
Abstract
Background and objectives
Resilience – the ability to bounce back after a stressor - is a core component of successful family caregiving for people living with dementia. In this manuscript, we describe the preliminary empirical validation of a new behavioral framework developed from existing literature for assessing care partner resilience, CP-R, and propose its potential value for future research and clinical care.
Methods
We selected 27 dementia care partners who reported significant challenges prompted by a recent health crisis of their care recipient from three local university-affiliated hospitals in the United States. We conducted semi-structured interviews to elicit care partners’ accounts of what they did to address those challenges that helped them recover during and after the crisis. Interviews were transcribed verbatim and analyzed using abductive thematic analysis.
Findings
When persons with dementia experienced health crises, care partners described various challenges in managing new and often complex health and care needs, navigating informal and formal care systems, balancing care responsibilities with other needs, and managing difficult emotions. We identified five resilience-related behavioral domains, including problem-response (problem-solving, -distancing, -accepting, and -observing), help-related (help-seeking, -receiving, and -disengaging), self-growth (self-care activities, spiritual-related activities, and developing and maintaining meaningful relationships), compassion-related (self-sacrifice and relational compassion behaviors), and learning-related (learning from others and reflecting).
Discussions and implications
Findings support and expand the multidimensional CP-R behavior framework for understanding dementia care partner resilience. CP-R could guide the systematic measurement of dementia care partners’ resilience-related behaviors, support individual tailoring of behavioral care plans, and inform the development of resilience-enhancing interventions.
Approximately 55 million persons live with dementia worldwide, which is expected to increase to around 140 million by 2050 (World Health Organization, 2021). The progressive dependency that results from dementia establishes a compelling need for continued research on how best to support care partners (mainly family members and friends) through the course of the disease (Bremer et al., 2015). Care partners often devote extensive efforts to supporting persons with dementia, including assistance with activities of daily living, care coordination, and management, addressing problems related to cognitive impairment, managing co-occurring chronic diseases, responding to changes in behavior and mood, and facilitating social engagement for individuals no longer able to do so (Sadak et al., 2015).
Many studies have found that dementia caregiving is associated with unique stressors that can give rise to physical and mental health consequences, such as depression (Teahan et al., 2018), burnout (Alves et al., 2019), poor quality of life (Srivastava et al., 2016), and cognitive problems (Allen et al., 2017). Despite these difficulties, many care partners derive high satisfaction, meaning, and purpose (Shim et al., 2013) from caregiving activities, experience heightened intimacy and connection with persons with dementia, acquire new skills, adapt successfully to changes, and maintain a stable quality of life during the caregiving journey (Nguyen, 2022). These positive outcomes of caregiving reveal the presence of resilience in dementia care partners and justify the need to continue studying behaviors that promote it.
Resilience, broadly defined as the capacity for bearing, recovering, or growing from challenging experiences, is a critical factor that buffers the adverse consequences of caregiving stress and can facilitate growth in dementia care partners (Teahan et al., 2018). Care partner resilience may be a protective factor against depression and caregiver burden, and can facilitate better physical health and quality of life (Zhou et al., 2021). This highlights the importance of improving care partners' resilience, particularly in crises and stress, as a target for interventions.
Despite the growing awareness of the importance of enhancing resilience in dementia care partners, relatively few resilience-based interventions target this group (Gitlin et al., 2020). Barriers to developing relevant interventions include a limited understanding of care partners’ resilience in the context of the unique dementia-related challenges, and the lack of clear, observable indicators of the resilience process that can be used as outcome measures (Gitlin et al., 2020; Zhou et al., 2021). These barriers hinder the exploration of behavioral mechanisms of change associated with dementia care partners’ resilience. A better understanding of the behavioral mechanisms of change can help researchers and practitioners to select impactful treatment targets and intervention components (Onken et al., 2014); it can also help explain how and why certain interventions work and result in more consistent efficacy and effectiveness than others (Gaugler et al., 2021).
A previous systematic literature review used a thematic analysis approach to summarize qualitative and quantitative descriptions of resilience-related behaviors among dementia care partners, informing the development of a behavioral framework for dementia Care Partner Resilience (CP-R). The original CP-R framework consists of four intersecting domains, and each domain includes several behaviors: (a) problem response (problem-solving, problem-distancing); (b) self-growth (self-care activities, spiritual-related activities, and developing and maintaining meaningful social relationships); (c) help-related (help-seeking and help-receiving); and (d) learning-related (learning from others and reflection) (Zhou et al., 2022). Care partners often engage in behaviors from different domains simultaneously. However, not all relevant behaviors may have been identified because none of the reviewed studies systematically examined dementia care partners’ resilience in the context of specific challenges. Health crisis of persons with dementia is one of the common and significant challenges experienced by most care partners (Hopkinson et al., 2021). During the health crisis, care partners often experience cumulative and elevated care burdens due to care recipients’ declining health and functions before reaching the point of crisis (Afonso-Argilés et al., 2020; Shepherd et al., 2019). In addition, as care partner resilience is about the capacity to bear, recover, and grow from challenges, an acute health crisis is a discrete event that offers a unique opportunity to observe resilience behaviors and processes that promote care partner recovery from a challenging situation over a relatively short timeframe. Its acuity marks the event with heightened recall and the ability to report what happened and how the care partner responded. This study aims to validate and expand the CP-R framework by identifying (1) care partners’ challenging experiences during health crises of persons with dementia and (2) behaviors they engaged in response to these challenges.
Methods
Study design
This study was one component of a parent study that utilized semi-structured interviews, survey measures, and Electronic Medical Record (EMR) reviews that examined care partners’ experiences when persons with dementia had a health crisis resulting in an unplanned acute care encounter (hospitalization, emergency room [ER] visit, or observation status) (Sadak et al., 2019). We selected a sub-sample of dementia care partners and conducted a qualitative study, using semi-structured interviews to examine care partners’ resilience-related behaviors adopted during crises. Interview data were analyzed using an abductive thematic approach to allow us to “move back and forth between observation and theoretical generalizations” (Tavory & Timmermans, 2014) to attain surprising observations and formulate more promising hypotheses (Timmermans & Tavory, 2022). We conducted the study and reported results following the Consolidated Criteria for Reporting Qualitative Studies (COREQ) (A. Tong et al., 2007).
