
Abstract
Reminiscence therapy has the potential to improve quality of life for people with dementia. In recent years reminiscence groups have extended to include family members, but carers’ experience of attending joint sessions is undocumented. This qualitative study explored the experience of 18 family carers attending ‘Remembering Yesterday Caring Today’ groups. Semi-structured interviews were transcribed and subjected to thematic analysis. Five themes were identified: experiencing carer support; shared experience; expectations (met and unmet), carer perspectives of the person with dementia’s experience; and learning and comparing. Family carers’ experiences varied, with some experiencing the intervention as entirely positive whereas others had more mixed feelings. Negative aspects included the lack of respite from their relative, the lack of emphasis on their own needs, and experiencing additional stress and guilt through not being able to implement newly acquired skills. These findings may explain the failure of a recent trial of joint reminiscence groups to replicate previous findings of positive benefit. More targeted research within subgroups of carers is required to justify the continued use of joint reminiscence groups in dementia care.
Introduction
In 2012, an estimated 670,000 people in the UK acted as primary carers for people with dementia (Alzheimer’s Society, 2012). Caring for someone with dementia is associated with high levels of anxiety and depression (Cooper, Balamurali, & Livingston, 2007), lack of personal time and opportunities to socialise (Croog, Burleson, Sudilovsky, & Baume, 2006) and greater levels of strain and distress than carers of other older people (Moise, Schwarzinger, & Um, 2004). Whilst the vital role of carers has been acknowledged by the NICE-SCIE guidelines (2006), carer-reported quality of life is still varied (Alzheimer’s Society, 2012). Over half (52%) carers report they do not receive sufficient support to enable them to carry out their caring role (Alzheimer’s Society, 2011). The National Dementia Strategy (NDS) in England acknowledged that ‘family carers are the most important resource available for people with dementia’ (Department of Health, 2009, p. 49) and recommended the development of peer support networks for people with dementia and carers (objective 5). However, it is not yet clear which model(s) of peer working should be adopted (DoH, 2009, p. 42), nor whether psychosocial interventions are most effective when person-centred or relationship-focussed.
Psychosocial interventions
Meta-analyses of carer-focussed interventions demonstrate small to moderate effects upon psychological morbidity and caregiver knowledge (Brodaty, Green, & Koschera, 2003), burden, depression, knowledge, and subjective well-being (Pinquart & Sorensen, 2006), and recommended interventions include psycho-education, skills-training, and multi-component programmes (Gallagher-Thompson & Coon, 2007; Olazaran et al, 2010).
Brodaty, Green, and Koschera (2003) suggested that the only significant feature of interventions which improved carer well-being and burden was the involvement of the person with dementia and their families. Subsequently, there has been a move to develop more relationship-centred interventions. Promoting a positive relationship may prevent the breakdown of the dyad relationship and thus reduce the likelihood of the person with dementia being placed in alternative care (Brodaty et al., 2003). A review of programmes involving patients and family members concluded that it was beneficial to involve family members in interventions for people with dementia (Martire et al., 2004), but a more recent review concluded that programmes for dyads may improve some, but not all, aspects of functioning for the carer and person with dementia (Smits et al., 2007).
Reminiscence therapy
Reminiscence therapy has been popular and widely used across Europe for a number of years, promoting communication and well-being for people with dementia through stimulating earlier memories which are often intact. This encourages social inclusion, increased levels of well-being, pleasure and cognitive stimulation (Woods, Spector, Jones, Orrell, & Davies, 2005). More recently, reminiscence programmes such as the ‘Remembering Yesterday Caring Today’ (RYCT) group programme (Schweitzer & Bruce, 2008) have included carers alongside the person with dementia following evidence to suggest that this joint approach leads to a reduction in carer stress (Thorgrimsen, Schweitzer, & Orrell, 2002; Woods et al., 2005). However, a recent large scale randomised controlled trial of RYCT compared to treatment as usual showed increased carer anxiety symptoms, plus levels of caregiving stress increased with the number of sessions attended (Woods et al., 2012).
Woods et al. (2012) highlighted the need for systematically recorded information on the experiences of those participating in reminiscence programmes, as well as those who did not participate or dropped out, in order to clarify the unexpected findings of their study. To date there has been no qualitative research regarding peoples’ experience of attending reminiscence groups. Therefore, an evaluation of the RYCT approach through in-depth semi-structured interviews would ‘fill in gaps’ not explored by existing quantitative measures and will also contribute to the emerging literature on dyadic interventions.
Method
Design
The study design was a qualitative inquiry using in-depth, semi-structured interviews and thematic analysis. This method was selected to allow exploration of carers’ own experiences of attending the RYCT intervention. The RYCT intervention (Schweitzer & Bruce, 2008) was delivered as part of a larger randomised controlled trial, the SHIELD (Support at Home: Interventions to Enhance Life in Dementia) Carer Supporter Programme (Charlesworth et al., 2011).
