
Abstract
Background
Governments are being challenged to integrate at least part of dementia care into primary care. However, little is known about the current role of general practitioners (GPs) regarding dementia care, especially in countries that do not have dementia strategies in place. The aim of this study was to explore the experiences of GPs, persons with dementia and their family carers in Portuguese primary care settings, to better understand GPs’ contribution to dementia care.
Methods
A qualitative interview study of participants recruited from six practices in different social contexts within the Lisbon metropolitan area was carried out. Purposive sampling was used to recruit GPs, persons with dementia and carers. Interviews with GPs explored dementia care comprehensiveness, including satisfactory and challenging aspects. Interviews with patients and carers explored the experience of talking to GPs about cognitive impairments and related difficulties and the type of help received. Thematic analysis of interview transcripts was carried out using the framework approach.
Results
Five major themes were identified: GPs have a limited contribution to dementia care, the case of advanced dementia, doctor–patient relationships, doctor–carer relationships and management of chronic conditions other than dementia.
Conclusion
General practitioners seemed to contribute little to dementia care overall, particularly regarding symptom management. The exception was patients with advanced stages of dementia, given that specialists no longer followed them up. Remarkably, GPs seemed to be alone within primary care teams in providing dementia care. These findings strongly suggest that Portuguese primary care is not yet prepared to comply with policy expectations regarding the management of dementia.
Keywords
Introduction
The increasing prevalence of dementia challenges governments to develop and improve services for persons with dementia, and especially to integrate dementia treatment and care into primary care (Alzheimer-Europe, 2017; WHO, 2017). There is consensus about the essential role of GPs, namely recognising early manifestations of dementia, disclosing the diagnosis, monitoring and managing care needs, and coordinating care (Aminzadeh et al., 2012). Nevertheless, evidence suggests that dementia is under recognised and under managed in primary care (Prince et al., 2016).
The few studies assessing the quality of post-diagnosis services indicate primary care underperformance in several domains, for example assessing signs and symptoms of dementia (Wilcock et al., 2016), managing anti-psychotics (Connolly et al., 2012), managing depression (Connolly et al., 2012; Wilcock et al., 2016) and assessing social support and carers’ needs (Connolly et al., 2012; Wilcock et al., 2016). Another study indicated that most carers had received insufficient information from GPs, but nonetheless expected their guidance (Peterson et al., 2016). Foley et al. (2017) explored GPs’ dementia care educational needs and found that GPs mostly focused on neuropsychiatric symptoms (NPS), while patients and carers identified the need for GPs to engage in counselling and signposting of local services. A more recent study focused on carers’ needs and barriers to dementia management in primary care (Wang et al., 2018). Carers seemed to be more in need of care guidance and psychological support, whereas GPs gave limited help because of their heavy workload. Previous research also suggests that persons with dementia may receive lower levels of care for cardiovascular comorbidity than those without dementia (Connolly et al., 2013).
Various barriers to the recognition and management of dementia in primary care have been identified, and a growing body of evidence focuses on their complex and multifactorial characteristics (Balsinha et al., 2019). Three systematic reviews on this topic highlight the importance of patient factors (e.g. non-compliance with care and medication), GP factors (e.g. a general lack of knowledge regarding dementia, lack of training in communicating with the patients and their families) and, thirdly, system characteristics (e.g. limited availability of support services) (Aminzadeh et al., 2012; Koch & Iliffe, 2010; Mansfield et al., 2018).
The Portuguese population has currently the third highest estimated prevalence of dementia in OECD countries (OECD, 2019). The Alzheimer Europe Yearbook 2019 estimated that 193,516 people with dementia lived in the community in Portugal, where the population is over 10 million people (Statistics-National-Institute, 2018). Using the 10/66 Dementia Research Group algorithm, a prevalence rate of 9.2% (95% CI 7.8–10.9) was reported in a Portuguese sample of community-dwelling older people; the authors argue that strict DSM-IV criteria may underestimate the real prevalence of dementia (Gonçalves-Pereira et al., 2017).
While this represents a public health challenge, everyone in Portugal has access to the National Health Service (NHS), in principle. General practitioners are considered to be their first point of contact with the NHS and provide a gatekeeping function (Gonçalves-Pereira & Leuschner, 2018). People registered in primary health centres in Portugal are grouped in ‘family files’, which means that all members of a three generation family will probably consult the same GP. However, this is not a universal picture. For instance, a relevant proportion of people still lack an appointed GP and that could be the case of people with dementia moving to their adult children home in other health centre area. Portuguese GPs are allowed to prescribe anti-dementia medication, but patients are only reimbursed with neurologists’ or psychiatrists’ prescriptions. Patient access to these specialists in the NHS is mainly limited by waiting lists, mandatory referral by GPs and, in some cases, travelling long distances (Balsinha et al., 2019). Although Portuguese GPs are ‘specialists’ strictly speaking, the use of this term is commonly applied to doctors other than GPs. Therefore, in this article, the term ‘specialist’ will refer to neurologists and/or psychiatrists.
A dementia strategy was published in Portugal in 2018 (Dispatch n° 5988/2018). The strategy assigns primary care for the tasks of early screening for cognitive impairment, working with secondary care to enable integrated diagnosis and management of people with dementia, and to coordinate person-centred care for both patients and families with health and social care community services. The implementation of this strategy through an official policy or plan was to follow but has not taken place yet.
