
Abstract
Introduction
Health research that focuses on Indigenous Peoples must ensure that the community in question is actively engaged, and that the results have context relevance for Indigenous Peoples. Context relevance is “the benefits, usability, and respectful conduct of research from the perspective of Indigenous communities.” The purpose of this study was to apply two tools within an already-published scoping review of 76 articles featuring research on cognitive impairment and dementia among Indigenous Peoples worldwide. One tool assessed levels of community engagement reported in the corpus, and the other tool assessed the context relevance of recommendations in the corpus. We hypothesized that research with higher levels of reported community engagement would produce recommendations with greater context relevance for Indigenous Peoples.
Methods
We employed semi-structured deductive coding using two novel tools assessing levels of reported community engagement and context relevance of recommendations based on studies included in the existing scoping review.
Results
Application of the two tools revealed a positive relationship between increasing community engagement and greater context relevance. Community engagement primarily occurred in studies conducted with First Nations, Inuit, and Métis populations in Canada and with Australian Aboriginal and/or Torres Strait Islander Peoples. Research with Alaska Native, American Indian, and Native Hawaiian Peoples in the USA stood out for its comparative lack of meaningful community engagement.
Discussion
There is opportunity to utilize these tools, and the results of this assessment, to enhance training and mentorship for researchers who work with Indigenous populations. There is a need to increase investigator capacity to involve communities throughout all phases of research, particularly in the pre-research stages.
Keywords
Introduction
Dementia is a growing health concern worldwide due to expected increases in prevalence rates from over 55 million worldwide in 2019 to an expected 139 million in 2050 (World Health Organization, 2021). The limited available evidence suggests that dementia is also an emerging health concern among some, though not all, Indigenous populations. Bryant et al. (2022) reported in a scoping review of 76 studies of Indigenous populations from seven countries that researchers have found higher prevalence rates of dementia in Indigenous Australians compared to non-Indigenous Peoples (Li et al., 2014; LoGiudice et al., 2016; Smith et al., 2008), high prevalence rates among American Indians compared to non-Hispanic whites in a sample from the western USA (Carty et al., 2020), faster rates of increase in dementia rates in First Nations versus Non-First Nations Peoples in Alberta, Canada (Jacklin et al., 2013), and diagnoses at younger ages in Māori and Pacific Peoples and among Aboriginal Australians (Cullum et al., 2018). Conversely, a recent study in Brazil by Gatz et al. (2023) found that Tsimane and Moseten Peoples had the lowest prevalence of Alzheimer’s and related dementias based on available evidence from all populations worldwide.
Given the increase in dementia at a global scale, the World Health Organization, in their 2017 global action plan (World Health Organization, 2017) called for Member States to double the output from global dementia research between 2017 and 2025 to address the increase in dementia prevalence worldwide. They also called on Member States to, “Strengthen research capacity for academic collaborations on national priorities for research into dementia by engaging relevant stakeholders, including people with dementia” (World Health Organization, 2017, p. 33). In 2021 the Alzheimer’s Association emphasized a need for increased racial and ethnic diversity in the Alzheimer’s caregiving workforce and clinical trials (Alzheimer’s Association, 2021). Similarly, the National Institutes of Health (NIH) in their 2022 report on the progress of dementia research emphasized the importance of increasing diversity in clinical trial participation (NIH, 2022). The NIH report highlighted the need for community engagement, with the primary rationale being to increase diversity of participants through recruitment and retention in clinical trials (NIH, 2022, p. 35).
Increased engagement with Indigenous communities in dementia research is thus recognized as essential by multiple organizations and prior researchers. At the same time, there is a need to critically assess existing knowledge to determine levels of community engagement and the relationship between community involvement and the relevancy of the research recommendations. Dementia research may present unique challenges for community engagement, which may be related to historical harms from research in general and lack of perceived cultural safety of clinical mental health care, including dementia care (Chakanyuka et al., 2022; Hamilton et al., 2021; Wendt et al., 2022). In addition, multiple studies have reported community values regarding caring for Elders, including people living with dementia to remain “in country” or “on the land,” and with their families and communities, whether rural or urban (Chen et al., 2020; Hulko et al., 2010; Jacklin et al., 2015; Johnston et al., 2020; Lanting et al., 2011; Pace, 2020; Smith et al., 2011). Research in dementia may be perceived by some Indigenous people and their communities as likely to result in unwanted removal from home to an institution (Duran, 2019; Hulko et al., 2010). This can be seen as disrespectful as cultural norms revere Elders and they are expected to be cared for by the family (Hulko et al., 2010; Johnston et al., 2020). Therefore, collective worth and usability of research for research participants and for their communities may be a critical factor for Indigenous people when deciding whether to consent to participate in dementia research (Brayboy et al., 2012; Hull & Wilson (Diné), 2017; LaFrance & Bull, 2009). Community engagement is thus helpful for producing relevant research results and recommendations, as well as for increasing participation.
Health research that focuses on specific communities can benefit from active participatory engagement with communities throughout the research process (Cochran et al., 2008; Harfield et al., 2020; Peltier, 2018). This is especially so for Indigenous Peoples owing to long histories of colonial subjugation. As a result, Indigenous communities often perceive risks of participation in mental health research to be relatively high in relation to potential tangible benefits (Gone, 2022; Wendt et al., 2022). Thus, direct benefits to communities (i.e., interventions, funding, capacity building, data ownership for community uses, and sharing of results with lay audiences) are often deemed essential by community decision-makers to offset the perceived higher risks, and to rebuild trust (Carroll et al., 2019; Claw et al., 2018; Sandoval et al., 2012). Moreover, in moving beyond re-enacting and re-enforcing models of extractive research that prioritize colonial epistemologies, mental health research should proactively support application of Indigenous knowledges within research by Indigenous Peoples (Fish & Gone, 2024). The focus of this study is to assess the levels of reported community engagement in research, as well as the “context relevance” of the recommendations represented in peer-reviewed literature utilizing a previous scoping review (Bryant et al., 2022) of research with Indigenous Peoples worldwide that centered on cognitive impairment and dementia.
Indigenous lens on community engagement
Broadly, community engagement includes how involved the population of focus is within the research approach and analysis. However, Indigenous health and research priorities, epistemologies, and values differ from non-Indigenous research paradigms (Harfield et al., 2020; Huria et al., 2019; Redvers et al., 2023). For example, non-Indigenous research paradigms may simply be concerned with recruiting adequate numbers of diverse participants so that research findings are properly powered and generalizable to some broader population. However, solely attempting to increase participation in research among Indigenous Peoples does not reflect respect for Tribal sovereignty or relationships and is unlikely to be effective given the need to rebuild community trust (Carroll et al., 2019; Claw et al., 2018). This practice still imposes non-Indigenous research methods and misses the point that little is currently known about Indigenous perspectives and knowledges about dementia and dementia care (Fish & Gone, 2024; Hulko et al., 2010; Racine et al., 2021). Indigenous community engagement is both possible and necessary for creating culturally-safe and scientifically-sound interventions and research designs that reflect Indigenous research methods, epistemologies, and values (Harfield et al., 2020; Huria et al., 2019; Walls et al., 2019).
