
Abstract
Objectives
Social isolation and loneliness affect the quality of life of people living with dementia, yet few interventions have been developed for this population. The purpose of this study was to assess the feasibility and acceptability of ‘Connecting Today’, a remote visiting program designed for use with care home residents living with dementia.
Methods
This was a feasibility study to assess whether Connecting Today can be delivered in care homes, and was acceptable to family and friends and people living with dementia. We used a single-group before/after design and included residents ≥ 65 years old with a dementia diagnosis from two care homes in Alberta, Canada. Connecting Today involved up to 60 min per week of facilitated remote visits for 6 weeks. To understand feasibility, we assessed rates and reasons for non-enrollment, withdrawal and missing data. We assessed acceptability with the Observed Emotion Rating Scale (residents) and a Treatment Perception and Preferences Questionnaire (family and friends). Data were analyzed with descriptive statistics.
Results
Of 122 eligible residents, 19.7% (n = 24) enrolled (mean age = 87.9 years, 70.8% females). Three residents withdrew from the study before the first week of calls. Among 21 remaining residents, 62%–90% completed at least 1 call each week. All the calls were completed by videoconference, rather than by phone. Alertness and pleasure were observed for ≥92% of residents during calls. The 24 contacts rated Connecting Today as logical, effective and low risk.
Conclusions
Facilitated, remote visits are feasible and highly acceptable to residents and their family and friend contacts. Connecting Today shows promise to address social isolation and loneliness for people living with moderate to severe dementia because it can promote positive engagement in meaningful interactions with their family and friends while they are living in a care home. Future studies will test effectiveness of Connecting Today in a large sample.
Keywords
Introduction
Being alone (social isolation) is a critical factor that influences feeling alone (loneliness) (Statistics Canada, 2021). The opposite of loneliness is social connectedness, a subjective construct indicated by feelings of intimacy, caring and belonging (O’Rourke & Sidani, 2017). For decades, research has highlighted high rates of loneliness among older adults living in care homes (i.e., long-term care) (Victor, 2012), and with dementia (Alzheimer’s Society, 2013). Yet, few interventions have been developed for use with people living with dementia in care homes (Hung et al., 2021; O’Rourke et al., 2018; Quan et al., 2019). The purpose of this study was to assess the feasibility and acceptability of Connecting Today: a facilitated remote visiting program, designed to support people living with dementia to engage positively with their care partners, family members and friends, and address loneliness.
Literature review
Social isolation, or limited social contact (Ashida & Heaney, 2008; R. M. Lee & Robbins, 1995), is a modifiable cause of loneliness (Weiss, 1973). Empirical studies, including both a quantitative metaanalysis (Masi et al., 2011) and multiple qualitative studies conducted with older adults (Cattan & Ingold, 2003; Cattan et al., 2003; Hooper, 2003; Moyle et al., 2011; Pettigrew & Roberts, 2008; J. M. Smith, 2010) support that social isolation contributes to loneliness. When family and friends distance themselves from the older adult living with dementia (Vikström et al., 2008), people living with dementia experience decreased social contact (Hackett et al., 2019). One study found that weekly visits, number of contacts, and phone calls reduced by half following a move to a care home (Port et al., 2001). Family and friends may distance themselves from the person living with dementia as a result of their own difficult experiences with advancing dementia symptoms (Dupuis & Smale, 2000), personal and societal stigmatizing beliefs related to dementia and aging (Milne, 2010), logistical issues such as geographical barriers, or discomfort within care home environments (Miller, 2019).
The term ‘intervention’ refers to a rational cognitive, verbal or physical action designed to respond to a particular problem and achieve specific goals (Sidani & Braden, 2011). Visiting programs (also called ‘personal contact interventions’) are a specific type of intervention, designed to address loneliness and are defined by the use of scheduled visits with a family member, friend, or volunteer (O’Rourke et al., 2018; O’Rourke et al., 2020). Visits could occur in-person or remotely, and should promote positive, meaningful interactions in order to address loneliness (O’Rourke et al., 2018, 2020).
Previous visiting programs have aimed to connect older adults living in the community with a volunteer visitor or ‘befriender’ (Andrews et al., 2003; Cattan et al., 2011; Van Orden et al., 2013), or used videoconferencing (Moyle et al., 2020; Schwindenhammer, 2014; Tsai & Tsai, 2011; Tsai et al., 2010) or email (Moses, 2003) to connect care home residents who were cognitively intact with their family or friends. However, people living with dementia were excluded from these studies. Studies of touchscreen tablets and telepresence robots exist, but were aimed to support interactions between people living with dementia in a community setting with their care partner (as opposed to in a care home separate from their care partner) (Moyle et al., 2017), or were used for activities like playing games or digital story books, or for video-simulated presence (Hung et al., 2021). Although people living with dementia represent at least 70% of care home residents (Canadian Institute for Health Information (CIHI), 2022), a recent systematic review did not identify any experimental or quasi-experimental study of a visiting program aimed to address loneliness for use with people living with dementia in care homes (Quan et al., 2019).
Key stakeholders support the logic and potential benefits of a 30 to 60-min visiting program, if it were adapted for use with people living with dementia (O’Rourke et al., 2020). To date, there have been just three previously published studies of visiting programs which had undergone feasibility assessment or pilot testing for use with people living with dementia. One study (n = 5) explored use of a telepresence robot to assist care home residents with mild to moderate dementia with video calls to family (Moyle et al., 2014), and another (n = 3) used a software program to prompt conversations between people living with dementia and their carers (Purves et al., 2015). While participant mood and verbal interactions during calls were positive, these small studies employed technologies that are not widely available, and excluded people living with severe or moderate dementia who could not communicate verbally, seriously limiting their application in care home populations. A third feasibility study of a visiting program (n = 17) used iPads and Skype which are widely available, but the visits were not facilitated beyond equipment set-up. Some found the visits distressing, and this study also excluded people living with severe dementia or without ‘adequate language capacity’(Van Der Ploeg et al., 2016).
To address this gap, we developed a facilitated remote visiting program, Connecting Today, for use to support regular, engaging visits between people living with mild, moderate, or severe dementia in care homes and their care partners, family and friends. Connecting Today was developed in phases as per the Medical Research Council recommendations for complex interventions (Campbell et al., 2000; Craig et al., 2013). Development (Phase 1) involved scoping reviews to understand the problem and describe the intervention (O’Rourke et al., 2018; O’Rourke & Sidani, 2017), and a mixed methods study to explore acceptability of visiting programs (in general) from the perspectives of health care providers and family and friends of people living with dementia (O’Rourke et al., 2020). The purpose of the current (Phase 2) study was to assess the feasibility and acceptability of Connecting Today, which was designed to address loneliness, and promote quality of life, of care home residents living with mild, moderate or severe dementia in care homes.
Methods
Design and procedures
We used a quasi-experimental one-group pre and post-test design to deliver the intervention and to collect feasibility and acceptability data at baseline and at 6 weeks. We chose 6 weeks because this was a common timeframe to assess outcomes from previous studies focused on interventions to address loneliness in other populations of older adults (Moses, 2003; Schwindenhammer, 2014; Tsai et al., 2010; Tsai & Tsai, 2011; van der Heide et al., 2012), and we wanted to evaluate how many participants would continue with the study for 6 weeks as a part of our feasibility assessment. We initially invited participants to complete 12 weeks of visits, but withdrawal rates (reported below) indicated that this longer timeframe would not be feasible.
