia can benefit from digital interventions
Digital interventions provide opportunities for connectedness. Their use can scaffold social interaction, stimulate conversations (Bielsten et al., 2020; Hicks et al., 2019), and connect people living with dementia to their peers and community (Hicks et al., 2019; Kerkhof et al., 2022; Rai, Prasetya, et al., 2021). When used with family, digital interventions can foster feelings of closeness (Beentjes, Kerkhof, et al., 2020; Bielsten et al., 2020; Rai, Griffiths, et al., 2021; Ryan et al., 2020). Digital interventions focusing on leisure provide opportunities to connect with hobbies and interests, creating feelings of enjoyment (Hicks et al., 2019; Rai, Prasetya, et al., 2021; Ryan et al., 2020). However, enjoyment depends on how ability and progress is appraised during use. When people appraise their progress and ability as positive, this produces feelings of achievement (Beishon et al., 2021; Hicks et al., 2019), whereas poor progress leads to frustration and disengagement (Beishon et al., 2021; Hicks et al., 2019).
For some, noticeable changes in cognition and behaviour reinforce positive experiences of use (Beishon et al., 2021; Sheehy et al., 2022). Appraising digital interventions as a positive experience has the potential to improve people’s perception of their technology skills (Kerkhof et al., 2022; Ryan et al., 2020; Smith et al., 2020), and empower people to use technology in different settings and for different purposes (Hicks et al., 2019; Ryan et al., 2020).
Integration of quantitative and qualitative syntheses
The integration of evidence reveals how people living with dementia can benefit from using digital interventions and how delivery might be optimised (Figure 3). Integration of evidence summarising benefits of using digital interventions and how these benefits might be achieved.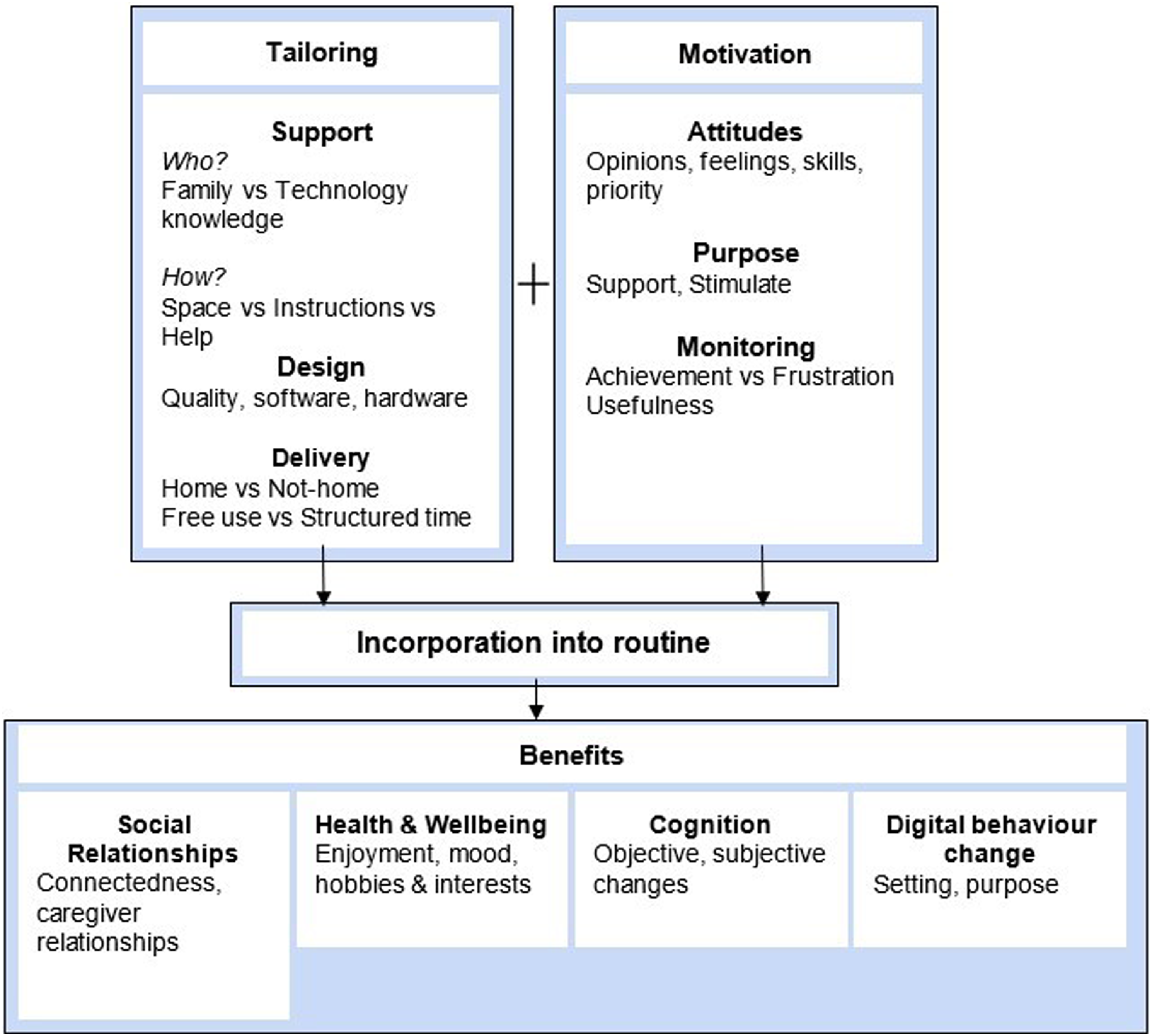
Benefits to digital intervention use
Benefits were identified qualitatively and quantitatively in social relationships, health and wellbeing, and cognition. Additionally, changing where and with whom people living with dementia used digital technologies was identified in the qualitative synthesis.