The ‘Remembering Yesterday, Caring Today’ programme
The RYCT intervention is a structured psychosocial intervention for individuals with dementia and their family carers over 10 months (12 weekly sessions followed by seven monthly sessions). Each session lasts 2 h and follows a programme of topics intended to allow reminiscence over the life-course (e.g. schooldays, going out, working-life). Groups are held in community settings and transport is arranged for those people who had difficulties travelling independently. A trained team (including NHS or voluntary organisation staff, volunteers and carer supporters) attended per dyad so that all participants have the necessary support and guidance throughout. In the SHIELD programme, groups ranged in size from 4 to 15 dyads. Four of the weekly sessions included a group for family carers away from the individuals with dementia. The first two carer groups focused on ‘communication’, whilst the second two had a focus on ‘reminiscence at home’. However, carers were often keen to use the time to share information and caring experiences.
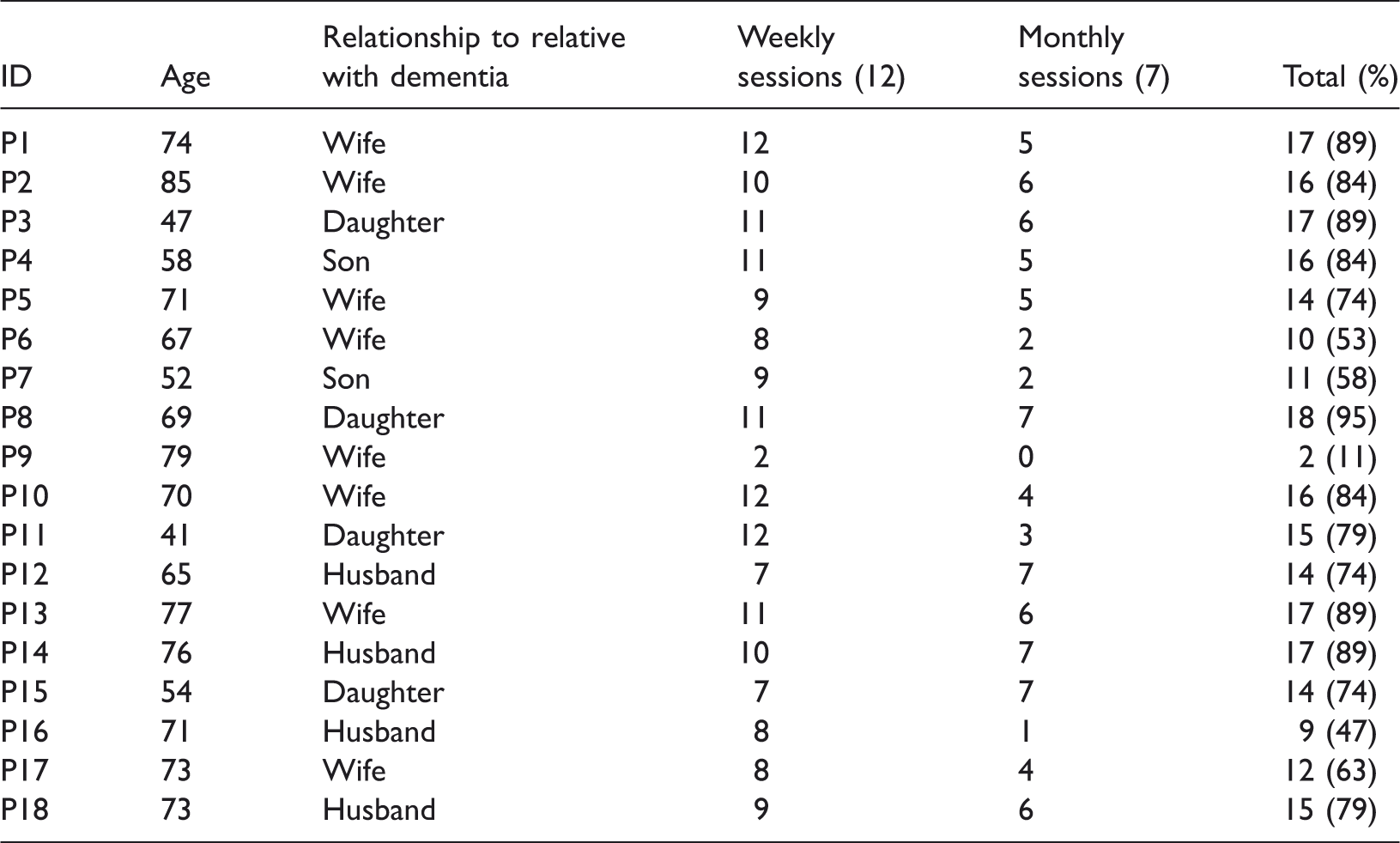
Participants
Social and demographic characteristics and RYCT attendance of the carers in the sample
Ethical issues
Participants were contacted in August 2012 following ethical approval from the University of East Anglia Health Ethics Committee (2011/2012-61). Potential participants were sent an information sheet detailing the study aims and procedures along with a consent form. Those who verbally agreed to take part met with a member of the research team (NM, NC or ED) and the study discussed with them. Written consent was sought from participants prior to being interviewed. All participants who were approached for interview gave their consent, including consent for audio recording.
