
Abstract
Objectives
The aim of this integrative review was to identify and synthesize the literature on peer support interventions for people living with or caring for someone with a rare or young onset dementia.
Design
A literature search of articles was performed using the Nipissing University Primo search system, a central index that enables simultaneous searches across databases which included MEDLINE (PubMed), Web of Science, PsycINFO, CINAHL, Sociological Abstracts, Cochrane Library.
Results
The eleven papers that met the inclusion criteria spanned eighteen years and from five countries. Studies reported on peer support programs that were either hospital-based (n = 6) or community-based (n = 4), and were predominantly led by disciplines in the health sciences. Only one study did not involve delivering services. There was a range of methodological quality within the studies included in the review. Further analysis and synthesis led to the identification of three overarching peer support themes. These included: (1) peers as necessarily part of social support interventions; (2) a theoretical portmanteau; and (3) dementia spaces and relationality.
Conclusion
Consistent with a much larger body of work examining peer involvement in social interventions, this review reinforced the valuable contribution of peers. A full understanding of the mechanisms of change was not achieved. Notwithstanding, the issue of studies neglecting to sufficiently conceptualize and describe interventions is an important one – drawing attention to the need to continue to explore varied delivery, including co-produced models, and more effective evaluation strategies to inform the dementia care sector.
Introduction
The World Alzheimer Report (Gauthier et al., 2021) estimates that there are 55 million people living with dementia worldwide. The report also indicates that only 25% have a diagnosis and 30% are misdiagnosed. Within these figures are those living with a rare, inherited, or young onset dementia (see, for example, Murray et al., 2011; Tang-Wai et al, 2004). While the primary cause of dementia is Alzheimer’s disease (AD), Harvey et al. (2003) suggest that atypical or vascular causes may account for approximately 25% of all diagnoses. Atypical forms of dementia are more likely to be diagnosed in individuals under the age of 65 (Brotherhood et al., 2019). Recently, Hendricks et al. (2021) calculated that there are 3.9 million people between the ages of 30 – 60 living with young onset dementia.
Individuals who are diagnosed with dementia at a younger age face a myriad of intersecting bio-medical, life stage and structural challenges that are increasingly recognized within the literature. Foremost, age, atypical symptom profiles and a lack of specialist neurological services for those living outside large urban centres often result in a delayed or inaccurate diagnosis (Canadian Academy of Health Sciences, 2019). Individuals not only face a future of neurodegenerative decline, but the loss of employment, unexpected marital and childcare transitions, disrupted relationships, and social exclusion due to numerous systemic barriers preventing full citizenship participation (Mayrhofer et al., 2018; Millenaar et al., 2016; Sonnicksen, 2016). Problem-solving and coping due to these psychosocial circumstances are also hindered by an absence of dementia services that can flexibility tailor supports for individuals with a non-Alzheimer’s diagnosis, who are younger in age and who may require a family-centred approach to care (Harris & Keady, 2009; Novek & Menec, 2021).
Peer support, while long familiar in the mental health and disability sectors, has recently achieved more prominence within dementia care. Peer support has been defined in a variety of ways but is generally presented as “a system of giving and receiving help founded on key principles of respect, shared responsibility, and mutual agreement of what is helpful” (Mead et al., 2001: p. 135). Positively received by service users and providers within the health and social care sectors, virtual or face-to-face peer support for care partners as a supplement to professional support are commonplace. Peer support for people living with dementia is less widespread, although opportunities for socialization among peers is common in many not-for-profit dementia organizations. For individuals affected by a rare or young onset dementia, tailored peer support or opportunities to engage with peers is patchy at best (Brotherhood et al., 2020). This gap in support means that their access to peers is by connecting with others who are associated with multiple different conditions, dementia stages and ages.
There is a growing body of literature on peer support in dementia care reporting a variety of positive outcomes for people living with dementia and care partners. A recent scoping review on peer support (Carter et al., 2020) and a systematic review on support interventions for care partners (Dam et al., 2016), however, have identified various methodological limitations in this body of literature. Therefore, there are still gaps in the evidence of what works to facilitate an adoption of peer support best practice models in service delivery. Nevertheless, outcomes for care partners are reported to include improvements in understanding dementia and care strategies through experiential sharing, a sense of belonging, feeling less alone, reduction in stress and anxiety, and sharing and empathy (e.g., Lauritzen et al., 2015; Smith et al., 2018; Willis et al., 2016). Although understandings are more restricted for people living with dementia, outcomes include reduced loneliness and isolation, and improved overall wellbeing (e.g., Theurer et al., 2015; Willis et al., 2016). The homogenization of peer support delivery means it is difficult to generalize from these studies as to whether either the models and/or the outcomes are meaningful specifically for people living with a rare or young onset dementia and their care partners.
Methods
Aims
The aim of this integrative review was to identify and synthesize the literature on peer support interventions for people living with or caring for someone living with rare or young onset dementia. Research questions were: 1. What are the characteristics of people living with rare or young onset dementia and/or their care partners investigated in the literature? 2. How is peer support conceptualized in the literature? What are the theories or mechanisms of change in peer support? 3. What are the specific interventions (or components of interventions) using peer support (e.g., supportive counselling, telephone support, education, social/recreational), how is it delivered, and what are the reported outcomes? 4. What is the methodological quality of the available evidence on peer support in rare or young onset dementia care and support?
The review protocol was registered with PROSPERO, an international prospective register of systematic reviews (ID CRD42020164951).