The Connecting Today intervention
An intervention theory describes how a specific goal is addressed by components of an intervention to affect outcomes (Sidani, 2015). Similar to other visiting programs, Connecting Today contains a core component (i.e., mechanism of effect) of positive, routine social contact with remote visitors (i.e., their care partners, family or friends). Connecting Today also contains a second core component which sets it apart from previous visiting programs: interactions with a facilitator, who provides social support to residents and their remote visitors in order to promote engagement during the calls (Figure 1). Description of the Connecting Today intervention theory.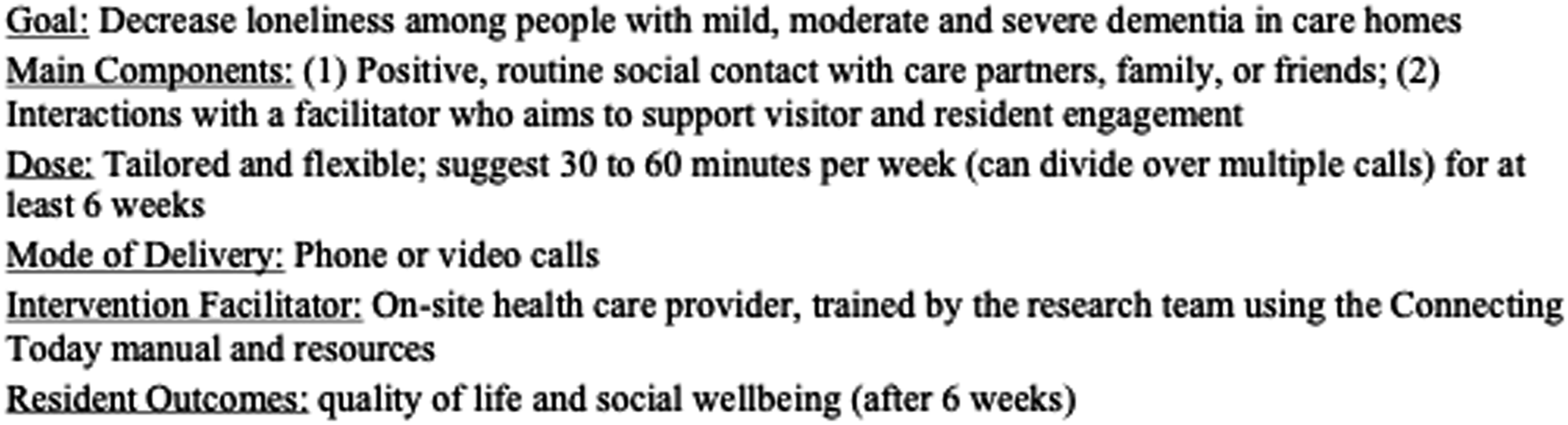
Connecting Today was implemented in the following steps: (1) We used videoconference and our Connecting Today instruction and resource manual to train an onsite member of the care staff to be the intervention facilitator at each site. The research team provided each facilitator with the training manual and the equipment to complete phone and video calls with residents at their site, including a cell phone, handset, and an iPad with data plan. Training to facilitate Connecting Today sessions involved review of the training manual and participating in several zoom meetings with the research team to become comfortable with the technology, ask questions, and practice using the Observed Emotion and Rating Scale (described in more detail below). It took 8–10 h to train each facilitator. (2) The trained facilitator worked with designated decision-makers (i.e., a person on-file who makes health care decisions on the resident’s behalf) to tailor visits for residents whose level of cognitive impairment prevented them from making these decisions on their own. The facilitator met with each person living with dementia, or their designated decision-maker, to identify a list of up to three remote visitors (i.e., care partners, family members or friends) to call each week. The decision-maker also has the option (but was not required) to participate as one of the resident’s remote visitors. In this meeting, they also determined the weekly ‘dose’ of the intervention (between 30 to 60 min), selected the mode of delivery (phone or video-call), talked about how to meet individual hearing, vision, communication and other needs, and discussed possible individualized engagement prompts in detail (e.g., familiar stories or music; or pictures, people or activities they would like to see). The facilitator discussed examples of strategies to engage with people living with dementia in verbal and non-verbal interactions (from the intervention manual), but what was done to engage each resident was tailored and highly individualized. This approach capitalized on the expertise and creative ideas of the facilitator and decision-maker, both of whom knew the resident well. (3) A research assistant called the remote visitors by phone to provide them with information and obtain their consent to participate in scheduled, weekly calls and complete the study measures. (4) Before the first call, the facilitator sent remote visitor participants several resources (by mail or email) about interacting with people living with dementia, and informed the remote visitors of the call schedule. When setting the call schedule, the facilitator considered the resident’s routines, their remote visitors’ availability, and their own work schedule. (5) Facilitation during each call involved having the facilitator set-up equipment, track participant attendance, assess resident mood for the first 10 min of the call, and use the tailored engagement prompts throughout the call. After the first 10 min, the facilitator could leave, if privacy was desired by the resident and their remote visitors. The facilitators and remote visitors discussed challenges and strategies at least every other week, either during or after the call, in order to improve the call experience.
Intervention facilitators
The facilitators contacted eligible residents (or their decision-makers) to obtain consent-to-contact, met with the residents/decision-makers to tailor the calls, and facilitated the calls each week. Site managers in each care home reviewed the role, and identified a health care staff member to serve as a facilitator (both sites chose recreation therapy assistants). The facilitator was granted ∼8 h per week in lieu (paid by the research grant) to complete the facilitator role over 9 months (including time required for training and program delivery). Because of staff turnover at the care homes, we trained three facilitators, replacing the facilitator at one site, who left their position after 5 months.
Inclusion criteria
Eligible residents were: (1) ≥ 65 years old; (2) diagnosed with dementia (any type); and (3) had a Cognitive Performance Scale score suggesting mild (1), moderate (2–3) or severe (4–6) impairment (Carpenter et al., 2006; Hartmaier et al., 1995). To participate in this study, residents (or their decision-makers) needed to identify at least one care partner, family member or friend of the person living with dementia with whom the person with dementia would desire contact, who were 18 or older, and who understood English (necessary for facilitators to support the call). Because facilitators were prepared to support verbal and/or non-verbal interactions, participants were included, regardless of their abilities related to verbal communication.
Recruitment
We recruited participants between February and October 2021 from two care homes from a single continuing care operator in an urban centre in Alberta, Canada. In February, June and October 2021, a care home staff member used their clinical record data (i.e., from their Resident Assessment Instrument 2.0 data set) to generate a complete list of all potentially eligible care home residents who were 65 or older, diagnosed with dementia, and with a Cognitive Performance Scale score between 1 to 6 (Hartmaier et al., 1995). They gave the list to the on-site facilitator, who contacted all residents (or decision-makers) to ascertain if they were interested in the study and would agree to follow-up by a research assistant by phone. The research assistant obtained oral consent to participate by phone (audio-recorded) from the residents (or their decision-makers), and their remote visitors. While remote visitors could invite others to join the calls on an ad hoc basis, we did do not complete the consent process or collect data from any of these other individuals, unless they approached the research team to request study participation. A minimum of 20 resident participants were needed to generate accurate estimates of the feasibility and acceptability of Connecting Today with 90% confidence to estimate a proportion of 15% (e.g., of withdrawals or missing data) within 9 points of accuracy (Hertzog, 2008). Anticipating missing data due to study withdrawals, we aimed to recruit 30 participants to allow us to assess resident acceptability every week for 6 weeks.
