
Abstract
Introduction
Psychosocial dementia interventions may be less effective when used with populations for whom they were not initially intended. Cultural adaptation of interventions aims to increase effectiveness of interventions by enhancing cultural relevance. Use of theoretical frameworks may promote more systematic cultural adaptation. The aim of this review was to provide a comprehensive synthesis of published cultural adaptation frameworks for psychosocial interventions to understand important elements of cultural adaptation and guide framework selection.
Method
Five scientific databases, grey literature and reference lists were searched to January 2023 to identify cultural adaptation frameworks for psychosocial interventions. Papers were included that presented cultural adaptation frameworks for psychosocial interventions. Data were mapped to the framework for reporting adaptations and modifications to evidence-based interventions, then analysed using thematic synthesis.
Results
Twelve cultural adaptation frameworks met inclusion criteria. They were mostly developed in the United States and for adaptation of psychological interventions. The main elements of cultural adaptation for psychosocial interventions were modifying intervention content, changing context (where, by whom an intervention is delivered) and consideration of fidelity to the original intervention. Most frameworks suggested that key intervention components must be retained to ensure fidelity, however guidance was not provided on how to identify or retain these key components. Engagement (ways to reach and involve recipients) and cultural competence of therapists were found to be important elements for cultural adaptation.
Conclusions
Comprehensive frameworks are available to guide cultural adaptation of psychosocial dementia interventions. More work is required to articulate how to ensure fidelity during adaptation, including how to identify and retain key intervention components.
Keywords
Introduction
Psychosocial interventions can improve quality of life, delay functional decline, and reduce depression in people with dementia and their families (Bennett et al., 2019; Laver et al., 2016; Watt et al., 2021). Psychosocial interventions may involve use of psychological, behavioural and/or social approaches or strategies to improve individuals’ outcomes (England et al., 2015). However, a growing body of work has argued that interventions developed for one population may not be effective when directly applied to other cultures or populations (e.g., Cardemil, 2010; Castro et al., 2010; La Roche & Christopher, 2009; Lau, 2006). Developing a new intervention for each new population can be costly and time consuming (Castro et al., 2010).
One approach to address this issue is cultural adaptation, “the systematic modification of an evidence-based treatment (EBT) or intervention protocol to consider language, culture, and context in such a way that it is compatible with the client’s cultural patterns, meanings, and values” (Bernal et al., 2009, p. 362). Cultural adaptation of dementia interventions is increasingly conducted (e.g., Brijnath et al., 2022; Parker et al., 2022) and in particular should be considered when an intervention is found to be less effective with a new population (Cardemil, 2010). New populations may have different characteristics compared with the original intervention population or their response to the intervention may differ (Lau, 2006).
Cultural adaptation changes cultural sensitivity including both “surface level” changes (e.g., matched language and/or images in intervention materials) to increase acceptability and “deep structural” changes (e.g., incorporation of cultural values) to ensure intervention impact (Resnicow et al., 1999). For example, a skills training intervention for caregivers of people with dementia was adapted for Latino populations in the United States (US) to include resources in Spanish and English, bicultural workers to deliver the intervention, and increased use of visual aids and verbal activities to account for lower literacy levels (Gallagher-Thompson et al., 2003). Culturally adapted psychosocial interventions, including those for people with dementia, have been shown to be effective for minority groups in Western countries, and people from non-Western and lower-middle income countries (LMICs) (e.g., Arundell et al., 2021; Hall et al., 2016; James et al., 2021; Rathod et al., 2018)
The many challenges of cultural adaptation have been extensively documented and continue to be explored (Barrera & Castro, 2019; Cardemil, 2010, 2015, 2015; Castro et al., 2010; Miranda et al., 2005). Foremost is the “Fidelity-Adaptation Dilemma” (Castro & Yasui, 2017), describing the tension between delivery of evidence-based interventions as developed to ensure effectiveness and the need to address local population needs by making changes. Cultural adaptation specifically considers where there is intervention-population mismatch and makes purposeful changes that aim to increase the relevance and fit (Castro et al., 2010). However, this presents a risk that the intervention may be adapted in a way that decreases effectiveness (Cardemil, 2010). It has been suggested that fidelity can be maintained by strategic cultural adaptation that retains an intervention’s core theoretical components while making changes to ensure cultural relevance for the new population (Castro & Yasui, 2017). There are some examples of this with psychosocial interventions for people with dementia and their families; James and colleagues (2021) showed that evidence-based dementia interventions that retained the core therapeutic components of the intervention remained effective when adapted for local contexts, such as incorporating local language and customs, removal of reading and writing tasks or adding services such as blood pressure screening to increase attendance.
Researchers and practitioners can apply cultural adaptation frameworks to support transparent, replicable adaptation of dementia psychosocial interventions; these are defined as “a systematic way to carry out and document adaptations that can be useful for planning, replication, dissemination and translation” (Bernal et al., 2009, p. 364). Frameworks may be process models (i.e., directed steps for adaptation) or content-specific models (i.e., consideration of areas of the intervention that can be targeted for adaptation) or a combination of both (Ferrer-Wreder et al., 2012). Frameworks are designed to provide consistency and clarity in cultural adaptation research and to assist with real-world implementation.
As cultural adaptation research has increased over the past 20 years (Rathod et al., 2018), there has also been an increase in published cultural adaptation frameworks. Practitioners and researchers need guidance to select the appropriate framework for their intervention and populations (Rathod et al., 2018). Two recent reviews summarise available guidelines and frameworks for adaptation of health interventions (Escoffery et al., 2019; Movsisyan et al., 2019). Both reviews emphasised the important steps for adaptation: planning (gather information, assess the community, select the intervention, consult with stakeholders); conducting (decide what needs to be adapted then adapt the intervention) and testing (pilot, implement, evaluate). The engagement of the local community was identified as important for meaningful adaptation. From these reviews, the steps to guide adaptation are clear (i.e., planning, conducting, testing); they are included in “process model” cultural adaptation frameworks. It is less clear which aspects of the intervention should be considered for adaptation. Both reviews included cultural adaptation frameworks, but an in-depth exploration was out of scope.
The aim of this review was to provide a comprehensive synthesis of published cultural adaptation content-specific frameworks.
Specific questions were: • What frameworks for cultural adaptation of psychosocial interventions are publicly available and how have they been applied? • What are the main elements of cultural adaptation included in the identified frameworks? • What are the commonalities and differences across the frameworks?
Methods
The systematic review protocol was registered prospectively on the PROSPERO database (CRD42021266156). Reporting is according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (Page et al., 2021) (see APPENDIX for PRISMA checklist).
Eligibility criteria
Papers were included that discussed a new content-specific framework for cultural adaptation of face to face, psychosocial interventions. The search was not limited to empirical studies and included all paper types (systematic reviews, primary research papers, commentaries, etc.)
