
Abstract
Background
Although published studies have examined the perceptions of caregivers who are attending to older adults with dementia concerning the values of human dignity and/or autonomy in institutional settings, none have explored the possible differences in actual behavior that relates to these values for caregivers from diverse ethno-cultural backgrounds.
Aims
Explore how caregivers with varied cultural backgrounds may differ in their real-time behavior regarding the autonomy and dignity of older adults with dementia and thereby determine whether that real-time behavior reveals new aspects of respect and disrespect for both the autonomy and dignity of those older adults.
Research Design and Methods
A qualitative research based on non-participatory observations, was meticulously recorded using a written journal and a rigorous microanalysis to analyze the collected data. We made 58 shift-based observations (morning and evening) of 29 caregivers from 3 ethno-cultural groups working in 3 nursing homes in Israel. These groups included Israeli-born Jews (Sabras), Israeli Arab-Muslims (Arabs), and immigrants from the Former Soviet Union (IFSU).
Results
(1) IFSU caregivers demonstrated more respect for autonomy and dignity, but also demonstrated disrespect for these values. (2) the main difference between the IFSU caregivers and other caregiver groups pertained to respect for their autonomy. The main specific facets of autonomy where IFSU caregivers surpassed their colleagues were information provision and persuasion. (3) toward both autonomy and dignity of these older adults, previously unaccounted for in the models we used, were discovered among the varied groups of caregivers, with only minor gaps between these groups.
Discussion and Implications
This study—the first of its kind to focus on the real-time behaviors of caregivers from diverse ethno-cultural backgrounds—reveals the potential effects of culture on applying practices related to dignity and autonomy during daily care. The findings may have important implications for caregiver training in multicultural societies.
Introduction
According to a 2015 UN report, the world fertility rate is declining, while life expectancy is steadily increasing, thereby leading to an increasingly aging population. A key chronic disease that primarily (although not exclusively) targets older people is dementia (Aledeh & Habib Adam, 2020; Ekoh et al., 2020), characterized by pathological changes in the brain that significantly impair both cognitive and behavioral functions. Studies have found that about two-thirds of dementia patients are hospitalized in nursing homes, usually when they are in the advanced phases of the disease (Bentwich, Dickman, et al., 2018a; Bickel, 1998).
A main problem for older adults in nursing homes is the lack of personal control that characterizes their daily routine. The last two decades have supposedly witnessed a shift in this regard toward a person-centered care (PCC) paradigm. One of its central principles is autonomy—in particular, more respect for patients’ autonomous control over their decisions—which also plays a crucial role in overall healthcare ethics (Bentwich, Dickman, et al., 2018a). However, the living experience of older adults with dementia who are residing in nursing homes was described by a team of Scandinavian researchers as “living in [a] prison without bars” (Heggestad et al., 2013).
Against this backdrop, several previous studies have investigated the extent to which autonomy is respected and nurtured in the context of older adult care in nursing homes, including for older adults with dementia, mainly by interviewing their caregivers (Furtado et al., 2021; Leino-Kilpi, et al., 2003b; Moilanen et al., 2021; Schopp et al., 2003; Scott, 2003a; Scott, et al., 2003b; Wikström & Emilsson, 2014). In a similar vein, the importance of respecting the human dignity of older adults, especially in nursing homes, has also been acknowledged (Heggestad et al., 2013). Specifically, the typology of human dignity, as devised by Lennart Nordenfelt, emphasizes the lack of sufficient respect for dignity in older age. According to Nordenfelt’s typology, four distinct dimensions of dignity are notable as universal aspects, namely, (a) dignity of merit, (b) dignity of moral stature, (c) dignity of identity, and (d) human dignity or (menschwürde) (Nordenfelt, 2004; Nordenfelt & Edgar, 2005). Given this typology, the loss of the dignity of identity is associated with older age, given the societal tendency to “forget” about the individual identity of older adults, especially those with physical or cognitive disabilities. In fact, the studies that have investigated the respect for autonomy and dignity in nursing homes have yielded different models for the facets of autonomy found in older people care, including two pivotal models specifically related to the care for older adults with dementia in nursing homes, as based on a large number of interviews (Leino-Kilpi, et al., 2003a; Scott, 2003a; Scott, et al., 2003b; Tranvåg et al., 2013).
A decade ago, a 2012 World Health Organization report established that the reality of dementia care is increasingly based on multicultural caregivers, as they had become the vast majority of that workforce (WHO, 2012). Indeed, previous research by Bentwich and her colleagues showed that, contrary to earlier studies in nursing homes, different ethno-cultural groups have significantly different perceptions regarding the dignity and autonomy of older adults with dementia (Bentwich et al., 2017; Bentwich, Dickman, et al., 2018a, 2018b). In addition, for one of the main ethno-cultural groups of caregivers that Bentwich and her colleagues studied (i.e., immigrants from the former Soviet Union), an earlier study found similar results regarding limited respect for the autonomy of patients with dementia on the part of these particular caregivers (Iecovich & Rabin, 2014).
A culture includes collections of values, beliefs, and habits learned during socialization, which then shape the spheres of ideas, perceptions, and decisions, and how those individuals act and react (Doswell & Erlen, 1998; Rassin, 2008). In other words, each caregiver has his/her own particular collection of cultural values, which that individual then carries into the caring interface with the patient. Indeed, people from diverse ethno-cultural backgrounds have been shown to have varied attitudes toward older adults (Zhou, 2007). It has also been suggested that family caregivers from different cultural and ethno-cultural groups may have different perceptions regarding people with dementia and the ways of coping with the situation of caring for their loved ones who are suffering from this illness (Nielsen et al., 2021, 2022). According to a review study by Botsford and colleagues on the influence of ethno-cultural background on dementia and caregiving, that aspect seems to be responsible for differences in dementia and caregiving experiences. Notably, it was discovered that culture has a substantial impact on how people perceive dementia and care. Additionally, this study emphasizes the ongoing need for examining how ethno-cultural background affects and shapes care experiences (Botsford et al., 2011)
Still, thus far, none of the published studies on the perceptions of human dignity and/or autonomy within institutional settings have examined whether and how these possible differences between caregivers from diverse ethno-cultural backgrounds also appear in their actual behavior. In addition, the facets of dignity and autonomy in the context of care for older adults with dementia have not yet been explored based on the actual behavior of caregivers from diverse cultural backgrounds when caring for this population of aging adults.
Supposedly, caregivers’ perceptions are ultimately expected to evolve into a corresponding behavior fitting their perceptions (Chaiklin, 2011; Geller, 1992). However, in fact, previous research in social sciences shows that this might not be the case. Hence, varied studies do indicate the critical need to examine actual specific behavior, not merely probe for general attitudes and ideas (Al-Krenawi & Graham, 2005; Chaiklin, 2011; Davis, 1985; Pestello, 2007; Pestello & Pestello, 1991).
Aim of the Study
This study explores whether and how caregivers’ cultural background may shape their real-time behaviors regarding aspects of human dignity and autonomy or their lack thereof in their daily care of older adults with dementia. The study also examines whether such real-time behaviors in this circumstance can reveal new facets of dignity and autonomy or a lack of these key characteristics.
Methodology
Research Design
This study is an ethnographic qualitative empirical ethics research utilizing non-participatory field observations of caregivers from various cultural backgrounds for the data collection, and a microanalysis to analyze the collected data (Bavelas et al., 2000; Erickson, 1992, 1996). The first author, a social worker with 17-year experience as a social worker of a nursing home and a PhD candidate at the time of performing the study, carried out the observations on two separate shifts per caregiver (i.e., morning and evening). The second author is a bioethicist with both experience and interest in studies related to culture and the care for older people and was the PhD advisor of the first author. It should be noted that the field-observations based study reported here was part of a larger study that also included interviews with some of the observed caregivers, as well as more rich informants (e.g., head nurses, senior social workers, managers of the observed nursing homes). However, it is well beyond the scope of a single article to describe and account for all the results and their implications of both interviews and observations. Therefore, in the current article, we focus on the observations segment of the study alone, and compare it in the Discussion section to previous relevant literature that mainly focused on interviews or questionnaires (rather than real-time observations).
Research Population
This study’s population included 29 formal caregivers (sometimes known as nurses’ aides) from three ethno-cultural groups: 10 Israeli-born Jews (Sabras), 10 Israeli Arab-Muslims (Arabs), and 9 immigrants from the former Soviet Union (IFSU). The inclusion criteria for the study were any caregiver (female or male) in the nursing homes enrolled in the study who was affiliated with one of the ethno-cultural groups and who has at least 2 years of experience in their job. These caregivers were chosen from three nursing homes in Israel, where they work in specialized units for older adults with dementia. They were selected for the study using purposive sampling and were approached in their workspace face-to-face directly by the first author. Three caregivers decided not to participate in the study, and their decision was honored without any further attempts to recruit them later. Moreover, one caregiver from the former Soviet Union declined to participate in the study after field observation had begun. Since there were no more IFSU caregivers in either of the three nursing homes, the research population did not reach the symmetrical number of 30 caregivers. However, please note that saturation was reached (i.e., the observed caring routine did not seem to yield new themes of autonomy or dignity) by the time the analysis of the 8th–9th caregiver per each of the observed cultural groups was conducted, thereby indicating that there was no need to recruit any further participants for the study.
This population of caregivers yielded 58 field observations. These three cultural groups of formal caregivers represent key groups of formal care providers working with older adults with dementia in many of the nursing homes in Israel. Based on previous research, it was assumed that the Sabra caregivers group had a potentially more Western-liberal perception (Remennick, 2002; Zisberg et al., 2015). Following Bentwich and colleagues’ research, the current study chose Arabs and IFSU caregivers to represent multicultural perspectives—namely, a supposedly non-Western perspective. Given the limited space here, further elaboration of the cultural distinctiveness of these groups in Israel can be found elsewhere (Bentwich, Dickman, et al., 2018a; Bentwich, Dickman, Oberman, et al., 2018c); still, in the Discussion section, we do elaborate on the cultural facets of these groups that are relevant for explaining and further substantiating the results of the current study.