Participants
Eligible participants were care partners of persons with dementia who lived at home before an unplanned acute care encounter for a medical problem (hereinafter referred to as “index acute care encounter”). The investigators, in collaboration with information technology staff of three local university-affiliated hospitals, developed an EMR algorithm to identify older adults (age 65+) with an ICD-9 or ICD-10 diagnosis code for any dementia (World Health Organization, 1993) who: (1) were discharged in the previous 7 days after an index acute care encounter; (2) had two or more additional chronic conditions; and (3) had an identifiable next of kin. The research coordinator (E. I.) contacted 446 “next of kin” for screening. Identified individuals were eligible to participate if they were 18 years and older, read and spoke English, self-identified as a care partner (e.g., they schedule and accompany the patient to medical appointments), their care recipients living at home before the index acute care encounter, and were able to verify that the patient had cognitive impairment based on a score of 2+ on the caregiver-rated AD-8 dementia screening tool (Galvin et al., 2005). Through pre-screening, we found that not only family members but also friends could be listed as next of kin in the EMR system. A total of 100 care partners were deemed eligible and gave informed consent to complete parent study measures and 60–90-min in-home interviews with a master’s prepared social worker. Using convenience sampling, we pre-screened 28 care partners at the time of enrollment in the parent study, asking about challenges they experienced in connection with health crises of persons with dementia: “For the health crisis leading to your loved one’s emergency room visit or hospital care, what situations did you find most difficult/challenging/stressful to deal with?” Of these pre-screened care partners, 27 screened participants reported challenging experiences and participated in an additional resilience interview that formed the basis for this report. Ethical approval was granted on 11/6/2017 by the Institutional Review Board at the University of Washington.
Data collection
We conducted semi-structured interviews (Supplementary File 1) to elicit information about behaviors care partners adopted to address challenges during health crises of persons with dementia, and that they believed helped them adapt and recover (positive resilience outcomes). Resilience outcomes for dementia caregiving include outcomes related to adversity (i.e., care partners’ and persons with dementia’s health and quality of life after the crisis) and care partners’ reports of personal growth (Zhou et al., 2021). The research team reviewed and approved the data collection protocol after two pilot interviews.
Data analysis
Interviews were de-identified, transcribed verbatim, and analyzed using an abductive thematic analysis approach (Tavory & Timmermans, 2014). We used the abductive approach, rather than deductive or inductive approaches, as we aimed to intentionally challenge and expand a pre-existing framework (Tavory & Timmermans, 2014); the thematic analysis method was chosen as it allows for a transparent and systematic synthesis of empirical evidence into categories and themes (Vaismoradi et al., 2013). The five-step process of an abductive thematic analysis (Tomasella, 2022) includes:
Step 1: Open coding
Without trying to fit the data into the pre-existing behavioral framework of dementia care partners’ resilience (Zhou et al., 2022), two coders (Y.Z. and D. H.) first conducted open data coding of 10 participants’ interview data, including all the interview data from resilience interviews and other parent study data relevant to care partners’ resilience. For abductive analysis, open coding is not atheoretical but uses preexisting knowledge and theoretical maps to “open our coding” (Timmermans & Tavory, 2022). To initiate exploration of “what do challenges mean to care partners?,” two coders identified any situations that care partners found difficult/challenging/stressful to navigate during persons with dementia’s health crisis as “challenges.” To explore what “behaviors that indicate resilience processes to care partners,” two coders sought to identify specific behaviors care partners adopted to address challenges and behaviors care partners themselves associated with resilience outcomes.
Step 2: Develop an abductive codebook of challenges and resilience-relevant behaviors
After the open coding phase, we developed the first draft of an abductive codebook of themes pertinent to challenges and resilience-related behaviors based on previous literature. As there was no existing framework for care partners’ challenges during persons with dementia’s health crises, we based our review on known care partner stressors associated with persons with dementia’s crises (MacNeil Vroomen et al., 2013): (1) lack of knowledge; (2) communication challenges with healthcare providers; (3) emotional challenges; (4) heavy care responsibilities; (5) lack of time for personal or social activities due to increased caregiving; and (6) challenges in care transitions. Definitions of each health crisis-related stressor for care partners are given in Supplementary File 2. Resilience-related behaviors include four themes and nine sub-themes: (1) problem–response behaviors (problem-solving, problem-distancing); (2) self-growth behaviors (self-care activities, spiritual-related activities, and developing and maintaining meaningful social relationships); (3) help-related behaviors (help-seeking and help-receiving); and (4) learning-related behaviors (learning from others and reflection) (Zhou et al., 2022). Definitions of each theme and sub-theme are presented in Supplementary File 3.
Step 3: Update the codebook using open-coding results
We compared open coding results and the codebook in research team discussions. While many initial codes were collated into the first draft of the codebook, new codes, such as “challenges due to the ER/hospitalization conditions and service provision,” “being present,” “normalizing persons with dementia’s negative attitudes,” and “checking and keeping records of persons with dementia’s symptoms (blood sugar and pressure, etc.),” and “asking other family members not to call” were recorded to retain the potential for generating new themes and sub-themes.
Step 4: Use the updated codebook to inform the coding process
Two coders reviewed the rest of the 17 cases with the updated codebook in mind. We emphasized openness to identifying new codes for challenges and resilience-related behaviors. During this process, weekly meetings between two coders were conducted to discuss any new codes and the potential to form new themes. We developed an updated codebook with new themes through the interactive analysis process. We found no new themes in the last five cases, indicating saturation.
Step 5: Generate a thematic map
After completing the first round of coding for all interviews, we reviewed relevant literature to refine the names and definitions of all the themes and sub-themes. A thematic map was drafted and revised, with minor changes, after group discussions with all authors. Using the updated thematic map, two coders reviewed all interviews again to count the number of participants who reported each challenge and resilience-related behavior and ensure that no other themes were identified. We incorporated additional feedback from peer reviewers when finalizing the thematic map. Throughout the process of analysis, we maintained an audit trail of raw data (recording, transcripts) and analytic materials (Rodgers & Cowles, 1993).
Findings
Characteristics of participants and acute health crises
Characteristics of persons with dementia and their care partners.