Data collection
Research assistants collected data throughout the study and in telephone interviews with the residents or their decision-makers, and entered data directly into a secure University server or into REDCap (depending on the item). Facilitators carried a notebook with information about how to tailor each resident’s calls, and used a laminated sheet with a dry-erase marker to note their observations during calls. They entered the observational data into REDCap with their iPad immediately after the call. REDCap is a secure web-based data platform for electronic data capture, hosted by the Women & Children’s Health Research Institute at the University of Alberta (Harris et al., 2009). A care home staff member extracted demographic data from the residents’ clinical records from the most recent time period prior to the first call, and sent it to the research team following institutional protocols for data security.
Demographic measures
Demographic data were collected from the residents’ clinical record for variables that may influence loneliness, identified from our comprehensive review (O’Rourke & Sidani, 2017). These included age, sex, education, Cognitive Performance Scale score (Morris et al., 1994), Activities of Daily Living-Hierarchy Scale score (Morris et al., 1999), Depression Rating Scale score (Burrows et al., 2000), Social Engagement Scale score (Mor et al., 1995), absence of family/friend contact, conflict with family, staff or other residents, recent loss of loved one, marital status, number of medications, hearing and vision impairments, and significant other involvement in care planning. Previous research has established the Resident Assessment Instrument item’s reliability (inter-rater and internal consistency) and validity (criterion, convergent, and predictive) (Canadian Institute for Health Information, 2012; Lawton et al., 1998; Mor et al., 1995; Phillips & Morris, 1997; Poss et al., 2008). Following consent, the research assistant asked residents/decision-makers about resident information not contained in the clinical records including: cultural/ethnic background, gender identity, and current amount and mode of weekly contact with visitors.
Feasibility measures
The research assistant recorded in a study participation log the number of eligible residents who expressed interest, consented, and their stated reasons for non-enrollment and study withdrawal. We assessed the feasibility of using a dementia-specific quality of life tool to evaluate relevant outcomes, based on rates and reasons for missing data. At baseline and 6 weeks, the research assistant telephoned the decision-makers to complete the DEMQOL-proxy (32 items, 4-point Likert scales). The DEMQOL-proxy can be used to measure quality of life with a total score or an overall quality of life item, and there are single items that assess social relationships. Because there is currently no validated loneliness scale for use with people living with dementia, we selected social relationship items from the validated DEMQOL-proxy (S. C. Smith, Lamping, et al., 2005; S. C. Smith et al., 2007). These single items reflect known indicators of loneliness (Hughes et al., 2004) and are relevant to the aims of Connecting Today including worries about: (1) getting in touch with people; (2) having enough company; and (3) being able to help other people.
We did not recruit any residents who could consent on their own behalf, so we only used the DEMQOL-proxy (and not the self-report) version of the tool in this study. Evidence supports the DEMQOL-proxy’s internal consistency (α = 0.0.87 to 0.92) and test-retest reliability (ICC = 0.82 to 0.84) when used with people living with mild to moderate and severe dementia (S. C. Smith, Lamping, et al., 2005; S. C. Smith et al., 2007), and its content, convergent and discriminate validity (Cohen-Mansfield et al., 2011; S. C. Smith, Lamping, et al., 2005; S. C. Smith, Murray, et al., 2005).
Acceptability measures
Developing interventions with the perspectives of key stakeholders in mind is important to identify issues related to intervention acceptability prior to proceeding to a large (Phase 3) trial to assess intervention effectiveness (Sekhon et al., 2017; Sidani, 2015). We used several measures to assess acceptability, broadly defined as the appropriateness of implementing Connecting Today from the perspectives of key stakeholders (i.e., the resident and their remote visitors) (Sekhon et al., 2017). Acceptability is a complex, multi-component construct, including participant burden and how individual’s experience an intervention and their attitudes towards it (Sekhon et al., 2017). Acceptability has been operationalized in a variety of ways in studies of people living with dementia, including assessing rates of participation and experiences when engaging in an intervention (Jenewein et al., 2021; Orr et al., 2021). To understand acceptability of Connecting Today, the facilitators documented attendance at each call, reasons for missed calls, and frequency and length of calls in a participation checklist. To understand acceptability of people living with dementia during sessions, the facilitators used a validated observational mood measure, the Observed Emotion Rating Scale (Lawton et al., 1996, 1999), to assess how they experienced and responded to Connecting Today sessions. The scale was specifically designed for use with people living with dementia, and describes indicators for two positive states (pleasure, general alertness) and three negative states (anger, anxiety/fear, sadness). The facilitator rated the presence of each affect state over the first 10 min of the call on a 5-point ordinal scale [not in view/never, <16 sec, 15–59 sec, 1–2 min, and > 5 min]. Evidence supports inter-rater reliability for each state (κ = 0.76 to 0.89) and concurrent and discriminant validity for use by trained raters with people living with dementia (Lawton et al., 1996, 1999). A research assistant and the PI trained the facilitators. We completed independent ratings of video observations of people living with dementia that were available in the public domain until we achieved similar results and agreed upon the rationale for the final ratings. The facilitators noted that rating was easier in clinical practice (as compared to during video observations), because they know each individual and could better understand the nuances of the individual’s expressions. We held regular team meetings to discuss ratings (e.g., what is challenging to capture) to minimize ‘skill drift’ among facilitators and promote standardized application of the rating criteria (Bellg et al., 2004).
After 6 weeks of participating in Connecting Today (and within 2 weeks of the last session), the research assistant completed a short (15 min) telephone interview with the remote visitors to complete the Treatment Perception and Preferences measure, which was designed to operationalize the construct of acceptability (Sidani et al., 2018). This measure captured perceptions of the logic, effectiveness, suitability, willingness to participate in sessions, ease of delivery, and risks related to Connecting Today (5-point Likert scales from 0 = not at all to 4 = very much). Although all participants had recently experienced Connecting Today, we included a description of the Connecting Today intervention before completing the measure, as per the developers’ recommendation. This measure has demonstrated good internal consistency (α > 0.85) and validity (Sidani et al., 2018). The remote visitors were also invited to participate in a semi-structured interview related to their perceptions of the benefits and challenges of Connecting Today, and the results from that qualitative data, including lessons learned, and how challenges such as sensory issues or technical challenges were addressed (for men and women and people with moderate as compared to severe impairments), will be reported in separate manuscripts.
Data analysis
We summarized all data with descriptive statistics (e.g., means, standard deviations, frequencies). We produced descriptive estimates of the DEMQOL-proxy at baseline and 6-weeks for use in sample size calculations for a future trial. We did not assess ‘preliminary effects’ with inferential statistics because this can produce uninterpretable results, and the purpose of this study was to describe the feasibility of critical intervention and study processes (Hertzog, 2008; Kistin & Silverstein, 2015). We used conventional content analysis (Hsieh & Shannon, 2005) to generate new categorical variables from open-ended items about participants’ reasons for non-consent, withdrawal, or missing data. FLFDP reviewed every response and attached code(s) that summarized the meaning of each response. Because participants could report more than one reason, more than one code could be attached to each response. FLFDP and HMO met weekly to clarify the codes, and to collapse synonymous codes as needed.