To our knowledge, most of the evidence available on how GPs provide dementia care comes from countries with some type of dementia strategy (Connolly et al., 2012; Peterson et al., 2016; Prince et al., 2016; Wilcock et al., 2016), and little is known about the countries that do not have dementia strategies in place as is the case of Portugal. Gaining knowledge about the experience of dementia care of patients, carers and GPs could inform future strategies or policies in countries where they are still non-existent or scarcely implemented, but also in those countries where official guidance is more available.
The aim of this study was to explore the experiences and perspectives of GPs, persons with dementia and their family carers about the current role of GPs in providing dementia care and the issues that impact on this role.
Methods
A qualitative study, involving individual semi-structured interviews, was performed. A purposive sampling was used to recruit participants (Ritchie, Lewis et al., 2003). Primary care services in different social scenarios within the Lisbon metropolitan area were selected. A contact person in each practice recruited the GPs. The inclusion criterion was experience of providing care to persons with dementia. The GP sample included both genders and a range in years of clinical experience. The persons with dementia were recruited by their GPs, taking into account the inclusion criteria: having a dementia diagnosis according to ICD-10 DCR and being able to give informed consent. The patients with dementia comprised both genders, were in different stages of dementia and had different types of kinship with their carers. The inclusion criteria for carers were to be the primary carer and to chaperone the patient in consultations. All primary carers were family carers. Ethics committee approval was obtained for the study and written informed consent was obtained from each participant.
The sample size needed was estimated to be 10–12 participants using Guest et al.’s (2006) methods. Sampling led to an initial recruitment of 10 GPs and 10 dyads of persons with dementia and their carers, across six general practices. Nine doctors were matched with 10 dyads, and a 10th doctor was recruited for sample saturation purposes. Data saturation criteria were based on an initial analysis sample of 10 interviews and on a stopping criterion of two interviews where no new ideas would emerge (Francis et al., 2009). These criteria were met at the sixth interview with persons with dementia and 10th interview with carers. In the case of GPs, only in the last interview did new ideas fail to emerge.
A total of 28 participants were interviewed: 10 GPs, eight persons with dementia and 10 carers. Severity of dementia was assessed with the Clinical Dementia Rating (CDR) (Morris, 1993). Two of the 10 persons with dementia had advanced dementia (Alzheimer and frontotemporal sub-types) and were not able to be interviewed. The ability to recall what happened in GPs’ consultations was limited by cognitive impairment in three participants. This led us to focus the interview on their subjective experiences, which is also a valid way to learn about the experiences of persons with dementia (Wilkinson, 2005). All interviews were conducted between March and December 2018. For the participants’ convenience, the interviews with persons with dementia and their carers took place in their homes and with GPs at their practices. The interviews were conducted one-to-one to enhance the in-depth approach.
Quality framework for dementia care delivery in GPs’ consultations.
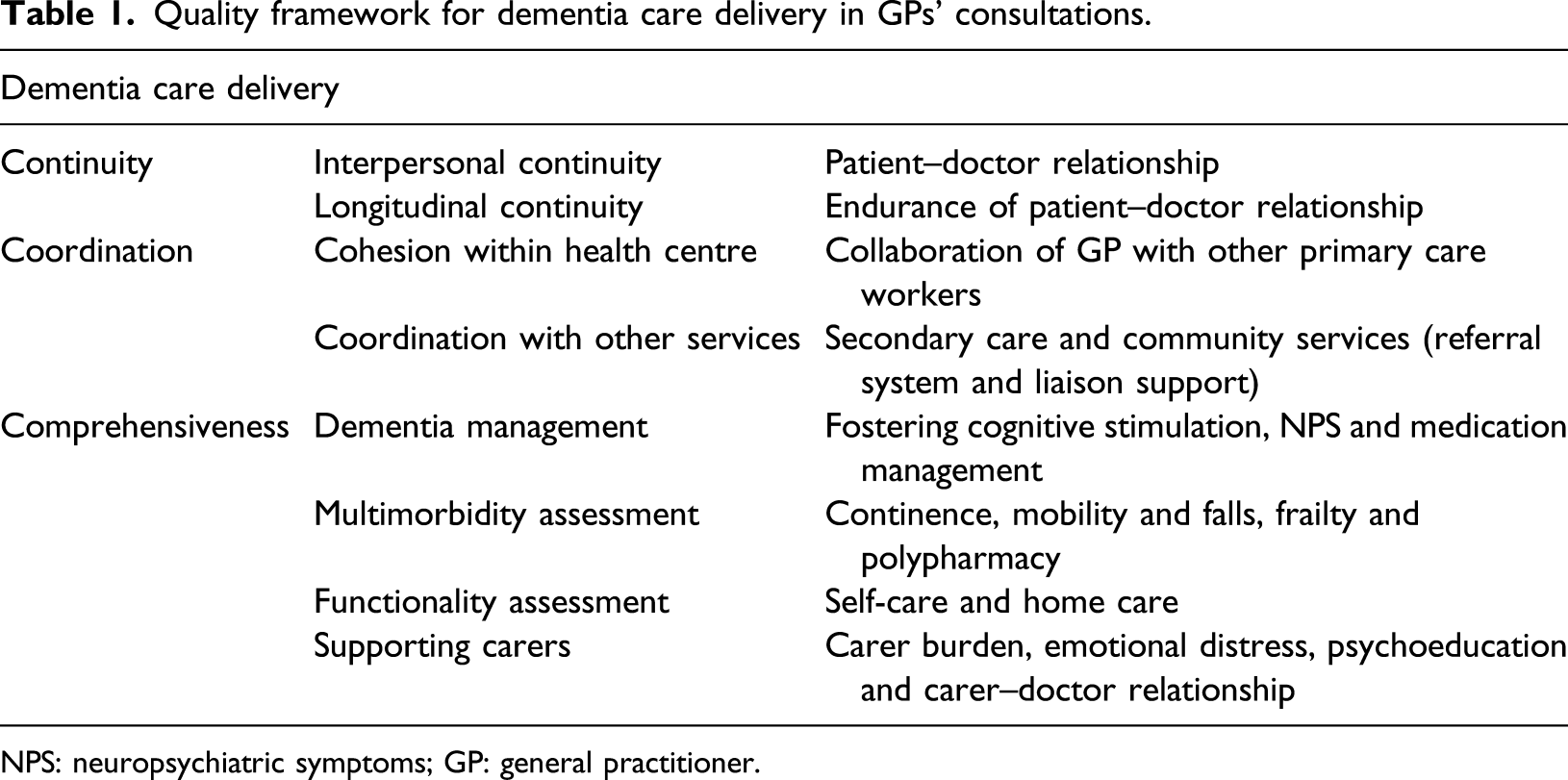
NPS: neuropsychiatric symptoms; GP: general practitioner.