Design
Given design heterogeneity among the studies within the literature an integrative review was adopted. Looking both broadly and critically at the area of interest, an integrative review includes: (1) problem identification; (2) systematic literature search; (3) data quality appraisal; (4) analysis and synthesis; and (5) presentation and dissemination (Toronto, 2020). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) was followed to report this review (Page et al., 2021). The quality appraisal was conducted using the Joanna Briggs Institute (JBI) appraisal tools for qualitative research and quasi-experimental (non-randomized) studies (JBI, 2020) and the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018). Data synthesis was consistent with an integrative convergent design (Noyes et al., 2019).
Search strategy
A literature search was performed in February 2021 and updated in December 2021 using the Nipissing University Primo search system, a central index that enables simultaneous searches across databases to which the library is subscribed as well as content beyond the university’s collection. The databases included MEDLINE (PubMed), Web of Science, PsycINFO, CINAHL, Sociological Abstracts, Cochrane Library using different iterations of the following search terms: ‘peer support’; ‘peer mentoring’; ‘peer befriending’; ‘peer volunteering’; ‘dementia’; ‘young onset dementia’; ‘early onset dementia’; ‘young onset alzheimer’s disease’; ‘early onset alzheimer’s disease’; ‘frontotemporal dementia (FTD)’; ‘familial FTD’; ‘dementia with Lewy bodies’; ‘posterior cortical atrophy’; ‘familial Alzheimer’s disease’; ‘primary progressive aphasia (PPA)’, and Boolean operators, ‘AND’ and ‘OR’. Additional articles were obtained by searching reference lists of included studies. Less common dementias may be categorized using different terms (e.g., young onset, early onset, rare dementia). ‘Rare dementia’ was not included as a search term because it provided very few results in a pilot search. The specific diseases or conditions included as search terms were those that are more common among rarer forms.
Inclusion/exclusion criteria
The population of interest in this review included persons 18 years and older, living with or caring (e.g., spouse/partner, child, other relative or friend) for someone living with a rare or young onset dementia, defined as people living with a rare dementia at any age or people living with dementia with a younger age of onset (that is, under 65 years). Diseases or conditions of interest included including Alzheimer’s disease, FTD, Lewy body dementia or other less common forms (e.g., primary PPA, posterior cortical atrophy, familial FTD, familial Alzheimer’s disease). Peer support included any type of program delivered alone or with other interventions (i.e., multicomponent) that involved peers who possess experiential knowledge of living with or caring for someone living with dementia or a part of natural or embedded social networks (such as family, friends, or neighbours) (Dennis, 2003).
Studies were included if they focused on the population of interest and the program as described above, published in English language, and were primary research studies using any methodology (qualitative, quantitative, or mixed methods). There was no time limitation to the publication date. Studies were excluded if the population of interest was older than 65 years and the type of dementia was not reported, support interventions included peers and non-peers or paid peers and did not report primary data.
Study selection and data extraction