Data Collection
In this study, data were collected using non-participatory field observations of the caregivers in their actual work environment (i.e., nursing home), with an emphasis on their interactions (verbal and non-verbal) with residents with dementia. No relationship with the caregivers was established prior to study commencement in order to facilitate as ‘neutral’ observations as possible on the part of the researcher who conducted the observations. Caregivers were notified upon the beginning of each observation, but the observer kept some distance to allow as “natural” an environment as possible for the caregivers (e.g., the observer sat in the corner of the room). The caregivers were also notified that the first author (who conducted the observations) was a PhD candidate at the time of the study and doing ethnographic field work for his dissertation, stemming from his personal interest and past background as a social worker delivering institutional care for patients with dementia.
All observations were carefully documented in field notes by the same observer (i.e., the first author). The qualitative research literature considers the documentation of real-time field observations as a fundamental methodology, as it allows for a genuine reflection of the reality being studied (Fitzpatrick & Boulton, 1994). Specifically, this kind of methodology has been found to be extremely effective when a researcher is interested in describing and conceptualizing the daily practice of care, as in the case of our study (Bolmsjö et al., 2006). Furthermore, non-participatory observations also allow the researcher to concentrate on observation and develop optimal sensitivity to the myriad of complex meanings of those observations in real-time compared to using participatory observations (Krathwohl, 1993).
Admittedly, the observer immigrated from the former Soviet Union in his early childhood (i.e., at the age of 5), thereby theoretically positioning him as having affinity to one of the observed ethno-cultural groups (i.e., IFSU caregivers). However, the same thing could be said had he been born in Israel as a Jew or an Arab, thereby theoretically creating an affinity with one of the other observed ethno-cultural groups of caregivers (i.e., Sabras and Arabs, respectively). Moreover, we trust that the meticulous field notes taken during the observations, coupled with the fact that these field notes were analyzed only after all observations were performed, created a research environment that minimized any possible crude bias in the analysis of the data. We further elaborate on this point in the next sub-section – Data Analysis-when discussing the steps that were taken to achieve trustworthiness.
In the current study, 58 observations were conducted in two full shifts: morning (6:00–14:00) and evening (15:00–20:00). The conscious choice to observe each caregiver twice was based on a solid rationale—namely, the differential and unique nature of the tasks during each shift might shape the interactions between caregivers and patients. The shifts were continuous without substantial breaks, excluding negligible, very short bathroom breaks that those caregivers took between routine tasks.
It’s also important to emphasize the broad scope of the observations conducted in the current study compared to previous studies that focused on autonomy and human dignity. Thus, to the best of our knowledge, none of the previous studies spanned more than 500 hours of field observations. For example, in Orlov and Niko’s study conducted in a nursing home for patients with dementia in Sweden, the data consisted of around 150 hours of video recordings and complementary field notes. This study focused on events concerning human dignity only, without reference to patient autonomy (Örulv & Nikku, 2007). In another study conducted in Sweden, the goal was to explore how one woman with severe dementia and so-called behavioral disturbances acted in relation to her care providers and how the care providers acted in relation to her. To meet this goal, 14 participant observations, including one woman with dementia and six care providers, were performed. All these observations were made during the morning shifts - about 2 hours a day, within a limited scope of 28 hours (Graneheim et al., 2001). In a study conducted in Norway, how the dignity of patients with dementia is preserved or harmed when they live in a nursing home was examined. Observations were made of 15 patients with dementia in two nursing homes. The observations focused exclusively on the morning hours (07:30 - 10:00). Moreover, this study focused more on patients and their relatives and not on caregivers. Altogether, the length of these observations was still around 185 hours (Heggestad et al., 2015).
Data Analysis
In qualitative research, data are analyzed by arranging and constructing the information collected to interpret and understand the diverse meanings inherent in that data (Polkinghorne, 2005). This analytical process aims to provide meaning to, then interpret, and generalize the phenomenon being studied (Puurveen et al., 2015). In this study, the analysis was done via an ethnographic microanalysis of interaction (also known as micro-ethnography) as informed by two models of human dignity and autonomy in the context of the care for older adults in an institutional setting. The microanalysis was performed on the content of the observations to identify the existing facets of human dignity and autonomy found in the models used in this study (see below for further details) and look for new facets that have not yet been reflected in any of the existing models (Bavelas et al., 2000; Erickson, 1992; Jones, 2007; Lotzkar & Bottorff, 2001).
This current analysis of the direct interactions between caregivers and older adults with dementia allows a high resolution of detail regarding the communication and conduct of caregivers in real-time (Erickson, 1996; Garcez, 1997; Guillemin & Gillam, 2004; Truog et al., 2015). The importance of using microanalysis is that this analysis can illuminate the prevalence of the various facets of dignity and autonomy for each caregiver’s examined observations. By shedding light on the prevalence of different facets of respect and disrespect toward autonomy and dignity among different cultural groups of caregivers who are attending to patients with dementia, the current study offers a more nuanced understanding of the actual implementation of these different facets among varied cultural groups of caregivers. In fact, the current study follows the footsteps of previous micro-ethnographic research precisely used in the context of studying the interactions of caregivers with older adults (i.e., (Grainger, 1993; Silverman, 2013; Silverman, 2016)), and studying the verbal and non-verbal expressions of persons living with dementia as indicators of PCC giving (Staehler et al., 2022). Our study also takes its inspiration from other qualitative field observations studies that were specifically done in order to trace differences between cultural groups that could not be pinpointed using standard quantitative questionnaires (Motta-Ochoa et al., 2021; Rochanavibhata & Marian, 2022). In addition, through the Discussion section that follows, possible explanations for the main differences that were found between the cultural groups of caregivers are presented to highlight some of the possible cultural underpinnings for these differences.
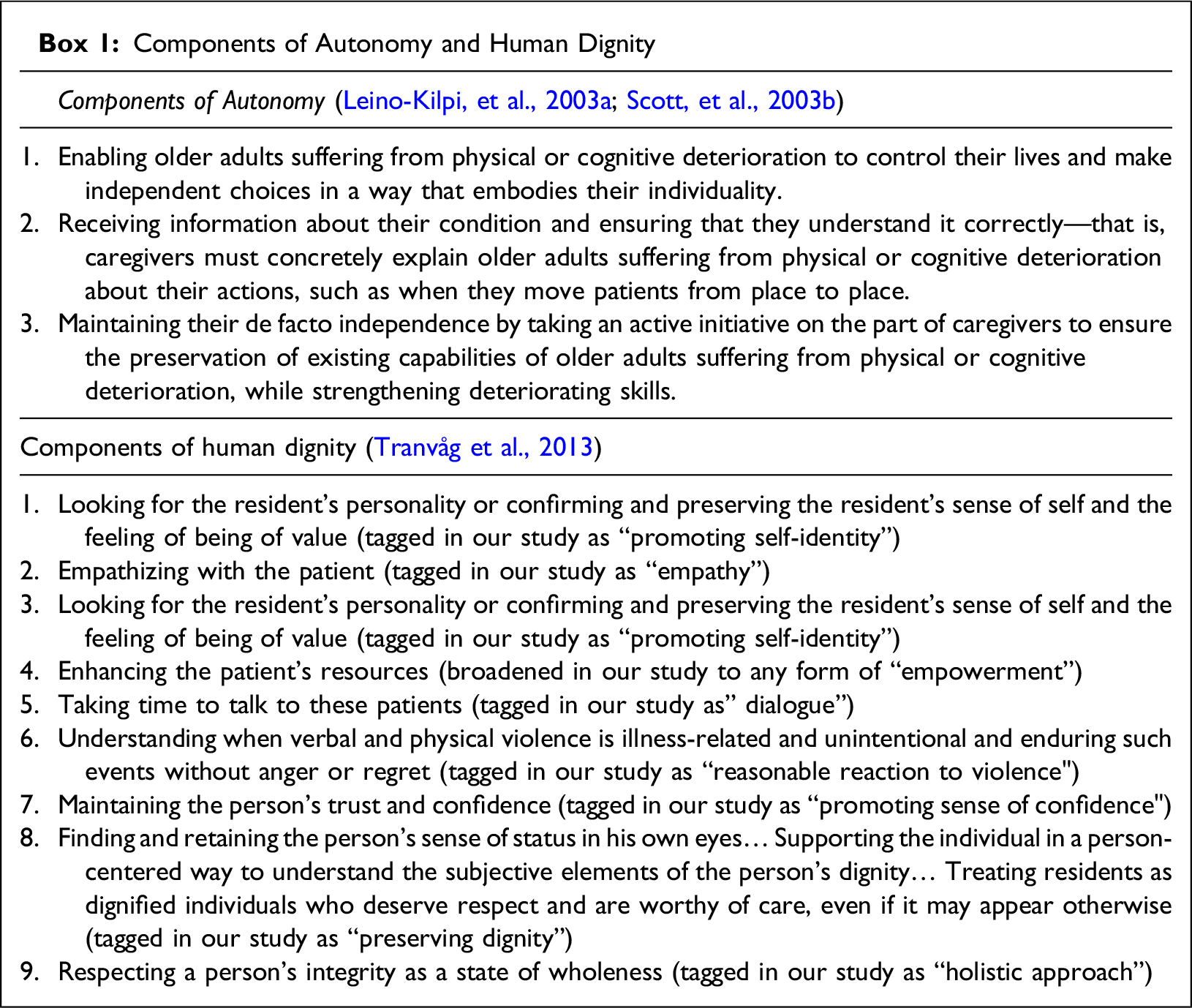
In the current study, two theoretical frameworks were employed as the basis for the microanalysis, both of which were briefly mentioned here in the Introduction. The first is the theoretical framework of autonomy developed by Leino-Kilpi and colleagues (Leino-Kilpi, Välimäki, Dassen, Gasull, Lemonidou, Schopp, et al., 2003a; Scott, Välimäki, Leino-Kilpi, Dassen, Gasull, Lemonidou, Arndt, Schopp et al., 2003b). This model was developed in a large-scale study in five European countries (Finland, Spain, Greece, Germany, and Scotland). According to this model, three main themes play a key role in the respect or lack of it for the autonomy of older adults suffering from physical or cognitive deterioration. The second theoretical framework relates to the general concept of human dignity. As this study pertains explicitly to institutionalized nursing care of older adults with dementia, we chose the conceptualization of the dignity model as synthesized in Tranvåg and colleagues’ study that was specifically focused on that context (Tranvåg et al., 2013). However, we omitted the components that pertained to autonomy, as we wished to explore the two values separately. This novel model was informed by previous studies that pertained to gathering in-depth insights into long-term nursing care of people with dementia and identifying essential caring aspects for preserving their dignity (i.e., (Zingmark et al., 2002)). We chose to base our analysis on the latter model by Tranvåg and colleagues (Tranvåg et al., 2013), because in this study, in addition to the components illustrated in Zingmark et al.'s study, there are also additional components from other studies (e.g., “empathizing with the patient” as illustrated in (Randers & Mattiasson, 2004)).