Much has been written about approaches to community engagement with marginalized populations that aim to reduce power differentials in research between researchers and “the researched” and lead to better health outcomes for communities (Hicks et al., 2012; Wallerstein & Duran, 2010). Among various community-engaged approaches with Indigenous Peoples, Tribally-Driven Participatory Research (TDPR) (Mariella et al., 2009) represents the most engagement. Mariella et al. (2009) lay out the principles, tools, and methods of this approach and highlight the importance of relevance of research to Tribal Peoples stating, “Ultimately, tribes are further empowered by TDPR in which the information, analysis and outcomes are well understood, meaningful and provide increased ability to improve people’s lives” (p. 49). In this study, we assessed community engagement and context relevance of recommendations as reported in a body of peer-reviewed literature on the subject of dementia within Indigenous populations worldwide.
Understanding context relevance
To our knowledge “context relevance” has not been clearly defined in Indigenous health research to date. The meaning of “relevance” for health research is also not standardized (Dobrow et al., 2017). However, theoretical and practical “relevance” in health research was unpacked by Dobrow and colleagues (2017), and their recommendations for assessing relevance were used in this study. Context refers to the perspective of decision-makers or users of research, which for our purposes are both researchers and Indigenous communities, whose perspectives may differ (Bainbridge et al., 2015) because of how people value and interpret benefits. “Context relevance” in Indigenous health thus means more than “benefits” or “usability”, though those are aspects. To illustrate one such perspective, according to Harfield et al. (2020),“To provide the most benefit, research must be conducted respectfully and appropriately, occur in equal partnership with Aboriginal and Torres Strait Islander peoples and communities, and result in meaningful findings that are translated into policy and practice.” For the purposes of this review, we defined “context relevance” as “the benefits, usability, and respectful conduct of research from the perspective of Indigenous communities.” To appraise context relevance we focused on assessing the applicability of discussion and recommendations provided by research teams in peer reviewed publications. Broadly, this appraisal is inter-subjective; that is, it is constructed from the perspectives of both researchers and research users (Dobrow et al., 2017). Another characteristic is that the relevance of recommendations to Indigenous communities will be assessed by decision makers, community members, and other users of the research. They will assess the relevance of the work and will critically review to ensure the authors understand their research in relation to other decision factors such as economics, culture, social trends, politics, etc. (Dobrow et al., 2017).
This study
This study aimed to explore use of two novel tools for assessing levels of “community engagement” and “context relevance” within published Indigenous dementia research. Additionally, we applied these two tools to assess previously identified peer-reviewed research to determine any potential relation between levels of reported community engagement, and presence of context relevance in recommendations. Our hypothesis was that research indicating higher levels of community engagement would produce recommendations with greater context relevance for Indigenous Peoples. To assess application of the tools and test the given hypothesis, we utilized an existing corpus of peer-reviewed literature on cognitive impairment and dementia conducted with Indigenous Peoples (Bryant et al., 2022).
Methods
To explore the presence of “community engagement” and “context relevance” in this body of work, we developed two scoring tools. The data used to refine the tools was provided by a recently published scoping review. This already-published scoping review of 76 articles featured research on cognitive impairment and dementia among Indigenous Peoples worldwide conducted between 2000 and 2021 (Bryant et al., 2022). In their review, and thus in the current study, Indigenous Peoples were understood as people from any Indigenous population worldwide. In this paper, we use the terms Indigenous and Tribal interchangeably, while recognizing they may have different meanings in other settings. After developing the Community Engagement Scoring Tool and Context Relevance Scoring Tool we employed semi-structured deductive coding (Tolley et al., 2016) to assess the 76 articles previously summarized by Bryant et al. (2022). We coded for community engagement across the entirety of each article; context relevance measures were assessed within the recommendations that occurred in the abstract, discussion, and conclusion sections. All articles contained recommendations for coding.
Indigenous engagement
We conducted secondary data analysis of a pre-existing recently published scoping review spanning research with Indigenous Peoples worldwide. Our aims were to illuminate a pattern in research activities and reporting rather than make inferences about a specific population’s health. Thus, institutional review board and/or Tribal government approval were not required. Four of the five authors of this study are Indigenous researchers and one author is a non-Indigenous ally. Collectively, the authors represent over 100 years of related experience in research collaboration, lived experience, and employment with and within a variety of Indigenous community contexts in the U.S., Samoa, and Canada.
Measurement
Community Engagement Scoring Tool
Development of community engagement scoring tool.
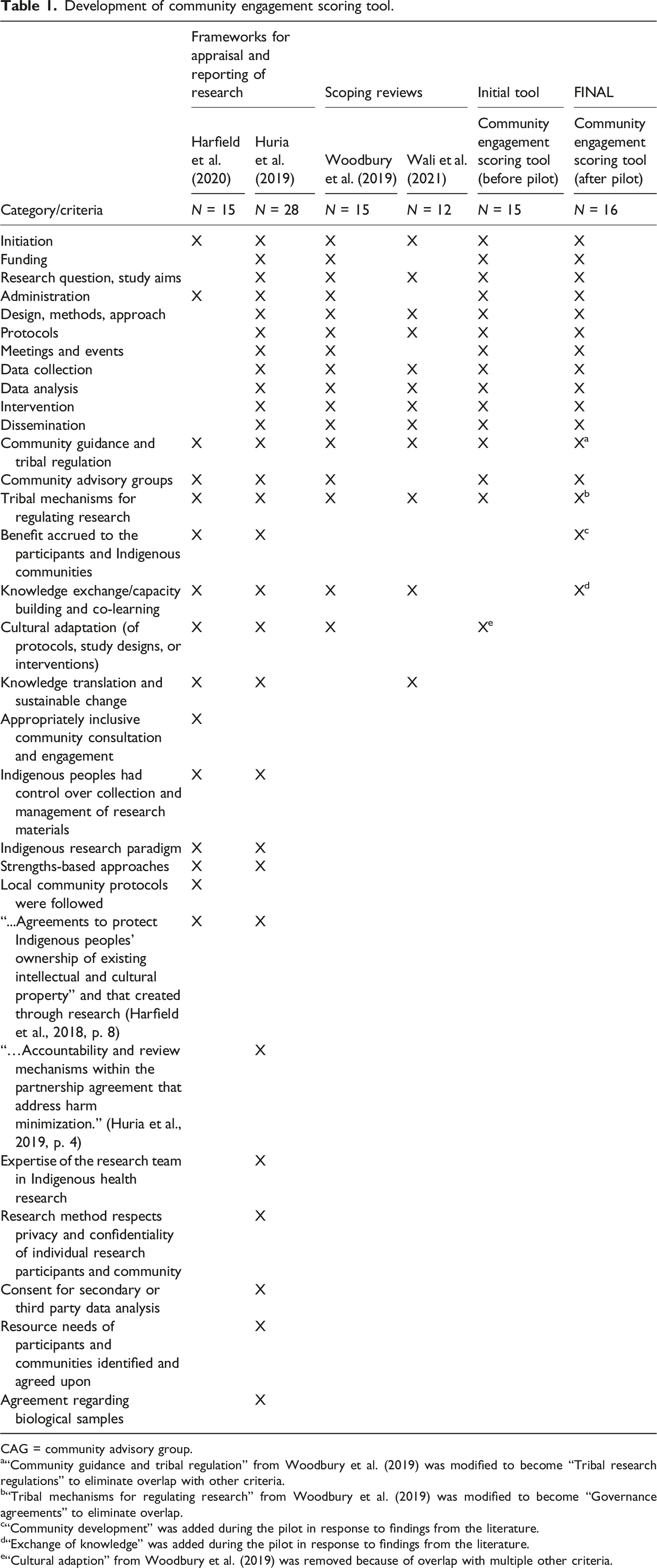
CAG = community advisory group.
a“Community guidance and tribal regulation” from Woodbury et al. (2019) was modified to become “Tribal research regulations” to eliminate overlap with other criteria.
b“Tribal mechanisms for regulating research” from Woodbury et al. (2019) was modified to become “Governance agreements” to eliminate overlap.
c“Community development” was added during the pilot in response to findings from the literature.
d“Exchange of knowledge” was added during the pilot in response to findings from the literature.
e“Cultural adaption” from Woodbury et al. (2019) was removed because of overlap with multiple other criteria.