The selection process for the review is represented in Figure 1. Records retrieved from the Primo search were imported into Rayyan, a free web and mobile app that provides semi-automation for screening articles (Ouzzani et al., 2016). Duplicates were identified by Rayyan and removed. One reviewer (AG) screened titles and abstracts after duplicates were removed. Full texts of 56 papers considered eligible for review were screened independently by two reviewers (AG, MPS) and discrepancies were resolved through discussion between both reviewers. Forty-eight papers were excluded because they did not meet the inclusion criteria. An additional nine papers were obtained by searching reference lists of included papers. The two reviewers independently screened the full texts of these papers resulting in the exclusion of five papers that did not meet the inclusion criteria. A total of 11 studies were included in this review. PRISMA flow diagram showing the process of selecting studies for the review.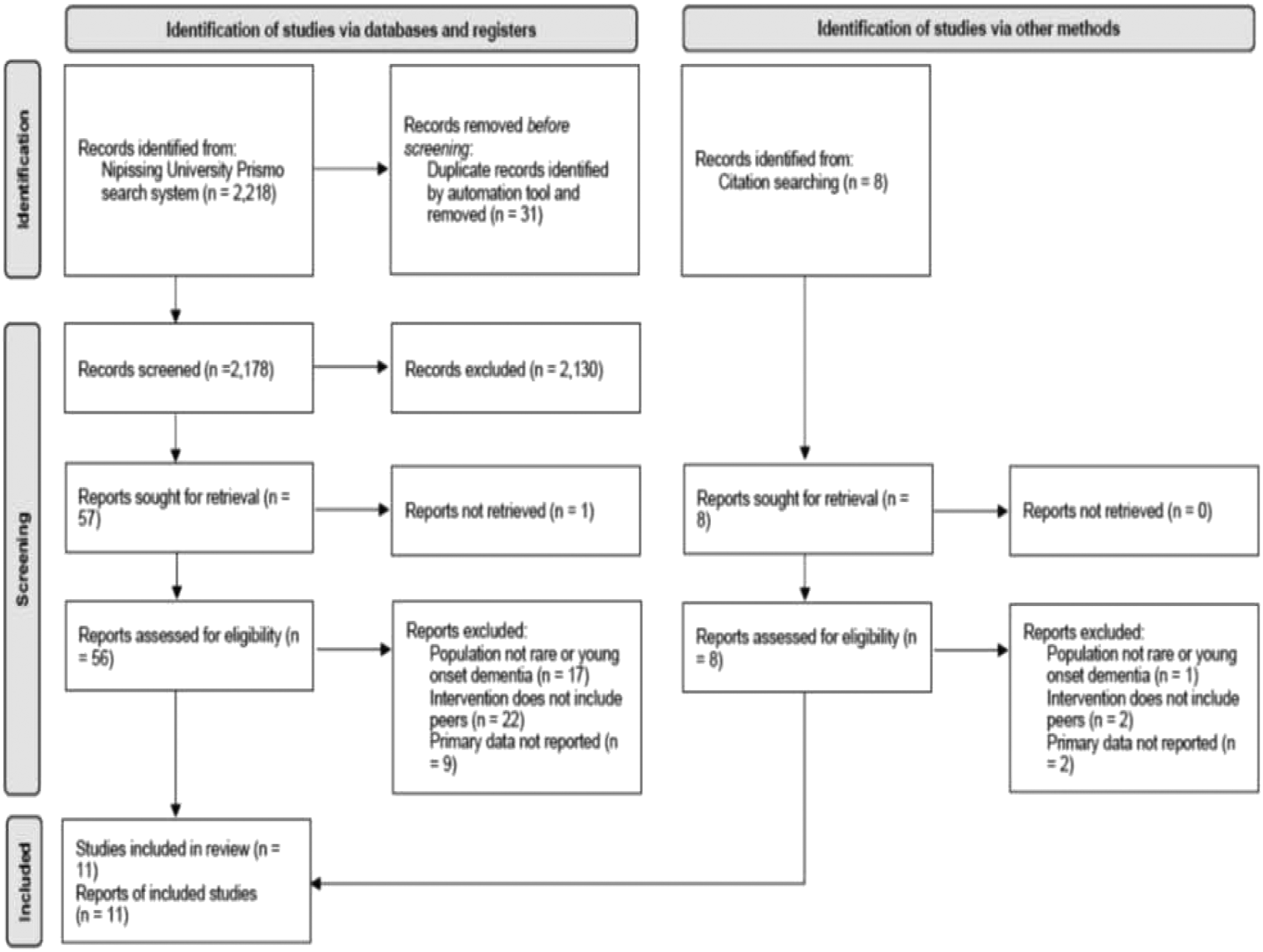
No authors were contacted for further information. A bespoke data extraction tool was created and included information on study characteristics including year of publication, country of origin, aims, design, sample size and methodology. Data extraction was undertaken by the two reviewers.
Quality assessment
The quality of included papers was evaluated by three reviewers (AG, MPS, VW) independently using the JBI Checklist Tools (2020) and in one instance the MMAT (Hong et al., 2018), with disagreements resolved by a second evaluation and further discussion until consensus was reached. No papers were excluded despite some being considered of low overall quality.
Data analysis and synthesis
Data analysis and synthesis was completed by two reviewers (MPS and VW). Both data immersion and reduction were completed by the creation of an enhanced data matrix which focused and organized the data (i.e., objective of intervention, conceptual background, delivery, outcomes) and memoing throughout this process (Toronto & Remington, 2020). Qualitizing the data occurred at this time whereby descriptive statistics in results sections were assigned words and/or phrases (Noyes et al., 2019). This was followed by an inductive coding process assisted by Atlas.ti version 8 to facilitate the development of themes relevant to the research questions (Braun & Clarke, 2006).
Results
Study Characteristics
Eleven papers included in the review spanned 18 years and from a range of countries including: Canada (n = 4), United Kingdom (n = 4), Australia (n = 1), US (n = 1) and Germany (n = 1). Studies reported on support programs that were either hospital-based (n = 6) (Diehl et al., 2003; Jokel et al., 2017; Marziali & Climans, 2009; Morhardt et al., 2019; O’Connell et al., 2014; Taylor-Rubin et al., 2020) or community-based (n = 4) (Carone et al, 2016; Clare et al., 2008; Davies-Quarrell et al., 2010; Phinney et al., 2016) and were predominantly led by disciplines in the health sciences. Only one study did not involve delivering services (Stamou et al., 2020).
Four papers were published between 2003 and 2010 describing interventions for frontotemporal dementia (FTD) (n = 2) (Diehl et al., 2003; Marziali & Climans, 2009), a support program established by people living with dementia (n = 1) (Davis-Quarrell, 2010) and an internet-based self-help network (n = 1) (Clare et al., 2008). The remaining seven papers published between 2016 and 2020 were interventions for primary progressive aphasia (PPA) (n = 3) (Jokel et al., 2017; Morhardt et al., 2019; Taylor-Rubin et al., 2020), social/recreational programs (n = 2) (Carone et al., 2016; Phinney et al., 2016), video-conferencing support group for people in rural settings (n = 1) (O’Connell et al., 2014) and exploring post-diagnostic needs of people living with or caring for someone living with dementia (n = 1) (Stamou et al., 2020).
Summary of included studies (n = 11).
