
Abstract
Earlier diagnosis and longer working careers is resulting in more individuals being identified as having Mild Cognitive Impairment or Early Onset Dementia (MCI/EOD) when they are still in the workforce. While there is growing interest in the dementia research community and beyond to develop technologies to support people with dementia, the use of technology for and by people with MCI/EOD in the workplace has had very little attention. This paper presents a two-part study involving interviews and participatory sessions to begin to understand the workplace experiences and the role of technology among people living with MCI/EOD. We present our findings from working with seven people with MCI/EOD and two care partners to explore technology design. Our results indicate several similarities as well as a few differences between MCI/EOD and later-onset dementia with respect to challenges using technology and design considerations for supporting engagement and use of technology. Lessons learned through the process of working with people with MCI/EOD through participatory methods is presented along with recommendations to foster an inclusive, respectful, and empowering experience for participants with MCI/EOD.
Introduction
Being employed is often far more important than a means to earn a wage; it can provide a sense of productivity and worth, membership in a group, and the opportunity to contribute to society (Waddell & Burton, 2006). Many people dedicate significant time, effort, and passion to their vocation, which makes this a valued aspect of their personhood. Changes in a person’s abilities, such as changes in cognition caused by dementia, can profoundly impact a person’s ability to engage in employment.
Dementia is an umbrella term for progressive, irreversible neurological disorders involving a decline in cognitive functioning (Chambers et al.,2016). There are currently an estimated 50 million people living with dementia globally, and that number is predicted to rise to 152 million by 2050 (Australia et al.,2019). Dementia is a public health priority that significantly impacts the directly affected persons, their families, and the health care system (Winblad et al.,2016). The incidence of dementia increases with age; the term “early-onset dementia (EOD)” is often used when there is a dementia diagnosis below the age of 65.
“Mild cognitive impairment (MCI)” is the diagnosis used when there is evidence of modest cognitive decline from a previous level of performance in one or more cognitive domains (i.e., complex attention, executive function, learning and memory, language, perceptual-motor, or social cognition) based on: (a) Concern of the individual, a knowledgeable informant, or the clinician that there has been a mild decline in cognitive function; and (b) A modest impairment in cognitive performance, preferably documented by standardized neuropsychological testing or, in its absence, another quantified clinical assessment (Sachdev et al.,2014). MCI can (but does not always) progress to dementia and can interfere with work performance. This paper uses the blended term “MCI/EOD” to describe people living with cognitive deficits due to suspected MCI or dementia, persons with clinically diagnosed dementia, and persons with clinically diagnosed MCI; however, we recognize that MCI and EOD are not the same and have differences that can impact everyday activities differently.
Dementia is normally associated with the post- retirement period of life, but with the current global trend toward later retirement ages and earlier diagnosis, dementia is becoming and is expected to become still more common in the workplace (Evans, 2019). While the topic is of increasing importance, little is known about what happens when someone who is employed develops MCI/EOD (Evans, 2019), nor how technology might play a role in supporting related changes (Shastri, 2019).
To the authors’ knowledge, there are no systematic methods to create technologies that support MCI/EOD in the workplace or to gain an understanding of related design considerations. The purpose of this research is to explore how to capture the working experiences of people with MCI/EOD to provide insights about how technology is used as well as what would be beneficial in technology designed to support people living with MCI/EOD. The research questions guiding this paper are 1. What are the experiences of people with MCI/EOD with technology in the workplace? 2. How can people with MCI/EOD be involved in designing new technologies to support workplace engagement?
This paper will cover two parts—semi-structured interviews and participatory workshops with people with MCI/EOD to answer the aforementioned research questions.
Related literature
Our literature review was unable to find literature that specifically focuses on designing technology with or for people with MCI/EOD in the workplace context; hence, we take a broader perspective that focuses on building upon existing strategies for adapting design methods for people with dementia. In this section, we present research around the experiences of people with MCI/EOD at work and related technology research in dementia to provide an overview of different related approaches. The reader will note references from the field of human-computer interaction (HCI). This is because HCI research is increasingly exploring inclusivity and accessibility in the design and development of new technologies (e.g., interfaces, systems, services, and tools) for people of all abilities.
MCI/EOD at workplace
According to Harris (2004), most people below the age of 65 living with EOD are employed when symptoms related to their condition emerge. MCI/EOD symptoms are often first noticed as difficulties in the workplace because most work-related tasks have cognitive-related elements that are impacted by symptoms, such as changes in memory, information processing, learning, communication, and visuo-spatial perception abilities (Prince, 2015; Ritchie et al.,2015; Rosenberg & Lyketsos, 2008; WHO, 2017).
People diagnosed with dementia under the age of 65 are a minority of cases compared to later-onset (i.e., over 65) and have different considerations. These include being relatively physically healthy and having different goals and responsibilities in their day-to-day lives (Lambert et al.,2014; Ritchie et al.,2018). As such, people with MCI/EOD have to come to terms with a diagnosis most commonly associated with later life. Moreover, most resources and approaches for supporting dementia are targeted toward later-onset and do not always map to early-onset (Bell & Leong, 2019). These factors combine to make MCI/EOD a unique and growing population, that requires targeted research and appropriate support.
While existing literature advocates for the critical role of employers in supporting people with MCI/EOD (Chaplin & Davidson, 2016; Ohman et al., 2001), there is a very little research focusing on understanding the experiences and challenges these individuals face in the workplace. Initial insights from Chaplin & Davidson (2016) suggest that employers often lack knowledge that would enable them to support someone with MCI/EOD in the workplace, such as failing to provide adequate adjustments, making decisions that cause further distress on the job (e.g., requiring additional training) or terminating the person’s job.
Technology for supporting dementia
Individuals who develop MCI/EOD experience varying degrees of cognitive decline. A study in 2010 showed technology (e.g., modifications to workstation, new computer/IT) and policy-based solutions (e.g., changes to work schedule, work from home, and restructuring job) as the ones that are most commonly used to provide work-place accommodations for people with disabilities (Meera Adya et al.,2010). For people with dementia to leverage technology more effectively, Bell & Leong (2019) suggest it is better to introduce technologies in the earlier stages of dementia at younger ages, when the memory and learning abilities of people still benefit their technology use. In turn, understanding how to involve individuals with MCI/EOD in research is becoming a research topic of itself (Astell et al., 2009a, 2009b; Lazar et al.,2017).