We then created definitions for each category (i.e. criteria) using the descriptions from the scoping reviews by Woodbury et al. (2019) and Wali et al. (2021). We piloted the initial tool (15 measures of community engagement) on 21 of the articles that were part of our sample from the scoping review by Bryant et al. (2022). During the pilot, we adjusted the categories as follows: we added two categories, removed one, and modified two. The new categories added were “community development” and “exchange of knowledge,” which were added in response to findings from the literature. Subsequently, “cultural adaption” from Woodbury et al. (2019) was removed because of overlap with multiple other categories. The category, “community guidance and tribal regulation” from Woodbury et al. (2019) was modified to become “Tribal research regulations” and redefined to eliminate overlap with other categories. The definition of the category, “Tribal mechanisms for regulating research” from Woodbury et al. (2019) was also modified and renamed to “governance agreements” to eliminate overlap. One category that met our original test for inclusion, “sustainability: knowledge translation and sustainable change for policy or practice,” from three of the sources (Harfield et al., 2020; Huria et al., 2019; Wali et al., 2021) was not included because it overlapped with our Context Relevance Scoring Tool - Applicability. Twelve other categories were not included because they were only present in the frameworks and not in the scoping reviews. See Table 1 which identifies the final 16 criteria applied and where they appear in the extant literature.
Definitions of the criteria for community engagement and context relevance in health research with Indigenous Peoples.
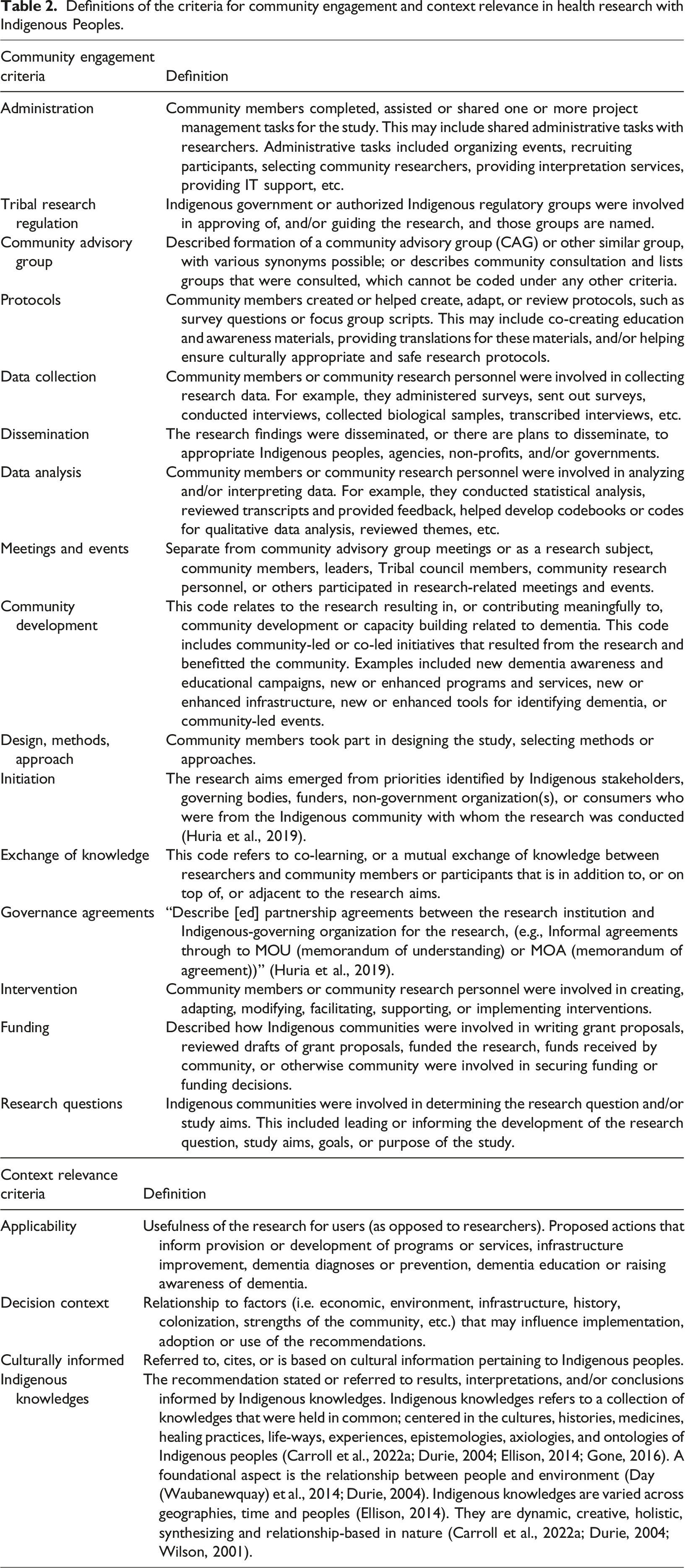
Table 2 displays a list and abridged definition of the 16 criteria for community engagement and the 4 criteria for context relevance. The full tools are available in Supplemental File 1. An important definition is that of “community” which appears in many of the criteria. For the purpose of this research, “community” is “a group of people living in the same place or belonging to the same language group or having a particular characteristic in common, at an organizational, local, state or national level” (Harfield et al., 2018, p. 7).
Context Relevance Scoring Tool
To develop the Context Relevance Scoring Tool we employed three key considerations for research relevance as defined by Dobrow et al. (2017). The aim of that work was to improve understanding of health research relevance by exploring it from both theoretical and practical perspectives while also outlining key considerations for measuring relevance. The three key considerations included: 1. Applicability of the results to community: This “considers both instrumental versus non-instrumental uses of research” (Dobrow et al., 2017, p. 9.) An example of an instrumental use of research in dementia was the development of the Kimberly Indigenous Cognitive Assessment, a diagnostic tool (LoGiudice et al., 2006). Non-instrumental uses of research were illustrated by the findings in Hulko et al. (2010, p. 335), “results lend support for efforts to revive and promote the role of Elders as educators and healers through traditional storytelling sessions…”. 2. Decision context for the research: This includes considerations of “a wide range of political, legal, media, economic and other contextual information, interactions and experiences, as well as prevailing organisational governance, leadership, culture and values” which all serve to inform research users’ decision-making about taking actions (Dobrow et al., 2017, p. 6). 3. Culturally informed recommendations: The research must “align with an intersubjective understanding of relevance” to the community in question (Dobrow et al., 2017, p. 9).