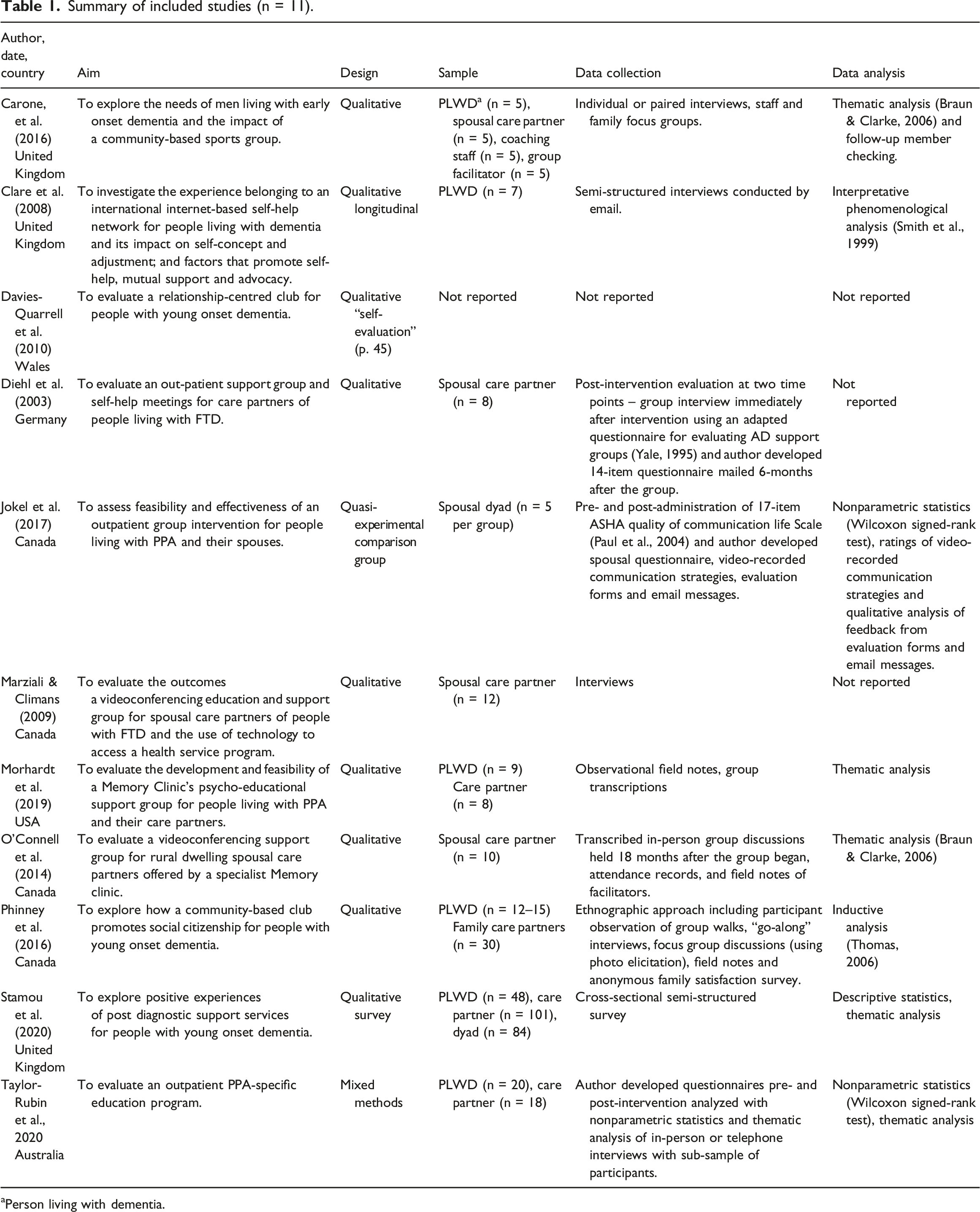
aPerson living with dementia.
Description of peer support within an intervention (n = 11).
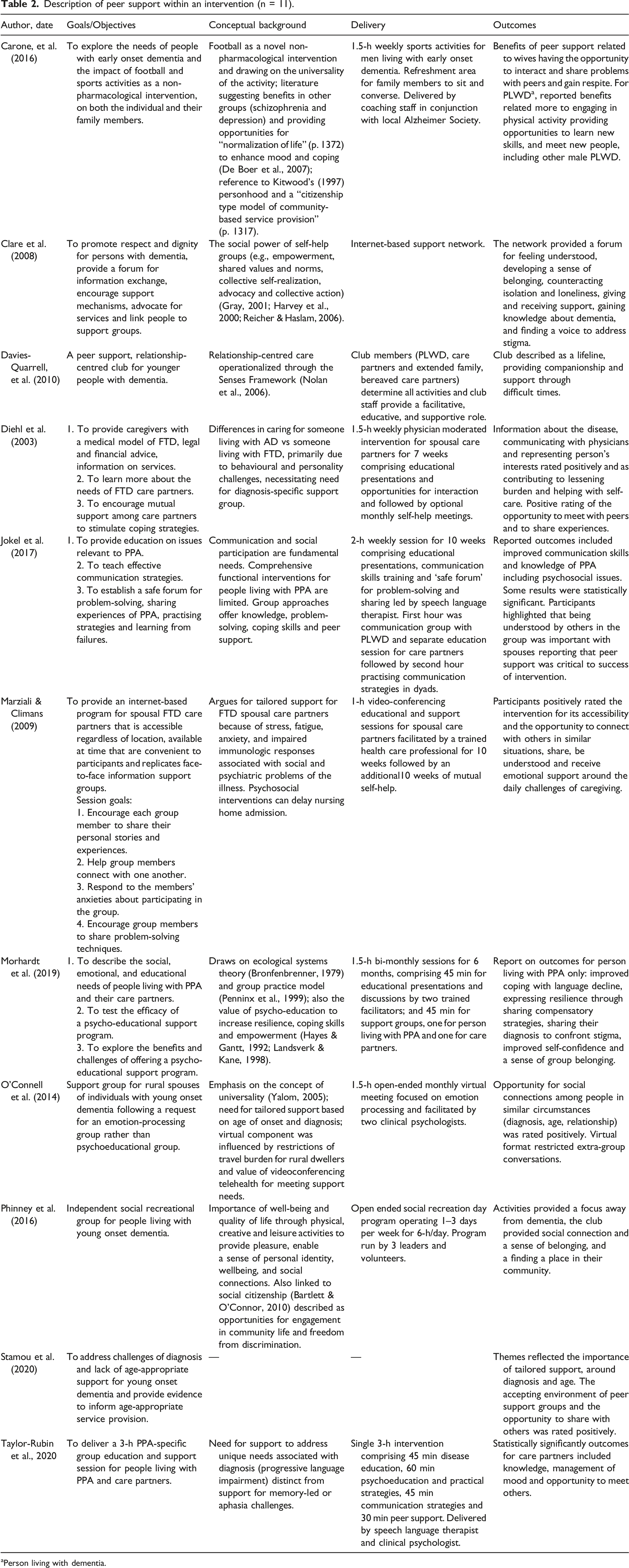
aPerson living with dementia.