Box 1 presents the three components of autonomy taken from Leino-Kilpi et al.'s model of autonomy, as well as nine components extracted from Tranvåg et al.'s model of human dignity that were used in the current study.
Components of Autonomy and Human Dignity
The microanalysis comprised three main stages. First, each interaction instance was classified into the relevant components of autonomy and/or human dignity according to the models by Tranvåg and Leino-Kilpi and colleagues, thereby employing the template-coding method (King, 1998). In cases where no appropriate classification was found (e.g., facets of disrespect were not included in these models), suitable classifications were added. In the second stage, we counted each of the interaction instances of the various components that related to autonomy and/or dignity (and/or the lack thereof) extracted during the previous stage of analysis. This counting was done per the observations of the caregivers (morning and evening, separately), so that at the end of this stage, we were able to obtain the number of interaction instances for each observed component that related to dignity or autonomy during each caregiver’s observed shift. In this stage, we also calculated the sum of interaction instances that reflected the components of autonomy and human dignity, or the lack thereof, for each caregiver’s observed shift. In the third stage, we opted to generate an aggregate overview of the prevalence of facets of autonomy or dignity (or the lack thereof) for each cultural group of caregivers by calculating the medians and means of interaction instances of autonomy and dignity for each cultural group of caregivers, as informed by the sums of interaction instances that reflected the components of autonomy and dignity, or the lack thereof, as calculated per caregiver in the previous stage. For further clarity, these three main stages are further explained in the Results section.
By employing the aforementioned structured 3-step careful analysis, we aimed at achieving an adequate level of trustworthiness for the study. For example, using a template-based analysis for the acquired data, allowed us to examine the data established through structured lenses, thereby decreasing the amount of unaccounted-for interpretation. In a similar vein, 10% of the raw data was coded separately by both authors, thereby achieving an inter-rater reliability rate of 80%, which constitutes a high degree of agreement between the two authors. By forming the analysis based on as many as nearly 60 observations, including two observations per caregiver, a basic triangulation was achieved, which was further strengthened by comparing our resulted analysis to other sources of information in the Discussion section.
Ethical Considerations
