
Abstract
Aim
Reminiscence therapy is a popular therapeutic intervention for people with dementia. This review set out to provide a better understanding of reminiscence therapy through a deeper analysis of its contents and delivery.
Method
This review examined 22 studies from the most recent Cochrane review (Woods, B., O’Philbin, L., Farrell, E. M., Spector, A. E., & Orrell, M. (2018). Reminiscence therapy for dementia. Cochrane Database of Systematic Reviews,
Findings
Thirteen reminiscence therapy components were identified. ‘Memory triggers’ and ‘themes’ were identified as the most common but were found not to be consistently beneficial. Reminiscence therapy was typically delivered in a care setting using a group approach; however, there was no consistency in session composition, intervention duration, as well as the training and supervision provided to facilitators. Operationalisation of theory within reminiscence therapy was not identified. Reminiscence therapy was not consistently delivered according to a programme/model. Lastly, as a result of a small number of studies, the components ‘life stages’, ‘activities’ and ‘family-only sessions’, showed beneficial promise. In summary, this review highlights that reminiscence therapy needs more consistency in content and delivery, in addition to a clear theoretical framework.
Introduction
Dementia
Dementia is an umbrella term for a group of chronic, progressive, terminal neurodegenerative brain disorders (McEwan & McCrory, 2015). Alzheimer’s disease (AD) is recognised as the most common (62%) (Alzheimer’s Society, 2014). Dementia is characterised by a decline in cognitive functioning, impairment of activities of daily living and behavioural changes (BMJ Best Practice, 2018). It is estimated that globally 50 million people have a diagnosis of dementia (World Health Organization, 2017), with higher prevalence rates in females (61%) compared to males (39%) (Alzheimer’s Research UK, 2015). With an increasing life expectancy and no dementia cure, it is estimated that the number of people living with dementia, worldwide, will increase by 204% to 152 million by 2050 (World Health Organization, 2017), with an estimated global societal economic cost of a trillion dollars (Prince et al., 2015). For the purpose of this review, dementia was defined in accordance with the most recent Cochrane Review by Woods et al. (2018). That is ‘a formal diagnosis according to the diagnostic and statistical manual of mental disorder – fourth edition (DSM-IV)’. In the Cochrane review (Woods et al., 2018) the main diagnostic categories included were vascular dementia (VD) and AD.
Quality of life
Within the United Kingdom, living well with dementia is a policy and procedural level priority (Department of Health, 2009). However the concept of ‘living well’ is ambiguous as it means different things to different people. It is suggested to be best equated with ‘experiencing a good quality of life (QoL)’ (Martyr et al., 2018; Small, 2007). However, like the concept of ‘living well’, QoL is also a complex and multilayered concept. The world health organisation conceptualised it in terms of one’s ‘physical health, psychological state, level of independence, social relationships and their relationship to salient features of the environment’ (World Health Organization, 1995, p. 1).
People with dementia have the same basic (physiological and safety needs) and psychological needs (love, belongingness and esteem needs) (Maslow, 1943) as those without dementia. Despite cognitive and functional changes occurring during the dementia disease trajectory, people with dementia can, and should, experience enjoyment and satisfaction in daily life (Hoe et al., 2009; Selwood et al., 2005). However, it is estimated that up to 90% of people with dementia will experience behavioural and psychological difficulties, which are frequently mistaken for dementia-related symptoms rather than symptoms of human distress, misperception and disorientation (The British Psychological Society, 2013). The psychological and behavioural symptoms of dementia extend far beyond the individual with dementia (Bidewell & Chang, 2011). The progressive nature of dementia involuntarily transforms the essence of a relationship into one that is generally care-driven and characterised by unidirectional interactions (Pearlin et al., 1990). Consequently, emphasis needs to be placed on supporting people with dementia, as well as family caregivers and care staff to establish new meaningful ways for connectedness.
The National Institute for Health and Care Excellence (2018) recommends that therapies for people with dementia must be tailored to the person’s needs and preferences. It recommends three interventions to promote the ‘cognition, independence and well-being’ of people with dementia (NG97): (1) Cognitive rehabilitation to support functional ability in people with mild to moderate dementia. (2) Cognitive stimulation therapy for people with mild to moderate dementia. (3) Group reminiscence therapy for people with mild to moderate dementia. This review will focus specifically on reminiscence therapy.
Reminiscence therapy
Reminiscence therapy is a strengths-based approach that can provide person-centred care as it draws upon past memories from people’s lives, memories which are considered to be often preserved in dementia (Woods et al., 2016). Reminiscence work with people with dementia is generally considered to date back to Butler’s (1963) ‘Life Review’ model. Butler (1963) considered Life Review to be an intuitive process whereby an individual looks back and reflects upon his/her life. It is considered to be a ‘dynamic process of adjustment’ (Woods et al., 2018, p. 7). It reflects Erikson’s (1950, 1959) eighth and final stage theory of psychosocial development, ‘ego integrity versus despair’. During this stage, people reflect back on a life lived and find meaning. If a life lived can be accepted in its entirety, ‘ego integrity’ is achieved.