Included articles considered all of the following: 1) Cultural adaptation: the “the systematic modification of an evidence-based treatment (EBT) or intervention protocol to consider language, culture, and context in such a way that it is compatible with the client’s cultural patterns, meanings, and values” (Bernal et al., 2009, p. 362) 2) Psychosocial interventions: interventions with a focus on non-pharmacological approaches to improving (or reducing risk to) psychological, social and everyday functional abilities (England et al., 2015) 3) Frameworks: graphical or narrative representations of the cultural adaptation process (Ferrer-Wreder et al., 2012) a. Specifically, content-specific frameworks which target areas of an intervention that may need to be considered for adaptation (Ferrer-Wreder et al., 2012)
Articles were excluded if they focused on any of the following: 1) Theory of cultural adaptation, with no specified framework (e.g. Bernal et al., 2009; Castro et al., 2004; Domenech Rodriguez & Bernal, 2012; Ferrer-Wreder et al., 2012; Lau, 2006) 2) “Process model” frameworks that describe a series of pre-defined steps to conduct the adaptation (e.g., Aguirre et al., 2014; Fendt-Newlin et al., 2020; Hwang, 2009; Kumpfer et al., 2008; McKleroy et al., 2006; Perera et al., 2020; Wingood and DiClemente, 2008) 3) Application or validation of an existing framework without proposing any changes to the original framework (e.g., Naeem et al., 2019; Rathod et al., 2019) 4) Frameworks to develop culturally specific interventions, not for adapting an existing intervention (e.g., Hockley et al., 2019) 5) Validation or adaptation of standardised assessment tools rather than an intervention; and/or 6) Frameworks about adaptation of psychosocial interventions relating to technology or technological interventions (i.e., not face to face)
Information sources and search strategy
Concepts and search terms.
Note. All three concepts need to be included: cultural adaptation AND frameworks AND psychosocial intervention.
Selection process
Search results were exported into Covidence and duplicates were removed. Two reviewers (SD and either LFL or YHJ) independently screened titles and abstracts for eligibility. Abstracts not available in English were translated using google translation software. Inconsistencies were discussed until consensus reached. In case of disagreement, articles were included for full-text review. Full texts were reviewed against eligibility criteria by at two reviewers (SD and LFL). Again, consensus was reached on inclusion or exclusion.
Data extraction
Framework characteristics.
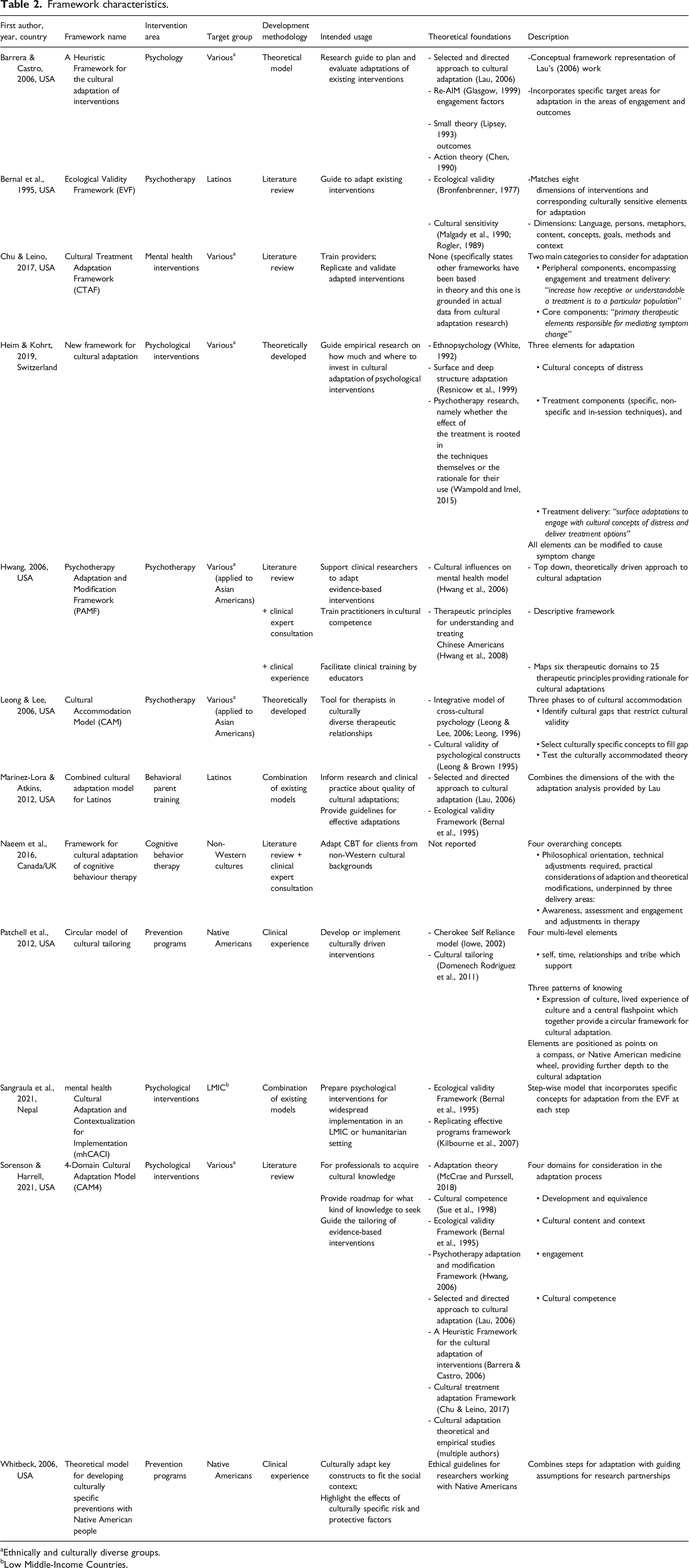
aEthnically and culturally diverse groups.
bLow Middle-Income Countries.
Narrative synthesis
A narrative approach to data synthesis was utilised: 1) conducting a preliminary synthesis, 2) conducting thematic analysis, 3) exploring concepts across papers, and 4) assessing the robustness of the synthesis (Popay et al., 2006).
Preliminary synthesis
The Framework for Reporting Adaptations and Modifications – Enhanced (FRAME) (Wiltsey Stirman et al., 2019) was used as the basis for preliminary tabulation of common adaptation elements identified in the cultural adaptation frameworks. FRAME was developed to support the systematic reporting of modifications to evidence-based interventions during intervention adaptation or implementation (Stirman et al., 2013; Wiltsey Stirman et al., 2019). It describes the different adaptation features: reasons for, the process, including what is modified and the nature of the modifications, and fidelity to the original intervention. SD initially tabulated the adaptation elements from each framework to FRAME, all authors independently reviewed the tabulation, and any disagreements were discussed as a whole group.
Thematic synthesis
Extracted data that did not map onto FRAME during preliminary synthesis were examined using thematic synthesis (Thomas & Harden, 2008). Each line of data extracted was coded by SD and themes developed in collaboration with all authors using a deductive approach to analysis based on cultural adaptation theory (e.g., Bernal et al., 2009; Cardemil, 2010; Lau, 2006). Coded data was cross-checked with original papers for context within each framework by SD and final accuracy of interpretation was discussed and agreed by all authors. Finally, two additional common cultural adaptation elements were identified; engagement and cultural competence (see Box 1 for definitions).