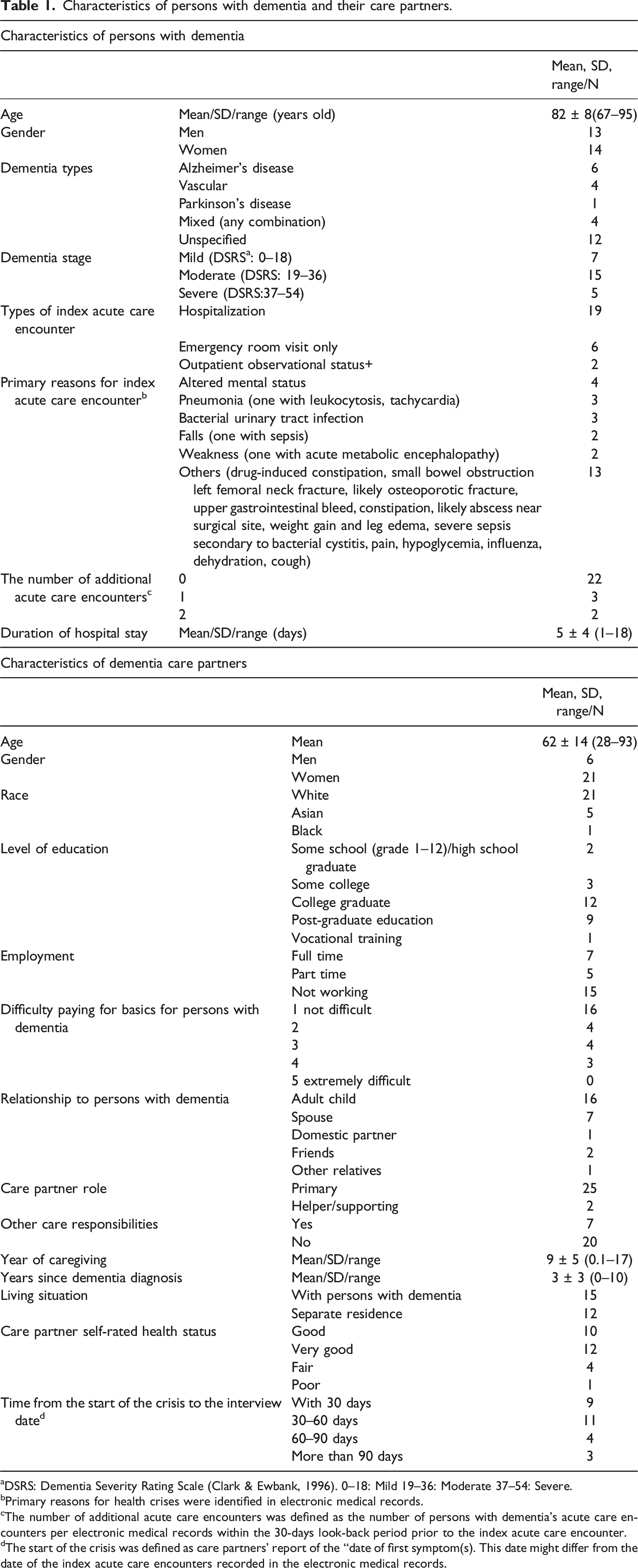
aDSRS: Dementia Severity Rating Scale (Clark & Ewbank, 1996). 0–18: Mild 19–36: Moderate 37–54: Severe.
bPrimary reasons for health crises were identified in electronic medical records.
cThe number of additional acute care encounters was defined as the number of persons with dementia’s acute care encounters per electronic medical records within the 30-days look-back period prior to the index acute care encounter.
dThe start of the crisis was defined as care partners’ report of the “date of first symptom(s). This date might differ from the date of the index acute care encounters recorded in the electronic medical records.
Challenges reported by care partners during the health crisis of persons with dementia
Challenges care partners experienced during persons with dementia’s health crisis.
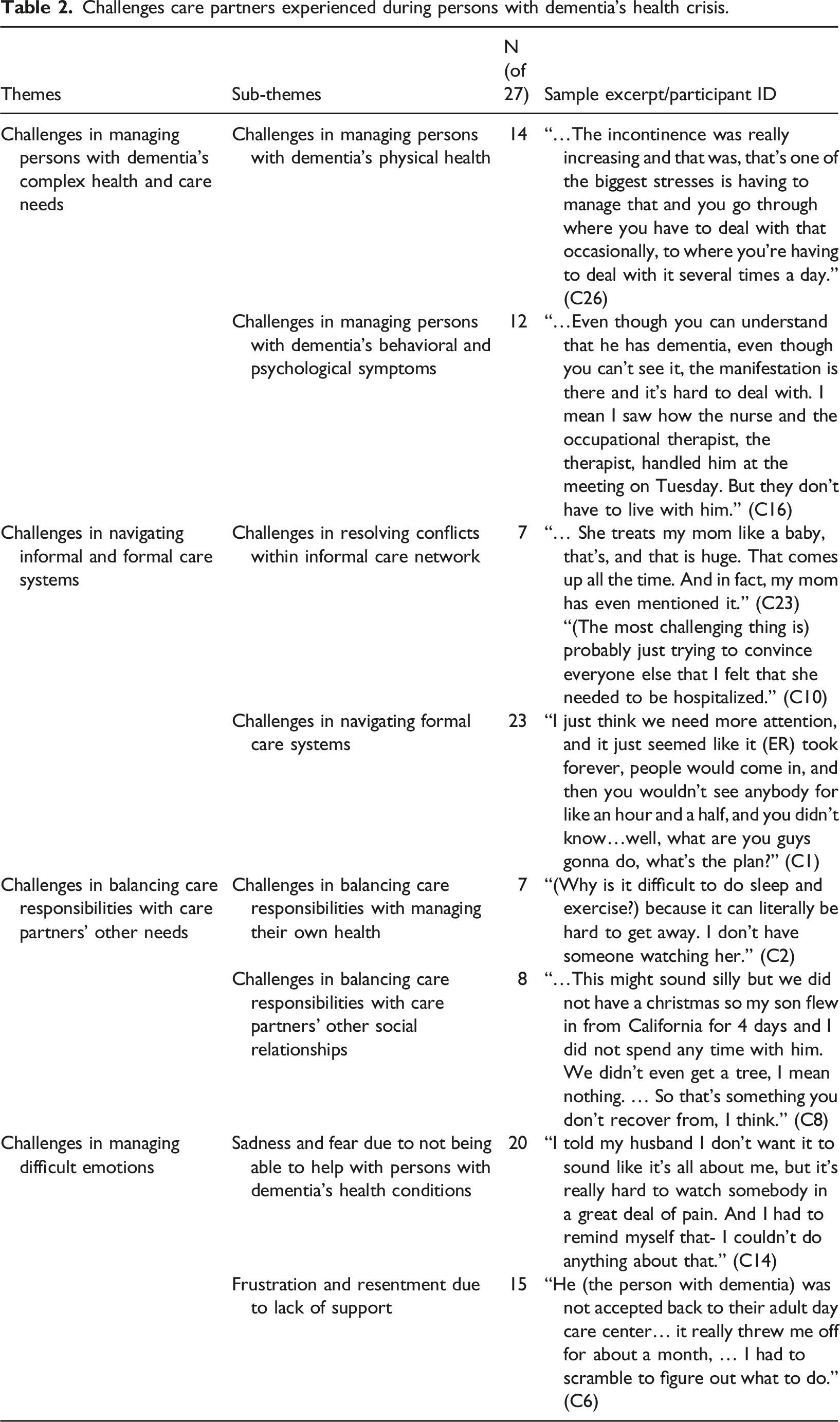
Challenges in managing persons with dementia’s complex health and care needs
Care partners reported challenges in managing persons with dementia’s complex health and care needs, specifically managing their deteriorating physical health (such as falls, mobility impairment, urinary tract infection (UTI), fluid and food intake, incontinence, constipation, and pain, n = 14) and exacerbated behavioral and psychological symptoms during the crises (such as emerging paranoia or aggression, n = 12). Several care partners reported worries about persons with dementia’s falls and having trouble lifting them or assisting them with mobility. Persons with dementia’s physical disability, such as aphasia and hearing impairment, pose unique challenges for care partners. One care partner shared that “(After the person with dementia fell), we were worried that maybe he’d broken something because he seemed to indicate that he was in pain, but it’s hard to tell because he can’t explain it. ” (C26)
Care partners also found that persons with dementia’s behavioral and psychological symptoms often resulted in resistance to care, which limited their ability to delegate care responsibilities to others. One care partner shared that although she was able to identify a paid caregiver who was a retired nurse; however, when the caregiver came over, “my husband was so hostile, kicked her out and told her to leave. I lost her too.” (C17)
Challenges in navigating informal and formal care systems
Persons with dementia’s complex care needs necessitated care partners to navigate informal care networks (n = 7) and formal care systems (n = 23). Care partners often encountered difficulties and conflicts when engaging with these care systems. For some care partners, the main sources of stress during the health crisis were the conflicts within the informal care network. These conflicts often resulted from the unfair distribution of care responsibilities, disagreement on care arrangements, and expectations from other care partners. One care partner shared that as the primary care partner, other family members expected her to keep them updated during the health crises: “I know that everybody’s well-intended and that people want to help, and I’m very grateful for the wonderful support network I have. But when I’m very stressed, I get very overwhelmed when I get lots of text messages or emails from people.” (C9)