Quality assessment of evaluation methods
Of the 11 included studies, nine were qualitative studies, with the remaining being quasi-experimental and mixed methods research. When reported (n = 9), data evaluating the impact of the peer support were collected using interviews only (Clare et al., 2008; Marziali & Climans, 2009), interview and focus group (Carone et al., 2016), standardized questionnaire (Jokel et al., 2017), adapted and author developed questionnaire (Diehl et al., 2003), author developed questionnaire and interview (Taylor-Rubin et al., 2020), post group discussion, field notes and attendance records (O’Connell et al., 2014), interviews, focus group, observation, and satisfaction survey (Phinney et al., 2016), and field notes and group transcriptions (Morhardt et al., 2019). The paper that reported on post-diagnosis supports described an author developed qualitative questionnaire (Stamou et al., 2020).
There was a range of methodological quality in the studies included in the review. Within the qualitative studies, most papers (n = 7) neglected to define peer support, include a statement regarding the location of the researchers culturally or theoretically, and/or a statement commenting on the influence of the researcher on the research or vice versa (i.e., reflexivity). Four of these papers were also identified as lacking clarity in terms of how the conclusions were drawn from analysis. These issues reflect many of those also raised by Carter et al. (2020) and Dam et al. (2016). The remaining 4 papers were of good quality overall. The quality assessment of the papers is set out in Supplementary File 1. There was no evidence in the studies published after 2013 of the use of the Template for Intervention Description and Replication (TIDier) (BMJ, 2014) to enhance the quality of reporting on interventions.
Theoretical and conceptual frameworks
The next stage of analysis and synthesis led to the identification of three overarching peer support themes. These included: (1) peers as necessarily part of social support interventions; (2) a theoretical portmanteau; and (3) dementia spaces and relationality. 1. Peers as necessarily part of social support interventions
An examination of findings specific to the contribution of peers demonstrated that, without exception, peers were viewed as an essential element within support programs for people living with rare or young onset dementia. The inclusion of peers as a necessary ingredient within multi-component support was also reinforced in Stamou et al.’s (2020) survey results. No authors identified any negative results emerging from peer involvement, although O’Connell et al. (2014) expressed concern about the management of extra-group relationships.
The positioning of peers to achieve support outcomes within a community-based service (e.g., Carone et al., 2016; Davies-Quarrell et al., 2010; Phinney et al., 2016) appeared to be distinctly different than that in outpatient interventions (e.g., Jokel et al., 2017; Morhardt et al., 2019; Taylor-Rubin et al., 2020). For community-based services the staff role was primarily facilitative and the emphasis on social participation and support through peers appeared to occur more naturally through walking (Phinney et al., 2016) or football (Carone et al., 2016), for example.
Within the outpatient interventions it was difficult to establish the exact nature of the support provided by peers, apart from peer discussions, due to detailed description being largely absent. Outpatient interventions were professionally designed apart from O’Connell et al. (2014) who involved service users in the design of a “emotional-processing group” (p. 386). In contrast to community programs, these were time-limited and most often characterized by diagnosis specific psychoeducation with scheduled peer support time (Jokel et al., 2017; Morhardt et al., 2019; Taylor-Rubin et al., 2020), or optional self-help following the professionally led education (Diehl et al., 2003). Here too, the psychologist’s, speech language therapist’s, physician’s or social worker’s role was in the foreground. The interventions targeted both people living with dementia and care partners, in the instance of PPA, and only care partners for people living with FTD. In addition, there were more flexible group agendas that purposively focused on virtual peer sharing among care partners despite being professionally facilitated (Marziali & Climans, 2009; O’Connell et al., 2014). Marziali and Climans (2009) also offered a 10-weeks self-help group at the conclusion of the formal sessions. It is worth noting here that the outcomes for the groups with a psychoeducation component, and evaluated using pre/post questionnaires, appeared to demonstrate participants valued the professional contribution followed by peer engagement. This was similarly reported by Stamou et al. (2020) where opportunities for social participation including “camaraderie” and “sharing with others” (p. 5) followed specialist advice and information, age-appropriate services, and interventions for physical and mental health.