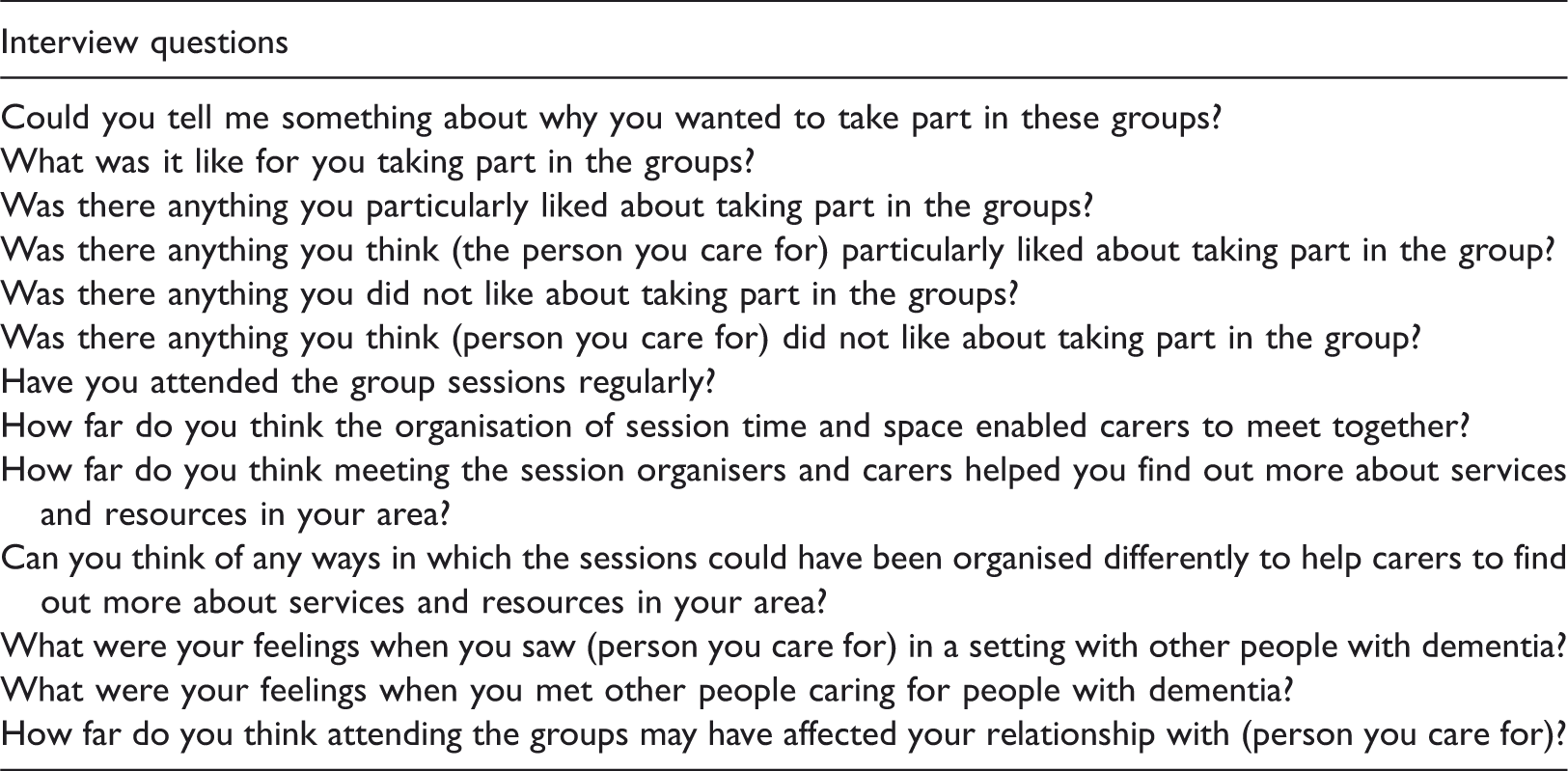
Semi-structured interviews
Semi-structured interview topic guide for family carers
Data analysis
Interviews were transcribed verbatim from digital recording, all personal identifiers removed to preserve anonymity and given a personal identifier number (e.g. P1, P2). All researchers read the transcripts for the interviews they carried out and listened to the digital recording to confirm reliability of the transcripts. The qualitative research software programme NVivo (Version 10) was used to support coding, management, and analysis of data to enhance rigour (Richards & Richards, 1991).