Interviews’ topic guide.
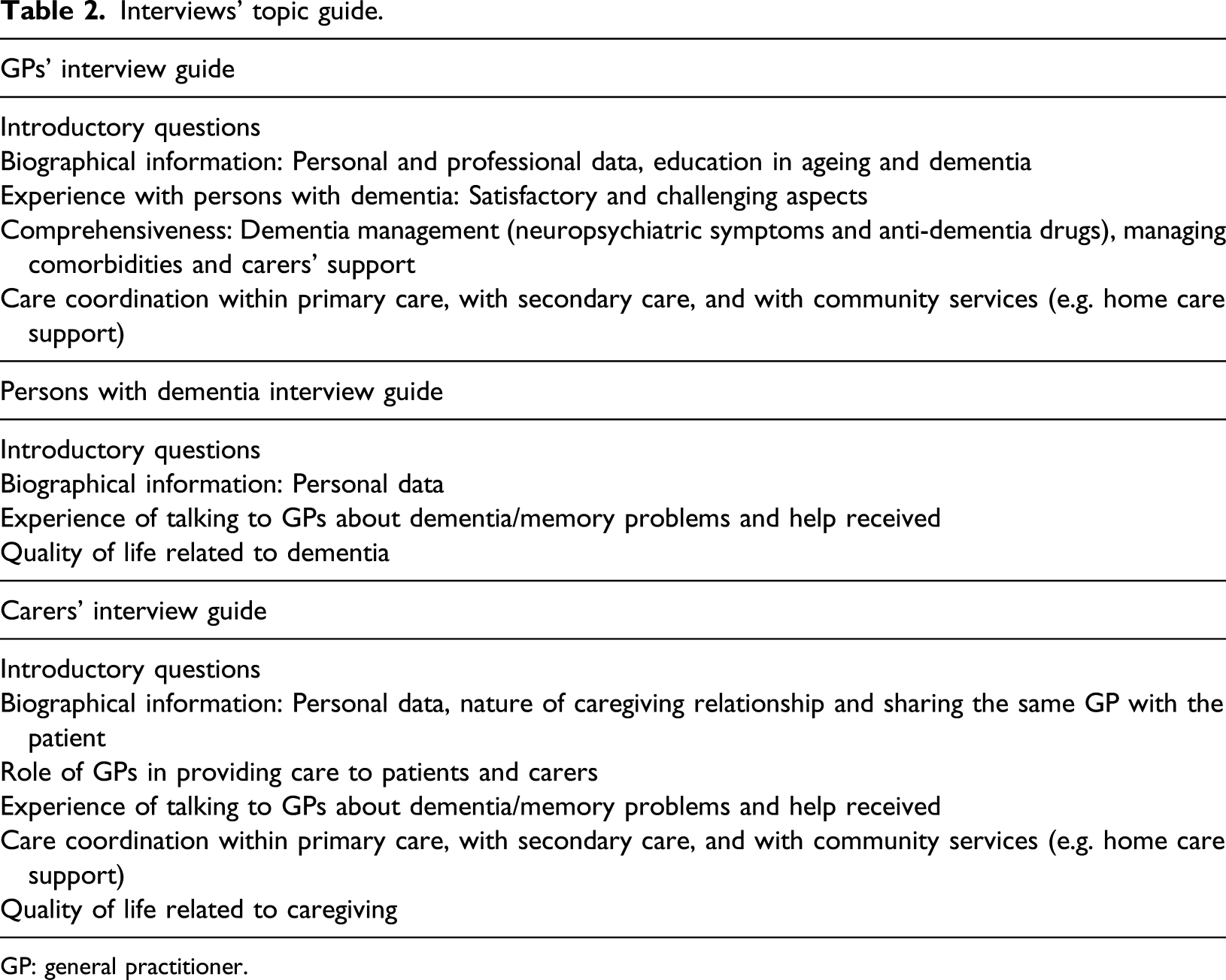
GP: general practitioner.
Six pilot interviews (two with each type of participants) were conducted to assure the length, detail and clarity of the interview guides and to identify gaps in the topics addressed. As a result, some questions were rephrased and sequentially aligned, and prompts were added to clarify the answers.