Related approaches for participatory research
Participatory design can be defined as a process where participants in the process typically have two principal roles: designers and users. Designers strive to learn the realities of the users’ situation while users strive to articulate their desired aims and learn appropriate technological means to obtain them (Simonsen & Robertson, 2012). Engaging participants in context (i.e., in their environment) is a crucial first step in many technology creation projects, particularly in accessibility and aging research (Dee & Hanson, 2016). Participatory design focuses on participants being involved in the design of new products and devices and is known to improve the usability and impact of interactive systems (Brankaert et al., 2019). Participatory design techniques have been used successfully with people with dementia (Hanson et al., 2007; Hawkey et al., 2005; Robinson et al.,2009; Savitch & Zaphiris, 2004).
To our knowledge, the only documented study that explores the involvement of people with EOD with participatory or HCI research is the work of Bell & Leong, (2019), who engaged people with EOD as “co-researchers” in a co-directed inquiry into their experiences. Their study provided insights into approaches taken for involving people with EOD in research and emphasized the role of research participants as co-researchers. They suggested a methodology for involving people with EOD in participatory research in a sensitive and productive manner. Furthermore, they encourage researchers to actively engage people with EOD as collaborators in every stage of technology design, rather than the traditional and more passive “participant” role.
From our literature review, there appear to be no documented studies to illustrate design of technology for people with MCI/EOD in the context of work. Considering the current trend toward direct inclusion of the intended users of technology in the technology’s development in addition to the special considerations related to people living with MCI/EOD, research needs to be done to directly include people in the creation of technologies intended to support their goals, such as engagement in employment.
Methods
There is no specific methodological guidance from the literature on how to best approach participatory research with people living with EOD or MCI, especially in a workplace setting. We consequently designed our study using the research presented above in combination with the authors’ expertise in capturing an understanding of experiences and collaboratively developing technology with people living with dementia.
This research was conducted as a two-part study with people living with MCI/EOD and their spouses, which are described below. Despite their utility, ethnographic observations in participants’ workplaces were not conducted in this study because participants had either left work (i.e., were on leave or unemployed) or had not formally disclosed their diagnosis to their employer and/or co-workers therefore requested they not be contacted. This research received approval by the Research Ethics Board at the University of Waterloo (study #40051).
Part 1: Semi-structured interviews
Semi-structured interviews were carried out in collaboration with researchers from occupational therapy, psychology, and engineering. The interviews were conducted with people with MCI/EOD and their family support partners (e.g., spouse) when they chose. Participants were recruited from the Waterloo-Wellington and Durham regions in Ontario, Canada by posting flyers on local businesses’ bulletin boards, contacting local dementia organizations, and through social media. Participants were screened over the telephone before scheduling interviews, and the capacity to provide verbal informed consent was evaluated over telephone. Before commencing the interview and discussion, each participant completed a demographic questionnaire. All interviews were audio and video recorded for later transcription and thematic analysis. MCI/EOD diagnosis was self-reported by the participants and no cognitive tests were examined during the study.
The guided interviews started with a discussion about the participant’s general experience of being in the workplace with MCI/EOD and covered three key areas of discussion: (1) the impact of their changes on their ability to work; (2) policies surrounding MCI/EOD at work; and (3) the use of technology/tools in the workplace. Data from the semi-structured interviews were used to answer the first question guiding this research, which was to gain an understanding of the experiences of people with MCI/EOD with technology in the workplace.
Part 2: Participatory sessions
Participatory sessions to explore potential ideas and extrapolate cues related to the design and development of technology for people with MCI/EOD were carried out with a sub-set of the individuals who participated in the semi-structured interviews from Part 1; the recruitment and verbal consent process was the same as the semi-structured interviews in Part 1. Data from the participatory sessions were used to answer the second question guiding this research, which was to develop a process of involving people with MCI/EOD in designing new technologies to support workplace engagement.
The participatory sessions were structured into four activities. These activities were communicated with the participants a few days before they participated in a session to convey what was going to happen during the sessions, as well as give them time to think about and prepare for the activities should they wish to do so.
Activity 1: Show and Tell
Participants were asked to bring one piece of technology (or a picture of it) that they like and use in everyday life and one piece of technology they dislike or have stopped using. Technology was defined as any object or artifact that helped the participant to complete a task. The Show and Tell activity was designed as an ice-breaker between the participants and the researchers.
Activity 2: Design your workspace
Next, participants were asked to recreate their work space or workstation from their workplace. This was done to contextualize the participants work environment and help participants recall by recreating their work environment.
Activity 3: Challenges at work
After recreating their work space, participants worked with the researchers (first, third, and fifth authors) to delve deeper into aspects regarding the participants’ challenge points (i.e., tasks or objects they had difficulty with at work). This includes identifying and describing why challenges occurred and strategies that were used or could be used to help mitigate said challenge points. Responses were probed through unstructured questions.
Activity 4: Brainstorming potential ideas
The last activity was an exploratory one to enable the participants to articulate their design preferences and goals. To focus the activity, the participants were asked to imagine a thing or a person that could help with navigating through the challenge points identified in Activity 3. The participants were then asked what they would like to tell this thing or person about their challenges and strategies.
Data analysis
Data consisted of transcribed recordings of interviews, field notes of observational research, and reflective notes made during the sessions. These were qualitatively analyzed using inductive thematic analysis, which involves analyzing, examining, and recording patterns or themes within the data (Daly et al.,1997). First, recorded responses captured during the semi-structured interviews and participatory sessions were transcribed verbatim by members of the research team to ensure reliability, validity, and accuracy of qualitative data collection (Halcomb & Davidson, 2006). Then, we used a multi-phased process similar to the approach used by Braun & Clarke (2006) to extract themes by executing the following steps: (1) becoming familiar with the dataset; (2) identifying preliminary codes; (3) exploring possible themes; (4) assessing and revising codes and themes; and (5) finalizing and defining themes. Passages from the transcripts were coded and arranged according to the two questions guiding this research. Coded passages were analyzed inductively, whereby the first author coded the data without trying to fit it into a pre-existing coding frame (Fereday & Muir-Cochrane, 2006). The dataset was structured using NVivo 12 Pro.