Ethics
Ethics approval for this study was received from the University of Alberta health research ethics board (Pro00104290). Operational approval was obtained from the continuing care operator to conduct research in the two study sites.
Results
Demographics
Characteristics of 24 resident participants at baseline.
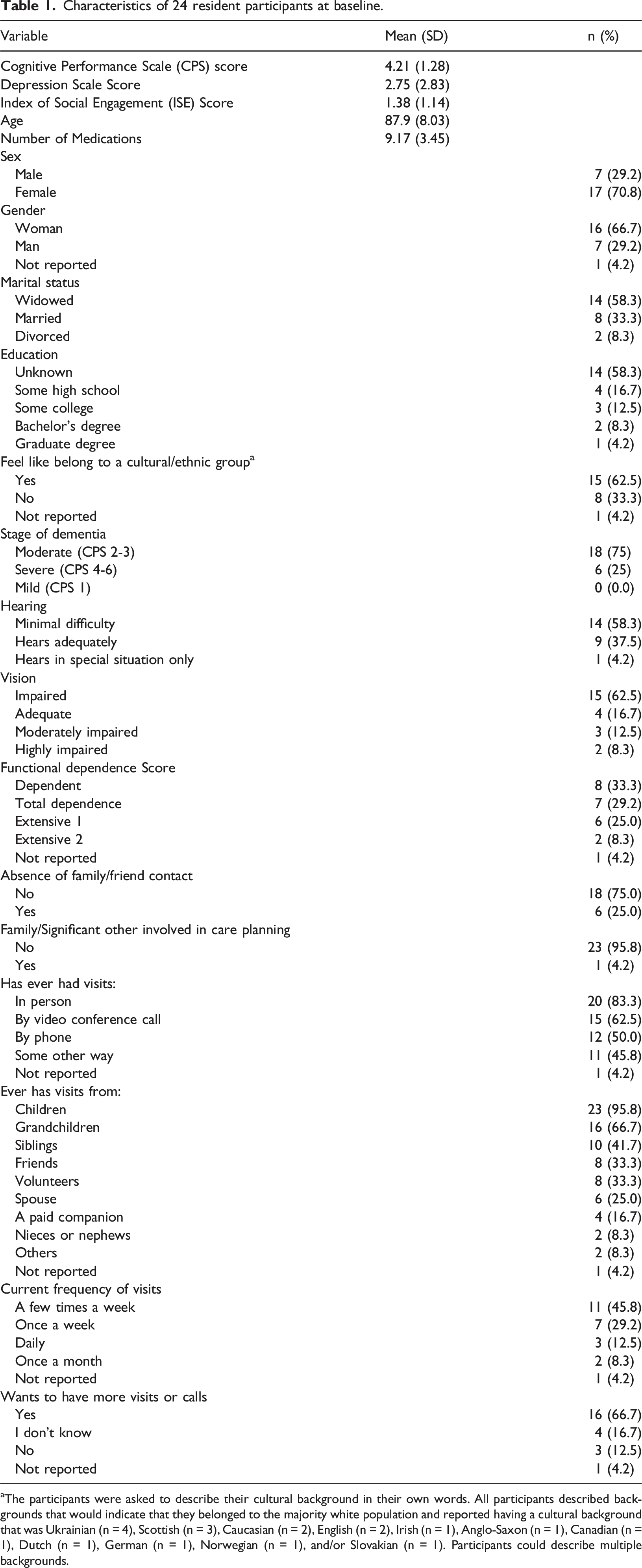
aThe participants were asked to describe their cultural background in their own words. All participants described backgrounds that would indicate that they belonged to the majority white population and reported having a cultural background that was Ukrainian (n = 4), Scottish (n = 3), Caucasian (n = 2), English (n = 2), Irish (n = 1), Anglo-Saxon (n = 1), Canadian (n = 1), Dutch (n = 1), German (n = 1), Norwegian (n = 1), and/or Slovakian (n = 1). Participants could describe multiple backgrounds.
Feasibility
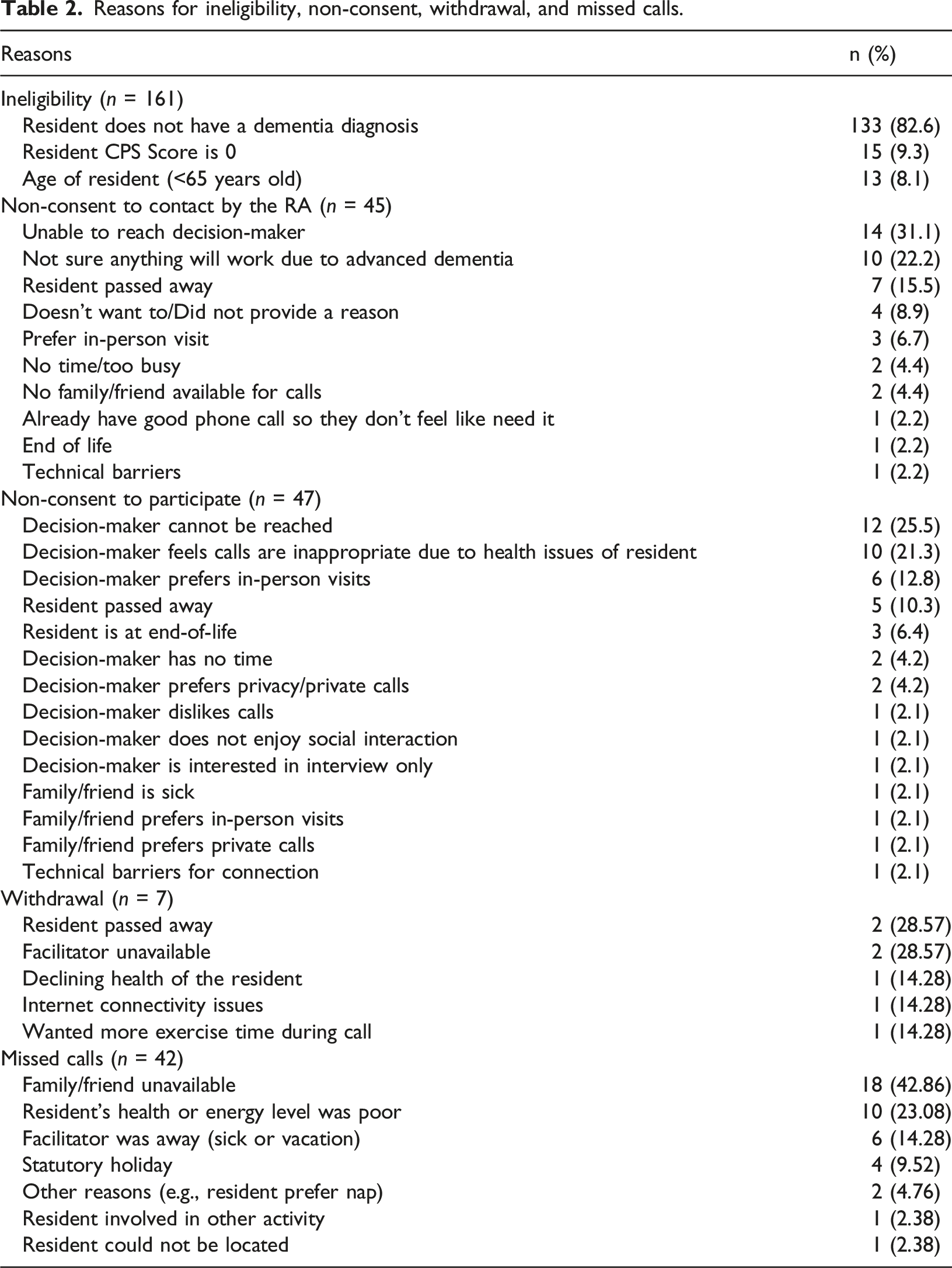
Reasons for ineligibility, non-consent, withdrawal, and missed calls.