Interviews were informal in style, enabling specific issues to be explored as and when they arose (Creswell, 2014). Expressions such as ‘memory problems’ (for dementia) could be used initially when talking to persons with dementia or carers, unless or until they used the specific term ‘dementia’ or ‘Alzheimer’s’.
Interviews lasted around 40 minutes and were digitally recorded, transcribed and anonymised. Transcriptions were always done before the next interview, allowing for new ideas to be explored and discussed by the interviewers (Creswell, 2014). The accuracy of the transcripts was checked by the primary author.
The codebook was designed by the first author, drawing on the study’s quality framework (see Table 1). It was tested in the coding of nine interviews (three per group of participants) by two of the authors, independently. Simultaneously, the authors performed inductive coding and discussed the themes emerging. An analytical framework with five themes was then developed and applied to each transcript. Any discrepancies were resolved by discussion and consensus.
The framework approach (Ritchie, Spencer et al., 2003), thematic analysis (Braun & Clarke, 2006) and data triangulation were core components of the data analysis. This approach enabled the transcripts to be handled in systematic stages, improving the transparency of results. Thematic analysis allowed inductive logic to be used for themes originally not anticipated to be included.
NVivo 12® was used to manage data analysis and simplify data retrieval.
Findings
Group characteristics (N = 28).
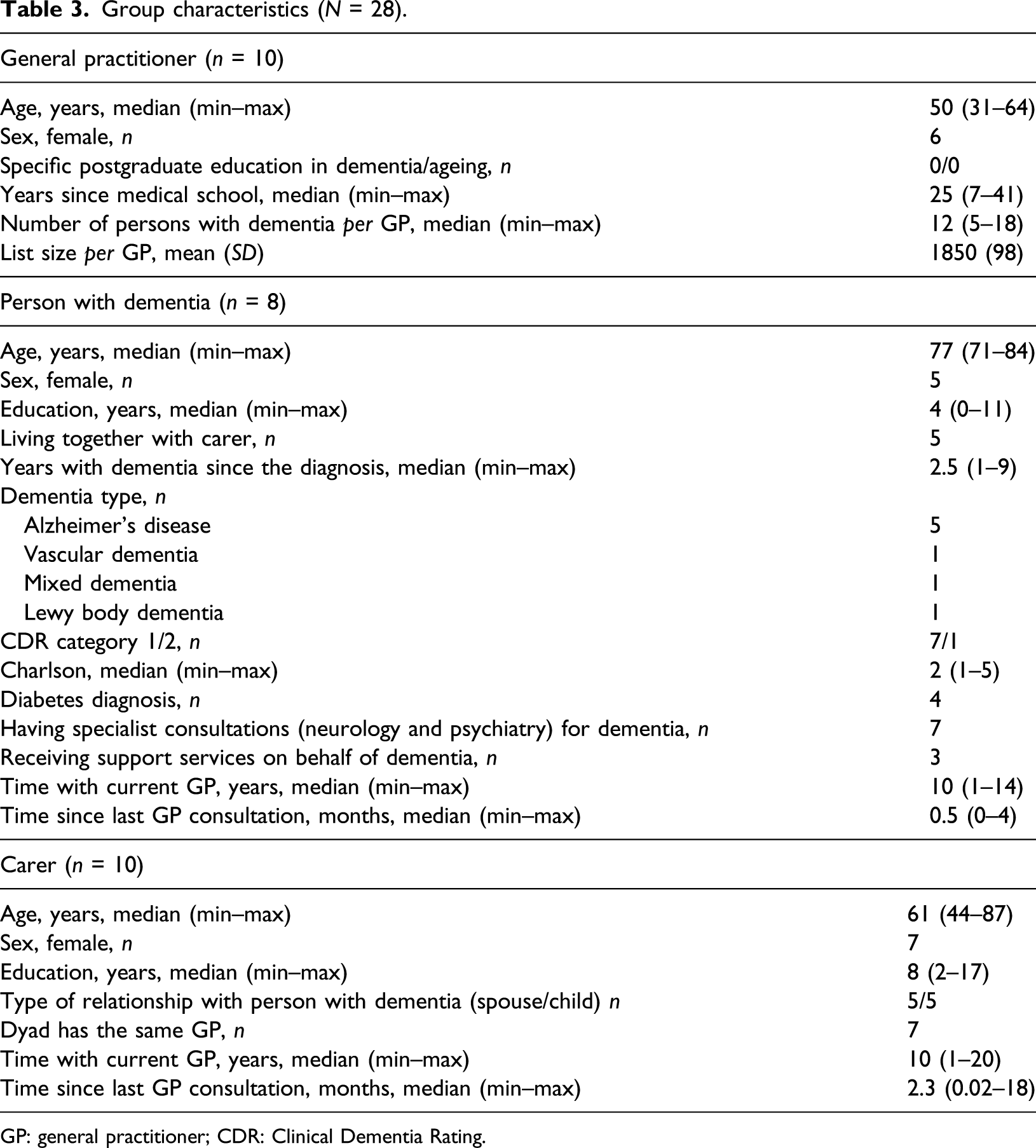
GP: general practitioner; CDR: Clinical Dementia Rating.
Six out of the 10 GPs were female. The median age of GPs was 50 years. None of them had had any specific training in dementia. The median number of patients with dementia in each of these GPs’ register was 12.