Results
Part 1: Semi-structured interviews
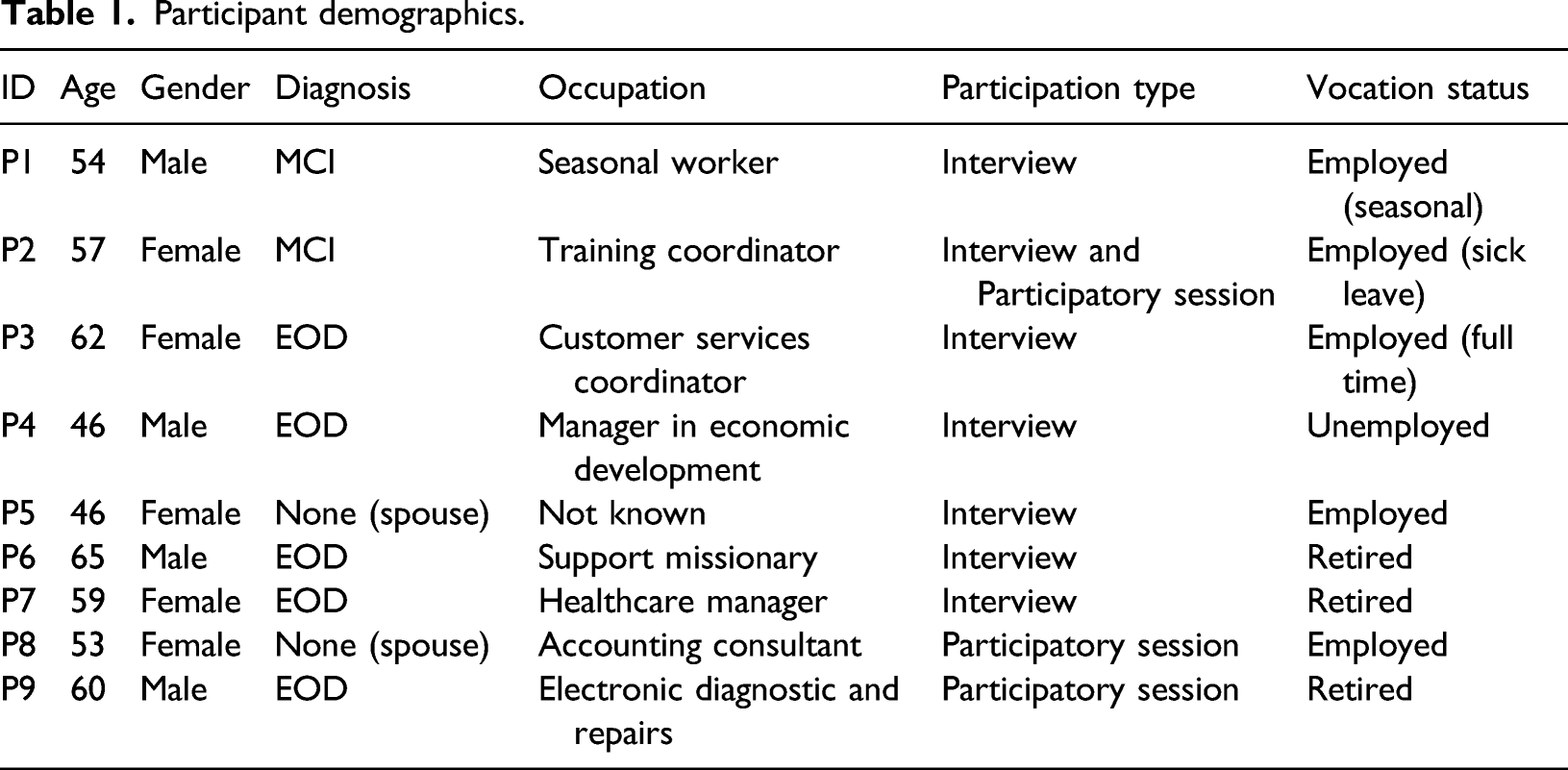
Participant demographics.
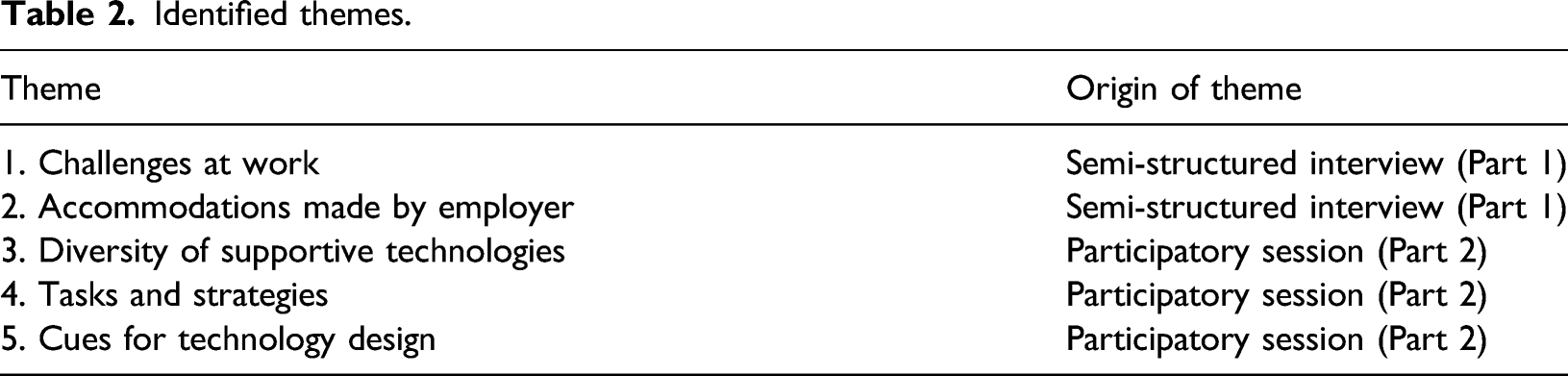
Identified themes.