Persons with dementia’s health crises also required care partners to interact with different parts of formal care systems. The main challenges included conflicts with healthcare providers, lack of access to services, tolerating unpleasant environments in healthcare settings, and navigating care transition. The conflicts with health care providers included disagreements on discharge plans, re-hospitalization, and medical procedures performed. Some care partners had difficulty accessing health care services due to the distance between home and hospital, bad timing (e.g., Christmas and Thanksgiving), and delays due to clinicians’ busy schedules. Long wait times and unpleasant environments (e.g., no place to sleep, hard to get water, no place for care partners to take a break, no spiritual-related services available for care partners) were especially difficult. Care partners reported difficulties related to care transitions during and after the health crisis, including navigating the logistics of care systems, such as transitioning persons with dementia between hospitals and other care settings, identifying home- and community-based dementia care services, and compensating for the lack of communication and coordination between care settings.
Challenges in balancing caring responsibilities with care partners’ other needs
Because of the intensive care responsibilities during persons with dementia’s health crises, many care partners reported challenges in balancing care responsibilities with other personal needs, such as their own health and well-being (n = 7) or maintaining other social relationships (n = 8). Care partners found it challenging to manage their own health: they reported difficulties getting good sleep, maintaining physical exercise, having access to healthy food, or having a moment to be alone during the crisis.
Care partners also felt a sense of loss as they could not maintain other important social relationships because of their care responsibilities, such as spending time with their friends and children. For some care partners who had other care responsibilities, they strived to manage different care responsibilities during crises: “It’s more difficult now because I’m helping some other people too. I have two little ladies that I help. I feel like sometimes they resent that I’m not there as much for them as I am for my sister (the person with dementia)” (C12).
Challenges in managing difficult emotions
All the challenges related to caregiving mentioned above resulted in various difficult emotions. Two types of emotions were the most common: sadness and fear due to persons with dementia’s health conditions (n = 20) and frustration and resentment due to lack of support from others (n = 15). Most care partners reported sadness, shock, traumatization, worry, and fear due to witnessing persons with dementia’s suffering and uncertainty about the outcome and its implications for them as care partners. One care partner explained the most stressful part for her during the crises was the unpredictability: “Your stress gets high because you don’t know at any moment what you’re gonna get.” (C2)
Another common care-related emotional difficulty was the frustration with the lack of support. One care partner shared:” “I think my biggest frustration sometimes is no follow-up. Like the social worker is someone who could be providing [some follow-up]. You get dumped on, and then you go to the next place. No one is saying, I am here, I want you to call me, I’m gonna check on you, see if this happened, what you need next, what isn’t working, do I need another referral. I mean, it falls all on you to do it all.” (C11). Some care partners feel frustrated that no one else can share this care responsibility with them: “Sometimes I do wish there was another person. Unfortunately, I’m the only child, I’m the only person left in her family. So, I get to do it all.” (C21)”
Resilience-related behaviors
Resilience related behaviors.
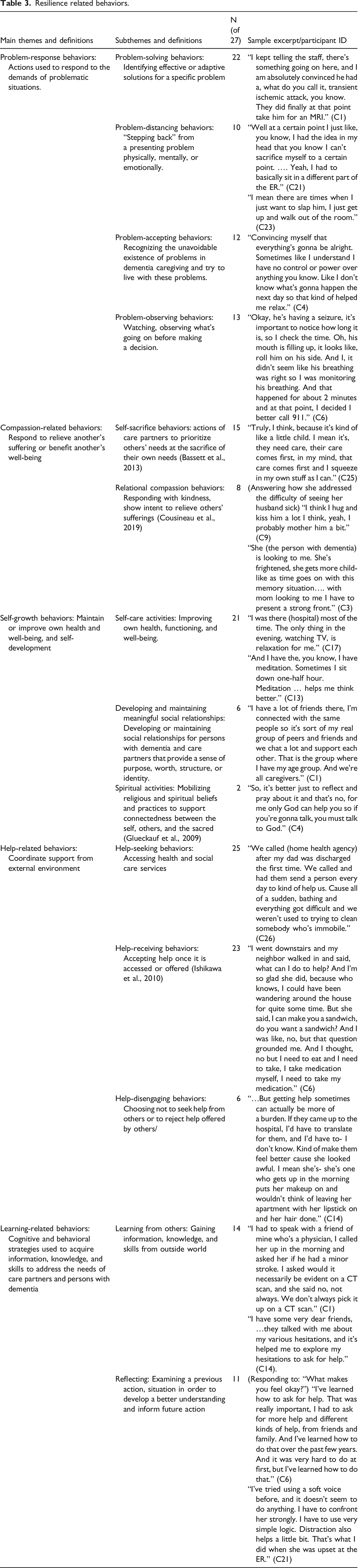
Problem-response behaviors
We have identified four types of problem-response behaviors from the interviews with the 27 dementia care partners, including problem-solving (n = 22), problem-distancing (n = 10), problem-accepting (n = 12), and problem-observing (n = 13).