Five of these eight patients were female. Their median age was 77 years and their median years of education were 4 years (corresponding to primary school education). Three of the patients lived alone. The median time since the diagnosis was 2.5 years. Seven patients had mild dementia (CDR = 1) and seven were being followed in specialist outpatient services for dementia. The median length of registration with the current GP was 10 years. Finally, seven out of the 10 carers were female. Their median age was 77 years. Half were spouses and the other half were adult children. Seven of the carers shared the same GP with their relatives.
Five major themes and four sub-themes were identified and are summarised in Figure 1. Thematic map.
All GPs perceived their role in providing dementia care as a difficult and challenging one. This complexity was highlighted by many GPs and their overall attitude to dementia care tended to be pessimistic.
To better understand how relevant dementia care provision in primary care is, the relative importance of dementia among other patients’ chronic conditions was specifically explored in patients’ and carers’ interviews. None of the patients talked about having dementia or Alzheimer’s disease, and only a few identified their ‘forgetfulness’ as their most important health problem. However, from the perspective of all carers, their dementia was the most important health problem for their relatives.
GPs have but a limited contribution to dementia care overall
Although only a few GPs perceived themselves as very limited in providing dementia care to their patients, none of the patients remembered discussing memory problems with their GPs. Carers also found difficult to identify any meaningful situation where they had received assistance from GPs regarding dementia care specifically.
Providing information in dementia
Most participants reported that it was uncommon for GPs to provide information about dementia. None of the GPs had written information (e.g. a leaflet) available but also neither carers nor the patients would usually ask for it. The few GPs taking a role on this area reported that providing information was challenging; the symptoms were difficult for families to understand and consequently were wrongly attributed to long-standing personality problems.
…understand that the patient is a victim, that their behaviour is not just to upset the family, it is not their bad temper…GP7
In addition, the uncertainty of dementia progression compromised communication and increased difficulties in disclosing information that could raise further concerns.
…it’s difficult to anticipate how it’s going to be for that patient… and when they question us, it’s difficult to give a defined prognosis (…) and to be assertive in addressing their concerns. GP9
None of the patients mentioned having received information about their ‘memory problems’. Furthermore, none of the carers recalled their relatives being informed about their condition either by the specialist or by the GP. Most of the carers themselves reported not having received much information about dementia from GPs or specialists (albeit to a lesser extent), particularly regarding NPS management. Well, I don't think that any of them [GP and neurologist] had helped me that much. C6
This led to reliance on problem-solving, for example by searching for information in the internet.
…some things I know because I searched in the internet… for instance, I learned that I should avoid antagonising her… C2
Nonetheless, some carers regarded practical experience as the most important way of understanding dementia and coping with it, perceiving the role of the doctors as irrelevant. No one really helped me to understand this [dementia]… but I think that may not be relevant after all… days go by and will notice the changes, learn by our own … C10
Neuropsychiatric symptom management
For most GPs, NPSs were one of the most challenging areas to manage in dementia and most relied on specialists to treat these symptoms. Since NPS were essentially considered to be ‘aggression’ and ‘agitation’, GPs also perceived them as uncommon in their daily practice.
Some situations have to be managed with medication, but generally they are already medicated by the neurologist, so I don’t need to do anything. GP8
When GPs had to manage aggression and agitation symptoms, most of them reported using mainly anti-psychotics, as first-line treatment; however, a few had to use coping strategies to overcome their difficulties in managing the medication. … as we do not prescribe these drugs every day, when I have to do it, I study or talk with my colleagues who have more experience instead. GP2
Although a few GPs acknowledged the importance of non-pharmacological measures to manage NPS, none of them described helping carers to manage these symptoms.
Only a few GPs usually addressed depression, but only in the context of differential diagnosis in the early stages of dementia.
At the early stages is difficult to make the differential diagnosis with depression, especially in the elderly. GP6
Most patients reported feeling sad or anxious too often without understanding the reasons for mood changes. Frequently, this was not considered a topic to be addressed by health professionals in general (including GPs) but to be accepted rather than confronted.
Sometimes I'm sad… but it's hard to say ... because now I’m feeling good, but tomorrow who knows?… That's how it is ... (...) but I have never talked about this with the GP, I never needed to … P1
Some carers reported difficulties in understanding and managing their relatives’ behaviour (particularly paranoid ideas about ‘invented robberies’), describing them as being stubborn for not acknowledging their ‘forgetfulness’
He says unimaginable things ... that everyone steals his things. Things disappear because he doesn't remember where he kept them, and he doesn't acknowledge that, he is very stubborn. C1
Anti-dementia drug management
Most of the GPs admitted having very limited knowledge about anti-dementia drugs, partially resulting from the lack of specific training in dementia. Moreover, some stated that the prevalence of patients with a diagnosis of dementia registered in their practices was low as compared with other conditions. I’ve never had training in dementia (…) the prevalence of dementia is so much lower than of other conditions that I don’t make an effort in studying it, and because I rely on the specialist to do it [anti-dementia drugs management] more effectively… GP2
Some of the GPs ended up delegating the management of these drugs to specialists because reimbursement was only possible with specialists’ prescriptions. Consequently, none of the GPs were used to initiating or stopping these medications, identifying their side effects or adjusting doses.
I don't even prescribe them because they are not reimbursed, so I usually leave it entirely to the specialist. GP8
There was variation in carers’ experiences of GPs’ management of these drugs. While a few carers reported that their GPs usually renew the prescriptions despite the reimbursement issues, a few others believed that GPs were actually forbidden from prescribing these drugs.
‘The GP just cannot prescribe that medication, so we never talked about that.’ C1
Dementia is not the GPs’ responsibility
One GP referred that ‘common sense’ regards dementia as a condition to be managed by neurologists, consequently keeping the patients away from GPs.