Ethical approval for this research was granted by the applicable Ethics in Research committee (IRB). The two main ethical issues in this study were ensuring the informed consent of the caregivers regarding their voluntary participation in the study and maintaining the confidentiality of the information collected during the fieldwork observations. Participating caregivers signed an informed consent form indicating that their involvement in the study was fundamentally voluntary and that they had the right at any time to decide to terminate their participation in the study. The documentation did not identify the patients but focused solely on the caregivers’ nursing care routine. As the patients were not part of the study population, their consent was not required. In addition, no visual or audio documentation was gathered, meaning there was no risk of identifying the patients. Finally, none of the collected data included any identifying information that might jeopardize any of the informants’ confidentiality.
Results
In what follows, we describe the main findings of the current study. We begin by illustrating the professional and cultural background of the informants, followed by indicating the building blocks of our analysis—namely, showing examples of the key components of autonomy and human dignity, or the lack thereof, along with a full analysis of a single observation full analysis. We then present the main overall findings of the data analysis, with an emphasis on differences found among the three cultural groups of caregivers on the one hand and new facets of human dignity and autonomy that the current study uncovered on the other hand.
The professional and cultural background of the informants (N = 29).
Building Blocks: Examples
Observation log excerpt and its corresponding themes of respect and disrespect for autonomy and human dignity (morning observation of Carolina).
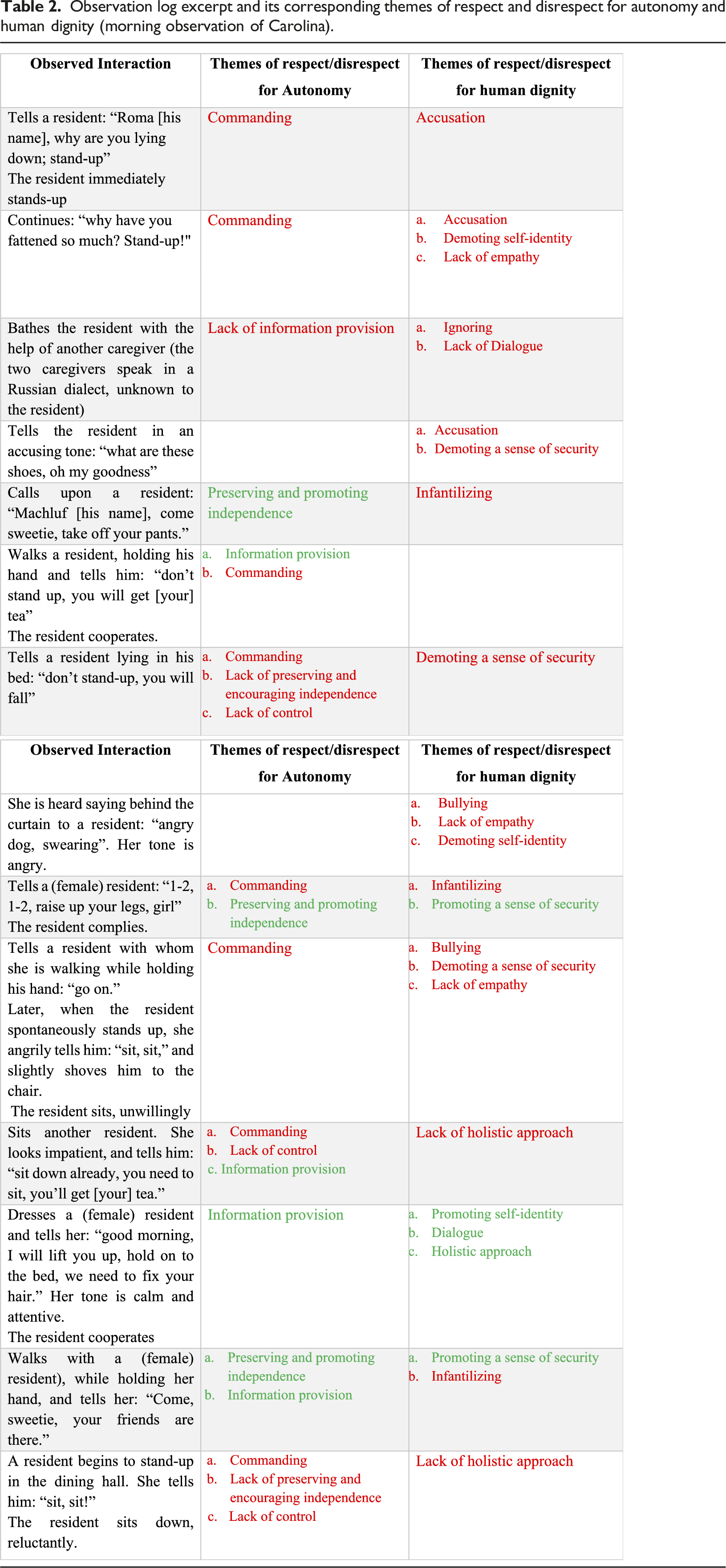
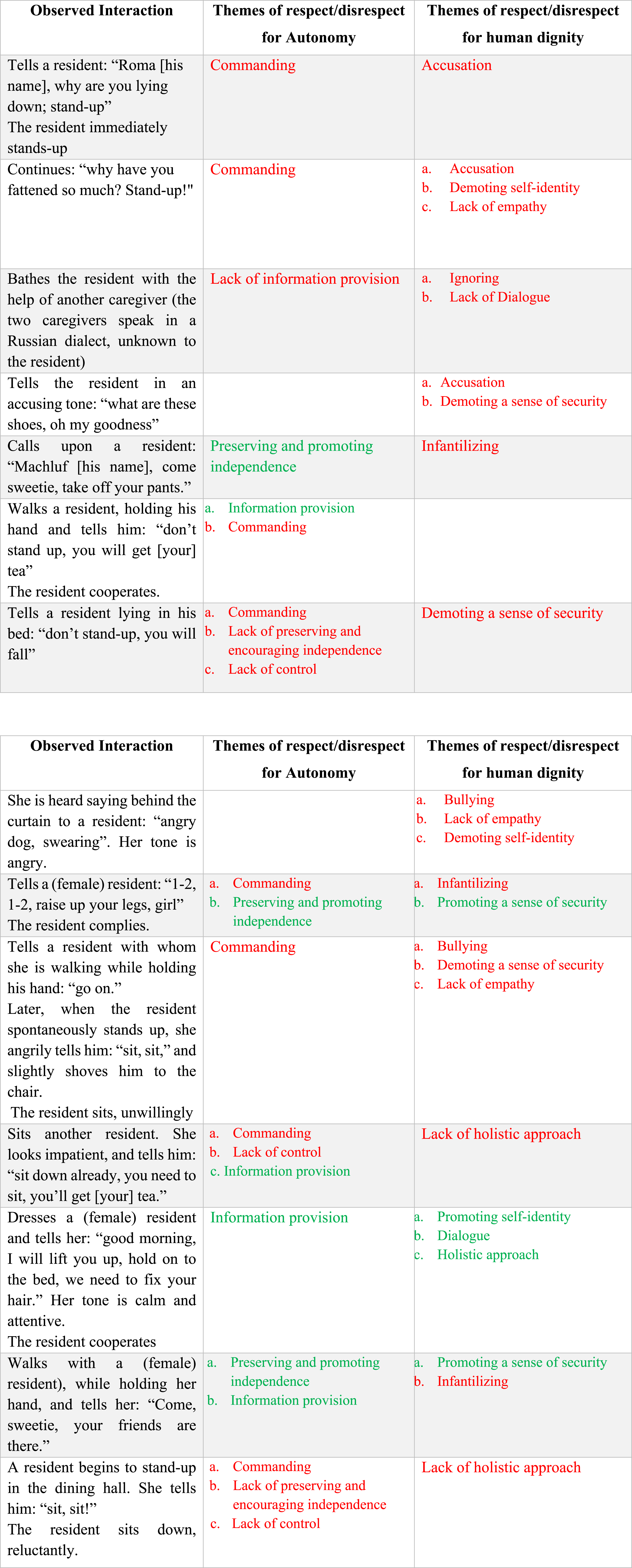
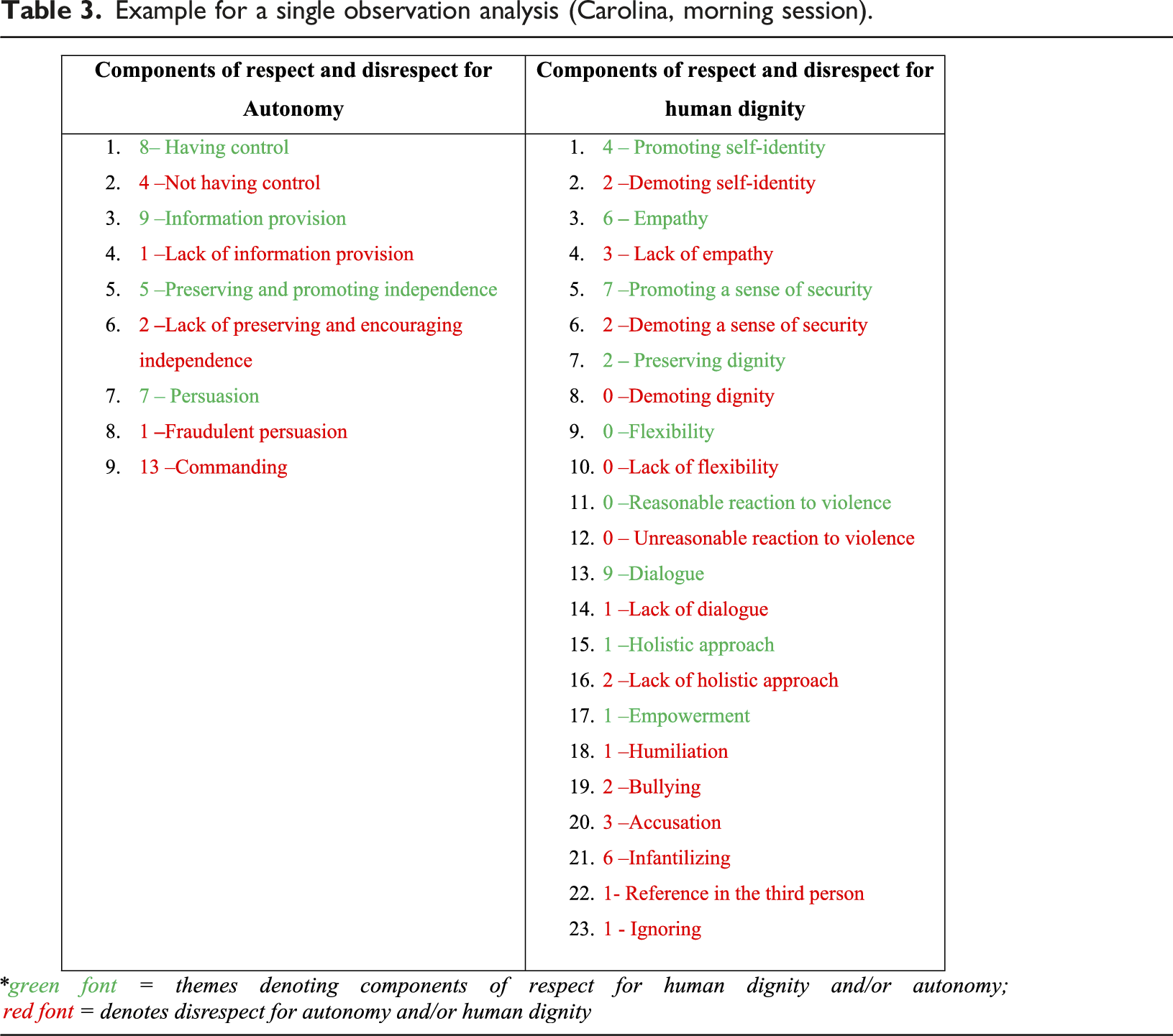
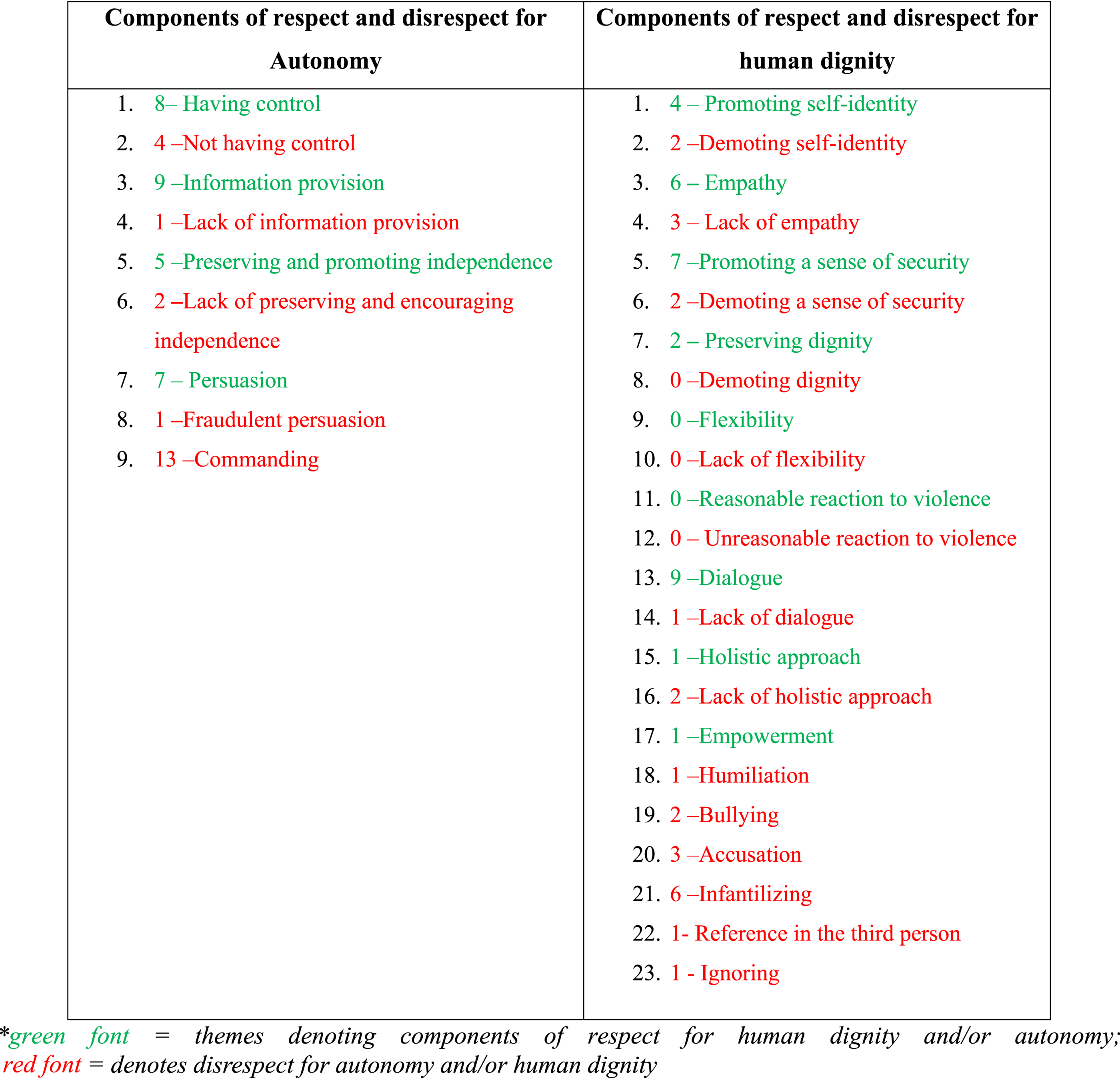
Compare, for example, the following two interactions were included in the observation of Carolina, as presented in Table 2. 1) Walks with a (female) resident while holding her hand and tells her: “Come, sweetie, your friends are there.” 2) Sits with another resident. She looks impatient and tells him: “Sit down already. You need to sit. You’ll get [your] tea.”
Both interactions manifested a mixed image of the preservation of dignity and autonomy, and the proportion of preservation and lack thereof are quite different. The first instance mainly shows the advocacy of autonomy (i.e., preserving and promoting independence, information provision) and human dignity (i.e., promoting a sense of security) while displaying only a minor lack of human dignity or disrespect for it (i.e., infantilizing). In contrast, the second instance mainly manifests a lack of respect for autonomy (i.e., command, lack of control) and human dignity (i.e., lack of holistic approach) while displaying only limited respect for the resident’s autonomy (i.e., providing information).
Example for a single observation analysis (Carolina, morning session).