Problem-solving behaviors were those used to develop effective, creative, or adaptive practical solutions for a specific problem. Examples included making arrangements to help persons with dementia adjust to a new setting in post-acute care, advocating for their own and persons with dementia’s needs, and finding creative ways to convince persons with dementia to receive medical attention. Problem-distancing behaviors included withdrawing from a presenting problem physically, mentally, or emotionally. Those behaviors included disengaging from conflicts with persons with dementia, the medical team, and family members involved in caregiving, avoiding situations that might be overwhelming, and emotional numbing such as sleeping and using alcohol.
In addition to problem-solving and problem-distancing behaviors, we identified two new responses: problem-accepting and problem-observing. We defined problem-accepting behaviors as recognizing the unavoidable existence of problems in dementia caregiving and trying to be non-judgmental and less reactive to problematic situations (Losada et al., 2015). Examples included accepting the uncertainties and the limitations of caregiving, perceiving the distress and challenges of crises as a normal part of the process, and normalizing persons with dementia’s attitudes and increased dependence. For example, when asked how they dealt with the uncertainty in caregiving, one care partner shared: “I’ve always been one to say don’t sweat the small stuff, you know it’s I just don’t stress about things that I can’t change. I mean, it is what it is.” (C10)
Problem-observing behaviors involve watching to see how the situation is evolving before making a decision about what to do. These behaviors included care partners monitoring their stress levels and care recipients’ symptoms before taking actions and preparing for further deterioration. One care partner described how they monitored their stress level to prevent personal emotional crises: “Initially, I can get very overwhelmed by something. I think over time I’ve sort of learned to use that as a cue to say, okay stop.” (C1)
Compassion-related behaviors
Compassion-related behaviors, those meant to relieve others’ suffering or benefit others’ well-being, included self-sacrifice (n = 15) and relational-compassion behaviors (n = 8). Understanding compassionate behavior as part of resilience emerged unexpectedly from our analysis.
Self-sacrifice behaviors were actions of care partners to prioritize others’ needs at the expense of their own needs (Bassett et al., 2013), such as reducing self-care and social activities, or quitting a job to be more present and provide better care for the person with dementia. One care partner explained how self-sacrifice was essential during the crisis: “…for this period of time, this (taking care of the person with dementia) is what I’m gonna do. I am not gonna be busy with friends, this or that… I don’t think of (this) as a negative thing. I can see the light at the end of the tunnel.” (C14)
Relational compassion behaviors were those used to respond with kindness and desire to relieve others’ suffering (Cousineau et al., 2019). Examples include expressing compassion through hugs and kisses, perceiving caregiving as a way of showing love, empathizing with persons with dementia and focusing on their needs, preserving their dignity, and calming their minds and emotions. One care partner explained that the way she empathized with the person with dementia also helped her to address difficult emotions: “To be dependent on me is a blessing and a curse for him. And I have to keep reminding myself what it’s like for him to be who he is with regard to me. And it isn’t just about me; it’s also about him. And that, sometimes, helps me to feel better.” (C23)
Some care partners shared how they felt responsible for relieving persons with dementia’s suffering while caring for other family/friends’ difficult emotions in the face of the crisis: “I have to be the stronger one as some (family members) don’t know how to handle their emotions. I just keep the feelings to myself and try to convince everybody everything’s gonna be all right. … I feel better, seeing them (other family members) okay.” (C4)
Self-growth behaviors
Self-growth behaviors are those used by care partners “to maintain or improve their health, well-being, and/or cultivate a better self through connecting with others” (Zhou et al., 2022). Self-growth behaviors include self-care behaviors (n = 21), developing and maintaining meaningful social relationships (n = 6), and spiritual activities (n = 2). In this sample, self-care behaviors were used more often than other self-growth behaviors in response to care recipients’ health crises.
Self-care behaviors are actions care partners use to maintain and improve their health, functioning, and well-being, such as eating well and getting enough sleep to keep up their energy, staying hydrated, spending time for hobbies, engaging in mindfulness and breathing practices, outdoor activities, and handing care responsibilities over to other family members. Developing or maintaining meaningful social relationships that provide a sense of purpose, worth, structure, or identity for both persons with dementia and care partners included connecting with support groups and socializing with and being supported by family and friends. Spiritual-related activities were defined as mobilizing religious and spiritual beliefs and practices to experience connectedness between oneself, others, and the sacred (Glueckauf et al., 2009). Care partners spoke of meditation, prayer, talking to God, and making meaning through religious interpretations of life challenges.
Help-related behaviors
Help-related behaviors – coordinating support from the external environment – were among the most commonly described, including help-seeking (n = 25) and help-receiving (n = 23). A few care partners described disengaging from help (n = 6) in some circumstances.
Help-seeking behaviors are those care partners used to access health and social services and care support. Examples included seeking guidance, information, and assistance from medical providers, asking family members and friends to step in decision-making and care responsibilities, seeking help for logistics; and searching for paid caregivers. Help-receiving was accepting the help and support that are available or offered by others, such as receiving support offered by family, friends, paid caregivers, support groups, mental health providers, and medical providers to manage persons with dementia’s symptoms, share care responsibilities, navigate the logistics of care, and address caregivers’ emotional needs.
Besides these two commonly adopted health-related behaviors, we identified a third subcategory of help-related behaviors: help-disengaging – making a deliberate choice not to seek help from the external environment or reject help others offer. This occurred when ‘getting help’ required even more effort than going it alone: examples include not allowing others to be present in the hospital and disengaging with families and friends who were not helpful. One care partner explained why disengaging support from families was helpful: “Getting help sometimes can be more of a burden…. If they came up to the hospital, I’d have to translate for them, and I’d have to, I don’t know, kind of, make them feel better because mom (the person with dementia) looked awful.” (C14)
Learning-related behaviors
Learning-related behaviors, including learning from others (n = 14) and reflecting (n = 11), are cognitive and behavioral strategies used to acquire information, knowledge, and skills to address the needs of care partners and persons with dementia.
Learning from others included strategies employed to gain information, knowledge, and skills from the outside world. These behaviors include consulting with friends and family, researching, getting information from doctors about the nature and progress of the health problem, and learning from others who have been through similar experiences. Reflecting involves examining a previous action and situation to form a better understanding of a current situation and inform future circumstances (Zhou et al., 2022), such as using previous life experiences to navigate the healthcare systems, be assertive, and ask for more help, and to choose communication techniques.