Because we aimed to use this tool specifically for research conducted with Indigenous Peoples, we added a fourth metric to the tool for context relevance: “Indigenous knowledges.” Recommendations met this criterion if they stated or referred to results, interpretations, and/or conclusions informed by Indigenous knowledges. While not seeking to define Indigenous knowledges, we created a criterion based on a literature review. Indigenous knowledges for this study meant knowledges that are held in common; centered in the cultures, histories, medicines, healing practices, life-ways, experiences, epistemologies, axiologies, and ontologies of Indigenous Peoples (Carroll et al., 2022a; Durie, 2004; Ellison, 2014; Gone, 2016). A foundational aspect is the relationship between people and environment (Day (Waubanewquay) et al., 2014; Durie, 2004). Indigenous knowledges are varied across geographies, time and Peoples (Ellison, 2014). They are dynamic, creative, holistic, synthesizing and relationship-based in nature (Carroll et al., 2022a; Durie, 2004; Wilson, 2001). This criterion differed from “culturally informed” in that recommendations included the terms or were derived from the meaning given above for “Indigenous knowledges” or a synonym (i.e. “Traditional Knowledge”, “Māori Knowledge”).
Each of the four metrics of context relevance (applicability, decision context, culturally informed, and Indigenous knowledges) were measured on a three-point scale. Articles were scored as “low” (score = 1), “medium” (score = 2), or “high” (score = 3). This is in alignment with guidance for indicator development in program development from the Centers for Disease Control and Prevention (US DHHS CDC, 2011, pp. 56–57). If all four criteria were met at a “high” level, an article would receive a score of 12 for context relevance. If multiple segments of text were coded in relation to one of the four metrics, and each segment received a different score, the highest level attained determined the final score. For example, if two recommendations were identified as having “applicability” and one received a low rank (1) and one a high rank (3), the score for “applicability” would be 3. The scores from each of the four criteria were summed to get a final context relevance score for each study, up to a score of 12.
Article selection
A scoping review by Bryant et al. (2022) identified the most recent, comprehensive corpus of articles about cognitive impairment and dementia in Indigenous populations, which included articles published between January 1, 2000 and December 31, 2021. We excluded two articles from the corpus reviewed by Bryant et al. (2022) because: (1) it was not possible to identify who the Indigenous participants were (Wiese et al., 2021) and (2) the relevant information was not provided (Martindale-Adams et al., 2017). Thus, the total number of articles included in this analysis was 74.
Deductive coding and tool scoring
We employed semi-structured deductive coding (Tolley et al., 2016) based on the two scoring tools. We used MAXQDA 2022 (Verbi Software., 2022) for qualitative coding. Code memos clearly defined each criterion to maintain consistency.
The primary coder (TK) read all 74 publications, highlighted recommendations, and then coded the recommendations for context relevance and corresponding levels of evidence. “Recommendations” refers to complete thoughts concerning research findings with respect to applications, implications, usefulness, or future research directions. Only recommendations in the abstract, discussion, or conclusion sections were included in scoring. While coding, TK refined definitions through an iterative process to clarify differences among codes and levels.
Following analysis related to context relevance, the primary coder highlighted all community engagement segments and indicated if each of the criteria were, or were not, met (yes = 1/no = 0). Single excerpts from a publication could have multiple codes related to both context relevance and community engagement. When authors referred to other articles or reports, including grey literature, for detailed information about their studies, we included the additional information related to community engagement in our coding.
To mitigate confirmation bias, we first coded articles for context relevance. We then, without knowledge of the publication’s context relevance, assessed segments of each article coded for community engagement. As a check for reliability, three authors (TK, SS, and VT) utilized the developed codebook and scoring tools and applied them to five publications individually. Codes and scores were reviewed for agreement, and any disagreements were discussed. When the group came together, there were various metrics where we didn’t agree (due to user error); once we discussed these, we had no residual disagreement.
Cross-tabulation of community engagement and context relevance scores.
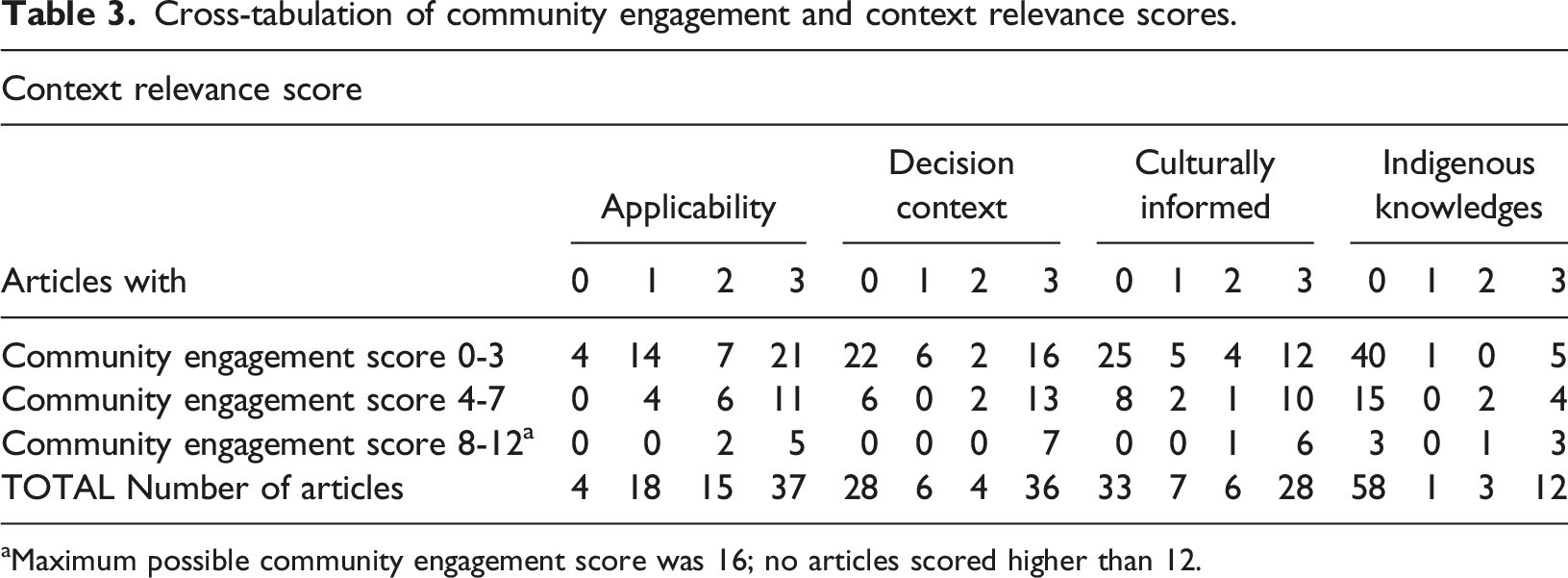
aMaximum possible community engagement score was 16; no articles scored higher than 12.