Box 1:
Definitions of adaptation elements
• • • • •
• • 1: Stirman et al., 2013, p. 2: Wiltsey Stirman et al., 2019, p. 3: Barrera & Castro, 2006, p. 4: Cross et al., 1989
Exploring concepts
Commonalities and differences between frameworks were explored by SD graphing the cultural adaptation elements identified in steps 1 and 2 (Popay et al., 2006) and all authors further analysing the data through thematic synthesis by developing analytic themes and grouping themes across frameworks (Thomas & Harden, 2008).
Assessing robustness of synthesis
Robustness of the synthesis was achieved by all authors examining, discussing and refining the analysis at each stage: preliminary synthesis, thematic synthesis, the identified adaptation elements, descriptions of each element and the synthesised analytic themes. Analysis was revised and finalised following critical reflection.
Results
Of the 2034 unique records identified through the database search (after duplicates removed), most were excluded (n = 1996) based on the title and abstract (see Figure 1). Thirty-eight full text articles were reviewed. Nine met the inclusion criteria (Barrera & Castro, 2006; Bernal et al., 1995; Chu & Leino, 2017; Heim & Kohrt, 2019; Hwang, 2006; Marinez-Lora & Atkins, 2012; Patchell et al., 2012; Sangraula et al., 2021; Sorenson & Harrell, 2021). Three additional eligible papers were found from hand searching reference lists of included papers (Leong & Lee, 2006; Naeem et al., 2016; Whitbeck, 2006). A total of 12 papers are included in this review. PRISMA flow diagram.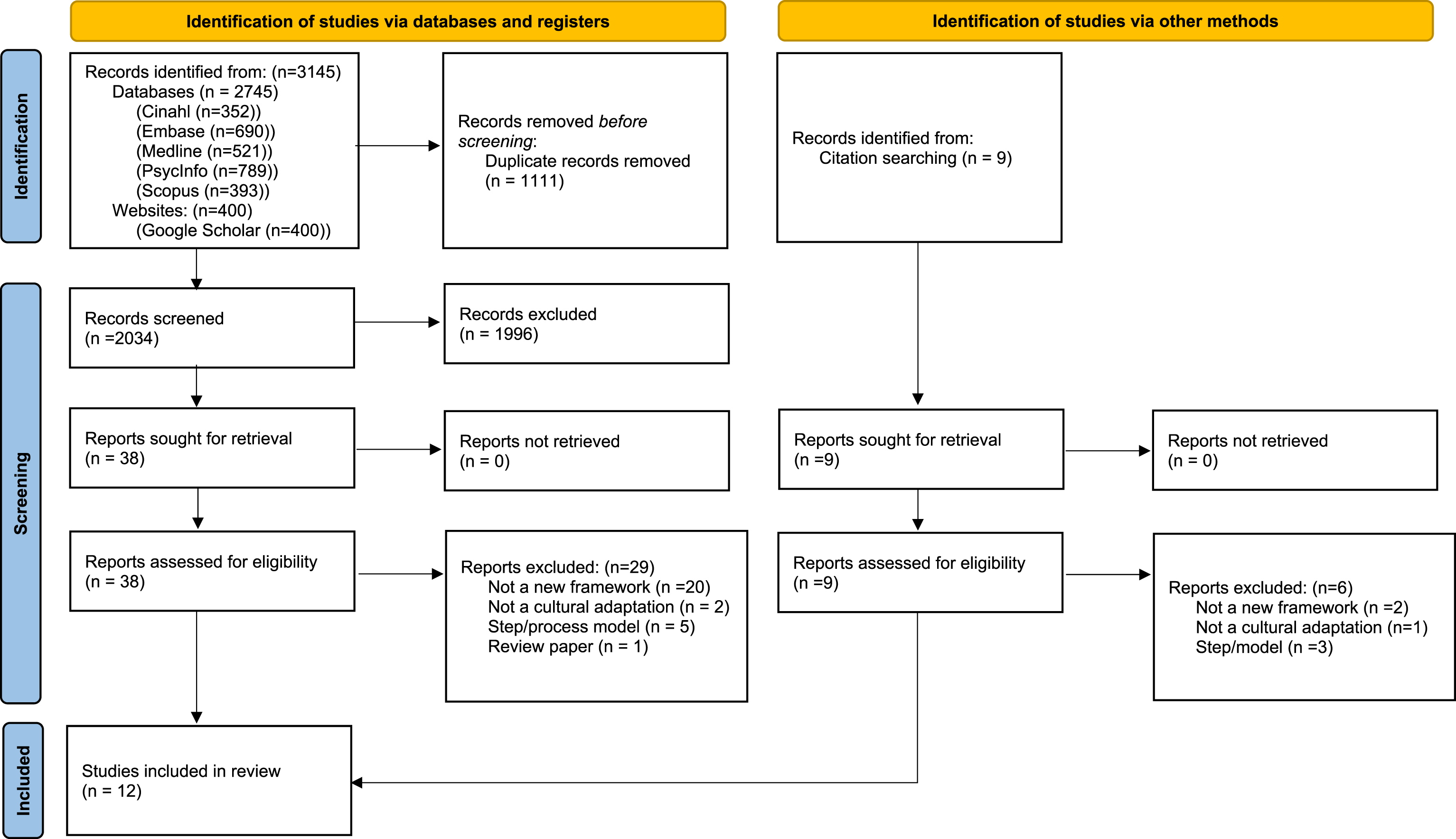
Characteristics and purpose of cultural adaptation frameworks
Included papers were published between 1995 and 2021. Most were from the USA (n = 9) (see Table 2). Most frameworks were for adaptation of non-specific psychological or mental health interventions (n = 8), others were for prevention programs (n = 2), behavioural parent training (n = 1) and one specifically for the adaptation of Cognitive Behavioural Therapy (CBT). No frameworks were specifically designed for dementia interventions. Six frameworks were developed for adaptation for any ethnic or cultural minority groups in a Western country, two frameworks were for adaptation for non-Western cultures or LMICs and four were for specific cultural groups in the USA (Latinos, n = 2; Native Americans, n = 2).
Most frameworks (n = 9) were primarily for application in guiding practitioners and local stakeholders through cultural adaptations (Bernal et al., 1995; Hwang, 2006; Leong & Lee, 2006; Marinez-Lora & Atkins, 2012; Naeem et al., 2016; Patchell et al., 2012; Sangraula et al., 2021; Sorenson & Harrell, 2021; Whitbeck, 2006). The other frameworks were applied in research: to test cultural adaptations (Barrera & Castro, 2006), validate adaptations (Chu & Leino, 2017) and to inform future empirical research (Heim & Kohrt, 2019). Three frameworks were also intended for clinical training (Chu & Leino, 2017; Hwang, 2006; Marinez-Lora & Atkins, 2012).