An inductive (bottom-up) thematic analysis was used as a systematic method of identifying themes or patterns within the data (Braun & Clark, 2006). An initial coding framework was developed by researchers (NM and NC) who independently identified words and phrases which described the experience of family carers attending the RYCT sessions. These pieces of text were condensed into codes such as ‘learning from other carers’ and ‘spending time with similar people’. Reliability of the codes was ensured through discussion between all researchers (NM, NC and ED) and subsequently applied to the remaining transcripts and continuously reviewed during this process to include new emergent issues in a modified analytic induction process (Murphy, Dingwall, Greatbach, Parker, & Watson, 1998).
Researchers independently coded the remaining data and met periodically with a member of the team not involved in the interviewing process to discuss codes and themes to ensure reliability (researcher triangulation). Disagreements between researchers were resolved through discussion with each other after completing their independent coding. The process of modified analytic induction reviewed negative or deviant cases which enabled the researchers to refine theoretical statements. The reviewers met to compare analyses, and a consensus on the content and explanation of each theme was reached.
Participant validation
Participants were sent a summary of themes following the data analysis stage of research and contacted via telephone to arrange a date for discussions of the findings. Lincoln and Guba (1985) suggest that participant validation is a crucial technique for establishing and enhancing the credibility of research findings. In order to obtain meaningful feedback, the researcher ensured that the analysis was written in accessible language and that further explanation was given to participants if required, as highlighted by Langdridge (2007). For these reasons, the summary was succinct and simple in terminology and participants were encouraged to ask questions if there were any details that they did not understand. Discussions were generated around whether the summary represented a good reflection of participants’ views and the themes which they could relate to the most. Where appropriate, participants were also asked if they could offer reasons for particular patterns observed by the researcher and whether they felt that they would like add any further accounts or comments.
Comments from carers involved in the validation exercise showed strong agreement with the findings of this study. Carers generally felt that the themes and subthemes matched their experiences and that they were able to relate to some of the findings under each theme. One carer disagreed with the negative aspects identified by other carers and was full of praise regarding the RYCT intervention. However, other participants were able to relate to one or two of the negative aspects, e.g. their embarrassment at some behaviours displayed by their relative, but overall had a positive experience of attending the groups.
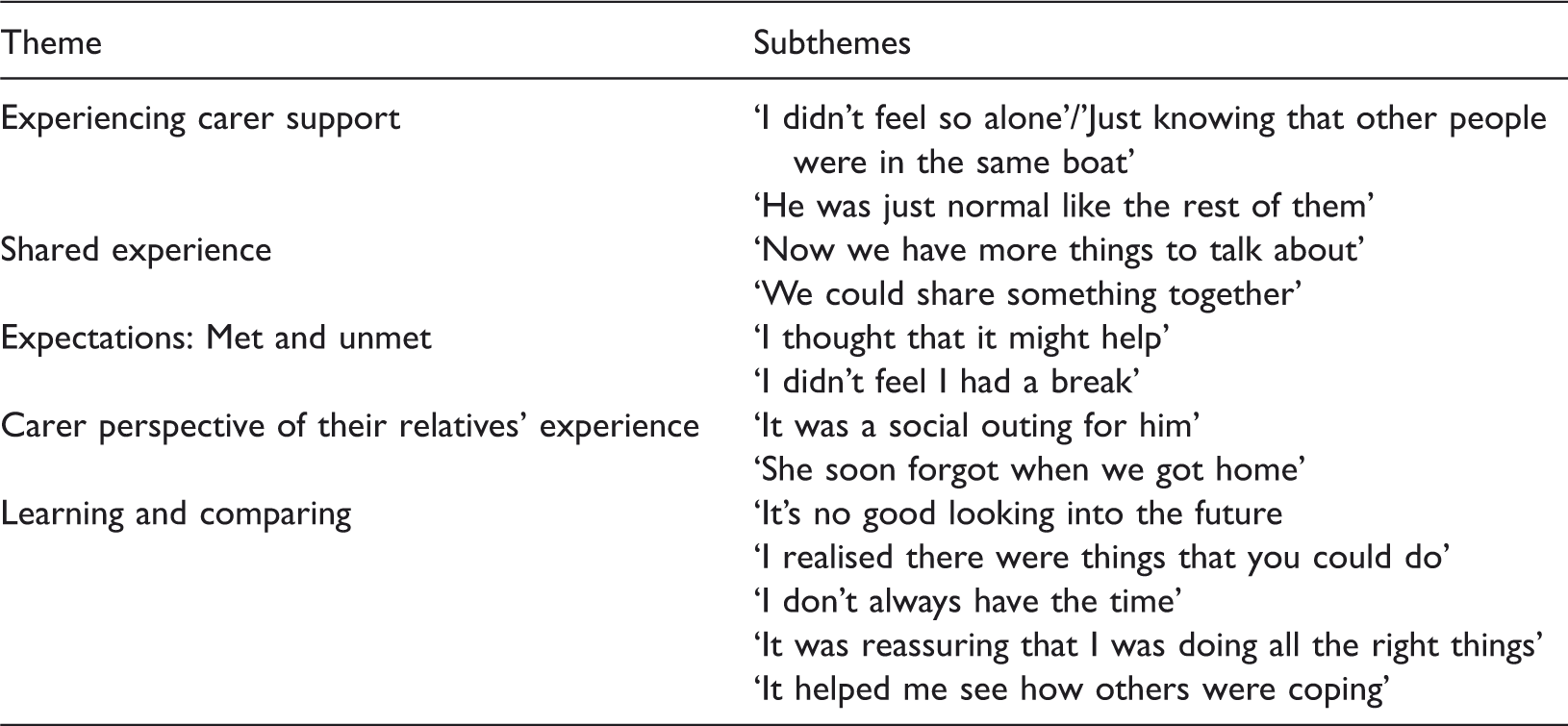
Results
Themes and subthemes from the thematic analysis
Expectations – met and unmet
‘I thought that it might help’
Expectations discussed by carers included meeting others in similar situations, developing a wider support network and learning new ways to cope with their relative. I wanted to meet other people who have got the same problem as L …, just to have an idea and see how they deal with their relatives for ideas that would be useful to me. (P10: 70, wife)
‘I didn’t feel I had a break’
Whilst attending together was seen by some carers as a positive aspect to the group, others found that the joint sessions increased feelings of burden and strain. I still had to get J … dressed, take him there, bring him back. It took a long time to prepare and get ready to go out … I didn’t feel I had a break … I resented the fact that it had to be with J … and not just with others. (P6: 67, wife) Ideally, I would have liked a lot more time allocated for the carers’ sessions. It felt quite rushed so even if you had questions to ask, those who were more articulate could use up the time. (P6: 67, wife)
Experiencing carer support
‘I didn’t feel so alone’/‘Just knowing that other people were in the same boat’
The RYCT group provided an important avenue through which carers could build supportive relationships with other carers. This was considered especially important for carers who reported feelings of isolation, identifying that meeting other carers reduced feelings of loneliness. For one carer, communication with group members substituted the decline in communication within her relationship. I was with adults that talked intelligently and that, to me, was my biggest bonus … that was my biggest gain, because that’s what I miss most of all. (P2: 74, wife). You don’t feel quite so isolated. When you talk to other people, it helps. I don’t have close family back-up. I also found some of the things that mum does, other people spoke of as well. (P8: 69, daughter).
‘He was just normal like the rest of them’