Interviews were carried out in-person at the participants’ preferred location between December 2018 and March 2019. Each interview lasted an average of 106 minutes with the shortest being 59 minutes and longest 174 minutes. Each interview transcription generated between 20–40 pages of single-spaced text.
Key themes from part 1: Semi-structured interviews
Theme 1: Challenges at work
The challenges discussed below were often first noticed in the workplace. Some participants recognized that there were problems at work (P1, P2, P3, and P7), while others did not. There was no clear consensus on identifying the starting point of difficulties at work and things that were challenging for one participant were not necessarily for another. However, several areas were more common across the participants:
Memory-related difficulties
Challenges related to changes in memory encompassed a wide range of abilities, changes in abilities, and resulting implications.
P1 talked about problems with initiating and completing tasks. He also mentioned his challenges with often forgetting work-related tasks.
“It’s the challenge in my brain that is (pause) you know, I’m wrestling in my head trying to, you know, okay, this is what I gotta do, this is... ’Cause it’s starting to slip away” [P1].
P2 explained how her memory-related challenges impacted her day-to-day tasks at home and her use of timers to remind her of tasks to complete, such as cooking. She also mentioned that there were instances where she forgot why the timer was set up in the first place.
“It (timer) was to help me with my next task. Like, to get me, to get me from my focus (sigh)... I don’t know how to describe it. it’s like I don’t know of anything else going on, and then I would set the timer. There were times the timer would go off and I didn’t even remember what it was for, but I just knew it was for something” [P2].
P6 had challenges with orientation while driving and completing work-related tasks. His family members first started noticing symptoms of dementia and he experienced an accident at work.
“Well my wife had said she’d seen symptoms for a couple years that I had not...a little disorientation driving, more emotional. Just subtle things. My daughter also acknowledged them to the point where, well it could maybe start to affect safety. Thirty-five feet up on a clay roof working away might not be as good a place (for him to keep working)” [P6].
P7, who had been a healthcare manager, had forgotten one of her client’s medications, which was a regular work-related task for her.
“I mean it was a common thing to make a med error like that but I had never made one in twelve years.” [P7]
Communication challenges
P3 felt her supervisor did not consider her memory-related challenges seriously and brushed it off when she was informed about it.
“She (P3’s supervisor) said ’I don’t believe it has anything to do with your memory. It’s something else and I know what it is..’. And I- That was it. And I didn’t say well, what it is, I just was shocked. I didn’t know what to say.” [P3]
P5 (spouse of P4) mentioned there had been no direct communication between P4 and P4’s employer until the organization decided that P4 would no longer be returning to work.
“I was totally in the dark until he (P4) told me he wasn’t going back. Like I knew about the HR (meeting) but he didn’t know he was not going back, it seemed like he was confused... So, you know, it would’ve been nice if he walked out of that meeting with a paper so that even I would know what was going on right?.. Like to actually leave with a paper so you know, and the family knows, what’s going on.” [P5]
Theme 2: Accommodations made by the employer
For many participants (P2, P4, P6, and P7), their diagnosis resulted in either early retirement or sick leave, both of which were unexpected for the participants in this research. Others mentioned that employers managed the situation in terms of the changes or accommodations made in the workplace.
P1’s main work-related tasks for his parks maintenance job involved lifting objects and driving a vehicle. Accommodations were made by P1’s employer, however, this was done to compensate for physical challenges that were unrelated to his MCI. P1 has not disclosed (at the time of our interview) his cognitive challenges to his employer due to fear of losing his current vocation.
“...because there’s nothing. Everything here (workplace) is heavier than five pounds so from that limitation until she (HR) removes that restriction or raises it, we can’t work within that. So when she (HR) finally did raise it, um, then I was able to come back and at least do most of what I was doing before ’cause not doing a whole lot of lifting anyway, but um, but you have to do some lifting” [P1].
The employer in P2’s case made accommodations by reducing the number of work hours, although this accommodation was not always upheld.
“I went back to work in (year) and I was accommodated with, I went back part-time, like just, like I was doing 9 hours a week and then 12 hours a week” [P2].
No accommodations were made by the employer in P4’s case, to the best of P5’s (spouse) knowledge. Even if accommodations were made, there was no coherent documentation on why (if any) accommodations made were not successful.
“It didn’t sound like (accommodations were made)... If it did I don’t know what it was... Even in the document that they supplied to HR, um, giving their reasons, didn’t say well we did this accommodation and still this was a problem, or we did that accommodation and it was still a problem.” [P5].
P6 mentioned flexibility with his job as a support missionary and a complete understanding by his employer when his diagnosis was communicated to his employer.
“Total understanding at work. No, (the diagnosis was) not a problem, just do what you can” [P6].
P7 did not ask for any accommodation from her employer. She felt she did not want to return to work because she had to deal with vulnerable populations and did not want to risk potential harm to her clients.
“...could I have stayed in my job longer? And the answer would be like absolutely not. There’s no way. Um, I mean, they’d have to bring in another case manager to hold my hand so, you know what I mean? And uh, there would be no job that I could do in that agency because on one level or nothing, or one level or another, we’re all looking at the well-being of vulnerable people” [P7].
Part 2: Participatory sessions
Two sessions with a total of three participants (P2, P8, and P9) were conducted; P8 is the spouse of P9. Similar to the semi-structured interviews, each session explored the personal experiences of MCI/EOD intending to explore potential ideas and extrapolate cues related to the design and development of technology.