Commonalities and differences across frameworks
Theoretical foundations:
Frameworks had diverse theoretical foundations, most incorporating multiple theories (see Table 2). Some frameworks (n = 4) were derived from cultural adaptation theory (Barrera & Castro, 2006; Heim & Kohrt, 2019; Marinez-Lora & Atkins, 2012; Sorenson & Harrell, 2021), others (n = 3) from cultural sensitivity literature for a specific cultural group (Hwang, 2006; Patchell et al., 2012; Whitbeck, 2006) and one from cultural validity of interventions (Leong & Lee, 2006). Bernal et al. (1995) developed the Ecological Validity Framework (EVF) based on the premise that ecological validity is strengthened through cultural sensitivity of interventions; some frameworks (n = 3) drew on the EVF as their theoretical foundation (Marinez-Lora & Atkins, 2012; Sangraula et al., 2021; Sorenson & Harrell, 2021). The mhCACI (Sangraula et al., 2021) specifically drew on implementation theory. The varied theoretical foundations and development methodologies were reflected in how the cultural adaptation elements were defined and used, and the emphasis during the cultural adaptation process.
Elements considered during cultural adaptation:
Summary of included cultural adaptation elements.
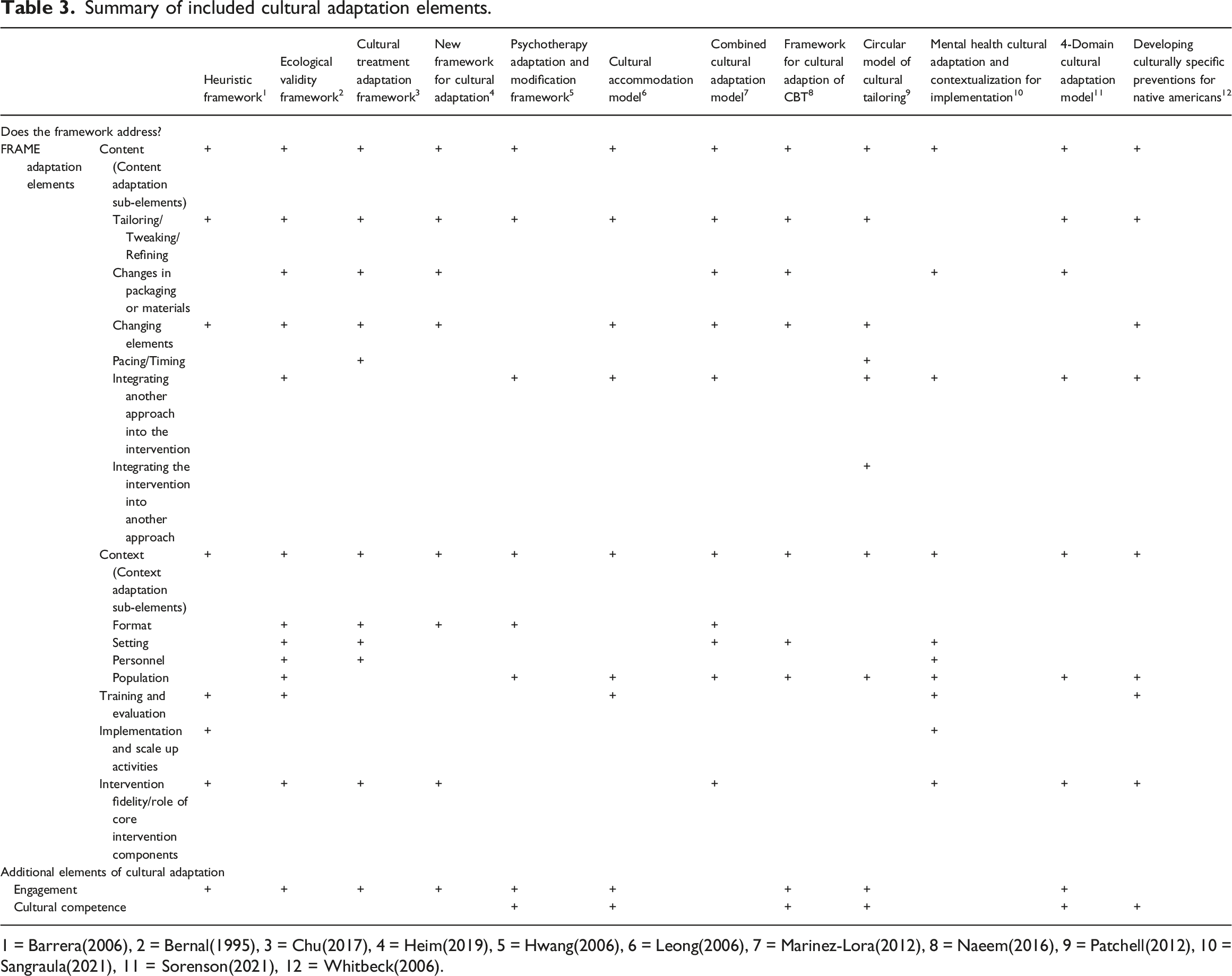
1 = Barrera(2006), 2 = Bernal(1995), 3 = Chu(2017), 4 = Heim(2019), 5 = Hwang(2006), 6 = Leong(2006), 7 = Marinez-Lora(2012), 8 = Naeem(2016), 9 = Patchell(2012), 10 = Sangraula(2021), 11 = Sorenson(2021), 12 = Whitbeck(2006).
Analysis of cultural adaptation elements:
Content
Synthesis of adaptation elements.
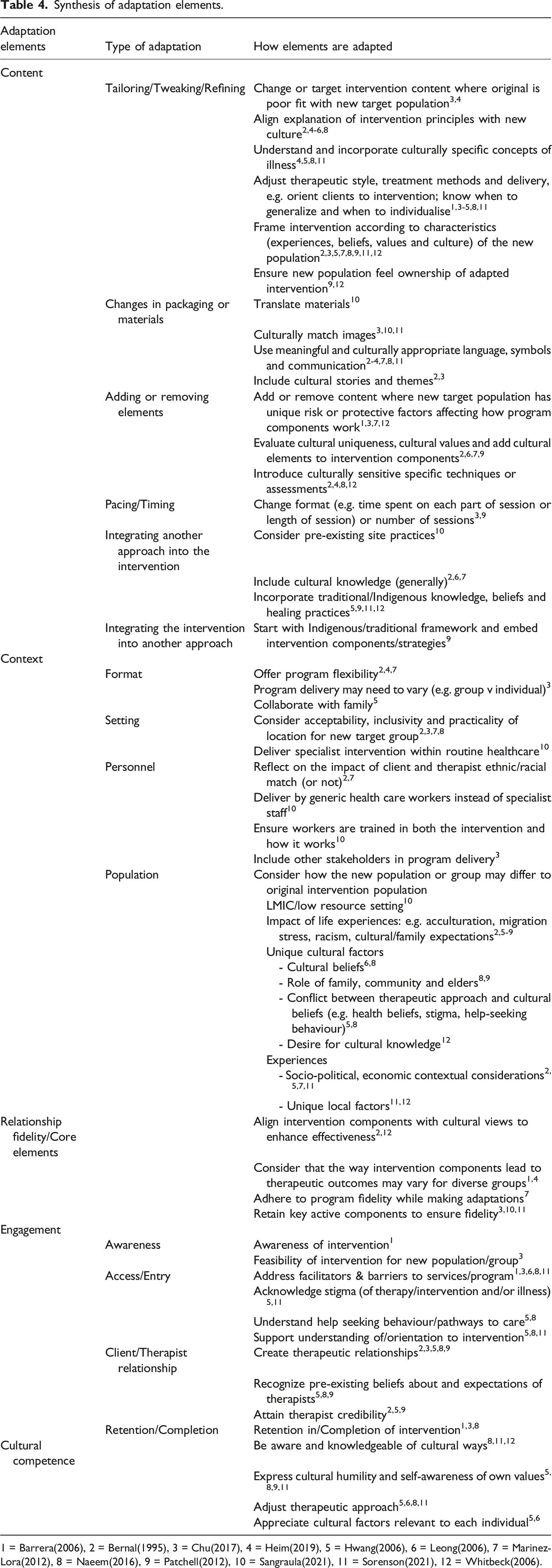
1 = Barrera(2006), 2 = Bernal(1995), 3 = Chu(2017), 4 = Heim(2019), 5 = Hwang(2006), 6 = Leong(2006), 7 = Marinez-Lora(2012), 8 = Naeem(2016), 9 = Patchell(2012), 10 = Sangraula(2021), 11 = Sorenson(2021), 12 = Whitbeck(2006).