Carers revealed their embarrassment at some behaviours displayed by their relative. Being with RYCT team members and other carers who had similar experiences provided a space where such behaviours were considered ‘normal’ and did not draw unwanted attention and allowed carers to relax. When I take him out I have to explain that he’s got dementia because he does silly things, which I do find a bit embarrassing, sometimes. It was good in the group not to have to keep apologising for him … because people do give you that look, sometimes, if they don’t understand. (P5: 71, wife).
Shared experience
‘Now we have more things to talk about’
Identifying topics of conversation with their relative was reported as challenging by carers, leading to reduced levels of carer confidence. Attending the sessions provided an important shared experience which carers could use to create ‘fresh’ discussions. Carers were able to provide prompts during discussions in order to stimulate memories of sessions. Through reminiscing, some carers learnt new information about their relatives’ lives; this also promoted new areas of conversation. I enjoyed the bits that we did together, because I was then able to talk to K … afterwards, knowing what he’d done and we could recap, so that was good. (P13: 77, wife) It’s nice talking about old times, about his school days and working days – things you forget but they remind you of what your life used to be like. (P5: 71, wife)
‘We could share something together’
Attending the groups with their relative was generally a positive experience for carers. This time spent together was described as ‘quality time’, as outside the sessions carers tended to focus on more practical day-to-day tasks with their relative. I got something out of it in that I spent quality time with her. When I visit her at home, I’m perhaps doing other things, like the washing or housework, so it’s not necessarily quality time with her, so that was good. (P3: 47, daughter) It was also an important advantage to meet so many people – the social contact, which J … and I lack, because of time and he is a very private, shy person, he doesn’t want to go out and meet people. I think he was very apprehensive, he doesn’t like groups and he’s become increasingly difficult in meeting groups … this was quite nice because the atmosphere was very friendly, very welcoming. J … enjoyed it and I liked what I saw and the people I saw. (P6: 67, wife) I liked that we were able to do things together, participating in the different activities together. I realised that there were things you could do to make yourself helpful and to relieve the stress and that you could play games. My L … likes dominoes and I couldn’t play dominoes but I realised that with a little patience I would be able to play with him. (P10: 70, wife)
Carer perspective of relative’s experience
‘It was a social outing for him’
Carers reported that their relative would ‘come alive’ at the groups, becoming more animated and engage in novel activities. One carer identified that within the home they were unable to engage their relative in the same activities as within the groups, leading to feelings of frustration. He enjoyed the cake-making as a social event. He enjoyed the novelty of doing things together there. He participated in almost every event and that doesn’t happen normally, at home … It was a social outing for him. He would dress up and get ready, but I can’t get him to do that normally on an everyday basis. (P6: 67, wife)
‘She soon forgot when we got home’
Reported benefits for the people with dementia included improvements in mood, confidence, and memory, however these were generally not maintained. Carers reported that their relatives appeared ‘brighter’ and ‘happier’ following the sessions but any benefits soon disappeared. Things were remembered, but it wasn’t a long-term thing. It was soon forgotten. No lasting impact. (P14: 76, husband) Well, we thought it would probably revive old memories and stimulate activity, but I think the progression has been too much and it hasn’t worked as well as I would have liked to have done … Things were remembered, but it wasn’t a long-term thing. It was soon forgotten. No lasting impact. It may have done right at the beginning, but these things aren’t diagnosed as early as they should be. If you can catch somebody early enough, it would be very beneficial for this type of activity. (P14: 76, husband)
Learning and comparing
‘It’s no good looking into the future’
Observing people perceived as having more advanced dementia was described as a positive experience for many carers, viewing this as ‘preparation’ for what may happen in the future. It was a learning process and I could see how J … might progress into and that’s important to know, without it hitting home suddenly. The gradual process is important and even if he was more advanced it’s still very good to know where he might be eventually. We don’t usually get that opportunity in life. (P6: 67, wife) I personally don’t gain benefit from talking with others who have more severe problems, for whatever reason and whatever stage – aggression, violence or anything like that. I know it does occur but I don’t want to hear about it because I’d rather deal with the situation that exists, not one that might exist. (P18: 73, husband).