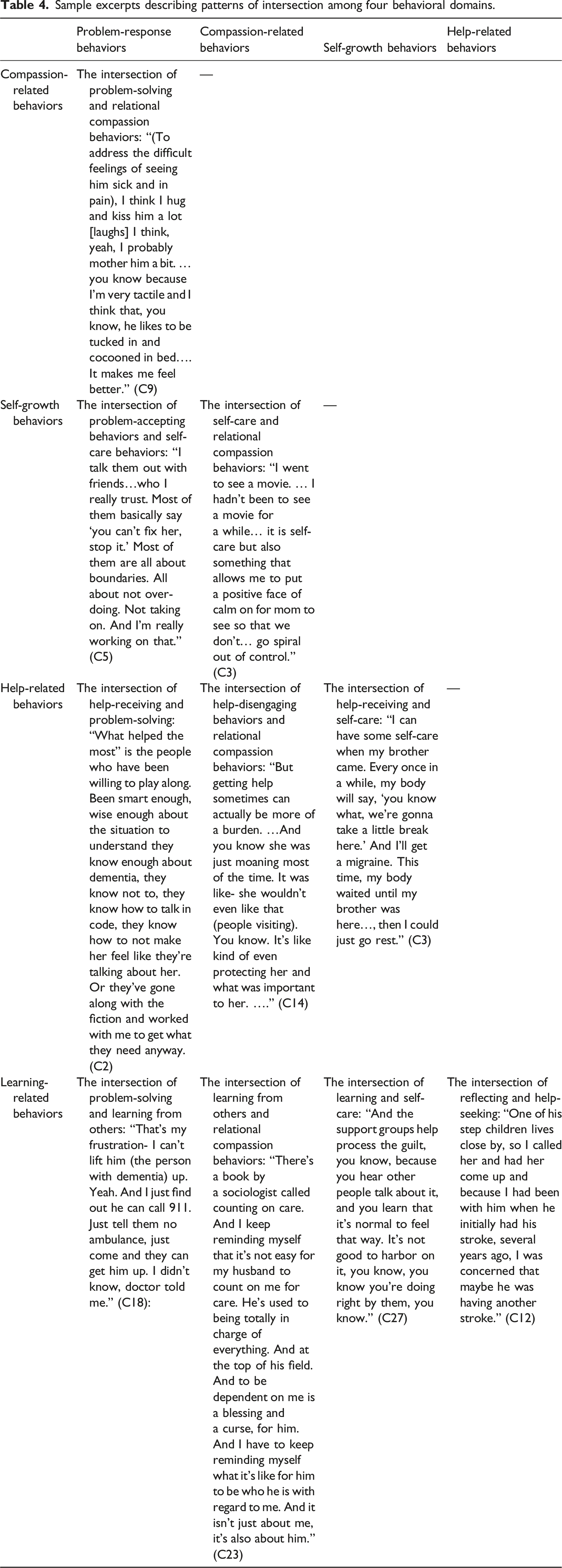
Intersections between the four domains of resilience behavior
Sample excerpts describing patterns of intersection among four behavioral domains.
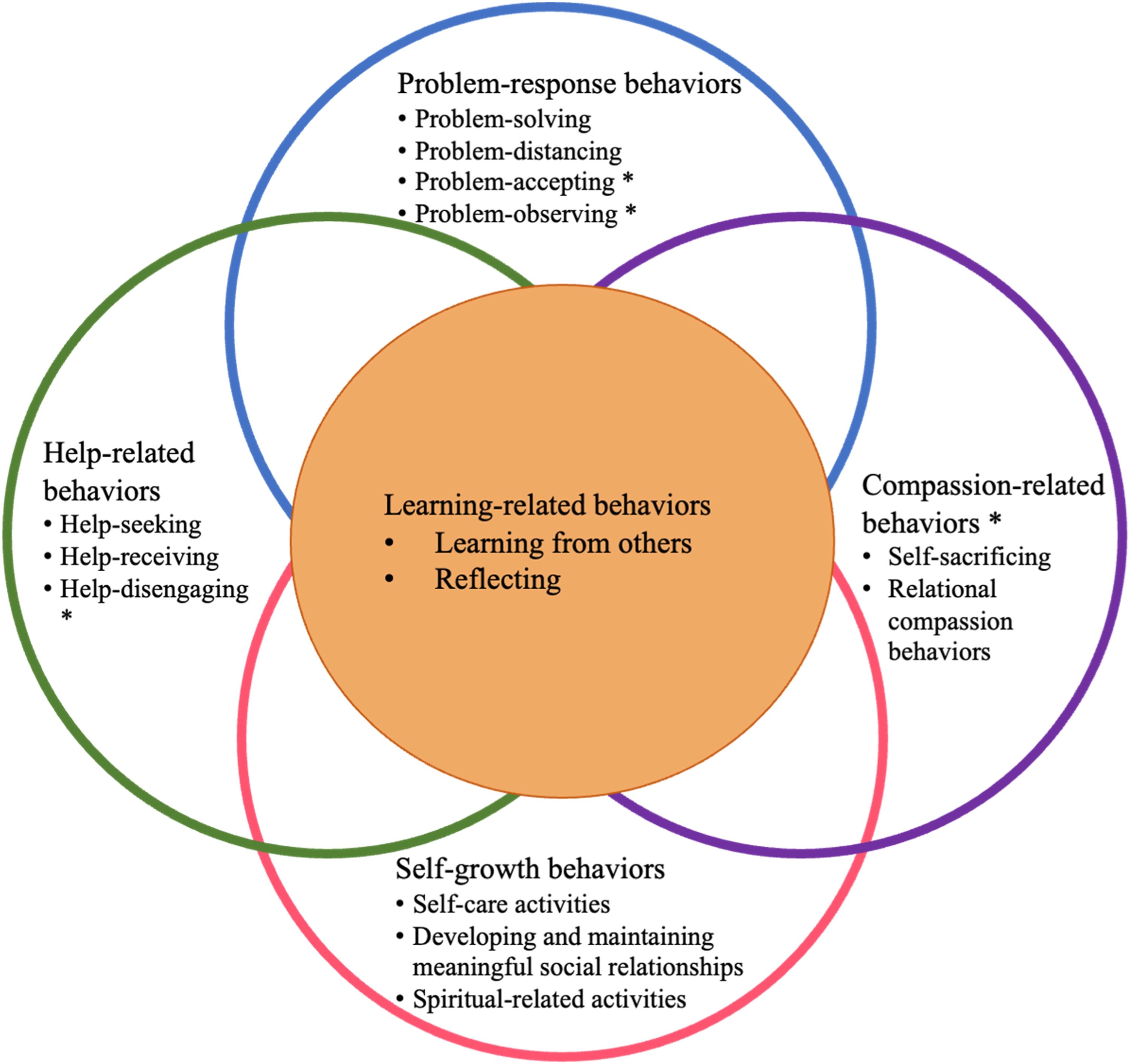
A Behavioral Framework for Dementia Care Partner Resilience CP-R framework. Note: * indicates newly identified resilience-related behaviors.