Context
Most frameworks (n = 11) suggested adaptation of context (population, setting, format and personnel) (Bernal et al., 1995; Chu & Leino, 2017; Heim & Kohrt, 2019; Hwang, 2006; Leong & Lee, 2006; Marinez-Lora & Atkins, 2012; Naeem et al., 2016; Patchell et al., 2012; Sangraula et al., 2021; Sorenson & Harrell, 2021; Whitbeck, 2006). However, consideration of the context for cultural adaptation differed across frameworks. One example is how they considered adaptation to accommodate the differences between the new population and the original intervention group (identified in n = 9 frameworks). Some frameworks incorporated consideration of unique cultural factors or individual and societal experiences, such as experiencing racism (e.g., Naeem et al., 2016), whereas the mhCACI specifically considered populations in new, low-resource settings (Sangraula et al., 2021). Other contextual considerations included the setting, such as the acceptability and accessibility for a new population to attend an intervention in a church hall compared with a community centre (Chu & Leino, 2017). Intervention format could also be changed, for example, from a group to an individual program to accommodate community stigma around the illness or the treatment (Chu & Leino, 2017). Personnel involved in intervention delivery could also be adapted, for example including other stakeholders (Chu & Leino, 2017). Alternatively, resources may vary in the new context affecting availability of personnel; the mhCACI incorporated the need to utilise non-specialist workforce to deliver specialist interventions (Sangraula et al., 2021).
Fidelity
Eight of the frameworks considered fidelity to the original intervention or the role of core intervention components as part of the cultural adaptation (Barrera & Castro, 2006; Bernal et al., 1995; Chu & Leino, 2017; Heim & Kohrt, 2019; Marinez-Lora & Atkins, 2012; Sangraula et al., 2021; Sorenson & Harrell, 2021; Whitbeck, 2006). Two approaches to maintaining fidelity were identified. One approach suggested fidelity is maintained by identifying and then retaining the “core components” of an intervention during adaptation, as articulated by the ‘Cultural Treatment Adaptation Framework (CTAF)’ (Chu & Leino, 2017), the ‘4-Domain Cultural Adaptation Model (CAM4)’ (Sorenson & Harrell, 2021) and the mhCACI (Sangraula et al., 2021). Core components are generally considered the key active intervention components, the mechanisms that bring about the desired change (Wholey, 1987). However, the CTAF names the deep structural components of an intervention the “core components” and suggests these alone are the key active components.
The second approach suggested that, following identification of the key components, these may then need to be purposefully adapted to align with cultural views of the new population or address specific risk factors to achieve similar intervention outcomes. This approach was reflected in the ‘Ecological Validity Framework (EVF)’ (Bernal et al., 1995), the ‘Theoretical model for developing culturally specific preventions with Native American people’ (Whitbeck, 2006), Barrera and Castro’s (2006) ‘Heuristic’ framework, and the ‘New framework for cultural adaptation’ (Heim & Kohrt, 2019). In summary, the frameworks differed in their definitions of what constitutes a ‘key active component’ of an intervention and offered little guidance on how to identify these. They also differed in whether fidelity to the original intervention is achieved by retaining core intervention components or by retaining therapeutic outcomes by strategic adaptation, including of core components.
Engagement
Engagement was included within nine frameworks (Barrera & Castro, 2006; Bernal et al., 1995; Chu & Leino, 2017; Heim & Kohrt, 2019; Hwang, 2006; Leong & Lee, 2006; Naeem et al., 2016; Patchell et al., 2012; Sorenson & Harrell, 2021). The frameworks suggest strategic modification to promote engagement by identifying and addressing barriers, such as stigma (Barrera & Castro, 2006; Chu & Leino, 2017; Leong & Lee, 2006; Naeem et al., 2016; Sorenson & Harrell, 2021), and facilitators, such as orientation to the intervention to facilitate access (Hwang, 2006; Naeem et al., 2016; Sorenson & Harrell, 2021). Engagement is also enabled via the therapeutic relationship (Bernal et al., 1995; Chu & Leino, 2017; Hwang, 2006; Naeem et al., 2016; Patchell et al., 2012).
Cultural competence
Cultural competence was included within six frameworks (Hwang, 2006; Leong & Lee, 2006; Naeem et al., 2016; Patchell et al., 2012; Sorenson & Harrell, 2021; Whitbeck, 2006). Cultural competence of the practitioner is described as an important consideration for cultural adaptation in half the frameworks (Hwang, 2006; Leong & Lee, 2006; Naeem et al., 2016; Patchell et al., 2012; Sorenson & Harrell, 2021; Whitbeck, 2006); this encompasses the need for cultural knowledge and respect, cultural humility, culturally acceptable therapeutic approaches, and individualised therapeutic accommodation.
Discussion
This systematic review identified 12 content-specific, cultural adaptation frameworks. Five main cultural adaptation elements were identified through the synthesis and there were commonalities in how the frameworks included these - all suggested that content modification was important for cultural adaptation, and context modification, intervention fidelity, engagement and cultural competence were also included in most frameworks. However, there was heterogeneity across the frameworks in terms of their application, specifically their intended usage, as well as how they defined and emphasised the different cultural adaptation elements. The interpretation of cultural competence in the frameworks varied, as did how the relationship between fidelity and key intervention components was guided by the frameworks during adaptation.