‘I realised there were things that you could do’
Learning about new coping strategies led some carers to change their behaviour, creating more ‘positive periods of time’ together, including engaging their relative in activities such as dominoes, cooking and creating memory boxes. I found it helpful to discover an activity I could share with L … Rather than just sitting looking at each other we could share something together. Another thing I found helpful is the writing down things, like daily activities, because I wasn’t writing things down. I was given a pad to write on. (P10: 70, wife). I can leave him, even to go up to the corner shop and know that he will be alright. I wasn’t able to do that before going to the groups. I now don’t worry so much and can relax a bit. (P10: 70, wife). Now, I don’t give him orders – I just say it in a couple of words. I don’t give him a long sentence because he won’t remember what he’s doing and he’ll get more flustered. If I raise my voice he gets flustered. When you’ve said something five times, your voice does get a bit higher, but I try not to do that now because I can see it in his face. (P5: 71, wife)
‘I don’t always have the time’
Due to the additional demands on carers’ time including having young families and being in employment, some carers found they were unable to implement the new tools and techniques learnt in the group, leading to feelings of guilt. It was felt that the techniques would be of benefit to their relative if they could put into practice what they had learnt. I think it’s had a negative impact on my confidence because I felt there is so much I can do with him but I’m not doing it. There is that push to do it for him but there wasn’t anything for me. There’s a lot more I could do for J … but it means spending a lot more time with him and I am doing things for him 24/7 already. (P6: 67, wife) I know that T … goes to a day centre five days a week and J … does cooking. My cooking skills have gone by the board but I felt I should make more of an effort. I haven’t done it. (P2: 85, wife).
‘It helped me to see how others were coping’
Observing other carers in the group display negative emotion towards their respective relatives allowed carers to reappraise their own negative feelings. Carers reported experiencing feelings of ‘irritation’ and ‘frustration’, however seeing other carers with similar feelings relieved some of their guilt at experiencing these feelings. It was good to see one or two others show their exasperation. I suppose I was castigating myself for not having the patience and looked upon it as letting him down. (P2: 85, wife). We’re in control of his happiness, in a sense, as much as you can be. Seeing other people doing it as well hammers it home that you can do it. You don’t have to put them in a home, at this stage, anyway. But you can never say never – it depends how it goes. (P4: 58, son). When I heard all the other stories of the other participants and saw what they were coping with, which were already diagnosed memory losses, I didn’t know where J … was in this picture and sometimes I wondered whether he should be there or not. (P6: 67, wife)
‘It was reassuring that I was doing all the right things’
Hearing about coping strategies from other carers and group facilitators enabled carers to feel reassured that they had the tools to cope with future situations, improving confidence in their own coping abilities. Additionally, carers were given reassurance that they were coping appropriately. It was reassuring that I was doing all the right things, as well – the practical things at home. So it was reassuring so I suppose, yes; but there are times when I feel absolutely inept. (P13: 77, wife). It gave us the time to talk about any problems we had and to talk with others and found out how they managed; their coping strategies and how they felt about how things were going with their people. (P8: 69, daughter). I don’t get a lot of positive feedback from my sister and my brother does not get involved at all, so I decided to do it anyway. So, it gave me the confidence to think I am approaching it the right way. (P3: 47, daughter).
Discussion
This is the first study that has used qualitative methodology to explore the experiences of carers attending a joint reminiscence group for people with dementia and their carers’. It demonstrates the value placed on peer support by family carers but also highlights some of the potential risks of introducing new skills and techniques to carers in the absence of support to implement those techniques.