Case examples
The following cases provide examples of care partners utilizing different resilience-related behaviors to overcome challenges during persons with dementia’s health crises. We marked core resilience-related behaviors from the CP-R framework in the cases.
Case 1
Jason, a 28-year-old Black man, had been caring for his father, Chris, age 80, for 4 years. Although Chris had been diagnosed with vascular dementia (severe, Dementia Severity Rating Scale [DSRS] score = 39), Jason had never been told that his father had been diagnosed with dementia, but had seen his father behave in uncharacteristic ways (yelling, swearing, and refusing to answer providers’ questions) during a trip to the emergency department for acute illness. Chris was diagnosed with a urinary tract infection and discharged home. The main challenge Jason experienced was navigating the healthcare system (accessing services from a distance and communicating with healthcare providers about how to care for his dad) and managing his sadness and fear because of his dad’s sudden and continuing deterioration.
Jason described how he put his dad’s care over everything else (self-sacrifice). He had tried to manage his responsibilities alone, to “be strong” for his family by not showing sadness and fear (help-disengaging), so other family members wouldn’t feel too sad and worried (relational compassion behaviors). He tried to solve some of these problems by looking for a closer service provider (problem-solving), asking for help (help-seeking), learning from healthcare providers about how to prevent UTI (learning from others), and monitoring the symptoms closely (problem-observing). He reflected on how his dad had taught him how to face death and uncertainty (reflecting), so he could learn to accept the uncertainty of human life and health (learning from others, problem-accepting). He went out for a walk when overwhelmed by his sadness (problem-distancing, self-care) and prayed and talked to God about his fear (spiritual-related activities). During the crisis time, he received a lot of support from his siblings: “Everybody just comes together and does the best thing they can” (help-receiving). Jason shared how these behaviors made him feel recovered and “grown up” because he was able to take care of his family and he felt he had become a less selfish person through the experience.
Case 2
Anna, a White non-Hispanic woman of age 69, had been the primary care partner for her mom, Denise, age 93, for 2 years, since her initial diagnosis of dementia of unspecified type. At the time of Anna’s interview, Denise’s dementia was moderate (DSRS score = 31). After moving Denise to a new place, Anna discovered she had fallen. Although Denise seemed uninjured at the time, the next day, she wasn’t walking and complained about pain. Anna called 911 and advocated to have her mom to be hospitalized. The main challenges Anna experienced included communicating with healthcare providers about Denise’s needs and preferences, managing her mother’s transition home after discharge, lack of needed services such as physical therapy, lack of specific instructions for Denise’s care, and fear and worry seeing her mom in pain.
Anna reflected on how she could be assertive in the past when she cared for other family members (reflecting), and used that experience to advocate for her mom (problem-solving). She actively sought help and collected more information from healthcare providers and friends to make decisions for her mom (help-seeking, learning from others). She received some support from social workers to prepare for her mom’s discharge (help-receiving). When feeling frustrated about the lack of support, Anna tried to acknowledge that crises were temporary and that she was doing all she could at that moment (problem-accepting). Anna tried to care for herself by doing something relaxing, such as walking, sleeping more, seeing friends, and watching TV (self-care, developing and maintaining meaningful social relationships). To respect Denise’s preference and reduce the stress of dealing with well-meaning visitors, she took sole responsibility for attending to her mom during her hospitalization (help-disengaging, relational compassion behaviors). When interviewed after the crisis, Anna reported that she had recovered and could incorporate new things she learned into everyday life. She had started to accept that new crises could arise in the future, but she was now better equipped to handle what might come.
Discussion
To our knowledge, this is the first study to systematically use empirical data to examine resilience-related behaviors of dementia care partners. Centering our exploration around a health crisis of persons with dementia, we identified four major challenges associated with this critical point in dementia caregiving. Our findings align with previous literature about care partners’ experiences of challenges during crises (MacNeil Vroomen et al., 2013). We also identified two new challenges associated with persons with dementia’s health crisis events: challenges in resolving conflicts within informal care networks and care partners’ frustration with the lack of support. Few interventions thus far address these challenges for dementia care partners (Manietta et al., 2022; Spillman et al., 2019).
Care partners’ behavioral responses to these challenges were used to validate and expand the multi-dimensional behavioral CP-R framework. We confirmed the existence of four domains, including problem-response, help-related, self-growth, and learning, each containing several behaviors. We identified a new compassion-related behavioral domain that includes self-sacrifice and relational compassion behaviors. We confirmed previously identified behaviors and discovered additional behaviors: problem-accepting and problem-observing in the problem-response domain and help-disengaging behaviors in the help-related domain. The identification of previously overlooked behavioral domains expands our understanding of how to conceptualize and operationalize resilience in the challenging journey of dementia caregiving.
Some studies suggest the positive impact of relational compassion behaviors on dementia care partners but do not directly operationalize and evaluate these behaviors. Previous studies showed that positive, loving relationships with persons with dementia, acceptance of caregiving roles (Kim & Chang, 2022), commitment to care (García-Toro et al., 2020), and balancing care responsibilities to care recipients and other family members (M. Tong & Xu, 2019) are associated with resilience. While self-sacrificing behavior has been conceptualized primarily as detrimental to care partners’ physical and mental health (Tatangelo et al., 2018), we see that it can reflect moral commitment and contribute to personal growth. In this study, care partners perceived it as a meaningful way to express gratitude for years of positive, committed relationships. When self-sacrifice is an intentional decision to lift responsibilities from others, it can also result in a sense of satisfaction. The case of Jason illustrates the importance of both self-sacrificing and relational compassion behaviors; both empowered him to overcome immediate challenges and feel he had grown from the experience as a caregiver for his family members.
Our findings align with the recent development of an evolving resilience literature focused on dementia care partners’ experiences, most of which emphasize the importance of some of the behaviors included in the CP-R: problem-solving, self-care, learning, and the use of social support (Altamirano & Weisman de Mamani, 2021; Liu et al., 2021; Nguyen, 2022). The CP-R framework brings together and organizes a broad range of behaviors that have served, individually or in combination, as intervention targets in different dementia care partner intervention models, such as Powerful Tools for Caregivers (Won et al., 2008) and Resourcefulness Training (Zauszniewski et al., 2016). By combining a range of resilience behaviors into a single empirically testable framework, CP-R could be useful in guiding the selection and tailoring of specific interventions to improve resilience and related behavioral outcomes. The case of Anna describes a resilient care partner; however, she might still benefit from coaching about how to access essential health care services for her mother, such as physical therapy, or learning how to provide some of those rehabilitation activities herself.