Dementia practitioners and researchers undertaking cultural adaptation can use a content-specific framework to support them to identify which of areas of the intervention can be targeted and enhance the transparency, consistency, and replicability of their adaption. However, the included frameworks were not designed for holistic adaptation of all types of psychosocial interventions for all populations, therefore when selecting a cultural adaptation framework, researchers and practitioners should consider the values and beliefs of the new population, the specific dementia intervention, and the purpose of the adaptation.
Limitations of current frameworks
Maintaining fidelity is complex
The identification and retention of the key intervention components are key steps in any health intervention adaptation to ensure fidelity (Escoffery et al., 2019; Movsisyan et al., 2019), however this can be challenging. Firstly, the frameworks rely on adapters to identify the key components of an intervention; however, original intervention developers rarely articulate which components are key, and which are peripheral (Berkel et al., 2010). Dementia interventions are complex psychosocial interventions, and it can be difficult to define the specific mechanisms that ensure intervention success (Cuijpers et al., 2019; Lemmens et al., 2016; Teahan et al., 2020). For example, in a recent cultural adaptation of a caregiver intervention for people with dementia using the Cultural Treatment Adaptation Framework (CTAF) (Chu & Leino, 2017), one-to-one delivery was described as a key intervention component, differing from the original CTAF model where delivery mode is classified as a modifiable peripheral treatment component (Webster et al., 2023). To retain fidelity during cultural adaptation, intervention developers should clearly articulate the program theory, in particular they should describe the key active mechanism components (O’Cathain et al., 2019).
Secondly, retention of the key intervention components can be difficult if they are not culturally appropriate (Barrera & Castro, 2006; Lau, 2006; Resnicow et al., 1999). For example, a key component of a dementia intervention may be training for caregivers to improve their assertiveness when interacting with medical personnel (e.g., Gallagher-Thompson et al., 2003). Yet, for some cultures assertiveness is considered a disrespectful communication style, therefore that component would need to be considered for adaptation (Leong & Lee, 2006). One approach might be to increase the new population’s acceptance of the intervention’s key components during the adaptation process, suggested in the mhCACI framework (Sangraula et al., 2021). An alternative is to consider “functional fidelity”, whether the adapted intervention has the same outcome as the original (Evans et al., 2021). With this approach the actual intervention component is less important than the function it performs in achieving the desired program outcomes (Hawe, 2015). Using the previous example, the outcome is the caregiver’s ability to be an advocate, and the intervention could be adapted to include another approach in the place of assertiveness training to achieve this.
There was no consensus amongst frameworks on what elements of an intervention can be changed, how they can be changed and by how much; all key to achieving fidelity during cultural adaptation (Bernal et al., 2009). Nor was guidance provided on how much an intervention can be changed and still be considered an ‘adapted’ intervention, rather than a ‘new’ intervention. As such, dementia researchers and practitioners should be aware that cultural adaptation frameworks can provide guidance and offer consistency but do not solve the “Fidelity-Adaptation Dilemma”.
Traditional practices only sometimes considered
Most psychosocial interventions are based on Western values and understanding of health (Henrich et al., 2010). Most adaptation frameworks were developed in Western countries for the adaptation of these Western interventions for minority cultural groups or non-Western countries. It is important to consider that cultural perceptions of illness and healing may not align with the therapeutic foundations of an intervention (Castro et al., 2010; Falicov, 2009; Hall, 2001). Therefore, it is imperative that incorporation of traditional knowledge and local beliefs and values are considered within the adaptation process (Summerfield, 2013). Ownership of an adapted intervention can be facilitated by acknowledging historical trauma and power imbalances (Huria et al., 2019). The two included frameworks that focus specifically on Native Americans (Patchell et al., 2012; Whitbeck, 2006) offer thoughtful guidance to ensure culturally safe, responsible and respectful adaptations for Indigenous communities. Approaches that are sensitive to the needs of Indigenous communities can be relevant to other populations (Wilson et al., 2020), therefore these frameworks could be applied more broadly.
Ensuring cultural competence of practitioners is part of cultural adaptation