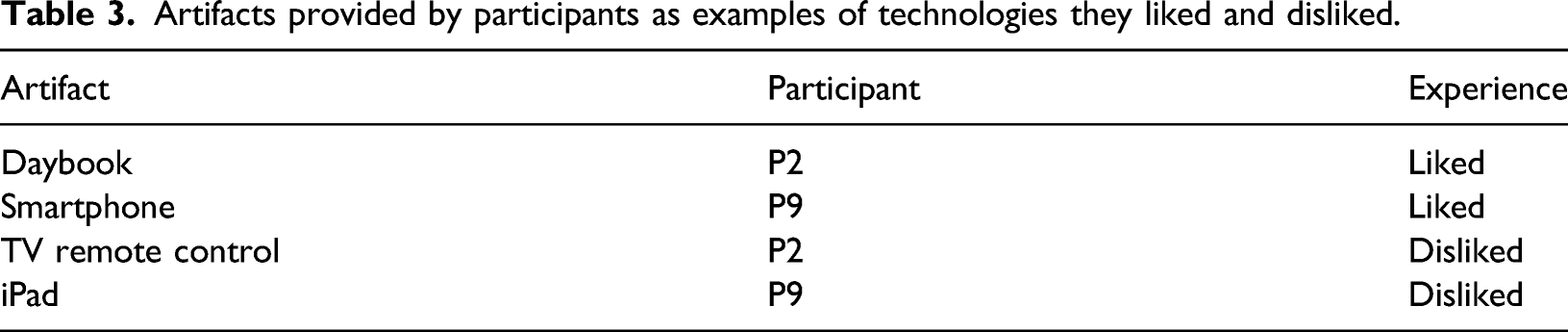
Artifacts provided by participants as examples of technologies they liked and disliked.
Theme 3: Diversity of supportive technologies
The artifacts participants shared with the authors ranged from electronically powered technologies such as smartphones to non-powered items such as daybooks as listed in Table 3 with the participants’ self-reported relationship with the artifact (indicated by liked/disliked).
P2 mentioned the use of a daybook to manage her day-to-day activities at work and home. P2 showed the first author how she input tasks and reminders in her daybook throughout the session.
“...so the daybook for sure, I write um, I write everything in here, the calls that I should make that day, and then there are times that I may add the stickies do help me as well, um, I might even add a sticky in here if there’s something else although I’m not seeing any right now.”[P2]
P9 mentioned use of a smartphone and his affinity for it to complete everyday activities. “There’s so much you can do with it (phone). You can actually make calls... If I need to find something, which I am researching, uh, this is the first thing I’ll be jumping at and then yeah. And it helps a lot.” [P9]
P2’s dislike of a TV remote control was brought-up when discussing technologies disliked/abandoned. She also mentioned that her dislike for the remote control stemmed from the need for multiple steps required as an input from her.
“Here is what I need. What I need is step by step by step. Number 1, number 2, number 3.” [P2]
“it’s like always starting a new system, and that’s the problem... I don’t remember that I have to start new system until I do it, and then I associate it and the color, and I repeat, repeat, repeat, repeat.” [P2]
P9 felt a dislike for his iPad, which was used in the context of his day-to-day life and not at work. This (dislike) mostly had to do with the iPad’s form-factor:
“...yeah, it’s (iPad) so big... Something like this [points at phone] is so ideal. You know?... And I always like the little gadgets. I’m a gadgets guy!” [P9]
Theme 4: Tasks and strategies
During Activity 3 (challenges at work), there was a wide breadth of challenge points (i.e., specific aspects about a task that were particularity difficult) and related-strategies participants used to mitigate these challenge points. The first author used sticky notes to highlight the points (Activity 3) mentioned by participants in the participatory session with P8 and P9, as seen in Figure 1. P2’s recreation of her work space during Activity 2 with sticky notes representing artifacts at her work-desk
P2 mentioned clutter, changing work-desks, and a smartphone to be her challenge points. Strategies used to mitigate these challenge points were color-coded cheat-sheets and asking for help from other people at work.
“the cheat sheets to me it’s you know, and also you know what else is I think part of this is learning about it, but learning which feature do you need and which do you not need. And that needs to be dictated by, I believe the employer, so what ...umm so it’s not felt like now this person has to now master the Blackberry.” [P2]
When asked to design their work space (Activity 2), P2 was quick to use sticky notes and recreate her work-desk, as seen in Figure 2. Different design preferences mentioned by P8 and P9
P9 mentioned memory challenges at work as his challenge point, similar to the theme that was mentioned earlier with the semi-structured interviews.
“Before I was, as I said, more sharper and getting stuff done and because the dementia now, I slowed down. And I go and start doing a project and then a few minutes later I forget, What was I doing again now? You know what I mean? That’s the, that’s the problem with dementia.” [P9]
P8 (spouse) also mentioned P9’s challenges with using new technology—for example, with appliances at home.
“No if we have (a) new appliance now, they are harder to navigate . Like it’s harder for him [P9] to learn, learn new things-” [P8]
“Like it doesn’t matter how easy it (new technology) is. It’s not the ease of use that’s the problem, it’s when you don’t remember what to do. So even if there’s a big block of red light flashing saying press here, press here, press here - that it still may not register. Right?” [P8]
Theme 5: Cues for technology design
During the fourth activity (brainstorming potential ideas) we discussed ideas for potential technologies through an imagination activity, namely, asking the participants to describe what they would tell a person or a thing (tool) about their challenges and strategies.
P2 mentioned how she would identify her challenges in the first place. For her, this signaled that there was a disconnect between what she wanted to do and what she was able to do.
“Well I think like for most people the first clue that something is not right is that you’re having an emotion around it, frustration, sadness, that feeling of being less than, incompetent, umm, unable to accomplish.” [P2].
P8 mentioned the need for less input (i.e., fewer steps required from P9) to use artifacts/tools.
“...you’d have a higher probability that he’d (P9) be able to do that (single-step input) than anything else... You know, once you start adding a second command, unless the first one’s a red light that says press here, and then the next light comes on and says... a green light and says press here, and then an orange light and says press here you know. And he keeps pressing until he gets to the final outcome.” [P8]
P8 also mentioned how socialization through technology is helpful to P9.