Key Differences Between the Cultural Groups of Observed Caregivers
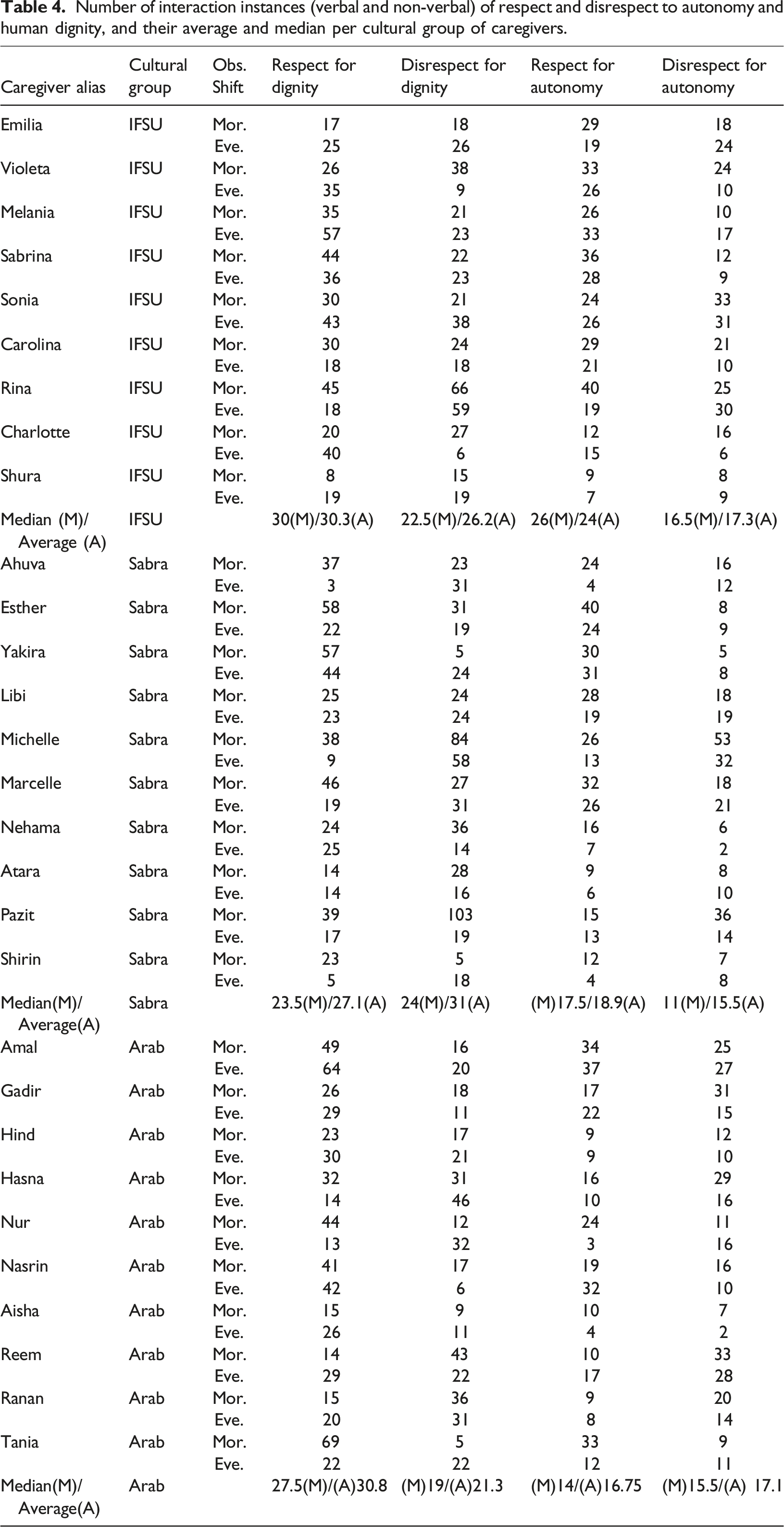
Number of interaction instances (verbal and non-verbal) of respect and disrespect to autonomy and human dignity, and their average and median per cultural group of caregivers.
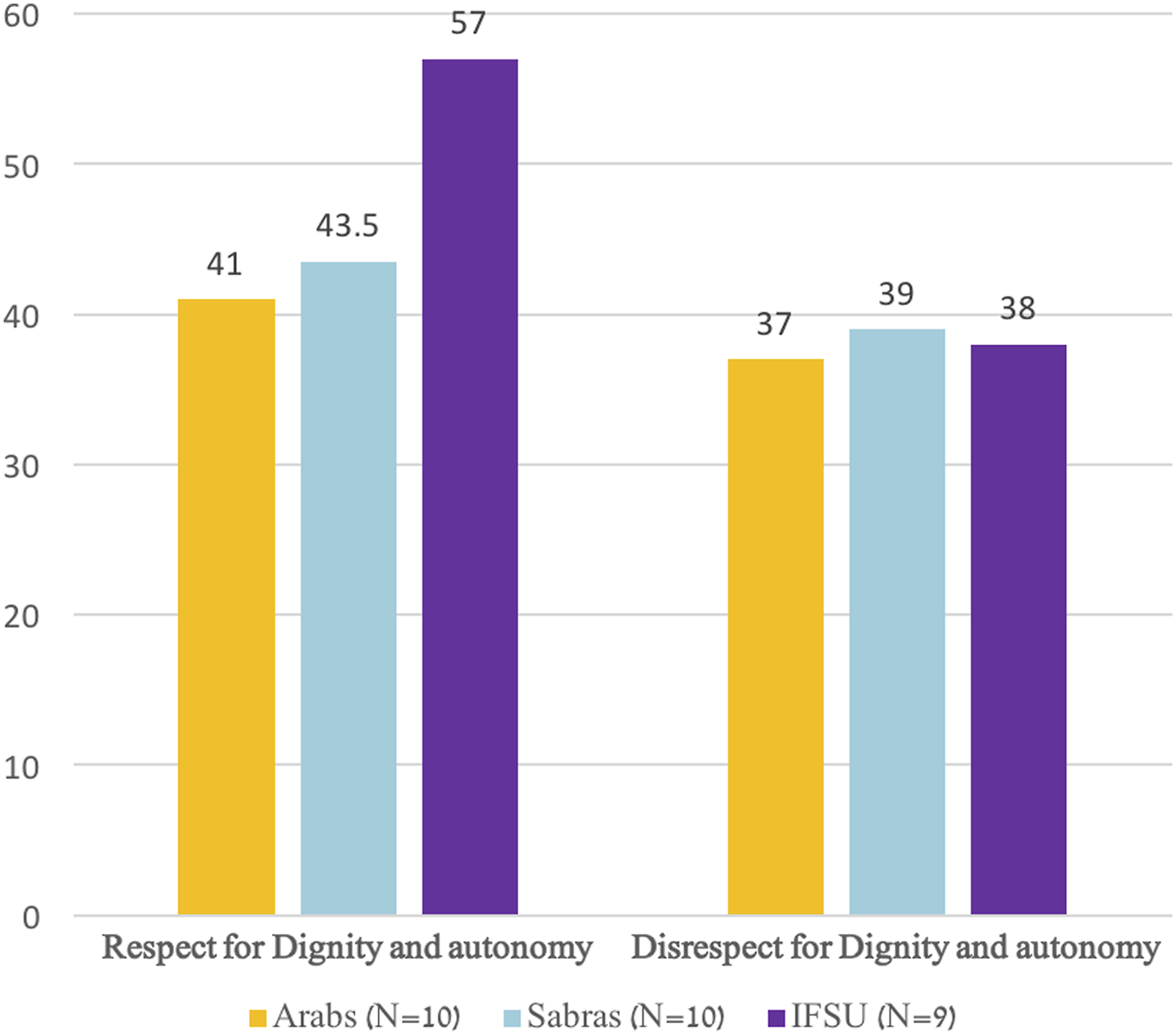
Overall respect and disrespect to autonomy and dignity, combined.
Detailed respect and disrespect to autonomy and dignity.
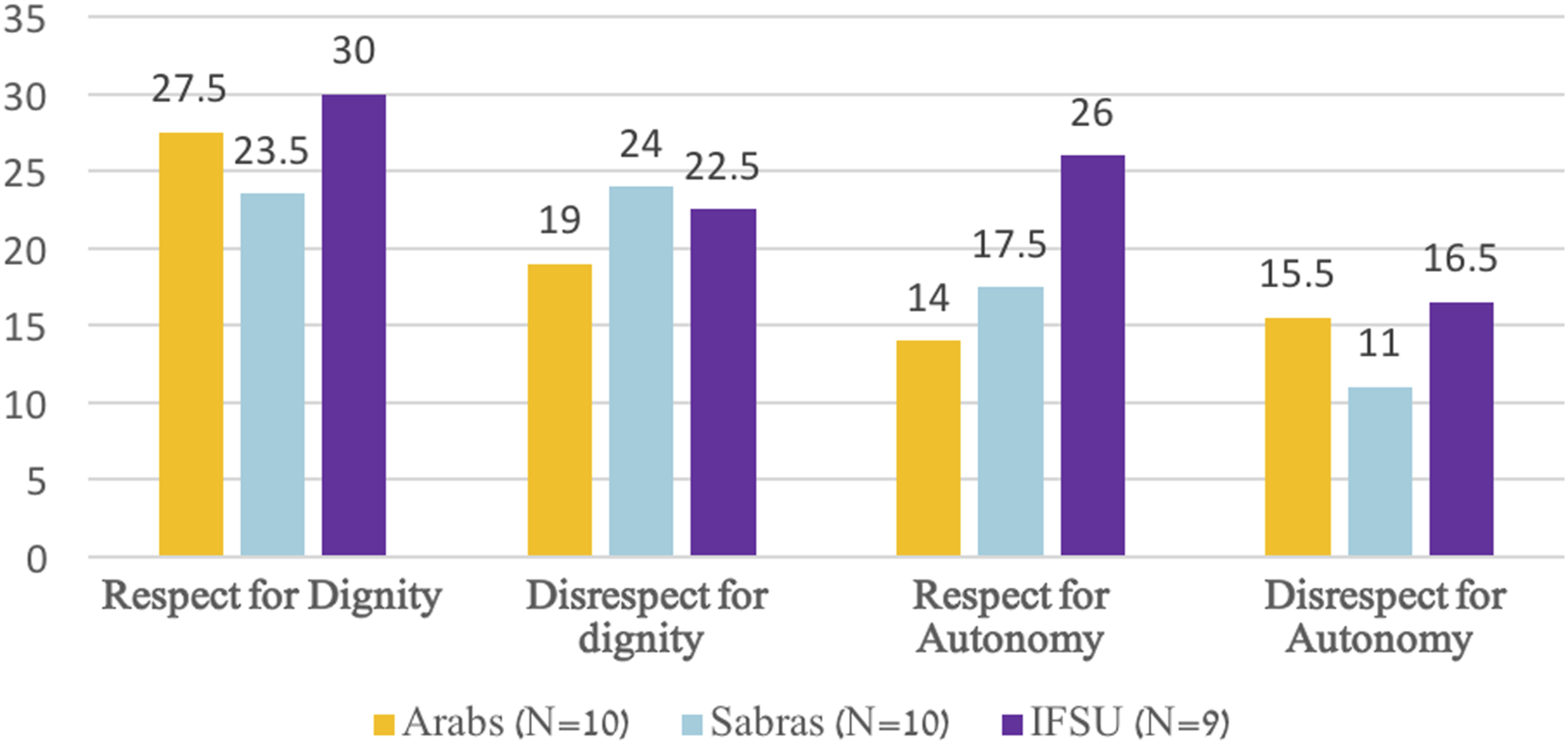
As can be seen in Table 4, the calculated average and median number of interaction instances per cultural group of caregivers were quite similar for each group and the focused category of analysis (e.g., respect for autonomy, disrespect for dignity). Still, in Figures 1 and 2 we opted to focus on the calculated medians in order to decrease the possible influence of outliers—namely, specific caregivers whose number of interaction instances of respect or disrespect for autonomy or dignity were extraordinary. Based on such an approach, and as Figure 1 demonstrates, there have been more instances of respect for both human dignity and autonomy among nine IFSU caregivers than the other two cultural groups of caregivers (i.e., 10 Sabras and 10 Arabs caregivers).