To what extent do support group members need to share similar characteristics and how does this impact on outcomes? The most homogenous support was offered by O’Connell et al. (2014) with care partner participants purposefully sharing similar age, relationship, and partner’s diagnosis (8 of 10 participants caring for someone living with FTD). It was not clear, however, if the extent of homogeneity here had any significant impact on outcomes. Community-based supports focused on younger age, and Clare et al.’s (2008) on-line self-help group and Davies-Quarrell et al.’s (2010) club model were also characterized by stage of dementia (early to mid). Outpatient interventions were condition specific (i.e., FTD, PPA) and emphasized the need for tailored psychoeducational support as opposed to the more commonly offered generic dementia education. Where care partners were involved most were female and spousal, although this appeared to be by chance (Carone et al., 2016; Marziali & Climans, 2009; Morhardt et al., 2019; Taylor-Rubin et al., 2020). Peer support for male care partners was notably absent. Stamou et al.’s (2020) survey to document post-diagnostic support needs identified the demand for age versus diagnosis tailored support. 2. A theoretical portmanteau
The theoretical foundations for each study, how they conceptualized both peer support and the lives of people affected by rare or young onset dementia, were both explicit and implicit but providing some evidence of the authors’ conceptual alignment. A blend of conceptualizations or ideas which we identified as a theoretical portmanteau were more common yet sometimes difficult to attribute to peer support specifically.
Peer support emerging from community-based programs seemed to be more affiliated with understandings emerging from self-help, personhood or person-centred care, the social model of disability and social citizenship. Clare et al. (2008) were unique in their exploration of digital self-help for people living with dementia arguing that both face-to-face meetings and professional involvement were not necessary to achieve coping benefits from support from peers. The authors also reported that self-help permitted the development of collective social identities which would in turn create social and political power to enable advocacy and change efforts (Gray, 2001; Harvey et al., 2000; Reicher & Haslam, 2006). The “accepting social environment of peer support” and opportunities to “have a voice” or “raising awareness on young onset dementia” (p. 6) were also identified by Stamou et al. (2020). The use of self-help in outpatient support for care partners was not expanded on or evaluated (Diehl et al., 2003; Marziali & Climans, 2009).
Explanations using or inferring Kitwood’s personhood or personalizing cultures (1997), normalization and social role valorization (Thomas & Milligan, 2018), and the right to full citizenship participation with and among peers for people living with dementia (Bartlett & O’Connor, 2010) were features in Davis-Quarrell et al. (2010) and Phinney et al. (2016) and implied in Carone et al. (2016). As Phinney et al. (2016) stated “…citizenship is not a fixed status but is performed through everyday experiences of movement and mobility…guided by a philosophy that foregrounds the importance of continued participation in activities they consider to be normal” (p. 389). This deviation from a deficit model to a strengths-based one, enablement and a relationship-based approach was underscored by Davis-Quarrell et al. (2010) and their use of the Senses Framework to examine the outcomes a club model for people with young onset dementia (Ryan et al., 2008). Remarkably, the Senses Framework dismissed a hierarchy among peer groups in their club model (i.e., person living with dementia or care partners or staff) and argued that relationship-centred care was achieved when all senses (achievement, belonging, continuity, purpose, security, and significance) were experienced among all groups, including staff (Ryan et al., 2008).
Elements of the mental health recovery model, including self-help, biomedical conceptualizations of caregiving stress and burden, Yalom’s (2005) therapeutic factors for group psychotherapy, and ecological systems theory were evident in the outpatient peer support interventions. Recovery model concepts such as connection with others, empowerment, meaning and identity (Leamy et al., 2011) and recovery capital (Tew, 2013) were evident to some degree in Diehl et al. (2003), Jokel et al. (2017), Marziali and Climans (2009), Morhardt et al. (2019), O’Connell et al. (2014) and Taylor-Rubin et al., 2020. Although overlapping with personhood conceptualizations, the emphasis in these relational support interventions for both people living with dementia and care partners appeared more aligned with the development of recovery capital and centering personal efficacy as well as longer-term coping.
The biomedical binary of coping dementia care partner/not coping dementia care partner was also evident in Diehl et al. (2003), Jokel et al. (2017) and Marziali and Climans (2009). Interventions that were delivered by psychologists (O’Connell et al., 2014; Taylor-Rubin et al., 2020) placed considerable importance on Yalom’s (2005) universality and altruism factors, although delivering support groups as opposed to group psychotherapy. Finally, Morhardt et al. (2019) introduced ecological systems theory (Bronfenbrenner, 1979) to explain how people “understand and cope with their illness in relation to others” (p. 1312), and group psychoeducation as a means of expanding social networks alongside normalizing experiences, developing tools for self-care (Penninx et al., 1999) and coping and empowerment (Hayes & Gantt, 1992; Landsverk & Kane, 1998). These conceptualizations were not returned to in their discussion of outcomes, and where relevant, if these were more salient for people living with dementia and/or care partners. 3. Dementia spaces and relationality
Whereas an evidence-informed model of peer support did not emerge due to the varied population and nature of the evaluations conducted, the studies encouraged valuable reflection on the grounds that individuals affected by dementia inhabit previously unimagined social spaces taking on meaning in relation to others who inhabit similar spaces. Moreover, there was a recognition that a sense of belonging via peer support (i.e., inclusion) was a requested space for people affected by rare or young onset dementia (e.g., Carone et al., 2016; Clare et al., 2008; O’Connell et al., 2014; Stamou et al., 2020). Yet peer support was a scarce resource in the broader community of dementia care services (e.g., Davis-Quarrell et al., 2010; Jokel et al., 2017; Marziali & Climans, 2009; Taylor-Rubin et al., 2020). Importantly, these were relational spaces where all individuals expressed, practiced, and shared their new identities.