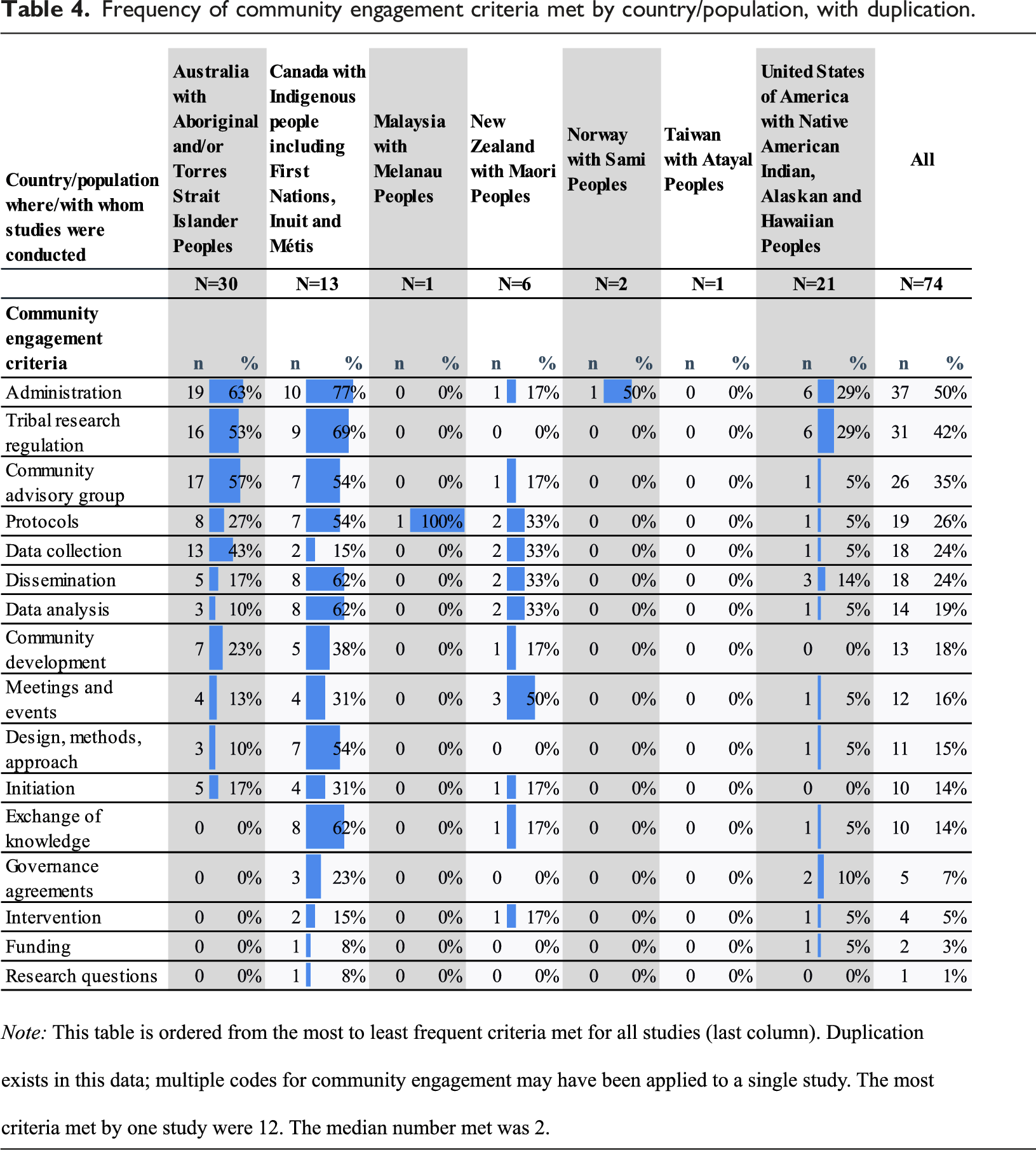
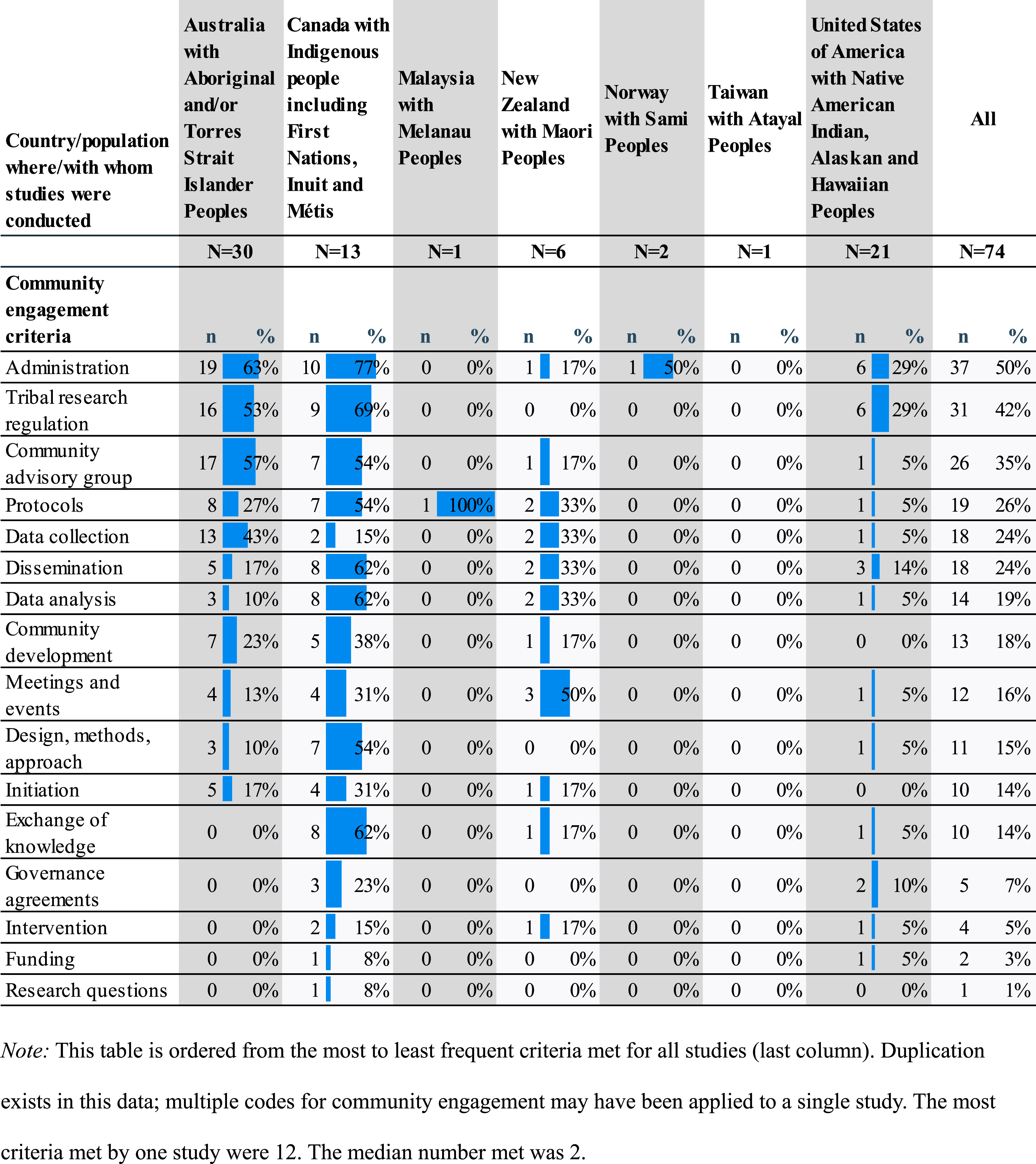
Frequency of community engagement criteria met by country/population, with duplication.