Whereas the median number of interaction instances of respect for autonomy and human dignity together was 57 for IFSU caregivers, the medians for their Sabra and Arab colleagues were merely 43.5 and 41, respectively. On the other hand, in terms of disrespect for human dignity and autonomy, the medians were quite similar among the different cultural groups, with 38, 39, and 37 median interaction instances of such disrespect occurring among IFSU, Sabra, and Arab caregivers, respectively.
The image for the possible differences among the three cultural groups of caregivers is further complicated when accounting for the median number of interaction instances of the varied facets of respect and disrespect for autonomy and dignity, separately, as shown in Figure 2. Thus, the main differences between the various cultural groups of caregivers appear to have revolved primarily around the facets pertaining to respect for autonomy. In this overall category, IFSU caregivers showed the highest median number of interaction instances that reflected facets of respect for autonomy; there was a gap of as many as 12 interaction instances between this group of caregivers and the cultural group of caregivers, which demonstrated the lowest median number of interactions related to the facets of respect for autonomy (i.e., Arabs). Yet, the IFSU caregivers also ranked the highest in the median of interaction instances that reflected disrespect for autonomy, although the number of such instances was lower (26 vs 16.5 for respect and disrespect for autonomy, respectively, among the IFSU caregivers).
Examples for facets of respect and disrespect for autonomy and human dignity.
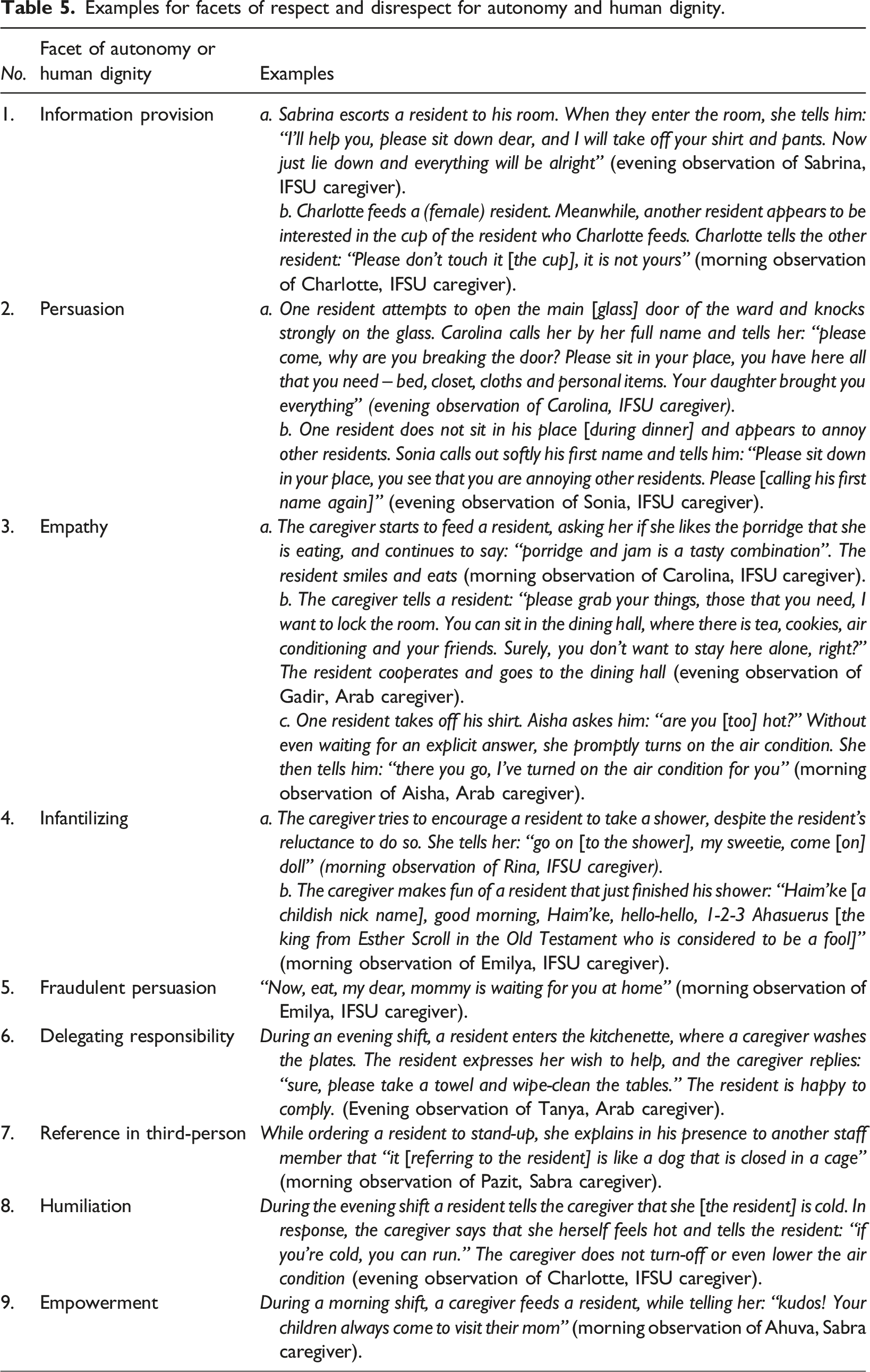
On the other hand, accenting the complexity of the collected data for three particular facets or components of disrespect for dignity, the IFSU caregivers were more dominant than the caregivers from other cultural groups: Verbal abuse (median of 1 among IFSU caregivers compared to 0 and 0.5 among their Sabra and Arab colleagues, respectively), infantilization (median of 3 among IFSU caregivers and 1 among their colleagues), and a lack of empathy as characterized by using dark and sarcastic humor, thereby scorning the patients (a median of 3.5 among IFSU caregivers compared to 3.5 and 3 among the Sabra and Arab colleagues, respectively). Some examples of these two components, as recorded in the observation log of the IFSU caregivers, are presented
The differences regarding respect and disrespect for human dignity were also relatively minor, although IFSU caregivers still led in this category as well (e.g., medians of 30, 27.5, and 23.5 for respect for human dignity among the IFSU, Arab, and Sabra caregivers, respectively). We stress this facet of the results, since it may serve as another indicator for the complexities in our results regarding the differences between the cultural groups of caregivers. Thus, one possible reason for the relatively minor differences between the IFSU and Arab caregivers in their respect for the dignity of older adults with dementia was empathy. Both of these groups of caregivers had a similar median of interaction instances per caregiver that specifically reflected empathy (6), as opposed to only 4 among the Sabra caregivers. In a similar vein, but from an opposite direction, infantilizing was a key component of disrespect for dignity that was manifested three times more often among IFSU caregivers than among the Arab and Sabra caregivers (median of 3 interaction instances per caregiver among the IFSU caregivers, compared to only 1 among their Arab and Sabra colleagues). Table 5 (Nos. 3–4) presents some examples from these observations, thereby demonstrating how these two components come into play in the observed interactions of the caregivers with the residents coping with Dementia.