Socially, digital interventions contribute to social interaction and integration by scaffolding conversation and connecting people living with dementia to their peers and community (Bielsten et al., 2020; Hicks et al., 2019; Rai, Griffiths, et al., 2021; Smith et al., 2020). Collaborative use was described as fostering feelings of closeness (Beentjes, Neal, et al., 2020; Bielsten et al., 2020; Rai, Griffiths, et al., 2021; Ryan et al., 2020), shown in the quantitative data as improvements in measures of caregiver relationships and mutuality (Chen et al., 2022; Laird et al., 2018).
Interestingly, leisure was rarely a focus for interventions, yet enjoyment was commonly described qualitatively as a benefit (Flynn et al., 2022; Hicks et al., 2019; Rai, Prasetya, et al., 2021; Ryan et al., 2020; Sheehy et al., 2022). Quantitatively, improvements were seen on measures of mood and positive affect indicating enjoyment (Kerkhof et al., 2022; Sautter et al., 2021; Shyu et al., 2022).
Changes in physical activity, alertness, and cognition are described qualitatively (Beishon et al., 2021; Flynn et al., 2022; Sheehy et al., 2022). These are consistent with improvements on quantitative measures of physical activity and cognitive tests following the intervention (Micarelli et al., 2019; Petersen et al., 2020; Thapa et al., 2020).
Changes to how people used digital technologies involves people feeling more motivated to use the technologies outside of the research context. These individuals used the interventions and other technologies for new purposes in different locations after taking part in studies Hicks et al. (2019); Kerkhof et al. (2022); Ryan et al. (2020). This was not featured in quantitative papers, as it’s not a variable measured numerically but indicates that positive experiences might contribute to making future interventions and technologies more desirable.
Optimising digital intervention delivery
A lack of reporting on how digital interventions were provided to participants means it is difficult to conclude the most effective way of providing digital interventions. For example, 39% of quantitative articles did not report either the location of intervention use, the method of intervention delivery, or the level of support given to use the intervention. From available information, structured digital interventions (those requiring a specified amount of use per day/week) provided at home more frequently produce positive effects. These interventions made up 29% of studies reporting location and requirements of intervention use, of which 73% demonstrated positive outcomes. Additionally, evidence from one qualitative study describes home-based digital interventions as more desirable because participants did not have to go out (Ryan et al., 2020). Further qualitative evidence suggests incorporation into routine is key to counteract barriers related to memory difficulties (Beishon et al., 2021; Kerkhof et al., 2022; Mattos et al., 2021; Rai, Schneider, & Orrell, 2021). Therefore, interventions with structured requirements for use, provided in the home environment may be more easily incorporated into routines because they are more convenient. This is important as people living with dementia require support to learn and use interventions (Beentjes, Kerkhof, et al., 2020; Critten & Kucirkova, 2019; Flynn et al., 2022; Kerkhof et al., 2022; Rai, Griffiths, et al., 2021), often provided by carer’s (Beishon et al., 2021; Flynn et al., 2022; Kerkhof et al., 2022), and therefore, the convenience of having interventions in the home may mediate instances where they are not seen as a priority because they require less time and effort.
Discussion
People living with dementia or mild cognitive impairment benefit from digital interventions, particularly those targeting cognition, health and wellbeing, and social relationships. Other benefits include enjoyment from intervention use and continuing to use technologies outside of the research parameters.
To gain benefits, individuals need to be motivated, otherwise interventions are not seen as a priority and forgotten. Motivation often comes from carers who describe a need to stimulate and support, but motivation is maintained when people living with dementia feel the intervention is useful.
People living with dementia require support to use digital interventions, which often comes from carers or people knowledgeable about technology. Also, interventions used at home which have specified requirements to how long they are used per day/week may be more likely to produce beneficial outcomes. The frequency and intensity of intervention use does not improve quantitative outcomes, and so this delivery method is likely effective because it provides a convenient and flexible way to incorporate interventions into routines.