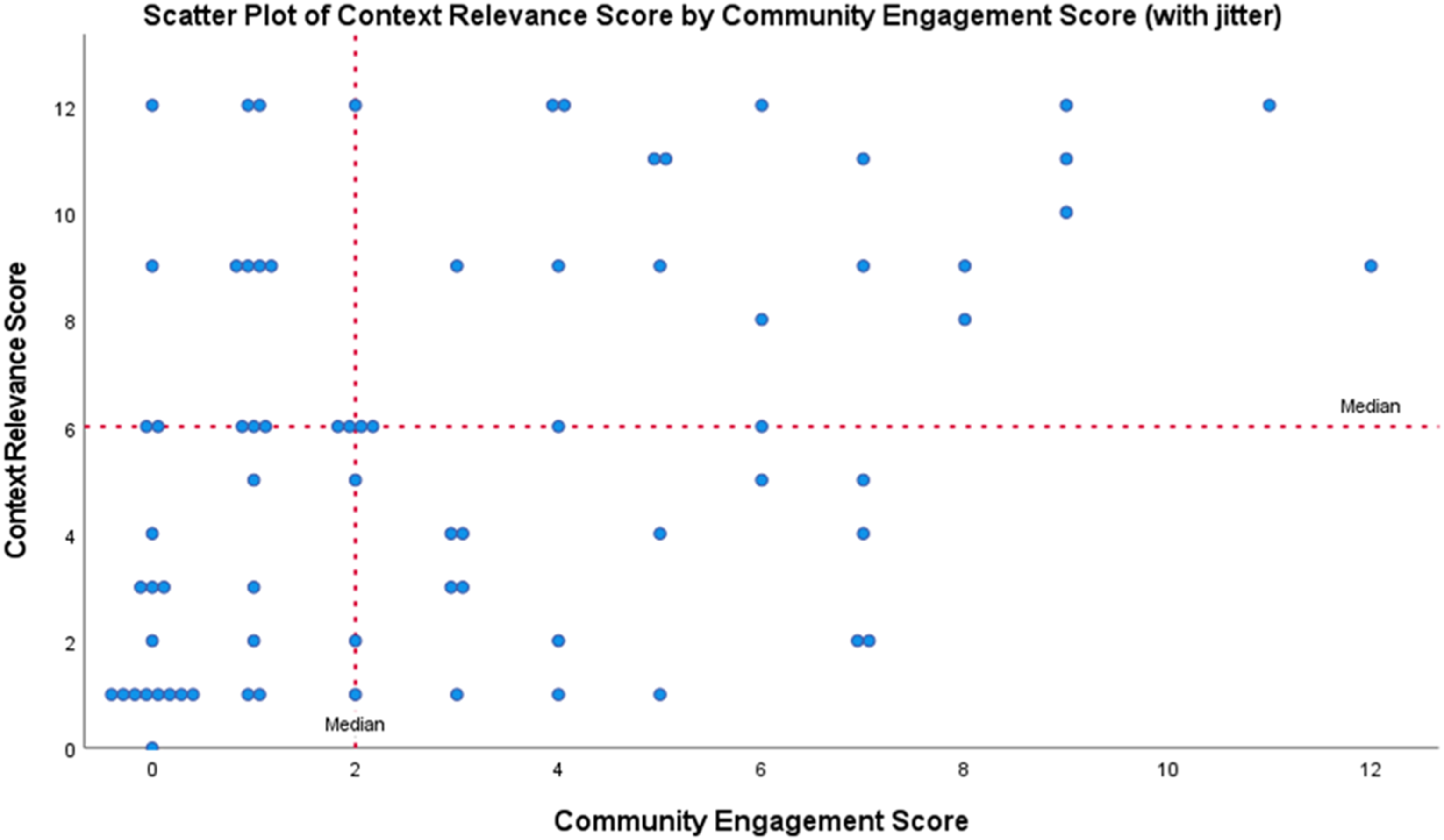
Plot of context relevance by community engagement.
Results
Seventy-six (76) documents that were analyzed by Bryant et al.’s (2022) scoping review were evaluated for inclusion in this study, and 74 documents were retained for analysis. Our research hypothesis was supported: Increased community engagement corresponded to increased context relevance of research recommendations (Figure 1). The data points in this figure were symmetrically “jittered” using SPSS version 28.0 (IBM Corp, 2021) for visual display purposes, so there is a random negligible but visible effect of scatter that results in rows of data points centered around their computed values. The left lower corner of the figure represents studies below the median for both community engagement and context relevance and includes 19 studies. A roughly similar amount (n = 18) appear in the upper corner and are above median for both measures. This is supporting evidence of a pattern whereby increased community engagement corresponded to increased context relevance in this body of literature. A Pearson correlation coefficient was computed to assess the linear relationship between community engagement and context relevance. There was a positive correlation between the two variables, r (72) = 0.421, p < .001 (two-tailed, α = .05).
As evident in Table 3, the relation between community engagement and context relevance was most evident when exploring articles that lacked both; except within the context relevance metric of applicability. For example, 40 articles with a score of 0–3 in community engagement had a score of 0 for Indigenous knowledges (context relevance). Similarity 25 and 22 articles, respectively, received the same measurement (0–3) for community engagement and culturally informed (score = 0) and decision context (score = 0) respectively.
Community engagement
Among the 74 articles included in this study, 24% (n = 18) did not report any community engagement (Figure 1). The most frequent activities that were reported among the remaining articles (Figure 2) were administration accommodation (n = 37, 50%); Tribal research regulation (n = 31, 42%); and being guided by a community advisory board (n = 26, 35%). About one quarter of studies included community in creating protocols (n = 19, 26%) or in data collection or dissemination (n = 18, 24%). Number of articles by metric of community engagement.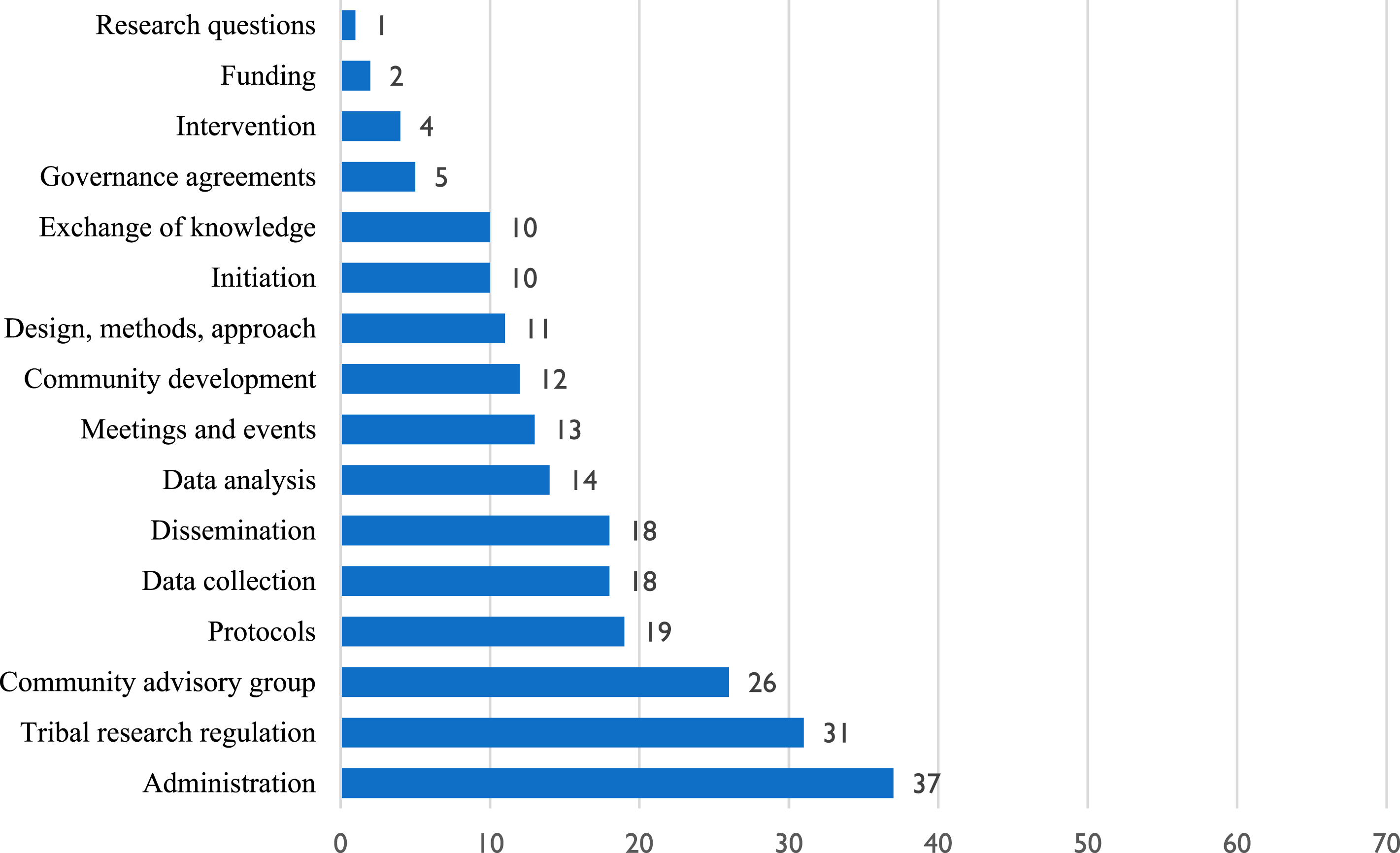
Very few studies reported including community in the pre-research stages of initiating the research (n = 10, 14%), helping to write grants to secure funding or providing funding (n = 2, 3%), and developing research questions or specific aims (n = 1, 1%) (Figure 2). About 1 in 7 (n = 11, 15%) involved communities in the designing the research, methods, or approach.