New Components of Autonomy and Human Dignity or Lack Thereof
In addition to finding nuanced differences between the cultural groups of caregivers in terms of their respect and disrespect for autonomy and human dignity, the current study revealed new components of respect and disrespect for autonomy and dignity. As previously explained, when performing the microanalysis of the logged (written) observations, we employed two relevant models of autonomy and human dignity that included certain particular components or facets of these two concepts. However, in the process of conducting that analysis, we discovered 10 new components that were not included in the original models. Most of these new components related to disrespect for human dignity (6), although two components related to respect for autonomy (empowerment and delegation of responsibility) and 1 corresponded with disrespect for autonomy (commanding). Figure 3 presents a bar chart of the 10 new facets and the number of caregivers who demonstrated each of these facets during the observations. Red bars denote disrespect for either autonomy or dignity, while green bars signify respect for these values. In addition, Table 5 (Nos. 5–9) presents each of the new facets not previously shown thus far in the Results section by using excerpts from the reported observations. New themes of respect and disrespect to autonomy and dignity.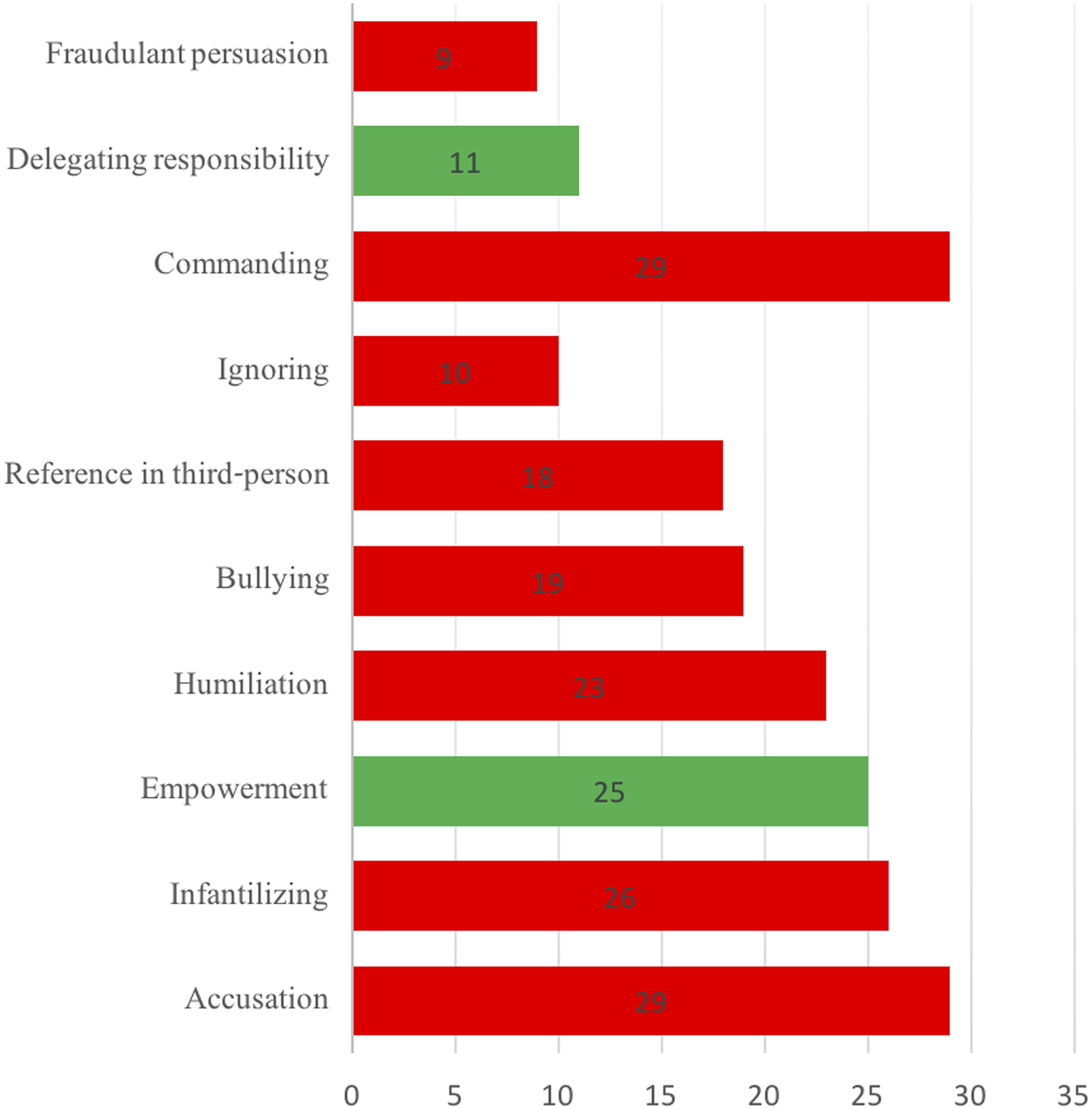
Discussion
Our study yielded three main and novel findings, especially when compared to the existing literature, which the current section discusses further. First, one cultural group of caregivers in our study—namely, IFSU caregivers—demonstrated more respect for autonomy and dignity. Second, the main difference between IFSU caregivers and the other groups of caregivers (i.e., Sabras and Arabs) pertained to the respect for autonomy; the main specific facets of autonomy in which IFSU caregivers surpassed their colleagues were information provision and persuasion. Finally, facets of disrespect for both autonomy and human dignity were discovered among all caregivers, but with more minor gaps between each.
Prominence of IFSU Caregivers in Respect for Autonomy and Human Dignity
In our study, IFSU caregivers demonstrated more interactions that expressed respect for autonomy and human dignity over the other two cultural groups of caregivers that were included in this study. These findings offer a stark contrast to previous studies on these groups of caregivers or some of them, which were based on caregivers’ perceptions rather than real-time observations of the daily care the caregivers provided. For example, one mixed-method study conducted by Bentwich and her colleagues on Arab, Sabra, and IFSU caregivers’ attending to older adults with dementia in Israeli nursing homes found that IFSU caregivers presented perceptions of autonomy and dignity with the least number of facets (or components) of these concepts (Bentwich, Dickman, et al., 2018a). Compared to IFSU and Sabra caregivers, Arab caregivers were found to prioritize the concept of dignity the most, regardless of the norms of the institutional setting (Bentwich et al., 2017).
Contrary to these findings, human dignity is recognized in the Islamic faith, but because of different cultural interpretations of that notion, its use and functions in geriatric health care are generally overlooked. Since older persons have complex healthcare demands, Islamic cultures and healthcare professionals often do not create support structures that can uphold autonomy and dignity (Atighetchi, 2007; Nasir & Abdul-Haq, 2008). The ethical principle of autonomy in Islamic countries has not yet been recognized as one of the main ethical principles of bioethics because the medical practice, in general, tends to be somewhat more authoritarian and paternalistic, without patients and their families playing essential role in determining the benefits and disadvantages of treatment, where and when such ethical dilemmas prevail (Brockopp & Eich, 2021).
Moreover, according to the WHO, family values are prioritized over respect for individual autonomy in many Islamic nations (WHO, 2008). Hence, in many Islamic countries - such as Egypt, Pakistan, and Turkey - the desires of elderly patients are frequently subordinated to the needs of their families and/or their social group. Additionally, older people with limited knowledge rely on doctors to make judgments in their best interests and worry that if they act differently, they will upset the doctors. These circumstances result in patients having less autonomy in comparison to patients in Western countries (Rashad et al., 2004).
Another earlier study performed by Rassin examined personal and professional values among IFSU and Sabra nurses and found that IFSU ranked values, such as integrity and trust between nurses and their patients the lowest, unlike their Sabra colleagues (Rassin, 2008). According to Rassin’s suggested interpretation, promotions in nursing staff in the former Soviet Union were mainly given based on their loyalty to the “system” rather than any initiatives designed to enhance the quality of humane and professional treatment of patients. Indeed, Iecovich and Rabin, who studied the self-reported practices of hospital nurses who were caring for older patients with dementia and other bedridden patients, found that Israeli nurses who had immigrated from the former Soviet Union reported using more physical restraints than other Israeli-born Jewish (Sabra) nurses (Iecovich & Rabin, 2014). Hence, IFSU nurses were less respectful of patients’ autonomy as they tended to use more physical restraints on their patients.
On the other hand, backing the findings in our study, Topaz and Doron studied nurses' attitudes toward older patients in acute care in Israel, as past studies have shown that nurses' affirmative attitudes positively do influence older patients' health. Nurses with positive attitudes toward the elderly translate these perceptions into practice by being able to listen attentively, bond deeply, assist respectfully, and engage in constructive relationships with their patients (Courtney et al., 2000; Jacelon, 2002). On the other hand, nurses with negative attitudes toward older people were more likely to use physical restrictions and disrespect the patients’ autonomy and dignity (Chien & Lee, 2007; Seedhouse & Gallagher, 2002). In Topaz and Doron’s study, one significant predictor of attitudes toward older people was the nurses' ethno-cultural background. In that study, 105 (62%) nurses were Jewish, and 65 (38%) were Arab. The Jewish nurses were primarily IFSU and of mostly Russian origin. They scored significantly higher than Arab nurses, meaning their attitudes were considerably more positive than those of Arab nurses. In light of these findings, Topaz and Doron call for further research to deepen the understanding of the influence of culture on nurses’ attitudes (Topaz & Doron, 2013)
Moreover, in an earlier study, eight focus groups were conducted with mostly family caregivers from eight racially and ethnically diverse groups, including Russians. The study aimed to examine cultural variations in caregiving experiences, care-related values and beliefs, care practices, and factors contributing to decisions about caregiver support services. The findings indicated that many of the Russian-speaking participants shared positive emotions about providing care, thus expressing happiness and joy, saying that they were thankful for the opportunity to help family members, which they considered a positive role in the Russian culture. Hence, in terms of their perception, caregiving was a source of fulfillment (Scharlach et al., 2006).
Notice, however, that both of these are attitudes-based rather than observational-based studies (Scharlach et al., 2006; Topaz & Doron, 2013) and were not conducted in the same context as our study. The first study focused on care for acute older patients in hospitals, rather than care for chronic patients with dementia in nursing homes, while the second study did focus on chronically ill patients, but the context was home-caregiving by family rather than formal caregivers. Therefore, while these previous studies do offer certain corroboration of our results, they were non-observational studies that were conducted in a similar context to our study. Hence the need for and importance of the current study, demonstrate a different perspective on the examined phenomenon through the use of field-observations instead of only interviews and questionnaires.
Moreover, most of the previous studies were not based on real-time observations of the daily care given to older adults with dementia in nursing homes. Rather, they were mainly informed by interviews or questionnaires filled out by the caregivers. In fact, and as noted in the Methodology section, the small number of studies that did involve real-time observations were either unsystematic in the manner in which the observations were recorded (Örulv & Nikku, 2007) or were based on a substantially fewer number of hours observed (Graneheim & Lundman, 2004; Jacobson, 2009). Moreover, none of these previous limited observation-based studies examined the possible differences between caregivers from various cultural backgrounds. Therefore, the current study highlights the need for more real-time observation-based studies when exploring autonomy and human dignity in the daily care of older adults with dementia, including any reference to the various cultural backgrounds of caregivers.