These studies recognized, largely using qualitative data, a variety of relational features common within coping networks or achieved during opportunities for social participation. These features remained more or less visible in formal multi-component groups, informal social/recreational programs or a self-help network, and whether they were delivered virtually or face-to-face. Relationality among others who were similar, whether a person living with dementia or a care partner, was reported as feeling normal and described as inclusive (Carone et al., 2016; Clare et al., 2008; Davis-Quarrell et al., 2010; Diehl et al., 2003; Marziali & Climans, 2009; Morhardt et al., 2019; O’Connell et al., 2014; Phinney et al., 2016; Taylor-Rubin et al., 2020). The relational aspects of these peer environments for care partners were also portrayed in terms of group reciprocity. The reciprocal nature of the groups through the sharing of experiential knowledge was thought to have positively promoted interpersonal competence and personal affirmation (Clare et al., 2008; O’Connell et al., 2014; Taylor-Rubin et al., 2020). Both Clare et al. (2008) and O’Connell et al. (2014) described reciprocity as reinforcing shared values and motivating genuine advocacy efforts for awareness raising and/or enhanced services. An engagement in advocacy activities to create positive social change may be an important feature within peer support for people who are younger in age.
Given dementia spaces also meant navigating change due to, for example, neurodegenerative decline or care transitions, relational safety among peers also seemed to be highly valued among study participants (Carone et al., 2016; Davis-Quarrell et al., 2010; Jokel et al., 2017; O’Connell et al., 2014). For example, Davis-Quarrell et al. (2010) using the Senses Framework (Ryan et al., 2008) described a sense of security as permission to be vulnerable in a supportive environment which in turn fostered personal growth. Jokel et al. (2017) described the value of people living with PPA practicing communication strategies with uncritical peers. Whereas community-based studies where focus was on the person living with young onset dementia there also appeared to be an emphasis on relational autonomy (Perkins et al., 2012). The creation of inclusive spaces and opportunities for social participation with peers supported both a participant’s selfhood and capabilities which, in turn, maintained both agency and autonomous action (Carone et al., 2016; Clare et al., 2008; Davis-Quarrell et al., 2010; Stamou, et al., 2020).
Discussion
The purpose of this literature review was to examine the characteristics of peer support for people affected by rare or young onset dementia, including benefits of participation and how this had been evaluated. Consistent with a much larger body of work examining peer involvement in social interventions, this review reinforced the valuable contribution of peers despite a full understanding of mechanisms of change not achieved. Notwithstanding, enthusiasm for peer support will likely remain, if not expand, and we thus draw attention to various considerations as these forms of support continue to be conceptualized, delivered, and evaluated.
Theorizing peer support
Thinking around who, why and how peers are included in support interventions for people affected by dementia continues to escape thorough theoretical clarity – that is, theorizing both the peer support and the characteristics and needs of the peer population. This is not unsurprising given that our theorizing about dementia, the complex lives of those affected, and policy and practice responses to the needs of people living with dementia are evolving across different disciplines. Many theoretical approaches have been criticized for either under theorizing structural influences on the lives of people living with dementia or avoiding how various constructs are applied at a practice level. In both instances these approaches neglect those in later the stages of their illness (Milne, 2020) and those who are living with an atypical or young onset dementia (Brotherhood et al., 2019). Studies in this review have not escaped these challenges.
Most studies in this review favoured an eclectic approach to peer support, yet congruent with explanations featuring elements from the recovery model, including self-help, disability studies and person-centred care. In other studies, these ideas informed the why but were not always articulated in terms of the who and how of peer involvement. For example, Phinney et al. (2016) argued the relevance of social citizenship to inform social participation with peers for people living with young onset dementia. While recognizing human rights and agency are valuable constructs for people living with dementia who are often denied these, clarity regarding how these informed the delivery of support were limited. Davis-Quarrell et al. (2010) adopted the lesser-known Senses Framework in their club model. The Framework positively focused on relationships among peers and others, but the study’s methods and analysis provided limited clarity on how the Framework guided any peer support delivery to the target population.
Arguably, the need for a broader and critical conceptual lens in dementia care delivery has been long recognized (Higgs & Gilleard, 2016), and yet any new or emerging conceptualizations were not explored within these studies. The exception was Davis-Quarrell et al. (2010), however, the study design made it difficult to extrapolate ideas for replication elsewhere. The complexities in peer support or peer influence for younger people with an atypical diagnosis due to everchanging family roles, neurodegenerative decline, and psychosocial transitions specific to age and stage were left largely underdeveloped. Despite the larger number of female care partners, normative assumptions around dementia caregiving were left unchallenged within peer delivery. Constructs around emotional labour, female identities, gender differentiated help seeking behaviours and others (Erol et al., 2016; Gilhooly et al, 2016; Pöysti et al., 2012), were only inferred by Marziali and Climans (2009) and O’Connell et al. (2014), and neglected elsewhere (e.g., Carone et al., 2016). Consumer driven or co-produced peer support models which complement both social disability and social citizenship paradigms, were not apparent among those studies aligned here although evident in Clare et al.’s (2008) report on self-help and O’Connell et al.’s (2014) emotional-processing group. Further, the desire to engage in advocacy efforts as identified by Clare et al. (2008) and O’Connell et al. (2014) required further explanation in terms of the target population and how this could be realized at a practice level. And finally, newer constructions emerging from relationship-centred or relational citizenship models (Kontos et al., 2017) were not explicitly expanded on, although resonating within some of the study findings and how these were discussed.