“...so she’ll (daughter) bring lunch for him or something like that. Uhh, we haven’t looked at technology in terms of helping...I think the one thing we know that’s very helpful is the social aspect of, you know, staying connected with people.” [P8]
P8 mentioned minimal need for navigation and easily digested content by using Netflix’s ease of use and recommendation system as an example.
“Netflix just uses that kind of information to give you what’s the latest thing. So when he clicks on it, all those new things come up, or the old ones, and he’ll just re-watch them. So from that perspective it works really well.” [P8]
P8 mentioned rule sequences are complex for P9 to follow and reiterates the importance of simple design through an example of sorting household garbage (trash) into correct containers.
“So (P9)’s dementia started before they had the new green box [organic waste], blue box [recyclables] program...The new sorting, the new garbage program right? So umm (pause), that’s a very very very difficult process for (P9) to navigate through. What goes in the green bin, what goes in the blue bin, what goes in the garbage. That’s very difficult for him to navigate.” [P8]
P2 proposes having a designated person at work or a “job-coach” with whom she could discuss her challenge points and develop related-strategies as way to solve her existing challenges.
“A career coach or a job coach...we were trying to put one in place to help with our clients, when they are out um in an employment situation and meeting challenges and its not until you just asked me this question and I am thinking, within an organization that, that is something that might be incredibly helpful.” [P2]
Discussion
Overall findings
A quote from P1 stands out as it describes most participants’ day-to-day experience:
“Every day is different. Some days are great, some days are different.” [P1]
Findings in this research echo studies such as Evans (2019); Ohman et al.(2001) that show changes in abilities of people with MCI/EOD, such as memory, concentration, and communication, often impact the workplace first. While changes at work can profoundly affect how a person engages in their vocation, it can be what first prompts the person to seek help, which may lead them to initiate the process of getting a diagnosis (Roach & Drummond, 2014).
The narratives captured from the participants in this research illustrate how complex and personal MCI/EOD is with respect to a work setting. As a result, establishing how to provide appropriate accommodation is also complex and personal. It is not only a matter of determining whether cognitive impairment is present; it involves intertwined and sometimes competing considerations, such as which abilities are affected, how this might impact one’s vocation, what resources are available, relationship with one’s employer, and how dynamic the symptoms are (Mair & Starr, 2011).
Not all workplaces can support employees with declining cognitive function to the same extent (Melillo, 2013). For example, P2 disclosed her challenges to her employer, who made some accommodations (e.g., reduced hours and ability to work from home). However, P2 stated that these were short-lived and later, not honored. In other cases (P3, P4) there were no perceived significant changes made. In most cases, it was the person with MCI/EOD themselves who had to come up with workplace adjustments. As they are the ones who are living with the condition and are the one that must perform with what is put in place, the person with MCI/EOD can and should play a key role the workplace accommodation process, however, this should be done in collaboration with their employer and (ideally) people who have expertise in providing such accommodations. Understanding what and how MCI/EOD can be accommodated by the employer and workplace would support researchers and tech developers in creating technologies that can complement the multiple stakeholders it impacts.
While the perspectives in this study are from employees (rather than from employers), the consensus was that many employers lack what they need to support people with MCI/EOD in the workplace, including knowledge of how to best support as well as tools to provide support; this aligns with findings by Ritchie et al. (2015), who explain in their study how no employers had previous experience supporting an employee with dementia and had to learn as they went. Findings such as these underscore a lack of understanding of dementia in the context of work. It also emphasizes the importance of developing cognitively accessible technologies that not only support engaging in employment (e.g., task completion), but support a better understanding of each person’s experience as well as the employer’s ability to support the employee. For example, a technology that can be used by a person with MCI/EOD with their employer, colleagues, and/or family could enable shared day-to-day communication and documented history that could then be used to deepen understanding of needs on both sides as well as collaboratively create and track strategies. Tools such as these may help employees with MCI/EOD and people in their networks to have more agency regarding whether and how they would like to engage with work as well as the transition out of work more gracefully, should that be the chosen direction.
Technology design
Although each person’s experience was specific to their vocation, environment, diagnosis, and personality, the variety of technology/artifacts that participants discussed shed some light on what makes technologies more usable for people with MCI/EOD. For example, P2 used a daybook for its simplicity and versatility and her phone for providing easy access to information were examples of favorite tools. In contrast, the iPad (P9) and the TV remote control (P2) were not viewed favorably due to their size and features that create confusion, respectively.
P2’s description of the daybook for her daily planning presented several insights on using a physical artifact to assist with tasks at work. Specifically, she used different colors in the daybook to signify various tasks, tearing pieces of pages to indicate the tasks of the corresponding day is completed. This also illustrated the value of having a single primary tool for keeping track of tasks. This example has direct implications for technology design, including the importance of color, indication of a completed task, and the ability to centralize information.
Technologies that P2 found helpful also presented challenges, such as her use of timers during daily activities like cooking but often forgetting why she had set the timer to begin with. This finding is consistent with Ohman et al.’s (2001) work where some participants developed strategies to remain in control of their vocation situation by trying to use memory aids such as tape records and calendars. These aids were, however, of questionable use because participants often forgot to bring them along with them or to use them when they had them available.
P8, the spouse of an individual with MCI/EOD (P9), mentioned the need for technology to require minimal input from her partner, such as having a clear sequence of very few steps. They also highlighted easily usable service like Netflix with its minimal need to navigate through tailored content. This highlights a similarity between MCI/EOD and dementia research. Furthermore, it aligns with other technology creation research, such as minimizing the number of clicks to reach different pages within an interface as a requirement for dementia-friendly interfaces (Kerkhof et al.,2017; Riley et al.,2009). Previous research has also shown the benefits of simple, intuitive interfaces that have been used for activities such as making music (Riley et al.,2009), creating art (Leuty et al., 2013), and playing games (Astell et al.,2014). Furthermore, it aligns with other technology creation research, such as minimizing the number of clicks to reach different pages within an interface as a requirement for dementia-friendly interfaces (Kerkhof et al.,2017).