Social context of carers
An important over-arching theme to emerge was the social function of the group for carers. When people with dementia have difficulties participating in social interactions, carers may therefore experience a reduced social network resulting from stigma or lack of opportunities to socialise (Croog et al., 2006). The group provided ‘bridging’ relationships which allowed carers to feel less isolated and provided reassurance through social comparison and interaction with other carers.
Carers identified the importance of attending the group together with their relative, describing this as providing more things to talk about and enjoying having a shared activity. Whilst this joint experience was beneficial to both adult-child and spousal carers, the experience appeared to be especially valued by spousal carers. Dementia can lead to changes in relationship between the carer and care recipient (Noyes et al., 2009) and a loss of activities undertaken as a couple (Elvish, Cawley, & Keady, 2013). Hellstrom, Nolan, and Lundh (2007) suggest that one aspect of living positively with a spouse with dementia may be a focus on ‘sustaining couple-hood’ which concentrates on maintaining shared activities. Spousal carers may look to retain their identity as a wife or husband through preserving the identity of their partners and themselves as a couple (Perry & O’Connor, 2002). Maintaining social roles as a couple may therefore act as a coping strategy for spousal carers, acting as a buffer against the challenges faced.
Carers also highlighted the value of comparisons to other carers. Seeing others coping well with their caring situation provided reassurance to some carers, whilst downward social comparison with those worse off also made people feel better about their own situation. On the other hand, seeing others with similar conditions created a sense of sadness for some carers, which has been shown to lead to disengagement from such social contact to protect themselves from witnessing situations which they may possibly face in the future (Locock & Brown, 2010). Obtaining guidance through comparisons with similar others helps people assess the appropriateness of their own attitudes, beliefs, and behaviours against standards of the other group members (Marsden & Friedkin, 1994). Such feelings are likely to fluctuate over the caring duration and should be considered by health professionals when considering possible interventions.
Expectations of carers
In some instances, carers’ expectations of the group were not met (e.g. not having enough ‘carer only’ time) which led to feelings of frustration and additional stress. Expectations may have related to carer needs that in turn may be related to motivations to care. Eisdorfer (1991) identified several motivations to care: a sense of love or reciprocity, spiritual fulfilment, a sense of duty, guilt, or social pressures. Spousal carers may have more intrinsic motivation which may reduce their psychological distress as compared to the more extrinsic motivation of many adult children who may feel obligation and duty to provide care for their parent (Pinquart & Sorenson, 2011). Some carers do not even define themselves as a carer; instead, they view their actions as a natural extension of their relationship (Elvish et al., 2013). Spousal carers who may face physical health problems and lack of opportunities to socialise may benefit from the social aspect and value the opportunity to socialise together, whilst the adult–child carers may benefit from the more educational and skill building aspects. Those carers who saw the groups as being of potential benefit to the person with dementia, appeared disappointed that positive effects – on mood, memory, and confidence – were short-lived, in some cases being specific to the group meeting.
Learning new skills: Reduction of, or addition to, carer stress?
The group enabled carers to acquire new skills and be reassured that they had the ‘tools’ to cope with future situations which may arise within their caring role. Carers who reported having little support from their family network especially reported feelings of reassurance and benefit from learning skills. This reassurance may develop though improving carer’s self-efficacy within their caring role. Exploring carers’ self-efficacy may also be important in determining who may benefit most from interventions (Biegel & Schulz, 1999).
However, some carers reported difficulties in utilising the skills that they had learnt within the group and subsequently experienced some feelings of guilt. Many working age carers have conflicting responsibilities, such as their careers, young children, or adolescents who require support and attention and experience role conflicts, increasing their risk for role overload (Barber & Pasley, 1995). By providing carers with information and advice on how to support their relative, carers may develop the belief that they ‘must’ take on the role of informal carer. If they are unable to implement the tools they have been given then carers may experience self-critical thoughts about themselves and their abilities to care affectively. This aspect may go some way to explain why carers in the original study showed an increase in levels of anxiety following their RYCT (Woods et al., 2012).
Positive and negative effects of joint reminiscence groups
The beneficial effects of the groups were largely centred around the sense of support from the group, feeling less isolated and alone, and the opportunities to learn new ways of coping or simply to be reassured that they were doing the right things already. Additional benefits came from a shared experience with the person with dementia and having more things to talk about. The negative aspects included the lack of a break from the person with dementia, and the lack of emphasis on the carers’ own needs, with the separate time for carers not being seen as sufficient by some. Seeing the person come alive in the group meeting, but not being able to maintain this change subsequently was difficult for some carers. Seeing people with dementia who exhibited more marked impairments than their own relative was appraised as an opportunity for learning by some carers, but to others it was experienced as an unwelcome vision of the future. Similarly, as mentioned above, seeing new ways of coping that cannot then be implemented may be an additional stress for some carers.