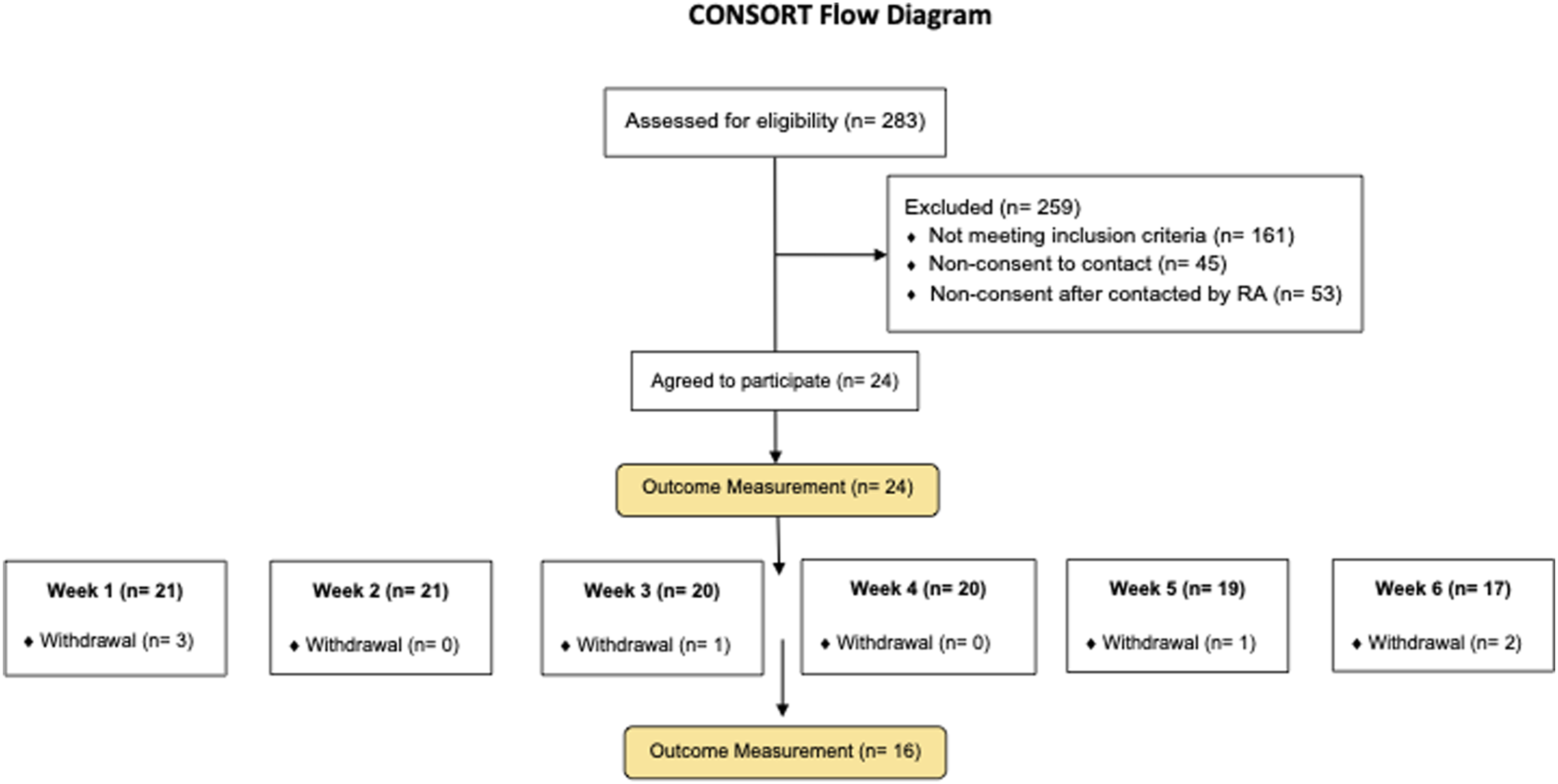
Study CONSORT diagram.
By far, the most common reason for ineligibility was not having a documented diagnosis of dementia (n = 133, 82.6%) (Table 2). Forty-five (36.9%) of the 122 eligible residents did not consent to be contacted by the researcher, most often because the decision-maker could not be reached (n = 14, 31.1%) or believed that nothing could help given the advanced stage of dementia (n = 10, 22.2%). Fifty-three (43.4%) of the 122 eligible residents did not consent to participate in the study after being contacted by the research assistant. The most common reasons for non-consent were that the decision-maker could not be reached (n = 12, 25.5%) or believed that calls were not appropriate given the health issues that the resident experienced (n = 10, 21.3%).
We recruited zero to three participants per month from each of two sites, for a total of 24 resident participants (19.7% of the total eligible population). Of the 24 residents, 17 (70.8%) remained enrolled in the study for 6 weeks. Of note, we had initially recruited 16 of the 24 participants to receive calls for 12 weeks, but the withdrawal rate by week 6 and the need to enroll additional participants suggested that a 12-weeks intervention delivery timeframe would not be feasible in future studies. We shortened the intervention period to 6 weeks, which allowed us to enroll 8 additional participants.
Two of the seven withdrawals (16.7%) occurred before the first call because the facilitator at the second site left after 7 months, and could not be replaced during the 9-months study period due to staff shortages resulting from the COVID-19 pandemic in care homes. Additional withdrawals occurred at each of weeks 1 (n = 1), 3 (n = 1), 5 (n = 1), and 6 (n = 2) for reasons most often related to the residents’ health conditions. No participants withdrew because of discomfort during the intervention, and just one resident withdrew due to internet connectivity issues (Table 2).