Since going on leave, watching the television became a more significant activity for P2 but was challenging because of difficulties with using her TV remote control. P2 mentioned that having a basic set of instructions as well as obvious graphical and/or text cues and highly contrasting colors for the different buttons on the TV remote control would assist her to know how to use it. P2’s challenges and identified desired changes in design that would provide support align with other literature describing difficulties encountered by people with dementia when using everyday technology such as telephones, alarm clocks, or radios (Rosenberg et al.,2009).
The participatory design sessions were intended to start with people bringing in examples of familiar technology/artifacts from their workplace. However, as P2 has been on leave from work for some time and spends most of her time at home, she brought an artifact she uses at home. Understanding how cues from everyday technology (such as a TV remote control) could inform technology design for the workplace was a topic that came up in our discussions. For example, P2 mentioned that a basic set of instructions similar to those that help her to use her TV remote control might have helped to mitigate her challenges with using a smartphone when she was still at work.
While we cannot generalize the experiences of our participants with all people with MCI/EOD, through this study we have developed an initial understanding of the ways people with MCI/EOD are currently using technology. This helps to map the technology’s relationship with their needs as well as intrinsically highlights what technologies are usable in different contexts and why. As explored through this research, there are few similarities or differences in terms of the types of technology used and abandoned. In other words, as is the case with people in general, people living with MCI/EOD are different, their abilities are different, what they like/dislike is different, and what they find helpful/challenging is different. Also, in line with the general population, complementing people’s abilities and preferences is central to the adoption and continued use of a tool.
Bell and Leong’s (2019) work argues that technologies designed for and adopted by individuals at the early stages of dementia may well continue to provide them with benefits as the symptoms of dementia progress. Astell et al. (2014) advocate for leveraging tools they are familiar with rather than asking them to adopt new technologies at later stages of dementia may provide greater benefit. Our research supports both these positions.
While interviews and participatory sessions can democratize the environment (Muller, 1993) and enable close contact between researchers and participants (which may help foster empathy in design (Wright & McCarthy, 2008)), it requires people with MCI/EOD to recall and verbalize their experiences. Our experience highlights the importance of exploring work-related technology needs whilst individuals are still in the workplace. While P2 and P9 had been out of the workplace for only a few months, they spoke mainly about their current experiences with technology (i.e., non-employment context). Moreover, affected cognition and memory can make it difficult or impossible for the participants to accurately recall specific details of their workplace and interactions with it, which can result in inaccurate data and cause feelings of frustration or ineptitude for the participants.
Recognition provides a relatively stronger representation of the relationships between events in that it involves concrete examples, which can trigger memories and support free (explicit) recall (Hockley & Consoli, 1999). Thus we hypothesize that providing participants with broader work-related artifacts as a stimulus (e.g., desk phones, monitors, and physical calendars) may result a more in-depth discussion around their usage and related benefits and challenges. Having examples of technology present may also support discussion through implicit cues (i.e., looking at and interacting with it triggers points of discussion) and enable participants to show what they mean, rather than describe it. However, selecting which technologies to use would have to be carefully done to minimize priming or biasing the participants and would be difficult to do if a broad number of vocations and/or workplace settings were explored.
Evaluation of the research process
Recruitment was difficult for this research. This is partly because of the difficulty in receiving a formal diagnosis of MCI or EOD before the age of 65 (Ohman et al., 2001), which means eligible participants may not self-identify as meeting study inclusion criteria. Potential participants are also often sensitive to how changes in cognition are impacting work and may not want to engage in research regarding this topic. Thus engaging in research in the area of MCI/EOD requires a great deal of empathy and patience.
Of the seven participants with MCI/EOD from the semi-structured interviews (Part 1 of the study), only P2 returned for the participatory sessions (Part 2 of the study). As with other types of research, it is essential to consider that participants may not be interested in further sessions/studies when invited, which may be due to various logistical (e.g., scheduling) and/or personal reasons; these difficulties may be exacerbated by the changes in life that come with having MCI/EOD. Furthermore, for people who are still actively employed, finding suitable times and locations can be challenging, especially those who want to be interviewed after work and feel overwhelmed with day- to-day life as is.
The severity of cognitive impairment and what abilities are impacted by MCI/EOD requires consideration when carrying out interviews and participatory sessions with people with MCI/EOD. In two specific cases, P5 and P8 (spouses) helped keep the conversation on-track throughout. In one instance, P9 mentioned his smartphone as a technology he liked and could use in the Show and Tell activity at the beginning of the session. Upon hearing this, P8 (his spouse) asked P9 to call her (P8) using his smartphone, to test if he could operate his smartphone, which P9 was unable to complete. This example reflects how people with MCI/EOD may overestimate their abilities based on free-recall alone, consistent with related symptoms. While in this instance, P8’s spouse correctly identified a mismatch between P9’s perceived and actual abilities, prior research has shown that family members or care partners can over/under-estimate the needs and abilities of their care partner with MCI/EOD (Hendriks et al.,2014). Thus, while support from care partners (in this case their spouse) enabled some individuals with MCI/EOD to engage in the research, prompting from their spouse impacted the direction of the conversation. This supports previous findings of the importance of distinguishing the needs and priorities of individuals with MCI or dementia from those of their family members (Astell, 2006, 2019). This example serves to highlight that having people with MCI/EOD physically engage in relevant tasks or activities is especially appropriate and valuable to ascertain their needs, abilities, and use of technology.
It was important to be flexible with the activities set out in our participatory sessions. For example, the participants (P8 and P9) forgot to bring the technology/artifacts for the participatory session (Part 2 of the study) for the Show and Tell activity. Calling the participants, the day before to remind them of the session and to bring their Show and Tell items could help to address this. To illustrate what the activity entailed and to give the participants time to think, the researchers discussed pieces of technology they liked and disliked. While this helped participants to provide their own examples, the researchers presenting their own examples first could have biased which technologies participants chose to focus on and what elements about them they liked/disliked. Moreover, having the technology (or a picture of it) present may act as an implicit cue for the person to recall details about what they like, do not like, and how the technology is used.