…most people think that dementia is for neurologists and I think we (GPs) do too. (…) They end up having less contact with us than they should have. GP5
Accordingly, some patients took the view that ‘memory problems’ were not to be managed by their GPs.
It is not worth talking about that, because the consultation with the GP is not about brains, he is not familiar with that. P9
Other reported that their mood changes were a matter to be taken care of by other professionals.
I don't think it's for the GP, maybe for the psychologist or neurologist… P4
Most carers also believed that dementia was a condition to be managed by ‘specialists’, being sceptical regarding GPs’ actual competence to help them regarding the difficulties they were facing.
I don't know... She is a GP... Maybe, if she had some medical specialty more focused on [dementia]… C2
In line with this, all carers recognised the role of GPs in managing their relatives’ health problems in general terms, but most of them restated that this would not apply to dementia.
(…) (GP) is very useful for managing other conditions, but with respect to dementia itself I think he doesn’t make much difference… he is not the specialist… C5
The Case of advanced dementia
Some GPs perceived themselves as responsible for delivering home care for patients with advanced dementia, although for a few this essentially meant managing intercurrent illnesses.
Sooner or later they end up needing home care and that fall upon on us. GP8
…when they have intercurrent illnesses, I make home visits. GP3
Most GPs reported that primary care nurses played a role in home care delivery but only regarding functional independence since they did not have specific training in dementia.
To help in carers education, falls prevention, how to adapt the house, etc. as in any other dependent patient. GP8
Carers of those patients in more advanced stages of dementia reported that their relatives had been discharged from the neurology clinic for more than 1 year; consequently, GPs and primary care nurses were the only healthcare professionals available to provide any type of care at home.
…the nurses came here a few times with the GP and told us how we should have our home adapted for this condition, I think they were great, very helpful. (…) Now, when we need something we call the GP. C9
Doctor–patient relationships
The type and quality of doctor–patient relationship was very much influenced by its duration (particularly if it was established prior to the onset of dementia), the characteristics of the dementia condition and the presence of carers during consultations.
A few GPs reported that a long-standing doctor–patient relationship allowed the maintenance of fulfilling relationships even in advanced stages of dementia. Moreover, the knowledge of premorbid characteristics (personality and attitudes) of patients allowed for more person-centred approaches, allowing the doctor to combine patients’ previous wishes with their current needs.
… what satisfies me the most is, when is possible to preserve their values, their will, based on what we know of these people and their families. GP4
On the other hand, a few GPs reported that their relationship with the patients could be compromised by pervasive cognitive impairment, which hampered clinical communication.
(…) this patient no longer has… well, he may hear what I say but later on he forgets, so I can’t have that much influence on his life, right? GP1
In addition, a few GPs also had difficulties in sympathising with patients’ problems and establishing rapport.
I find difficult to relate to these patients, because we repeat the same things over and over, like ‘watch out for the stairs’ … things that families tell them all the time, things they don't agree on, so… I don't think it's easy to foster a trusting relationship with patients with dementia. GP7
In contrast with their attitude towards carers, none of the GPs expressed the need to be alone with the patients; nevertheless, a few did recognise that the presence of the carer during consultations could compromise a truly person-centred approach.
… sometimes I have this concern, I realize that that person no longer has their intimacy because there is always someone present, sometimes someone in control. GP6
Regardless, most patients reported trusting and close relationships with their GPs, describing them as being available, thoughtful, trustworthy and ‘a friend’ to them.
I think he's an excellent man concerning talking with patients, he’s thoughtful. P4
Exceptions to this were the two patients that had only met their current GP after their diagnosis of dementia and had not established any kind of meaningful relationship.
For a few patients, it was difficult to recall what happened in consultations since the ‘memory problems’ began, so they described their overall impressions of the ongoing relationship with the GPs or gave ‘near answers’.
How are things going with your GP’s consultations?
She is a very delicate lady, very attentive! The best doctor I have ever had, I like her very much. P2
Doctor–carer relationships
The doctor–carer relationship seemed to be influenced by whether patient and carer were consulting the same GP, system characteristics and GPs’ attitudes to dementia.
Although most GPs expressed empathy about carers’ burden, their ability to assess carers’ needs depended upon the patient and carer consulting the same GP. This was seen as a necessary condition for GPs having time to assess carers’ practical needs (e.g. difficulties bathing their relative), as well as their emotional needs, otherwise they have to advise them to consult with their own GP.
It is difficult to help carers who are not my patients. I usually suggest them to talk to their GP. GP8
All GPs reported providing emotional support to carers, mainly through talking and listening, but only a few reported trying to identify carers’ stress, depression or sleeping problems. Moreover, a few GPs acknowledged that carers needed privacy in consultations in order to express their needs and concerns.
They are anxious, depressed, with sleep problems; they are another patient.... If they are your patients, it is easier because we can make an appointment for them, namely without the patient with dementia present, right? GP2
Most GPs identified carers as the key element of care coordination, which mostly consisted in assisting their relatives in daily living activities, ensuring GPs’ liaison with specialists (e.g. by transmitting information) and finding support services in the community. This was seen sometimes as an ethical obligation (assisting in daily living activities) and as something that could be easier for carers than for practitioners themselves (e.g. mobilising resources).