Level of community engagement differed by the community of study. Studies conducted with First Nations, Inuit, and Métis populations in Canada and with Australian Aboriginal and/or Torres Strait Islander Peoples documented higher community engagement than those with other Indigenous peoples (Table 4). In studies from the USA, researchers primarily included Indigenous communities for administrative purposes (i.e., helping to recruit participants) and when obtaining Tribal research approval. Each of these occurred in less than one third of cases in the United States. Research in New Zealand with Māori Peoples varied in community engagement scores up to a 6 and incorporated some less common activities such as meetings and events beyond the research team. Research in Malaysia, Taiwan, and Norway reported very little to no community engagement. However, there was a high context relevance of recommendations in the two studies reviewed in Norway (scores of 9 and 12).
Context relevance
Applicability
All but four studies presented recommendations that included a component of applicability (Table 3). Half of the studies (n = 37) made a recommendation that was rated as “high” for applicability; 20% (n = 15) were ranked “medium,” and 24% (n = 18) “low.”
Decision context
Close to half of the studies were ranked “high” for decision context (n = 36, 49%). However, almost an equal number, about 38% (n = 28) did not offer recommendations with any decision context included.
Culturally informed
Approximately 38% (n = 28) of articles presented recommendations rated “high” for being culturally informed. However, similar to decision context, nearly half of the studies (45%, n = 33) did not present any culturally informed recommendation.
Indigenous knowledges
Only 16 of the 74 articles that were focused on cognitive decline and dementia among Indigenous Peoples included a recommendation informed by Indigenous knowledges. Among those that did include Indigenous knowledges, 12 of them scored “high” for their inclusion.
Overall
Among all articles, the most frequent total context relevance score (e.g., sum of the four sub-scores) was a score of 1 (n = 14, 19%) (Figure 1). Articles with lower scores (0–3) accounted for over one third (n = 27, 36%). Articles with mid-range scores of between 4 and 7 accounted for roughly another one third (n = 22, 30%); and higher scoring articles (8–12) made up the remaining approximately one third (n = 25, 34%). A single article, which presented a case study and examined incidence rate in Indigenous Australians of a rare disease (Creutzfeldt-Jakob disease), received an overall context relevance score of zero (Panegyres et al., 2021).
Discussion
The aim of this study was to explore use of two novel tools for assessing community engagement and context relevance in Indigenous health research while also testing the hypothesis that research with higher levels of reported community engagement would produce recommendations with greater context relevance for Indigenous Peoples. We accomplished this by analyzing a corpus of peer-reviewed literature on cognitive impairment and dementia conducted with Indigenous Peoples.
Application of the tools and analysis of the scoring demonstrated a pattern whereby increased reported community engagement corresponded to increased context relevance in this body of literature (Figure 1). This was most evident when exploring publications that lacked both, as opposed to those where both were present and scoring high. It is thus important to impart knowledge and skills for creating and sustaining research partnerships that involve Indigenous communities in meaningful ways to create contextually relevant research.
Community engagement
Though there were 16 measures of community engagement, no published article on dementia and cognitive impairment among Indigenous Peoples included all elements of engagement. In fact, no article met more than 12 of the identified criteria. When communities were more actively engaged in the research (a higher score for community engagement), the research was frequently occurring with First Nations, Inuit, and Métis populations in Canada, or with Australian Aboriginal and/or Torres Strait Islander Peoples. Research with Alaska Native, American Indian, and Native Hawaiian Peoples in the USA stood out for its comparative lack of meaningful community engagement.
Government recognition of Indigenous rights and subsequent advocacy among international entities (i.e. United Nations) and academics for Indigenous rights in research may have opened doors for researchers in Australia, New Zealand, and Canada to engage communities in deeper and more authentic ways compared to in the USA (Government of Canada, C. I. of H. R, 2005; National Health Medical Research Council, 2018; United Nations (General Assembly), 2007; Hudson & Russell, 2009; Smith, 1999). On the other hand, codes of ethics for Indigenous participatory research and data ownership date back to the early to mid-1990s (Harding et al., 2012, p. 7) in the USA, so there has been awareness of these issues for about three decades. If the goal is to increase the benefits of research on dementia to participants and their communities, more attention must be paid to community engagement in the United States and other countries where it was reportedly lacking in our study.
Obtaining consent from a Tribal/Indigenous research board, government council, or other officially authorized entity and forming a community advisory group were the second and third most common community engagement tactics employed. Seeking official approval, such as through a Tribal research review board and forming community advisory groups are common, tangible, and often-cited structures in community-based participatory research and related approaches (Gittelsohn et al., 2020; Lonczak et al., 2013; Mariella et al., 2009). Tribal/Indigenous research review boards (Around Him et al., 2019; Buffalo et al., 2019) are growing in numbers and government research ethics guidelines often stress obtaining community consent and involving community as advisors, for both urban and rural locations (Haozous et al., 2021; Harding et al., 2012).
Despite 42% of the studies obtaining approval from Tribal/Indigenous authorities, only 10% of studies in the United States, 23% in Canada, or 7% overall, reported having signed a governance agreement. This finding suggests more attention to governance agreements may be needed in the future for cognitive impairment and dementia research among Indigenous Peoples. This attention will align research practice with respect for Tribal sovereignty and Indigenous community self-determination (Carroll et al., 2022a, 2022b). Mentorship and capacity building is needed to enable researchers to facilitate governance agreements, and for Indigenous communities to develop agreements that meet their goals and values.
While it is encouraging that half of the studies reported at least a minimal form of community engagement, many are calling for a much greater degree of involvement on the part of Indigenous Peoples in defining the research agenda and leading research (Carroll et al., 2022a; Redvers et al., 2023). In this assessment, only one article involved community in pre-research stages, as in development of the research questions, and only ten of 74 involved the community in the initiation of the research. Similarly, our analysis revealed that only two publications reported including the community in funding decisions.