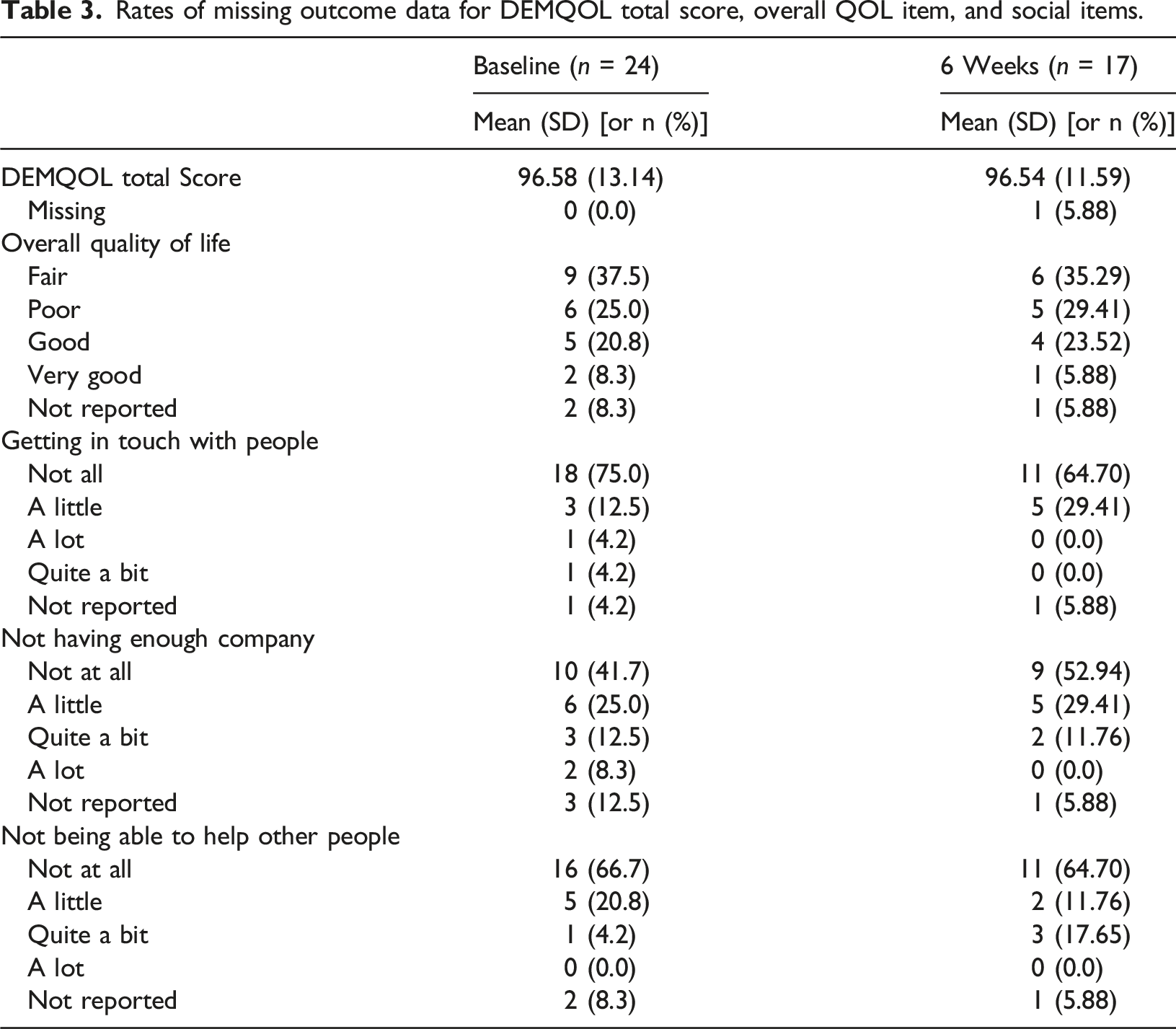
Feasibility of outcome assessment
Rates of missing outcome data for DEMQOL total score, overall QOL item, and social items.
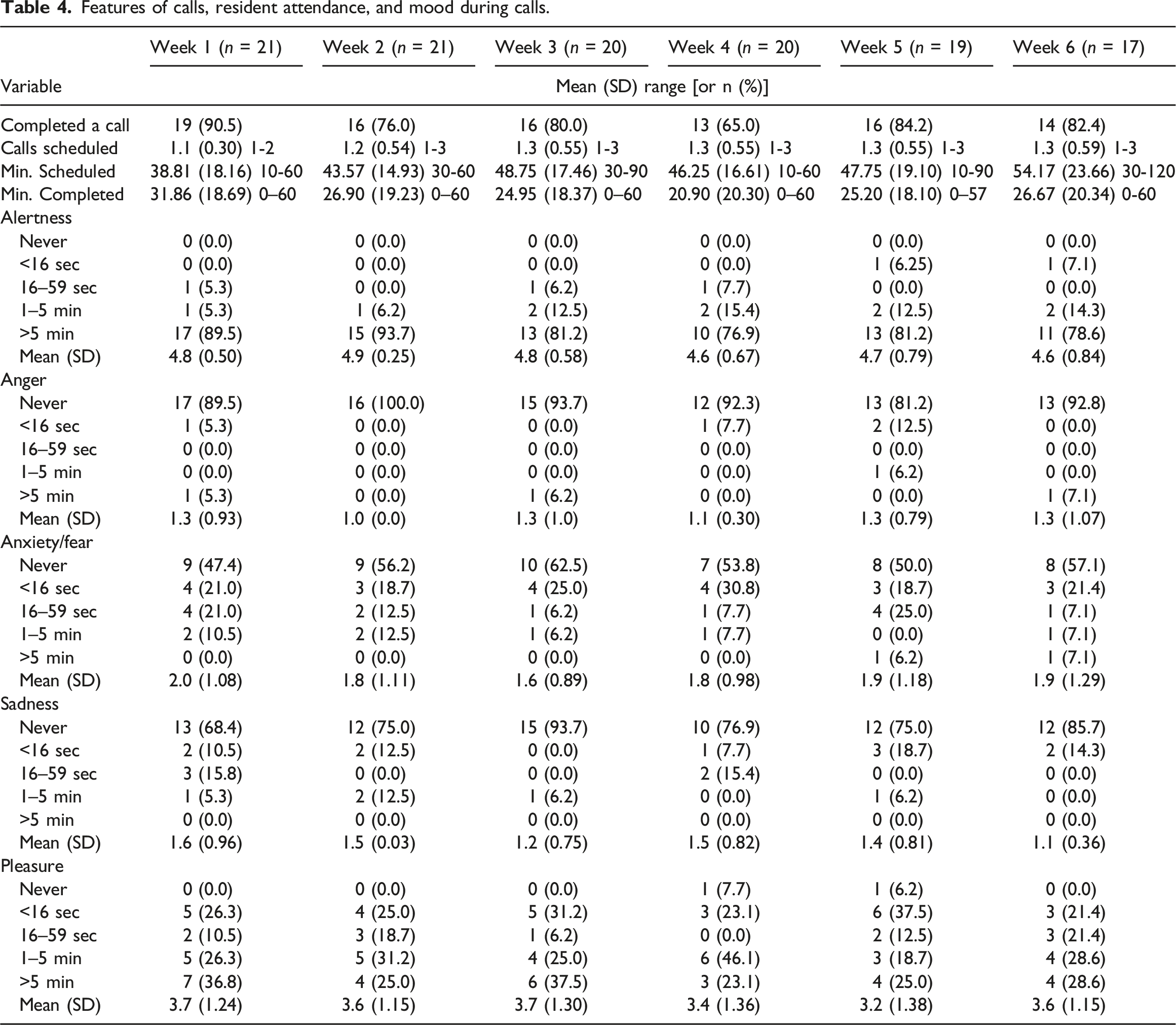
Acceptability
Features of calls, resident attendance, and mood during calls.
Remote visitor acceptability ratings (n = 24).