They have to understand that they have to help the patient with the medication, accompany them to consultations ...GP6
It’s much easier for them [carers] to talk to the neurologist than me (…) they are the liaison with the hospital. GP3
… usually they can mobilize resources more easily than I can, and more quickly. GP8
The few GPs, who regarded dementia as subject for specialists, considered the carers to be their primary focus of attention.
These carers are almost my only focus of attention in this problem [dementia]. Because, as a doctor, I feel I can't do anything for the patient, I have to send them to the neurologist. GP7
To some extent, this shift of focus was also the result of an insufficient knowledge about dementia.
… in fact, I feel more like I’m a doctor for the carer than for the patient, perhaps because I don't feel very comfortable in this area, I never had any specific training…GP3
Most of the carers who consulted their relatives’ GPs felt supported regarding their own needs.
… although she was ill, there she was, listening to me, talking to me (…) And I felt good, felt supported. C1
On the other hand, one of the carers who had a different GP from their relative felt misunderstood regarding their difficulties as a carer and that was taking its toll on their health. Other carers did not report any specific needs.
(…) for my sake it would be good that my GP would know the things I do for my mother, always running, sometimes I'm very anxious… if we both had the same GP, they would understand the reason for my complaints. C6
All the carers whose relatives were receiving home support services had to find these services on their own. One of them expressed that it would have been much better if there had been coordination between the health and social services.
But when we had to look for support services, we found no coordination between the practice and social services. C8
Management of other chronic conditions
General practitioners were recognised by most participants as playing an important role in managing the patients’ chronic conditions other than dementia. Nevertheless, none of the GPs reported assessing some specific conditions associated with dementia and with older age, such as frailty or the risk of falls. Polypharmacy was seen as an important issue to address by only one GP, who also highlighted the practical difficulties of the task. [In this patient] drug management is, by far, the most difficult. I have already de-prescribed several drugs… GP9
Some patients and most carers recognised that GPs played an important role in monitoring chronic health conditions other than dementia, such as diabetes.
I go see the GP because of diabetes… just for that…P7
… (GP) always schedules routine appointments to check blood tests results. C6
Discussion
This study describes the experience of GPs, persons with dementia and their carers regarding dementia care in primary care settings, in a country without a dementia strategy in place. To the best of our knowledge, this is the first study examining the current role of GPs in providing dementia care – and the issues that impact on this – in which data have been triangulated and integrated from multiple sources. Perhaps the most important finding was that these GPs, patients and carers shared limited expectations of what GPs can do about dementia, and these expectations were confirmed by their practical experience; for most of the participants, dementia should be and is mostly managed by specialists. Generally, GPs regarded dementia as a complex and challenging area of care, and for a few of them, its low prevalence in these primary care settings, as compared with other conditions such as diabetes, did not justify investment in dementia education. This last finding may reflect lower levels of knowledge about dementia prevention strategies or a pervasive stigma related with dementia, even in health professionals.
The first theme identified was that GPs have a small role in dementia care overall. The triangulation of data from patients, their carers and GPs revealed a stronger emphasis on GPs relying almost exclusively on specialists to manage dementia symptoms.
The general consensus of participants was that GPs rarely provide information about dementia, which is in line with previous research (Foley et al., 2017; Peterson et al., 2016; Wang et al., 2018). Surprisingly, this did not seem to be an issue to participants, given that GPs reported that carers did not usually ask them for information and most carers did not perceive it as a task for GPs. This was in contrast with studies suggesting that carers expect GPs to guide them through specific sources of information (Peterson et al., 2016) and provide care guidance (Wang et al., 2018). A possible explanation for these different attitudes is the lower educational background of the carers of this study.
In line with our findings, previous studies found a suboptimal management of NPS in primary care (Connolly et al., 2012; Wang et al., 2018; Wilcock et al., 2016). The triangulation of data in this study suggested that NPS misidentification along with little provision of information about dementia had important consequences for patients and carers alike. Most patients were experiencing emotional distress, regardless of being a symptom of dementia or an expression of emotional reactivity, which was being overlooked by themselves, carers and GPs. In fact, most carers attributed those changes to their character, including stubbornness. If not addressed, NPS can have a negative impact on the quality of life of patients and their families. None of the GPs expressed to need training in managing NPS, contrary to the findings in other studies (Foley et al., 2017; Koch & Iliffe, 2010). This may result from GPs relying on specialists to manage NPS, but can also reflect a flaw in the interview guide to address this topic. Remarkably, when specialists were unavailable, most GPs reported using anti-psychotics despite their lack of experience with these drugs. This is in line with literature which suggests that anti-psychotic drugs prescription is a common practice (Connolly et al., 2012; Wilcock et al., 2016). In Portugal, the OECD estimated in around 40 per 1000 the number of anti-psychotic prescriptions in people aged 65 years and over, but there are little data on anti-psychotic prescription in dementia (OECD, 2019). Despite national clinical guidelines for cognitive impairment recommending their use only under caution (Directorate-General-of-Health, 2011), there are indications that these drugs are overused in dementia. For instance, a study conducted in neurology and psychiatry outpatient services showed that 40% of a convenience sample of persons with dementia were on atypical anti-psychotics (Gonçalves-Pereira et al., 2010).