Elements of practitioner cultural competence were included in half the frameworks in this review. Effective delivery and outcomes of an adapted intervention may be compromised without a culturally competent practitioner working within a supportive structure. The inclusion of cultural competence recognises the importance of cross-cultural interactions and requires a practitioner to reflect on the impact of cultural knowledge, cultural differences, and how they will meet culturally unique needs (Cross et al., 1989). Program recipients’ perception of the cultural competence of their practitioner is positively correlated with intervention outcomes (Soto et al., 2018). However, there is a difference between a practitioner’s general competence and their cultural competence (Hayes et al., 2016; Imel et al., 2011). Although the inclusion of bilingual or bicultural workers may increase feasibility for diverse populations (Falicov, 2009), in effective cultural adaptation, workers, including bicultural workers, also receive cultural competence training (e.g., Belle et al., 2006; Cardemil et al., 2010; Wood et al., 2008). Further, a structure is required to support the incorporation of cultural competence into practice (Hwang, 2006).
Implications for framework use
This review found the CAM4 (Sorenson & Harrell, 2021) was the only framework that includes all the main synthesised adaptation elements: content, context, cultural competence, fidelity and engagement. However, the CAM4 incorporates fidelity only within the ‘Development and Equivalence’ phase of the framework. This means adapters identify and retain the key active mechanisms of the intervention at the start of the cultural adaptation process (Sorenson & Harrell, 2021). This review has highlighted the lack of consensus around how to maintain fidelity during cultural adaptation of complex psychosocial interventions, in particular the complexity surrounding the identification and retention of key components. Therefore, the CAM4 would be enhanced by considering fidelity not only at the outset but throughout each stage of the adaptation process. This concept is reflected in Figure 2. CAM4 adapted (to include fidelity throughout the cultural adaptation process).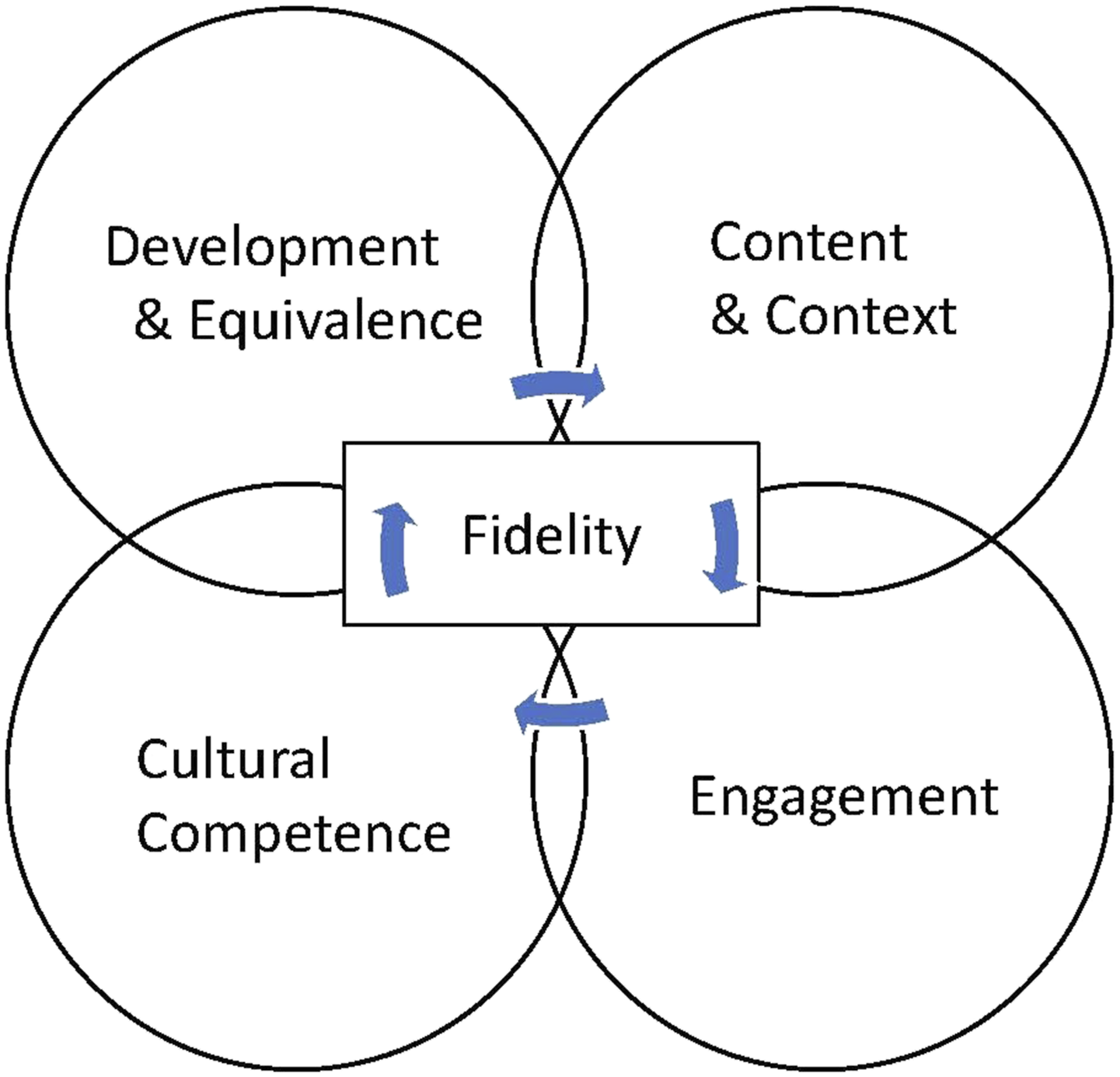
Strengths and limitations of this systematic review
This review contributes to cultural adaptation literature by building on recent reviews of adaptation frameworks and guidelines (Escoffery et al., 2019; Movsisyan et al., 2019). By focussing on the content perspective of cultural adaptation, an area included in process frameworks with little guidance or detail as to what to do, this synthesis of 12 frameworks collates important available information to support dementia researchers and practitioners in the cultural adaptation process.
This review has several limitations. First, our search terms were in English and most identified frameworks were developed in the United States, therefore caution should be taken when interpreting the results in a global context. Second, no quality appraisal or risk of bias evaluation was conducted for the review as the purpose was to identify available frameworks rather than appraise the data. To increase the rigor of this review, two reviewers were used throughout the screening and data extraction phases. The process of data extraction and synthesis of theoretical constructs was reviewed by all authors to ensure accuracy. An additional limitation is that cultural adaptation is guided by conceptual and theoretical papers as much as practical frameworks and these were excluded from the review. However, the included frameworks referenced many of the leading theoretical references to support their framework development or articulate their definitions and as such the concepts form part of the review. Finally, we included only original papers describing a framework therefore may have omitted elaborations or clarifications included in subsequent publications (e.g., Naeem et al., 2019; Rathod et al., 2019).
Conclusion
Comprehensive cultural adaptation frameworks are available to support cultural adaptation of psychosocial dementia interventions. These were predominantly developed for minority cultural groups in the USA, for adaptation of psychology interventions. This systematic review provides a summary of the main elements of content-specific cultural adaptation frameworks and a synthesis of how these can be applied during the adaptation process. Adapters should follow the steps for adaption (i.e., planning, conducting, testing), apply the selected content-specific framework to guide the adaptation, and draw on the extensive cultural adaptation literature to achieve meaningful and authentic cultural adaptation of dementia interventions. Consideration should be given to the impact of cultural competence. Cultural adaptation frameworks would be enhanced by incorporating consideration of fidelity throughout the adaptation process. To further ensure fidelity during adaptation, more work is required by dementia researchers and program developers to both articulate the key intervention components and ensure practitioners understand how they work.
Supplemental Material
Supplemental Material - Frameworks for cultural adaptation of psychosocial interventions: A systematic review with narrative synthesis
Supplemental Material for Frameworks for cultural adaptation of psychosocial interventions: A systematic review with narrative synthesis by Sally Day, Kate Laver, Yun-Hee Jeon, Kylie Radford and Lee-Fay Low in Dementia
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sally Day is the recipient of a PhD Scholarship from the Dementia Centre Research Collaboration (DCRC), University of New South Wales, Australia.
Ethics statement
Ethics approval was not required for this systematic review.
Human rights
This article does not contain any studies with human participants performed by any of the authors.