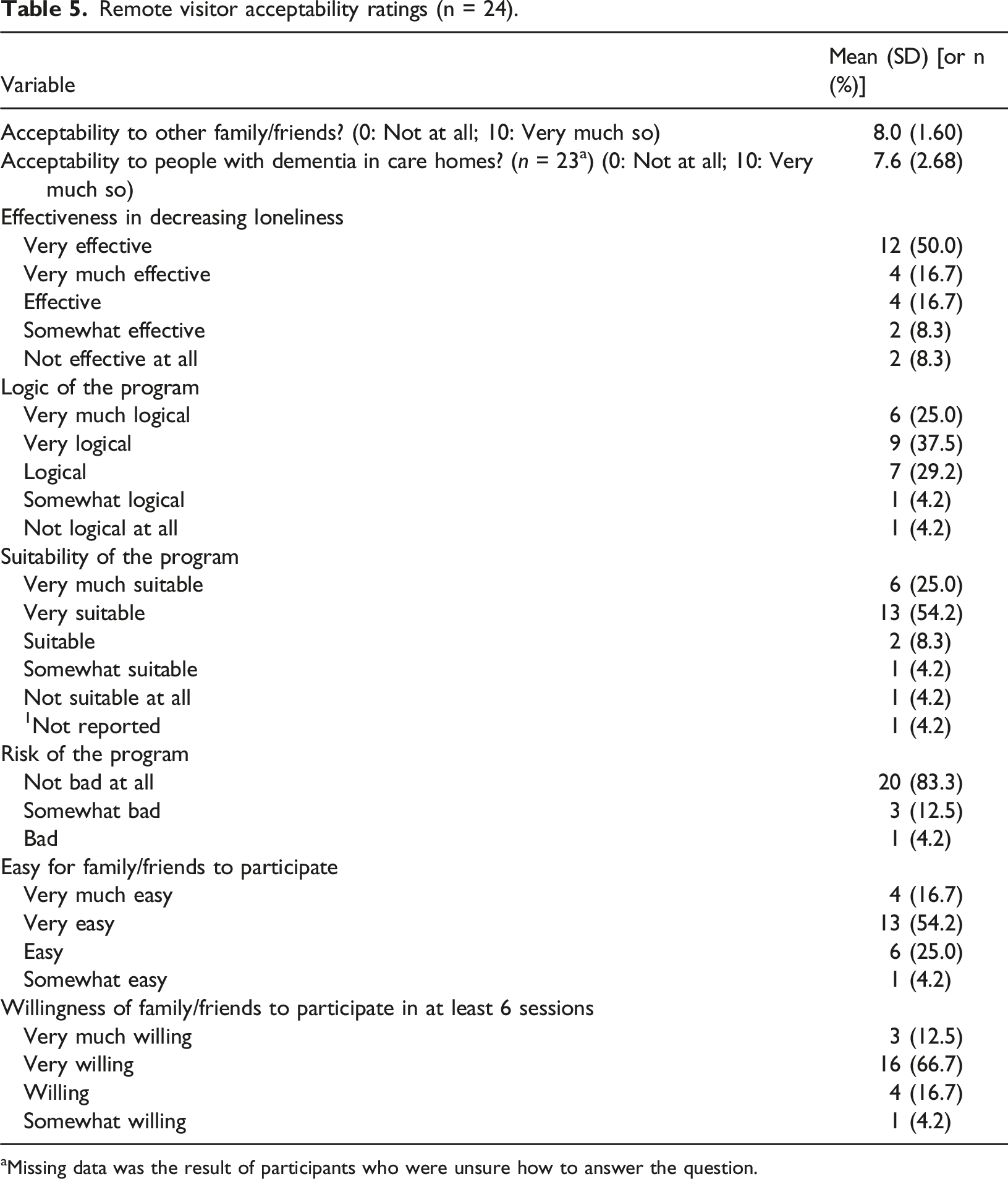
aMissing data was the result of participants who were unsure how to answer the question.
Discussion
The findings from this (Phase 2) feasibility study support the feasibility and acceptability of Connecting Today, a program that involves a trained facilitator who supports remote visits between people living with moderate to severe dementia in care homes and their care partners, family members or friends. Results also support the feasibility of planned approaches to recruitment and data collection for use in a future large (Phase 3) effectiveness trial. Below, we discuss key applications for future research and practice.
Feasibility
We delivered the intervention to 24 residents and their remote visitors, reflecting 19.7% of the total eligible resident population. Ours is the only study of a visiting program to include people living with severe dementia in care homes, and generated essential information about recruitment rates needed for planning larger studies. Previous pilot and feasibility studies have recruited 3 to 17 residents with mild to moderate dementia to participate; none have reported what proportion of the total eligible population their sample reflected (Moyle et al., 2014; Purves et al., 2015; Van Der Ploeg et al., 2016).
In relation to recruitment procedures, we excluded 133 people from the study (47% of the total population assessed) who did not have a dementia diagnosis. The prevalence of people living with dementia in care homes is at least 69% in Canada (Canadian Institute for Health Information (CIHI)., 2022), but a variety of social factors and co-morbid conditions lead to underdiagnosis (Bartfay et al., 2013). After establishing that Connecting Today works for people living with dementia (in a Phase 3 trial), future (Phase 4) implementation studies could assess the adaptations and effects of Connecting Today delivered in practice to people living with cognitive impairment in a care homes who do not have a formal dementia diagnosis (Pinnock et al., 2014).
In terms of retention, we observed a retention rate of 70.8% by 6 weeks in our facilitated remote visiting program. No one in our sample withdrew because of distress due to the intervention; withdrawals were primarily due to acute changes to resident health status. This suggests that participants may be interested to continue with Connecting Today visits for longer than 6 weeks, if there is no acute change in health status. In practice, Connecting Today could also be helpful if offered after recovery from an acute change in health status (e.g., following a hospitalization). However, research studies that aim primarily to look at program impacts should do so after 6 weeks, before study withdrawal rates exceed 30%.
In contrast to our findings, one other pilot study of a remote visiting program (n = 17) similarly used iPads and Skype, but included only people living with mild to moderate dementia, and their intervention was not facilitated beyond setting up the equipment (Van Der Ploeg et al., 2016). They observed that only 53% of their sample could complete 4 weeks of sessions. Most (63%) of their withdrawals resulted from inconsistent availability of the remote visitor and 11% due to resident distress from study methods, suggesting that their intervention was not acceptable to participants or feasible for use in care home populations (Van Der Ploeg et al., 2016). This highlights that a facilitator, a key component of the Connecting Today intervention, is needed to support positive interactions during remote visits in this population (Moyle et al., 2020).
Training on-site care staff to be the facilitators in an important strategy to support spread and sustainability (O’Cathain et al., 2019), if Connecting Today is found effective in future trials. Training on-site care staff to facilitate Connecting Today prevented missed visits due to infectious disease outbreaks, which can result in serious limitations as to who can enter the care home (Ickert et al., 2021). However, we excluded two participants before week one because of facilitator turnover, and recommend that future studies should train at least two facilitators at each site to prevent gaps in program delivery. In a future large trial, it would be important to interview key contacts at the participating sites (as a part of a concurrent process evaluation) to ask them whether and how facilitator training could be included in their future staff orientation programs. Findings from those interviews would inform future recommendations related to the use of Connecting Today in practice.
Regarding the duration of the intervention, previous research with older adults who were cognitively intact has used 6–12 weeks for the intervention period (Moses, 2003; Schwindenhammer, 2014; Tsai et al., 2010; Tsai & Tsai, 2011; Van der Heide et al., 2012). While we originally intended to offer 12 weeks of visits, a withdrawal rate of 29.2% by week 6 supported that a 12-weeks intervention period would not be feasible in future trials. In 43% of situations, withdrawal was related to the resident experiencing a decline in health (n = 1) or passing away (n = 2). Given that the average stay in care homes is less than 2 years in this complex and medically unstable population (Hoben et al., 2019), this suggests that facilitated remote visits should be offered to residents upon their admission to a care home in order to receive benefits from the intervention before they pass away or experience an acute health change (e.g., a fall, leading to hospitalization).