There are different guidelines regarding anti-dementia prescription in Europe (Petrazzuoli et al., 2017); in Portugal, only neurologists’ or psychiatrists’ anti-dementia drug prescriptions are reimbursed (Dispatch n° 13020/2011). Petrazzuoli et al. (2017) suggested that GPs who were allowed to prescribe anti-dementia drugs claimed higher engagement in dementia work up than GPs who were not allowed to do it. The study findings were consistent with this; despite Portuguese GPs being allowed to prescribe these drugs, the reimbursement issue seemed to affect their responsibility on their management. Consequently, most carers did not expect GPs to manage these drugs; in fact, a few actually believed that they were forbidden to prescribe them. Importantly, these findings suggest that this reimbursement issue can undermine GPs’ image as physicians recognised to manage dementia.
A theme unique to this study was that the patients with advanced dementia were no longer followed up by the specialists. General practitioners along with primary care nurses were, after all, the only health professionals making home visits to patients with advanced dementia. Nonetheless, the triangulation of data from carers and GPs suggested that the care they provided was mostly related to intercurrent problems (e.g. respiratory infection) and overall dependence, than to dementia itself. These findings might suggest that care needs in advanced dementia would be similar to those of palliative care, where these health professionals may have more training. Surprisingly, none of the participants reported any involvement of primary care nurses in caring for people and families living with dementia other than in advanced dementia and diabetes management.
This study findings suggest that a long-standing doctor–patient relationship enabled person-centred approaches from both patients’ and GPs’ perspectives. These findings extended those of previous research that an established doctor–patient relationship may facilitate the recognition of dementia (Adams et al., 2005; Pentzek et al., 2019). On the other hand, the dementia process can negatively affect the relationship, impairing communication and the establishment of trusting relationships, which could result from lack of training in communicating with persons with dementia, identified as a barrier in previous studies (Aminzadeh et al., 2012; Mansfield et al., 2018). Moreover, the presence of carers in consultations was reported by only a few GPs as a limitation to a person-centred approach, despite their lack of emphasis on trying to ensure more privacy by interviewing the patient alone.
Being registered with the same GP as the person with dementia made support for carers easier to provide. This was consistent with a previous study that found that having both carer and patient registered in the same practice would facilitate looking after carers (Parmar et al., 2020). In Portugal, GPs are accountable for the whole family, which facilitate a comprehensive approach to patients and their carers, and brief and simple family interventions (Gonçalves-Pereira, 2017). Despite their privileged position, the support provided by the GPs seemed to be mostly relational (i.e. emotional) rather than a formal psychoeducational approach. A theme unique to this study was carers being the primary concern of those GPs who held nihilistic views of dementia. This attitude poses potential ethical conflicts regarding the best interests of patients.
A consensus among participants was that GPs played a crucial role in managing chronic conditions. A particular example was diabetes. This may contradict previous suggestions that these patients may receive lower levels of diabetes care when compared with those without dementia (Connolly et al., 2013); however, the quality of diabetes follow up was not specifically assessed in the present study.
Importantly, this study findings seem to suggest that some comorbidities related to ageing and dementia were overlooked. While none of the GPs mentioned assessing their patients for frailty, recent studies found frailty to be highly prevalent in older patients with dementia in the community, contributing to NPS and carer burden (Sugimoto et al., 2018).
Strengths and limitations
This qualitative study encouraged interviewees to fully express their views on the complex topic of dementia care. The codebook was carefully constructed to optimise the precision of definitions and clarity of themes. The triangulation of data enhanced the validity of findings. Additionally, to understand the current role of GPs in dementia care, it is important to capture the views of both patients and carers (Nolan et al., 2002). The quality framework that guided the interviews was evidence-based and encompassed suggestions from carers and GPs. Its wide scope (e.g. multimorbidity assessment) ensured relevance to primary care contexts. Suggestions from persons with dementia should have been considered, but recruitment constraints applied.
There were other limitations. The study sample was small, so results are not necessarily transferable to other settings; however, primary care users were from different social settings. Purposive sampling may have introduced bias (e.g. patients nominated by their GPs may have better doctor–patient relationships). It is also possible that patients’ and carers’ discussions about their own GPs were influenced by the interviewers also being GPs, albeit not from their primary care practice. To address this potential interviewer bias, the interviewees’ anonymity was assured during the interviews, and a teamwork approach was used (Barry et al., 1999). Furthermore, all interviews were conducted in the participants’ own homes. Similarly, GPs interviewed by a fellow GP may have been prone to social desirability bias. However, GP researchers have been shown to gain richer data than non-clinicians when interviewing their fellow GPs (Chew-Graham et al., 2002). To address this issue, a teamwork approach was used when analysing and interpreting the data (Barry et al., 1999).
Implications for practice and research
Understanding the experiences of GPs, persons with dementia and their carers may help to plan a realistic role for primary care teams in dementia care. The study findings, particularly the themes not previously reported (e.g. the case of advanced dementia), have implications for clinical practice. For example picking up the work with people with advanced dementia who are no longer seeing specialists could be the first step in shifting dementia care into general practice. To expand these study findings, future research should focus on the content of GPs’ consultations in dementia and on the characteristics of primary care teams and how they impact GPs’ contribution to dementia care.
Conclusion
The findings of this study strongly suggest that primary care may not yet be prepared to comply with the national dementia strategy published in 2018. Future work will explore the barriers to dementia care from the perspective of users and primary care teams.
Footnotes
Acknowledgements
We thank Maria J. Marques for valuable comments on data analysis.
We thank the persons with dementia, their carers and the general practitioners who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was granted by the ARSLVT Research Ethics Committee n° 067/CES/INV/2017 and NOVA Medical School Ethics Committee n° 28/2017CEFCM, and written informed consent was obtained from each participant. Only individuals with dementia who were able to consent to participate were included as direct participants.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.