While the areas for exploration may be complex, participatory (hands-on) activities designed for people with MCI/EOD should be kept simple and targeted with objects/short notes/drawings that can provide ongoing cues. For example, while P9 was able to participate and communicate well in all activities of the participatory session, with the exception of the “design your workspace” activity, where he was unable to remember details well enough to recreate his workspace. In this instance, his spouse (P8) gave prompts to try and support recall, but could not provide assistance beyond this, as she was not familiar with P9’s workplace.
P2 used sticky notes with “challenge points,” “why,” and “strategies” written on them to provide her cues and elicit her challenges, why they occurred, and the strategies she used to mitigate them in the third activity of the participatory session (Part 2). This example reflects the importance of ongoing cues in activities for people with MCI/EOD, as they can aid in keeping the participants aware of what is being discussed and can support recall. This type of strategy is aligned with and highlights another similarity with reported successful uses of participatory design techniques with people with dementia (e.g. Hanson et al.,2007; Hawkey et al.,2005; Robinson et al.,2009; Savitch & Zaphiris, 2004).
The interviews (Part 1 of the study) and participatory sessions (Part 2 of the study) were initially designed to have participants (people living with MCI/EOD) share their experiences in a focus-group format. The aim of having a focus group was for the participants to share experiences in a way that can also identify similarities and differences. During recruitment, it became clear that many of the participants did not want to take part in a group format due to (a) location differences and (b) anonymity. The latter was because some participants were currently employed or on leave and were worried about being recognized. These aspects should be taken into consideration when designing studies for people with MCI/EOD, especially with respect to potentially sensitive aspects such as the work context. Having interviews in a one-on-one format instead of a focus group allowed us to probe deeper into aspects such as challenges and accommodations made at work.
Future work should also consider methodologies that more explicitly engage with the first-person perspective (e.g., phenomenology), including from employees, employers, caregivers, and other stakeholders.
Limitations
The sample size for this research was small. Given that this study focused on first-stage research and encountered challenges with recruitment, the number of participants in this work is in line with similar studies in this field (e.g., Kerkhof et al.,2017; Robinson et al.,2009), therefore deemed to be appropriate. The circumstances of many people with MCI/EOD in the workplace likely influenced the recruitment process (i.e., potential participants may be reluctant to come forward). Additionally, the perspective of the employer/co-worker and ethnographic observations from within the workplace is missing; both are crucial to the design of technologies as they provide significant and relevant context and related considerations. Regardless of potential difficulties in recruitment, as the abilities, experiences, and contexts of dementia in the workplace are so diverse, more extensive research needs to be done to gain a comprehensive view of this area. Specific research on how to better recruit and involve people living with MCI/EOD would be of benefit to supporting research with people with cognitive impairment in general.
While this research focused on technology use in a workplace setting, it was solely from the perspective of people living with MCI/EOD in a non-work setting; it is missing the employer and other relevant stakeholders’ perspectives. Future research should aim to capture multiple perspectives regarding the same individual and collect data in the workplace setting. This is a significant undertaking as it involves a trusting relationship between the researcher, employee, and employer, which can take considerable time and effort to achieve and maintain. This is complicated by the fact there is limited time between when most people realize they have MCI/EOD and when they tend to leave the workplace. Therefore, researchers who choose to engage in an ethnographic approach must have a clear rationale for the methods they choose; they must be sensitive to relationships, highly safeguard people’s trust, and carefully weigh the value of knowledge gained against the risk of harming well-being (e.g., maintaining/compromising anonymity and discussing traumatic experiences with people they do not know well).
There are many aspects and themes that warrant specific and deeper research, such as what aspects of technologies influence people with MCI/EOD’s attitudes towards them.
Conclusion and summary
This research was conducted to explore how to capture the working experiences of people with MCI/EOD to provide insights about how technology is used as well as what would be beneficial in technology designed to support people living with MCI/EOD. As alluded to by P8
“If you’re (technology developers) really good at what you do, you should be able to get us to what we want in fewer steps. Right?” [P8]
Through interviews and participatory design sessions, we discussed with people with MCI/EOD about how their interactions with everyday technologies at home (TV remote control for P2, smartphone use by P9, for example) could potentially give insights to designing technologies for supporting work. This approach may benefit people with MCI/EOD at work with the adaption of technology that is more familiar, rather than asking them to adopt and adapt to new technologies at later stages of dementia.
Many of the outcomes of this research align with what has been found in other studies related to designing to support dementia. The fact that changes in abilities are often first noticed at work, that there is very little perceived support, and that work can be a profoundly meaningful part of a person’s life points to a real need for related research and development. Namely, there is significant and relatively untapped potential to develop technologies for supporting people with MCI/EOD’s engagement in and relationships with work.
Through this research, we identified two major similarities with literature on research with dementia:
(1) People with MCI/EOD prefer simple and clear technology with as few steps as possible, and (2) methodological techniques with physical examples rather than recollection of past events can support clearer conveyance of facts. This research scratches the surface concerning the diversity of needs, abilities, and contexts related to supporting people with MCI/EOD at work. While technology cannot mitigate all challenges, it could play a significant role in many instances. New approaches, such as adaptive user interfaces, should be explored to see how they might enable dynamic and personalized support.
This paper contributes knowledge regarding how to design a collaborative study with people living with MCI/EOD and understanding how researchers can extrapolate cues from everyday technologies to help create new ones to support people with MCI/EOD at work. Future research using similar approaches could enable researchers to gain a deeper understanding and strengthen the methodological toolbox as a guide to design technologies for supporting people with MCI/EOD at work.
Footnotes
Acknowledgment:
The research presented in this paper is part of an international project titled “MCI@Work” with the aim of creating a digital tool to support role planning for people with MCI/EOD and their employers at work
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JTC 2017 as part of the Joint Programming Initiative (JPI) “More Years, Better Lives” (JPI MYBL) initiative. JPI MYBL is supported by J-Age II, which is funded by Horizon 2020, the EU Framework Program for Research and Innovation, under Grant Agreement #643850.
![]()