Completion of the DEMQOL-proxy by decision-makers resulted in very low levels of missing outcome data, which suggests appropriateness of this approach for outcome measurement in future (Phase 3) trials aimed at assessing intervention effectiveness. We observed missing data when decision-makers were not sure how to respond. In future studies, the tool can be reviewed with the decision-makers during the consent process so that they can identify someone else who knows the resident well to complete the DEMQOL-proxy, in the situation where they feel unsure if they can answer the questions. While some pilot studies may assess change in outcomes to explore ‘preliminary intervention effects’ for use in future sample size calculations (Lancaster, 2015), we chose not to in this feasibility study because of a high risk of both false negatives (e.g., resulting from small samples) and false positive results (e.g., resulting from imprecise and biased estimates of group differences) (Hertzog, 2008; Leon et al., 2012). We suggest that recent evidence identifying a minimum important difference on the DEMQOL measure (E. C. Lee et al., 2021) can be used in sample size calculations for future trials.
Acceptability
Most of the participants perceived Connecting Today as highly acceptable, assessed with validated scales. Similar to our previous assessment of acceptability of visiting programs (in general) (O’Rourke et al., 2020), remote visitors in Connecting Today reported that the intervention made sense as a way to address loneliness, and that it was easy to participate. A substantial majority of remote visitors (between 66.7% to 83%) rated the intervention in the top two levels of the 5-point Likert scale for each item. High acceptability likely contributed to our success in recruiting remote visitors to participate in the study, and can influence outcome achievement in future trials (Sidani & O’Rourke, 2022). Positive mood of residents during the sessions indicated their acceptability of Connecting Today visits. We can contrast findings from our feasibility study with that of the pilot study assessing use of an iPad and Skype, where some participants were distressed and therefore could not complete sessions (Van Der Ploeg et al., 2016). While reviews demonstrate a growing interest in technological solutions to promoting resident well-being (Bemelmans et al., 2012; Moyle et al., 2017), if we are to reach people living with moderate to severe dementia, our results support that a careful, tailored facilitation component is essential to promote acceptability and application of technology.
We assessed resident mood to understand resident acceptability. Enjoyment in the moment is, arguably, essential to quality of life in dementia; the creation of ‘quality of moment’ may be even more important that improvements in outcomes over longer time periods (e.g., at 6 weeks) in this population (Pringle, 2003). Mood assessment should be retained in future trials to be used as a process measure. It is also an intervention activity that supports tailoring, as it prompts the facilitator to assess how the sessions work for the resident so that they can adjust their approach accordingly.
Taken together, our findings suggest that the flexibility of the intervention was an important feature that supported both its feasibility and acceptability for use with people living dementia in care homes, and their family and friends. On average, more minutes per week were scheduled as compared to completed. This suggests that it is sufficient to offer 60 min per week of scheduled visits. The intervention dose was flexible and the engagement activities were individually tailored, features that have been highlighted as important to acceptability of visiting programs in our previous study (O’Rourke et al., 2020). While many people living with dementia in our sample engaged in calls that were short in duration, their experiences during those short calls were positive, suggesting that they find short calls meaningful and acceptable. Attendance each week was also flexible and optional. For 6 weeks, we completed a call with 65%–90% of residents each week. The most common reasons for missed calls during Connecting Today were that the visitor was not available or that the resident had poor energy in a particular week. Those situations are to be expected in this population, and do not necessarily indicate that Connecting Today is not acceptable, particularly if they choose to continue with the intervention in subsequent weeks. Only one person withdrew due to the features of the intervention (i.e., internet connectivity issues), no one withdrew because of the call schedule, and the ratings from both residents and their family and friends on other measures indicated high acceptability. Future research will need to be conducted to assess how missed visits may contribute to outcome achievement. Depending on the results of (Phase 3) effectiveness trials, it may be important to consider combining live visits with simulated presence in order to augment treatment effects. Simulated presence involves playing audio or video-recorded messages for the person living with dementia, and has been explored in small feasibility studies (Hung et al., 2018; Peak & Cheston, 2002). Our findings support that a higher dose of scheduled, facilitated live remote visits may not be acceptable to remote visitors and is unlikely to be feasible for implementation in care homes.
Strengths and limitations
Our study to understand feasibility and acceptability had several strengths. We recruited 24 participants with moderate to severe dementia and their remote visitors (more than the minimum of 20 participants that we required). Our recruitment strategy can be re-produced in future trials, and our methods allowed us to estimate the proportion eligible from the total number of residents in the care home. We demonstrated that it is possible to train on-site care home providers to deliver Connecting Today, a feature that will be necessary for future use of the program in large trials and in practice. In the future, it will be important to train more than 1 facilitator at each home, in case of facilitator absences. We assessed acceptability using validated measures. Limitations of this study included a smaller-than-required sample size to estimate resident mood each week due to missing data; lack of cultural diversity; and we did not recruit anyone living with mild dementia. While it is a study strength that our sample is representative of the target population, future studies are needed to assess feasibility and acceptability of Connecting Today among people living with mild dementia and from diverse cultural backgrounds.
Conclusion
Connecting Today is a feasible and acceptable facilitated remote visiting program for use with people living with moderate to severe cognitive impairment in care homes. The results of this Phase 2 feasibility study support the high acceptability of the intervention, from the perspectives of both the residents and their remote visitors, and lay a critical foundation to support planning for future studies. A large randomized controlled trial is the logical next step to assess Connecting Today’s effectiveness to promote social connectedness and quality of life.
Footnotes
Acknowledgements
We thank Heather Hanson (Alberta Health Services, Seniors Health Strategic Clinical Network), Sandra Woodhead Lyons (Institute for Continuing Care Education and Research), Heather Roland (Seniors’ Centre Without Walls), Suzanne Maisey (Alberta Health Continuing Care Branch), Carla Ickert and Jen Rygus (Capital Care) for their participation on the advisory committee. Their insights were essential to support the design of an intervention appropriate for care home populations, to recruit participants, and disseminate findings. We thank the site facilitators for sharing their expertise in supporting residents’ social interaction, and for their creativity and tenacity to promote engagement during Connecting Today sessions. We extend thanks to the study participants for sharing their expertise, time, energy and ideas to support tailoring of Connecting Today sessions to meet individual needs.
Authors’ contributions
HMO conceptualized, designed and obtained funding for the study, oversaw analysis, interpreted findings, and wrote the manuscript. JS supported study design, prepared ethics applications and oversaw all data collection. DC supported recruitment and data collection. FLFDP and HL completed data analysis and FLFDP prepared manuscript tables. MH, TH, KM, and VB participated in study conceptualization and interpretation of findings. All authors reviewed manuscript drafts for critical intellectual content, and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Alzheimer Society Research Program New Investigator grant (19-21) and a Professorship in Dementia Care Interventions from the Faculty of Nursing, University of Alberta.
Ethics approval and consent to participate
Written or oral consent for participation was obtained. Assent to participate was assessed before and during every research activity. Ethics approval for this study was received from the University of Alberta (PRO 00084244). Operational approval was obtained from the continuing care operator to conduct research in the two study sites.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available because participants consented to share data only with the research team. De-identified data are available from the corresponding author on reasonable request.