Informed consent
This study does not involve research with human participants and informed consent was therefore not required.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Databases searched. MEDLINE search strategy.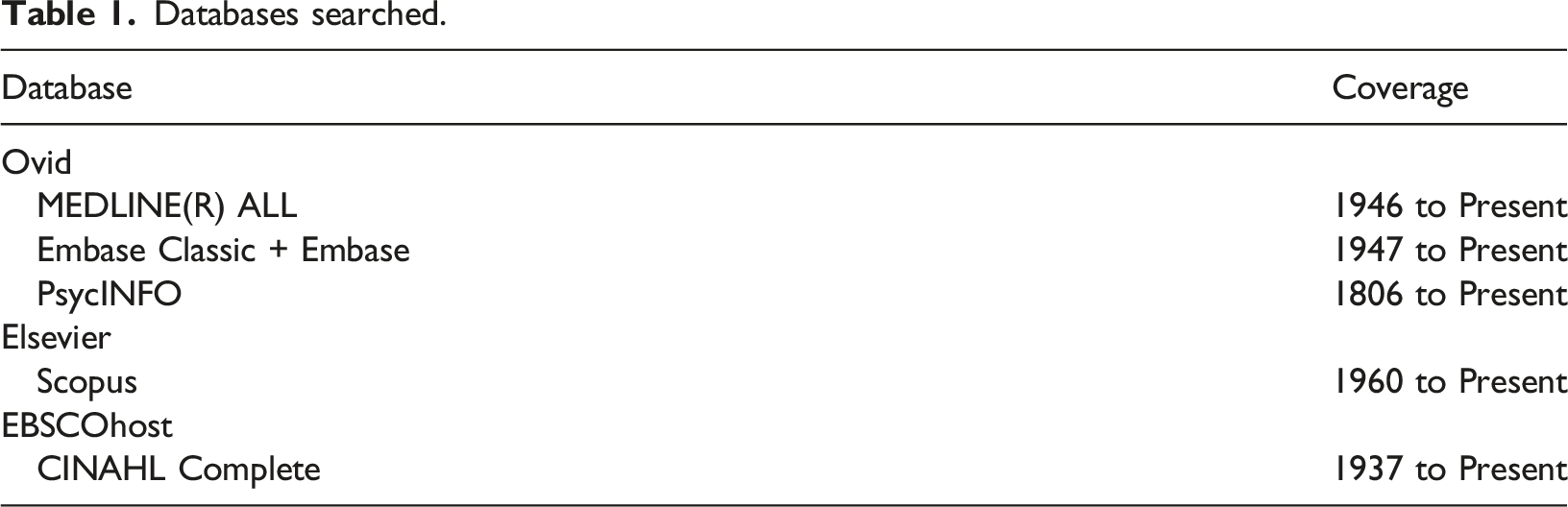
Database
Coverage
Ovid
MEDLINE(R) ALL
1946 to Present
Embase Classic + Embase
1947 to Present
PsycINFO
1806 to Present
Elsevier
Scopus
1960 to Present
EBSCOhost
CINAHL Complete
1937 to Present
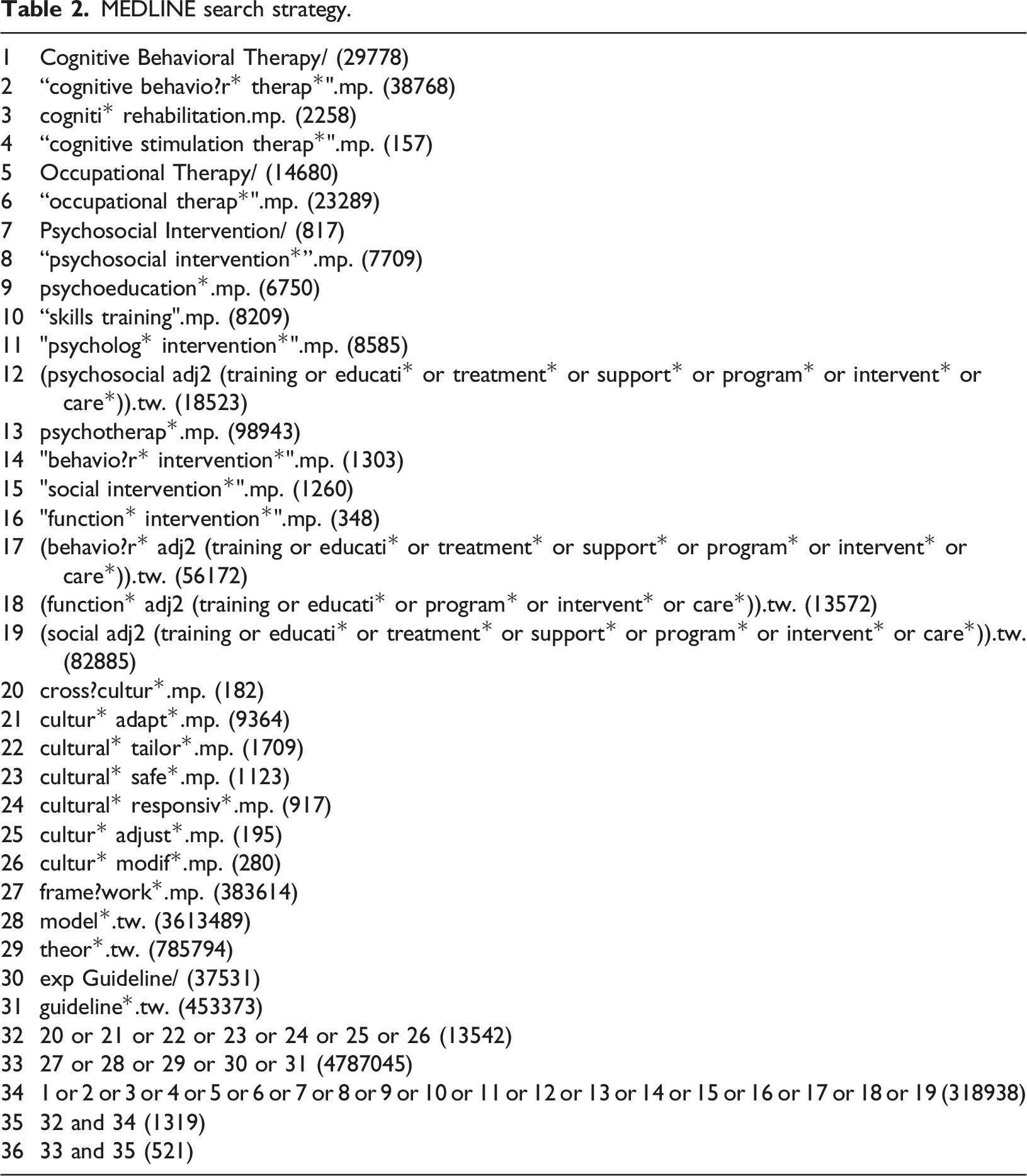
1
Cognitive Behavioral Therapy/ (29778)
2
“cognitive behavio?r* therap*".mp. (38768)
3
cogniti* rehabilitation.mp. (2258)
4
“cognitive stimulation therap*".mp. (157)
5
Occupational Therapy/ (14680)
6
“occupational therap*".mp. (23289)
7
Psychosocial Intervention/ (817)
8
“psychosocial intervention*”.mp. (7709)
9
psychoeducation*.mp. (6750)
10
“skills training".mp. (8209)
11
"psycholog* intervention*".mp. (8585)
12
(psychosocial adj2 (training or educati* or treatment* or support* or program* or intervent* or care*)).tw. (18523)
13
psychotherap*.mp. (98943)
14
"behavio?r* intervention*".mp. (1303)
15
"social intervention*".mp. (1260)
16
"function* intervention*".mp. (348)
17
(behavio?r* adj2 (training or educati* or treatment* or support* or program* or intervent* or care*)).tw. (56172)
18
(function* adj2 (training or educati* or program* or intervent* or care*)).tw. (13572)
19
(social adj2 (training or educati* or treatment* or support* or program* or intervent* or care*)).tw. (82885)
20
cross?cultur*.mp. (182)
21
cultur* adapt*.mp. (9364)
22
cultural* tailor*.mp. (1709)
23
cultural* safe*.mp. (1123)
24
cultural* responsiv*.mp. (917)
25
cultur* adjust*.mp. (195)
26
cultur* modif*.mp. (280)
27
frame?work*.mp. (383614)
28
model*.tw. (3613489)
29
theor*.tw. (785794)
30
exp Guideline/ (37531)
31
guideline*.tw. (453373)
32
20 or 21 or 22 or 23 or 24 or 25 or 26 (13542)
33
27 or 28 or 29 or 30 or 31 (4787045)
34
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 (318938)
35
32 and 34 (1319)
36
33 and 35 (521)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.