Strengths and limitations
Whilst there is a relatively small sample size, its diversity of social backgrounds, relationships, duration of engagement with the reminiscence group, covered wide variations in the experiences of family carers. The sample size clearly does not permit generalisation to other carers however the topic guide for the data collection facilitated the emergence of individual experiences and gave carers space to share their story which allowed for a rich amount of data to be gathered. The data-led analysis, researcher, and participant validation also increased validity of the results, however validation was only carried out with a proportion of participants rather than the whole sample (6 out of 18).
Implications
Service provision
The results from this study could have implications in terms of service development and provision. Firstly, carer outcome and experience of reminiscence appears to vary depending on the direction of caring relationship. In line with Pinquart & Sorenson (2011), spouses and adult children carers may have different needs and may struggle with different issues. As a result, spouses may benefit most from a reduction of carer demands (e.g. respite), whereas children may gain most from family-focused interventions targeted at strengthening the relationship with the care recipient. Carer expectations may be more carefully managed before engaging in such an activity to ensure that expectations of the group are realistic and in line with the aims of the group, for example, limited time apart from their relative. Different subgroups of carers may need more tailed interventions. Adult–child caregivers may be less likely to relate to spousal carers and find more meaningful comparisons to those in a similar caring situation.
Secondly, in order to consider the difficulties for some carers in the implementation of skills learnt in the group, psychosocial groups may usefully complement the skills training with a more comprehensive and individualised model of support (Kurz, Wagenpfeil, Hallever, Schneider-Schelte, & Jansen, 2010). This would not only include the acquisition of new skills but also the systematic transfer of newly acquired skills into the everyday context, and active expansion of the caring network. This would hopefully combat some of the guilt that carers identified when they were unable to utilise skills learnt in the group. This may be supported by combining group and individual formats of treatment delivery and by targeting specific caregiver subgroups such as spouses or children.
Finally, expectations which carers place on themselves in terms of their care-giving role should be explored further. Services that view family carers as being an extension to the professional caring team have been criticised (Henderson & Forbat, 2002; Nolan, Ingram, & Watson, 2002) for polarising the roles of carer and cared for, with little consideration of the nature of the relationship. Health professionals should be aware of the assumptions they make around the role of family members in caring for people with dementia, especially taking into account cultural and social expectations including the role of adult–children and spouses as this may guide more appropriate referrals to interventions. Vernooij-Dassen, Draskovic, McCleery, and Downs (2011) found that cognitive reframing; including challenging carers’ beliefs about their responsibilities to their relative has the potential to relieve feelings of anxiety, depression and stress.
Research
Whilst studies have acknowledged that attention needs to be paid to different subgroups of people with dementia in targeting effective psychosocial interventions (e.g. Smits et al., 2007), few have emphasised the need for consideration of subgroups of carers. In order to support carers effectively and efficiently, research should investigate the benefits of certain interventions for particular subgroups of carers.
Furthermore, to enhance reminiscence work with carers and their relatives, consideration should be made to the specific type of reminiscence work undertaken. There is increasing interest in life review therapy and the development of life story books with an emphasis on an individual’s memories, rather than on reminiscing in a group context. A review by Subramaniam and Woods (2012) of individual reminiscence work found that where studies included life review therapy there were immediate and longer-term psychosocial benefits to people with dementia compared to work that was less personalised and memory triggers were less specifically relevant to the individual. In terms of carers learning about their relative and spending time together, the more personalised life-review process may have greater impact for carers then a less personalised approach. This then misses out on the potential benefits of a supportive network of other carers and of learning from and comparing with their experiences.
This study has used a heterogeneous group of carers which means that it is difficult to identify benefits for particular subgroups of carers (Zarit & Toseland, 1989). Research would benefit from carrying out similar studies targeting particular groups of carers to explore whether this improves outcomes, both quantitatively and qualitatively through comparison to similar or non-similar others.
Conclusion
Joint reminiscence groups have the potential to provide a valuable model of peer support, however, care is required to manage participant expectations of the group and of themselves in their caring role. Increasing our knowledge in this area will help health professionals to refer carers to more suitable interventions which will hopefully increase effectiveness in supporting them within their caring role. Due to the recent trial of joint reminiscence groups failing to support previously positive findings, there is a need for more specific, targeted research within subgroups of carers. More systematic qualitative research into the experience of carers’ involvement in such joint interventions could illustrate the impact of reminiscence therapy and clarify the basis for its continued use in dementia care.
Footnotes
Acknowledgements
We would like to thank the participants for their time and contributions, and acknowledge the administrative support provided by Joan North.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CSP-RYCT project is part of the Support at Home: Interventions to Enhance Life in Dementia (SHIELD) programme funded through a grant held by North East London NHS Foundation Trust (NELFT) from the NIHR Programme Grants for Applied Research (RP-PG-060-1083). Professor Martin Orrell (UCL) is the Chief Investigator for SHIELD, with the other grantholders being Professors Woods (Bangor), Challis (Manchester), Moniz-Cook (Hull), Russell (Swansea), Knapp (LSE and KCL), and Dr Charlesworth (UCL). This paper presents independent research; the views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.