Characterizing the delivery and evaluation of peer support
Both community-based non-profit organizations and out-patient health services were responsible for the provision of peer support interventions asserting the need for tailored support given age and/or diagnosis. This rationale is supported elsewhere (e.g., Queluz et al., 2020). The role of peer support within a continuum of care and how this interacted with other health or social care services for people living with rare and young onset delivery was not illustrated in any study. Their delivery varied in a number of important ways that was no doubt a reflection of both funding and the extent of professional involvement. Community-based involvement in peer support was characterized by social participation and relationship development, particularly for people living with dementia who were younger in age. As Phinney et al. (2016) noted, dementia was not the focal point within these social networks. By and large outpatient peer support delivery for people living with dementia and care partners was time-limited, included with psychoeducation and its emphasis on dementia knowledge and coping skills. Three studies reported on virtual delivery with positive outcomes similar to face-to-face groups. This finding also echoes Carter et al. (2020) in their scoping review of peer interventions for dementia care partners. This is particularly timely given our current context, and recent shifts in thinking about the potential for virtual delivery in terms of reaching a population that is geographically dispersed or accommodating care partners and their caring or employment responsibilities.
Discerning the contribution of peer-led versus professional-led peer support, the ideal extent of heterogeneity or homogeneity among peers, and support for people living with dementia versus care partners was difficult to establish. Visible gaps in our understandings included peer support for children, parents or siblings who also play important caring roles and yet understudied and unnoticed in support programs (Roach et al., 2016), the role of peers for individuals where their dementia is in the later stages and/or their care partners, and ethnocultural, linguistic and other diverse groups where both the life course and inequalities require critical attention (Milne, 2020).
Regarding intervention evaluation, the studies reporting on peer support delivery focused on in-depth service descriptions including feedback from users (Carone et al., 2016; Clare et al., 2008; Davies-Quarrell et al., 2010; Marziali & Climans, 2009; Morhardt et al., 2019; O’Connell et al., 2014; Phinney et al., 2016) and outcome evaluations with an emphasis on the professional component of delivery (Diehl et al., 2003; Jokel et al., 2017; Taylor-Rubin et al., 2020). The contribution from the qualitative studies was welcomed given the complexities in support delivery. Though their lack of conceptual development and methodological rigour was at times disappointing, these contributions were important to stimulate further theorizing and reinforcing the need to develop more rigorous evaluation designs. In the case of outcome evaluations, the absence of a theory of change or logic model, where relevant, may have impeded the development of a more effective evaluation strategy including both process and outcome evaluations. An emphasis on the latter meant that the how (e.g., resources, activities, decisions) specific to delivery were not set out, reported on, or analyzed. The absence of process evaluations of peer interventions to inform randomized clinical trials was also recently identified by Walker and Peterson (2021).
Strengths and limitations
The strength of this literature review was that it provided an integrative synthesis of peer support for people affected by rare and young onset dementia which is an under-researched population. The review and synthesis also followed established protocols including an evaluation of the quality of the research, although challenging at times given differing methodological and analytical approaches. Our synthesis of how peer interventions were theorized adds an important contribution given this is often unaddressed in other reviews. The review is limited, however, due to the small number of papers that met the inclusion criteria. A review of studies addressing other rare conditions or chronic long-term illness in younger populations may have provided us with other valuable insights. The results of our quality review where authors neglected to address both theoretical and researcher bias or other views affecting reported outcomes also impacted on our own conclusions.
Conclusion
The lack of recognition of dementia diversity within the largely homogenous dementia care sector has resulted in people affected by rare and young onset dementia being denied opportunities to participate in tailored peer support. A growing body of literature on living with an atypical condition is now casting a light on varied dementia spaces characterized by, among others, health, illness, loss, change and caring, and in doing so, acknowledging the possibilities for peer support models purposefully directed to reach those previously forgotten. The broader issue of studies neglecting to sufficiently conceptualize and describe interventions is an important one – drawing attention to the need to continue to explore varied and innovative delivery (e.g., co-produced models) and robust process and outcomes evaluation methods to inform support delivery within the dementia care sector.
This work is part of a larger study exploring tailored and continuous multi-component support for people affected by rare or young onset dementia, including the contribution of peers. The important insights gathered here will contribute to the further exploration of models of support provision and their evaluation in the practice sector.
Supplemental Material
Supplemental Material - Peer support for people living with rare or young onset dementia: An integrative review
Supplemental Material for Peer support for people living with rare or young onset dementia: An integrative review by Mary Pat Sullivan, Veronika Williams, Adetola Grillo, Roberta McKee-Jackson, Paul M Camic, Gill Windle, Joshua Stott, Emily Brotherhood and Sebastian J Crutch in Dementia
Footnotes
Acknowledgements
This work is part of the Rare Dementia Support Impact project (The impact of multicomponent support groups for those living with rare dementias, ES/S010467/1) and is funded jointly by Economic and Social Research Council (UK), part of UK Research and Innovation, and the National Institute for Health Research (UK). The views expressed are those of the author(s) and not necessarily those of the ESRC, UKRI, the NIHR or the Department of Health and Social Care. Rare Dementia Support is generously supported by The National Brain Appeal (![]() )
)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Economic and Social Research Council (ES/S010467/1) and National Institute for Health Research (ES/S010467/1)
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
![]()
![]() ). He is also Clinical Director of the UCL Clinical Psychology Doctorate with overall responsibility for the practice based learning elements of the largest training course for clinical psychologists in the country. His research programme is grounded in clinical practice and focuses on understanding psychological processes in ageing and dementia and developing appropriately adapted psychological interventions.
). He is also Clinical Director of the UCL Clinical Psychology Doctorate with overall responsibility for the practice based learning elements of the largest training course for clinical psychologists in the country. His research programme is grounded in clinical practice and focuses on understanding psychological processes in ageing and dementia and developing appropriately adapted psychological interventions.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.