The benefits of using digital interventions found in this review are consistent with previous reviews exploring effectiveness of specific interventions. For example, touchscreen technologies and digital cognitive training improved the psychological wellbeing, cognition, social interaction, and relationships of people living with dementia (Hill et al., 2017; Pang et al., 2021; Tyack & Camic, 2017). Qualitative reviews corroborate this, evidencing benefits in the physical, mental, and social health of people with dementia using mobile health applications (Brown & O'Connor, 2020). Despite this, we cannot conclude with certainty that digital interventions are effective in improving cognition, health and wellbeing, and social interaction. This is because in depth statistical comparisons were impossible due to there being huge variation in how quality of life was conceptualised by authors, and how outcomes were measured. Additionally, the general quality of available quantitative evidence was inconsistent and low further reducing the certainty of benefits. This is important given that most included studies also only explored short term benefits, and thus it also cannot be concluded that the benefits that were identified are sustained. Similar uncertainty is acknowledged elsewhere, where low quality evidence, small sample sizes, and inconsistencies between technologies and designs mean that other reviews have also failed to provide convincing evidence of digital intervention effectiveness (Gates et al., 2019; Knapp et al., 2022; Topo, 2009; Van der Roest et al., 2017).
The qualitative review findings are largely consistent with theoretical models of adaption, specifically the environment-person fit (E-P fit) model’s notion that a good fit between a person’s competencies and environment is required for digital interventions to be desirable, accessible, and useful (Lawton & Nahemow, 1973). For example, our findings show that declines in cognition and poor skill appraisal reduce technology competence, leading to poor E-P fit, and non-adoption of digital interventions. According to our findings one method to improve this fit is by providing support. There is much evidence consistent with our finding that people living with dementia require support to use digital interventions (Evans et al., 2022; Gibson et al., 2015; Lariviere et al., 2021; Smith and Mountain, 2012). Previous frameworks have, like this review, identified that support comes from carers, or people knowledgeable regarding technology (Evans et al., 2022); without support this review found participants were likely to disengage.
The qualitative review findings are also consistent with the concepts described in the unified theory of acceptance technology (UTAUT) (Marikyan & Papagiannidis, 2023). This theory may explain our two novel findings. Firstly, we found that positive experiences using digital interventions resulted in participants using the technologies outside of the study parameters, such as with different people or in different settings (Hicks et al., 2019; Kerkhof et al., 2022; Ryan et al., 2020). Older adult literature describes gaining knowledge as influential for older adult technology use (Nygard & Starkhammar, 2007). For example, digital inclusion classes indicate that individuals learning to use technology show desire to learn about other technologies and this level of desire was mediated by positive experiences, with positive experiences being associated with a desire to learn new technologies (Betts et al., 2019). Aligning with the UTAUT (Marikyan & Papagiannidis, 2023), this is likely because gaining knowledge through classes improves performance expectance (predicted usefulness) and effort expectance (ease of use). In view of this, it is possible that a similar process is established through taking part in digital intervention research. This means that by learning technology skills through research experiences, people with dementia might adapt better to technology environments outside of study parameters.
Secondly, the review found that interventions provided at home, requiring structured frequency of use, were more likely to produce benefits. Like us, Pang and colleagues’ (2021) found no differences in effectiveness outcomes based on intervention length or intensity, suggesting that the delivery method is important for other reasons. Based on the E-P fit model and UTAT (Lawton & Nahemow, 1973; Marikyan & Papagiannidis, 2023) this method of delivery may be effective because it reduces environmental pressures by facilitating a convenient way to incorporate interventions into routines, a common strategy to aid memory (Cavanaugh et al., 1983; Ferland et al., 2013; White, 2023). Like others, we found carers were a key factor in this incorporation (Evans et al., 2022; Gibson et al., 2015; Lariviere et al., 2021; Smith and Mountain, 2012). Therefore, it is possible that barriers such as being too busy or interventions being too time consuming (Brown & O'Connor, 2020; McAllister et al., 2020), might be mitigated by home-based interventions which are more convenient to carer’s (Christie et al., 2018) because these reduce added burden (Arthanat et al., 2020).
Limitations
Several limitations are applicable to this review, firstly many different study designs and outcomes were included meaning effectiveness was determined by vote counting the direction of effect (McKenzie et al., 2023). This is acceptable in Cochrane guidance (McKenzie et al., 2023) but limited because it can only determine the presence of an effect, not the magnitude.