Previous studies disagree about what coping behaviors are desirable and what are not: for example, “avoidance coping” has been seen as undesirable and linked to anxiety and depression (García-Alberca et al., 2012), yet it can be helpful, especially when disruptive factors are beyond their control (Cooper et al., 2007). In the face of unmodifiable challenges, problem-distancing behaviors might allow care partners to restore equilibrium and prepare for managing longer-term challenges.
Additionally, we identified problem-accepting and problem-observing as important behaviors in response to specific stressors encountered during an acute health crisis of persons with dementia, as illustrated in the cases of Jason and Anna. Both ‘buy time’, allowing care partners to reflect before choosing how to take action. In a recent study, Nguyen (2022) identified “accepting their challenging situations” as an essential resilience process. Previous studies also found that patience/tolerance, resignification/acceptance, and cognitive reappraisal were related to resilience (García-Toro et al., 2020; Laird & Lavretsky, 2019). Both problem-accepting and problem-observing align with the theoretical foundations of the mindfulness intervention approach, which focuses on developing non-judgmental awareness and acceptance of present moments and experiences (Kabat-Zinn, 2009). A recent systematic review identified only five studies investigating the effect of mindfulness-based interventions in dementia care partners and found an immediate reduction in stress (Kor et al., 2018). Future studies could use the CP-R framework to examine the impact of mindfulness-based interventions on resilience.
Disengaging from others’ help has generally been considered problematic, especially when care partners reject informal or formal help in the face of high levels of perceived need for support (Apesoa-Varano, 2020; Zwingmann et al., 2020). As illustrated by both Jason and Anna’s experiences, we found that disengagement can be used to protect care partners’ time and energy during difficult times, maintain care quality, and protect the dignity of persons with dementia while reducing emotional stress for other family members. These findings supported the need to view care partners as competent and knowledgeable experts (Apesoa-Varano, 2020) and recognize their right to choose to reject unwanted or intrusive help, no matter how well meaning. Disengaging behaviors can also be used as a signal by other family members and care providers to re-assess when, where, and what support care partners need, and what support is not helpful.
We found that expanding the domains of resilience behaviors did not affect the overall pattern of intersection between them: all domains continued to intersect, and each could be associated with learning – an essential mechanism for improving resilience over time. Using a broad, situationally-tailored, domain-based, and learning-informed framework for developing resilience interventions could bring the strengths of different existing interventions together in a new, more flexible approach that can support care partners in overcoming the shifting and changing challenges that characterize the journey of dementia care (Gallagher-Thompson et al., 2020).
Strengths and limitations
Our study has many strengths. The data collection and analysis plans were firmly grounded in the literature and systematically guided by a clear theoretical framework, allowing us to intentionally elicit information relevant to resilience. Interviews were conducted shortly after care partners experienced challenges during their care recipients’ health crisis; such interview time points supported care partners’ detailed recall of their experiences. The abductive thematic analysis approach allowed us to move back and forth between prior understanding and new data to generate a more comprehensive behavioral framework for dementia care partner resilience.
Our study has several limitations. Although our relatively small sample includes heterogeneous care partner types (young, <35 years old; primary vs supporters; men and women; and those experiencing financial strain vs not), a few care partners of color (e.g., Black, Asian, and Latinx) were enrolled; this likely reflects the demographic makeup of the source hospitals’ patient population and is a gap requiring attention in future studies. We validated and expanded the CP-R framework based on care partners’ experiences addressing challenges associated with just one crisis situation – a health crisis of persons with dementia; findings may not be generalizable to other types of dementia caregiving challenges, especially the chronic stress and care burden associated with long-term caregiving. Further studies should examine the CP-R framework in different contexts of dementia caregiving, engage a larger number and more diverse participants, and use longitudinal study designs to examine care partners’ resilience over time and care status. The current study identified these resilience-related behaviors based only on care partners’ recall and qualitative, self-report descriptions; it is unclear how these behaviors, individually or in combination, related to resilience outcomes and what factors shape these behaviors, which warrants future investigation.
Implications
The expanded CP-R framework provides a comprehensive model for developing and evaluating behavior-based measures to capture dementia care partners’ resilience and inform future interventions. The unique contribution of the CP-R is that it organizes detection, understanding, and, potentially, cultivation of resilience-related behaviors as a focus for care partner interventions. This framework also allows future research endeavors to identify factors that may shape different resilience-related behaviors (e.g., dementia types and stages, dyad’s physical, functional, cognitive, and behavioral status, relationship quality, and sociodemographic characteristics) to understand how to enhance care partners’ resilience, and when, where, for whom, and which resilience-enhancing interventions are particularly needed. The resilience perspective could enrich existing evidence-based care partner interventions by evaluating how they influence the developmental process that underpins successful longitudinal caregiving. The expanded CP-R framework contains underappreciated adaptive behaviors (self-sacrifice, relational compassion, problem-observing, and problem-accepting) that can be used to guide the design of innovative mindfulness or compassion-based, resilience-oriented interventions.
The complex patterns of intersections among different resilience-related behaviors signify the importance of recognizing and promoting a flexible, varied behavioral repertoire that, in aggregate, can promote resilience. Future research should examine different adaptation patterns of resilience-related behaviors, predictors of different patterns, and how these patterns are associated with resilience outcomes. This holistic approach that considers multiple behaviors and their intersections in a unifying framework can inform the development of highly impactful multi-component interventions.
Supplemental Material
Supplemental Material - Validation and expansion of a behavioral framework for dementia care partner resilience (CP-R)
Supplemental Material for Validation and expansion of a behavioral framework for dementia care partner resilience (CP-R) by Yuanjin Zhou, Dilara Hasdemir, Emily Ishado, Soo Borson, Tatiana Sadak in Dementia
Footnotes
Acknowledgments
We would like to thank all the care partners who participated in the study and contributed their wisdom from their everyday care practices. The interview data generated during and/or analyzed during the current study are not publicly available due to their sensitive personal nature and the possibility of revealing the identity of the participants. However, authors are available for answering questions about data and analytic methods.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The parent study from which this study was developed was supported by an award (5R21AG054144-02) from the National Institute on Aging (PI Sadak). Author Y. Z. was supported by funding from the National Institute on Aging, Grant Number: P30AG066614, and Eunice Kennedy Shriver National Institute of Child Health and Human Development, Grant Number: P2CHD042849.
IRB statement
Ethical approval was granted on 11/6/2017 by the Institutional Review Board at the University of Washington (STUDY00002012).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.