Possible Socio-Cultural Explanations for the Differences in Respect and Disrespect for Autonomy Between IFSU Caregivers and Others
The current study found that the more substantial differences between IFSU caregivers and their colleagues (especially their Arab counterparts) occurred in the median number of interaction instances that thus were reflecting respect for autonomy. One possible general explanation for this finding, as discussed in the literature, relates to the unique socio-cultural situation in which mainly the women who immigrated to Israel from the former Soviet Union in the 1990s found themselves. Many people (both men and women) who immigrated from the former Soviet Union, especially from large, modern, and highly industrialized urban areas (e.g., Russia, Ukraine), were highly educated individuals employed in white-collar professions (e.g., engineers, physicians, teachers). Their higher education, along with the larger cities in which they resided, exposed them to Western culture and values, including ideas like personal autonomy and individual rights. However, when they immigrated to Israel in such high numbers, the local professional market could not offer many of them jobs that suited their professional knowledge and expertise.
Women were particularly vulnerable in this situation, as their rates of unemployment were up to three times higher than those of the male immigrants. Consequently, these women had to make particularly tough compromises regarding their places of employment. Indeed, previous studies have estimated that IFSU constituted the majority of the caregivers workforce in Israeli nursing homes (Remennick et al., 2001; Ron, 2008). In other words, it is possible that—although many IFSU caregivers had to compromise regarding their line of work—they still did not abolish the Western values and culture they had absorbed before immigrating to Israel. Furthermore, our results, coupled with reasoning that stressed the influence of Western values on IFSU caregivers, demonstrated the importance of paying attention to nuances in socio-cultural background in a particular context. In contrast to the general assumption cited from the literature (in the Introduction here), according to which IFSU in Israel are often taken to be subscribing to non-Western values, this current study points in a quite different direction.
Meanwhile, the Arab caregivers (all of whom were women in our study) may have been raised in a cultural environment in which the autonomy of women might be more limited. Thus, according to the literature, traditional Muslim-Arab communities are mainly characterized as patriarchal, meaning they are controlled by men (Al-Krenawi & Graham, 2005). Although the Arab-Muslim society in Israel is considered to be moving closer to Westernization, the spirit of the more traditional perspective is still influential, including greater family control and the expectations of women to abide by the patriarchal culture (Barakat, 1985; Sa ‘ar, 2007). In such a society, women are still expected to obey the men in their lives as well as assume the traditional role as the family caregiver, even when they go out to work, in exchange for men’s protection (Erez & Berko, 2010). Therefore, it could be argued that, as female Arab caregivers might experience a more limited version of personal autonomy in their own families, they are less able to respect the autonomy of the older adults with dementia who are in their care.
Another explanation for the specific lead of IFSU caregivers with respect for the autonomy of older adults with dementia has to do with the particular facets or components of autonomy in which these caregivers excelled. These components are information provision and persuasion, both of which are related to lingual communication. Admittedly, there are no accurate statistics regarding the percentage of IFSU residents in Israeli nursing homes. However, studies have shown that IFSU who came to Israel during the 1990s have experienced a substantially higher percentage of physical and cognitive disabilities in older age compared to their Israeli-born Jewish counterparts (Bodovski & Benavot, 2006; Osman & Walsemann, 2013, 2017). Therefore, one may deduce that the proportion of IFSU residents in nursing homes should be higher than their relative proportion in the general population. Assuming this is the case, some studies have shown the importance of such common language between the patient (or resident) and their caregiver, known as linguistic congruity, for the welfare of that patient (Burant & Camp, 1996; Martin et al., 2019; Valle & Gait, 2014). In fact, one study conducted in Australian nursing homes that included staff members who also spoke Greek or Italian found that residents who were Greek and Italian by origin were given fewer prescriptions for anti-psychotic drugs than were residents of the same origins in nursing homes with no staff members who spoke these languages (Runci et al., 2012).
On the other hand, studies have shown that language concordance can also increase the chances for problems in provided care. Speaking the same language can create a fit between patients and practice, but it may also become problematic (e.g., because of increased demand and feeling pressured to communicate) (Lindenmeyer et al., 2016). Moreover, the concept of “cultural distance” may account for the fact that language is not a guarantee of mutual understanding and good spirits. Language alone doesn’t guarantee shared life values and social understanding. If people speak different languages, they are also ready for possible misunderstandings, hence they know beforehand that it is there and they must cope with it. However, people are often not aware of this issue when they speak the same language, a circumstance that has the negative potential to escalate otherwise ordinary situations into conflicts (Gómez Parra, 2009).
This explanation regarding the negative side of language concordance between caregivers and patients (or residents in our case) fits our results about the facets of disrespect for dignity that were more manifested among the IFSU caregivers. At least two of these facets (i.e., verbal abuse and infantilization) fully revolve around negative verbal communication, while the remaining facet (i.e., lack of empathy) is linked to such verbal communication to a certain extent (e.g., scorning).
Meanwhile, these facets of disrespect for dignity particularly concern verbal communication, and the latter sort of communication was already presented above as being linked to respect for autonomy, when referring to positive verbal communication (i.e., information provision, persuasion). Therefore, it could be argued that the latter types of positive verbal communication are contrasted and undermined by the facets of disrespect for dignity that concern negative verbal communication found more prominently among IFSU caregivers. As such, these negative facets of verbal communication may also underlie the relative prominence of disrespect for autonomy found among IFSU caregivers, just as the facets of positive communication were suggested above as underlying the prominence of IFSU caregivers in demonstrating more interaction instances that reflected respect for autonomy. Indeed, in their qualitative interview-based study, about similar cultural groups of caregivers that attend to residents with dementia in nursing homes in Israel, Bentwich and colleagues also drew attention to the linkage between facets of respect to autonomy and dignity. Specifically, they highlighted the overall respect for dignity as sometimes underlying respect for a particular facet of autonomy (i.e., privacy).
Facets of Disrespect for Both Autonomy and Human Dignity
Our study found components of disrespect for autonomy and human dignity, including facets of such disrespect that were not accounted for in the theoretical models that we used to analyze the observations. Neither of the pivotal models employed for the evaluation of autonomy and human dignity in the care for older adults in institutional settings included any components of disrespect for these values. These components were mainly established by us, in light of the actions taken by caregivers that we encountered during the observations, being the inverse of the original components and pertaining only to the respect for these values. In addition, in terms of autonomy, and as our findings regarding IFSU caregivers do show, being the most respectful cultural group of caregivers does not necessarily correspond with having the least number of instances that reflects disrespect for this value — indeed, it is quite the contrary.
Therefore, the current study highlights the complexity of disrespect for autonomy and dignity between different cultures and within them, thereby yet again stressing the need for a nuanced understanding of how cultures may influence the behavior of caregivers in their daily care of older adults with dementia. This complexity also emphasizes the need to extend the existing models of dignity and autonomy in the context of caring for older adults in institutional settings so that they also include the facets of disrespect. Such findings further echo previous researchers like Brooker and Ronch, who warned against disrespect for human dignity in nursing home contexts (Brooker & Latham, 2015; Ronch, 2004), and other more general studies that point to the low quality of care in such contexts (Mysyuk et al., 2015; White et al., 2008).
The finding of numerous aspects of disrespect for dignity and autonomy in this study also highlights the importance of applying the PCC approach as devised by Kitwood and others (Kitwood, 1997; Love & Kelly, 2011). This approach focuses the care provided to older adults on respecting their identity and dignity rather than on the disease and disabilities they might have. More recently, Brooker developed a variation of PCC that is specifically designed for people with dementia—namely, person-centered dementia care (PCDC)—which may assist in decreasing the interaction instances of caregivers’ showing disrespect for the dignity and autonomy of older adults with dementia in institutional settings (Brooker & Latham, 2015; Li et al., 2017).
Study Limitations
The current study’s inherent limitation is that it focused on three particular cultural groups in a single country, which constrained the number of participants, given the methodology used. Therefore, more studies in Israel, as well as other countries, are needed to explore whether and how the differences between cultural groups in our study also exist in other contexts. Another possible limitation is that the observations recorded in written journals were from a single author (FK); therefore, it could be argued that this method of recording is biased, especially given the fact that this author is a member of one of the examined cultural groups (i.e., IFSU), although he is not a caregiver but rather a social worker. To this issue, we respond that given the interpretive nature of any qualitative study (in our case, interpreting daily care interactions through the prism of facets of autonomy and human dignity), any such interpretation is considered inherently biased and based on the perspective of the researcher. Furthermore, as noted in the Methods section, we employed three main mechanisms to ensure the trustworthiness of this study.
Conclusions
This study is the first of its kind to focus on the real-time behaviors of caregivers from diverse ethno-cultural backgrounds, thereby shedding light on aspects related to respect and disrespect for the dignity and autonomy of patients with dementia in nursing homes. The study uncovered intriguing complexities in these behaviors and linked them to possible cultural underpinnings. The study also revealed new facets of respect and disrespect for autonomy and dignity that were previously unaccounted for. Through these findings, this study illuminates how culture may play an important role in caregivers’ behaviors toward older adults with dementia as well as enhancing the understanding of nuances in terms of the respect and disrespect for autonomy and dignity in this context.
On a practical level, our study may have important implications for caregivers’ training in multicultural societies at least in two respects: (1) It stresses the importance of paying attention to and addressing possible cultural underpinnings for actual behaviors of caregivers from different socio-cultural backgrounds so as to ensure respect for the autonomy and dignity of older adults with dementia. (2) It emphasizes the importance of paying attention to any nuances regarding the manner in which cultures may play a role in caregivers’ actual behavior and the need to refrain from a monolithic perspective of any given culture when designing such training in multicultural societies.
Footnotes
Acknowledgements
We are in debt to all of the participants in the study, hard-working caretakers in different nursing homes, who were willing to give us the unique and invaluable opportunity for “shadowing” them during their daily shifts. We also wish to express our gratitude to the two anonymous reviewers for their insightful comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study received the approval of the research ethics committee of the Faculty of Medicine at Bar-Ilan University (Approval #03-2017).