Secondly, this review includes samples of people living with dementia, mild cognitive impairment, and probable Alzheimer’s disease because many studies used mixed samples, thus, to avoid excluding data, all are included. Therefore, findings may be more applicable to individuals in the prodromal or milder stages of dementia, as a larger proportion of the review sample fit this category. Previous literature shows digital technologies may be more beneficial to individuals with mild cognitive impairment than people living with dementia (Neal et al., 2021), which might explain the positive effects found. The findings on effectiveness should therefore be applied to other stages of dementia with caution.
Thirdly, most studies in this review explored digital intervention effects at the end of the intervention period, thus describing short-term benefits. Long term benefits have rarely been explored however, one review showed benefits of engaging in digital interventions were not evident at 12 months (Gates et al., 2020). Therefore, the longer-term sustainability of digital interventions is unknown.
Finally, poor methodological reporting means 20% of studies were of low quality thus, findings are low in certainty. The addition of qualitative data to the effectiveness synthesis adds some certainty, however, the trustworthiness of qualitative data is not graded. This lack of consistent high-quality evidence is not uncommon among reviews exploring digital technologies (Neal et al., 2021; Van der Roest et al., 2017), however, findings should be interpreted with risks of bias in mind because we cannot conclude with certainty that effectiveness of digital interventions is established.
Implications and recommendations
Digital interventions in dementia are popular reflected by the large proportion of pilot studies identified. Despite this, this review demonstrates little progress has been made making these real-world applicable, potentially due to researchers’ enthusiasm to invent rather than provide good quality evidence of effectiveness (Knapp et al., 2022). Previous reviews have also not provided convincing evidence because of the many varieties of technology and design being produced (Topo, 2009; Van der Roest et al., 2017). For example, this review describes 28 types of digital cognitive training programmes, despite well established, trademarked versions being available for testing (Kong, 2020). Although 29 of these were RCTs, only 32% were deemed high quality; many were feasibility stage, thus unready for large scale effectiveness testing and not real-world applicable. Further high-quality, large-scale research is needed to determine whether digital interventions are effective.
This review provides a summary of interventions already developed mapped on to the quality-of life domains they target. Consistent with others, the results show developments have mostly focused on improving cognition (Dequanter et al., 2021), however given that the quantitative benefits here remain inconclusive, alternative outcomes should be explored. Personal outcomes such as social relationships and self-concept remain underexplored (Neal et al., 2021). Compared to previous reviews, progress has been made developing digital reminiscence opportunities for community dwelling people living with dementia, which often target social relationships (Laird et al., 2018; Ryan et al., 2020). However, a lack of interventions focusing on leisure persists (Dequanter et al., 2021). This is surprising considering that over 65s spend approximately 7 hours a day on leisure activities (Payne, 2017), report a need for entertainment from technology (Egan & Pot, 2016), and report enjoyment using technology (Astell, 2013; Chirico et al., 2022; Lee et al., 2023). Leisure focused digital interventions do exist for people with dementia (Astell, 2019) but older adults tend to have negative attitudes towards gaming (Ferguson et al., 2016). Qualitatively, this review highlights evidence that pleasure can be derived from digital interventions, even when enjoyment is not their primary focus (Hicks et al., 2019; Rai, Prasetya, et al., 2021; Ryan et al., 2020) and therefore leisure-based technologies and making these more appealing to people with dementia requires further exploration.
This review also highlights the importance of creating personalised or tailored digital interventions for people with dementia so that they are desirable and accessible. General attitudes toward technology, which are underexplored, form part of this influence. Individuals with negative attitudes appear less motivated and less likely to engage and this is well documented as a barrier to digital intervention engagement (Christie et al., 2018; Pang et al., 2021; Smith & Mountain, 2012). Study recruitment for effectiveness testing is thus unavoidably biased, as individuals with positive attitudes, and motivation are more likely to take part in technology studies, unrepresentative of all people living with dementia. Echoing Holthe and colleagues (2018), future research should prioritise using participatory methods of intervention development, to better understand people’s attitudes towards technology and create interventions which are more desirable and accessible to all people with dementia. Also, given the importance of carer’s for supporting people with dementia to use digital interventions, like Bradley and colleagues (2023) we recommend that they too are considered when designing interventions.
Conclusion
This review synthesised studies exploring effectiveness and experiences of people living with dementia or mild cognitive impairment using digital interventions to improve their quality of life. This shows people living with dementia can benefit from using digital interventions if they are motivated, and if delivery is tailored and supported. Delivery might be optimised by providing interventions at home using structured time and frequency instructions because this allows easier integration into lifestyles.
Supplemental Material
Supplemental Material - Exploring the effectiveness and experiences of people living with dementia interacting with digital interventions: A mixed methods systematic review
Supplemental Material for Exploring the effectiveness and experiences of people living with dementia interacting with digital interventions: A mixed methods systematic review by Annabel Ditton, Hissah Aloda, Christopher Fox, Shirley Evans, and Jane Cross in Dementia
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Exeter.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.