Interestingly, climate science with Indigenous communities in the polar region offers a detailed look at how a set of Indigenous communities in the Arctic view the importance of involvement in the pre-research stages. There are obviously different approaches and methods in health research and climate research. Even so, the concerns and recommendations are applicable. A letter from four Indigenous leaders representing multiple regions in the Arctic to the National Science Foundation (Bahnke et al., 2020) articulated the harmful effects, missed opportunities, and costly duplication of efforts that were occurring in their region due to paucity of their communities’ involvement in the pre-research stages of investigations. This letter could serve as a model for researchers and funding entities for creating and supporting research in dementia with high context relevance.
For example, two recommended criteria for assessing grant applications were, “Does the project address a top community need or priority?” and “Does the project’s implementation methodology address the root cause of the problem and produce information that will lead to solutions?” While much as been written on the topic of how to effectively engage with communities in research and barriers to engagement (Lewis & Boyd, 2013; Lonczak et al., 2013; Mohammed et al., 2012), our results show that there remains a need to expand upon past work in health research with Indigenous communities to create effective Requests for Proposals (RFPs) and evaluation metrics for engagement and relevance to communities.
Context relevance
Seventy (70) of the 74 publications had some level of discussion that addressed applicability of the results to the community in question. Of the four metrics related to context relevance, this was the only in which most of the publications included the metric. However, within this metric, only 50% received a high rating. Similarly, 49% of the publications scored high for decision context. Possible reasons for these findings are that researchers may be most familiar with incorporating applicability and decision context into recommendations because these align with funder requirements for “impact statements.”
In general, lower community engagement scores corresponded with scoring zero (0) for decision context, culturally informed, and Indigenous knowledges. On the other end of the spectrum, all publications that scored “high” for decision context (n = 7) also scored higher for community engagement. Incorporating decision context requires detailed understanding of the factors affecting adoption of recommendations, as may be acquired by engaging with the community. This same explanation may apply to the other two criteria because more in-depth understanding of community is required to create recommendations that are culturally informed and incorporate Indigenous knowledges. Community engagement, including early stages in research development, is often needed to provide effective knowledge exchange between academic researchers and community-embedded researchers, leading to more relevant outcomes for communities (Harfield et al., 2020; Huria et al., 2019; Mariella et al., 2009).
Only 1 in 5 studies integrated Indigenous knowledges into recommendations; perhaps due to the substantial trust required on the part of communities. In a research context, trust develops within longer term relationships and requires mutually beneficial engagement (Whitesell et al., 2020). According to Simonds and Christopher (2013, p. 2189), “In Native American communities, knowledge is sacred and access to it must be earned.” Besides this, there may be unique barriers to community engagement for research with Indigenous Peoples relating to cognitive impairment and dementia. For example, past research harms and lack of cultural safety in clinical settings experienced by Indigenous Peoples could be a barrier (Chakanyuka et al., 2022; Hamilton et al., 2021). In particular, there may be heightened concern about studies, diagnoses, and interventions related to mental health that could result in removal from one’s community to an institution (Gone, 2008; Jacklin et al., 2015; Pace, 2020). Further, even diagnosis of cognitive impairment or dementia could be perceived as an assimilation practice that is unwanted, or pathologizing what some Indigenous Peoples conceive of as normal and healthy aging (Duran, 2019; Hulko et al., 2010; Johnston et al., 2020). While it would be inappropriate to make assumptions about all researchers, just as pan-Indigeneity is inaccurate and harmful, the relative lack of reported community engagement in this body of research suggests there may be barriers to engagement for community (i.e. paucity of trust, historical harms, wariness of cultural brainwashing) and to researchers. Further research should explore knowledges, attitudes, beliefs, and behaviors among researchers who conduct studies in Indigenous communities to better understand motivations and obstacles to engaging with communities who are Indigenous and to designing research to be more contextually relevant.
Limitations
A limitation of this study is that more recent research was not included. An additional 2,157 documents met approximately the same search criteria during the recent 18-month period from January 1, 2022 to June 30, 2023. This compares to 13,009 found by Bryant et al. (2022) for the 12 years prior (2000–2021). We also relied on published literature for coding community engagement and context factors. Actual partnership building efforts and collaborative work among teams represented in this literature may not always appear in written work for a variety of reasons, including space limitations in journals, explanations of partnerships in earlier publications, or conventional formulaic approaches to publishing and academic writing that do not always encourage verbose methodological or epistemological explanations. On the other hand, we did include community engagement mentioned in earlier publications when explicitly referred to for additional study details.
We did not assess whether and how engagement and relevance related to overall research quality. It is plausible that responsivity to local guidance or control alters research designs in ways that limit findings. The opposite could also be true. Next steps would be to assess this directly using an evaluation of research quality for each study.
We also did not include grey literature or creative research outputs (infographics, videos, etc.) in the current study, which may be more common formats distributed within communities and may allow space to discuss engagement and to elaborate on recommendations. Given these factors, it is plausible that our findings underestimate community engagement in Indigenous dementia research. Our scoring tools do not fully reflect the best practices for research with Indigenous Peoples as laid out by other researchers. Some examples include applying the CARE Principles for Indigenous Data Governance (Carroll et al., 2020); specifying how written research agreements protect intellectual property and potential financial benefits (Huria et al., 2019); and, addressing how the research takes a strengths-based approach (Tuck, 2009). Future work should consider how these and other aspirational goals are being achieved and how researchers are overcoming barriers to expanding relevance of research to Indigenous Peoples.
Conclusion
Two novel tools were developed to assess community engagement and context relevance within research involving Indigenous peoples. These two tools—Community Engagement Scoring Tool and Context Relevance Scoring Tool—were based in theory and systematically applied. These tools may be useful for assessing other bodies of research with Indigenous Peoples in conjunction with other tools for measuring research quality. Future research should examine if and how studies with high community engagement and high context relevance led to applications of the research for improving Indigenous health. Ideally, journals will provide sufficient space to enable complete reporting of community engagement for the purpose of assessing research quality from an Indigenous perspective (Harfield et al., 2018; Huria et al., 2019).
This study demonstrates a connection between ample community engagement and results that are relevant for community. Population health studies aiming to be highly relevant to Indigenous communities should include communities early and in multiple ways throughout the entire research process.
Supplemental Material
Supplemental Material - Increased community engagement of Indigenous Peoples in dementia research leads to higher context relevance of results
Supplemental Material for Increased community engagement of Indigenous Peoples in dementia research leads to higher context relevance of results by Tonya M. Kjerland, Shawnda Schroeder, Va’atausili Tofaeono, Melissa Walls, and Joseph P. Gone in Dementia.
Footnotes
Acknowledgements
We would like to acknowledge the technical support of librarian Devon Olson, School of Medicine & Health Sciences Library Resources, University of North Dakota.
Author contributions
The authors confirm contribution to the paper as follows: Tonya M. Kjerland: Conceptualization, Methodology, Validation, Formal Analysis, Investigation, Writing – Original Draft, Visualization, Project Administration. Shawnda Schroeder: Methodology, Validation, Writing – Review & Editing. Va’atausili Tofaeono: Validation, Writing – Review & Editing. Melissa Walls: Conceptualization, Writing – Review & Editing, Supervision, Funding Acquisition. Joseph P. Gone: Conceptualization, Writing – Review & Editing, Supervision, Funding Acquisition.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided by the Robert Wood Johnson Foundation. The views expressed here do not necessarily reflect the views of the Foundation.
Ethical statement
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online. Scoring tools and criteria exemplars are available in the online version as Supplemental File 1 and Supplemental File 2.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.