All too often, the narrative of dementia as a disease dominates and the personal identity and psychological needs of the person can become less important to those who are providing care. When considering Maslow’s hierarchy of needs (Maslow, 1943), the physiological needs of a person with dementia are more easily identified and met. However, it can be more difficult to recognise emotional and psychological needs (Duffy, 2009). Reminiscence therapy can act as a corrective tool. It promotes person-centred care, which is at the heart of all good dementia care and is underpinned by Kitwood’s (1997) concept of personhood. It has been argued that ‘understanding a person’s past history is crucial to providing person-centred care for someone with dementia’ (Brooker, 2007, p. 89). Reminiscence therapy can support this understanding and subsequently person-centred care.
Reminiscence therapy is an umbrella term for several related but distinct therapeutic approaches that aim to promote well-being. In keeping with the Cochrane review (2018), this review considered (Pinquart & Forstmeier’s, 2012) three broad categories of reminiscence work; (1) ‘Simple reminiscence’ typically involves ‘autobiographical storytelling’ (Azcurra, 2012) where individuals share personal memories and stories, (2) ‘Life review’ (Butler, 1963) is a more structured and evaluative form of reminiscence that typically involves individual sessions (Woods et al., 2005) whereby therapeutic approaches are utilised to support the exploration of life experiences (both positive and negative) chronologically (Gerben et al., 2010; Woods et al., 2005) and (3) ‘Life review therapy’ aims to re-evaluate negative memories and reframe these memories in a more positive view of life. In addition, the review considered a fourth category; ‘life story work’, which is becoming increasingly common. This approach places emphasis on creating a biographical narrative and commonly this results in the development of a ‘life story book’ (Woods et al., 2018).
Rationale
Reminiscence therapy is an established therapy for people with dementia (Woods et al., 2016). It has been recommended by The British Psychological Society (2014), National Institute for Clinical Excellence (2006, 2018) and Royal College of Psychiatrists (2014). A Cochrane review (Woods et al., 2018) evidenced that despite reminiscence therapy being endorsed by ‘best-practice’ guidelines, the effects of reminiscence therapy vary depending on the way it is administered and the context in which it takes place. The Cochrane review (Woods et al., 2018) found some evidence that reminiscence therapy can improve QoL, communication, cognition and possibly mood. However, the benefits evidenced were small. Woods et al. (2018) recommended that ‘more research is needed to understand these differences’ and to establish ‘who is likely to benefit most from what type of reminiscence therapy’.
It is currently unclear whether there is a standardised approach to reminiscence therapy content and delivery. This review aims to better understand reminiscence therapy through a deeper analysis of its contents and delivery. The Cochrane review (Woods et al., 2018) contains the most up to date ‘gold standard’ reminiscence therapy trials and therefore provides the best evidence, hence the value in exploring these studies in more detail. Consequently this review will consider only those 22 studies identified by this Cochrane review (Woods et al., 2018).
Review questions
This review set out to explore whether an operational definition of reminiscence therapy exists. The following review questions were devised to unpack the components of reminiscence therapy and in doing so, establish whether reminiscence therapy is being delivered in the same way between studies. What are the components of reminiscence therapy? Who delivers reminiscence therapy? (a) What level of training is provided to those who deliver reminiscence therapy? (b) Is supervision provided to those who deliver reminiscence therapy? How is reminiscence therapy delivered? (a) Length of sessions (b) Frequency of sessions (c) Follow-up (top-up) sessions (d) Where is reminiscence therapy delivered? Is reminiscence therapy underpinned by a theoretical framework? Is reminiscence therapy delivered according to a programme/model? Are there commonalities in the reminiscence therapy components utilised?
Method
Data extraction and synthesis
Data was extracted pertaining to the components of reminiscence therapy, who delivers reminiscence therapy (level of training and supervision provided), how reminiscence therapy is delivered (length, frequency, follow-up and location of sessions), and is reminiscence therapy underpinned by a theoretical framework and is reminiscence therapy delivered according to a programme/model (the author contacted 19/22 study authors to request more detail on programme/model used)
In gathering this data, it is hoped that a deeper understanding of reminiscence therapy can be achieved. In order to identify if there are commonalities in the reminiscence therapy components utilised, the author examined and compared reminiscence components used in studies that evidenced reminiscence therapy to be beneficial with studies that did not evidence reminiscence therapy to be beneficial.
Quality assessment outcomes for the studies reviewed
The risk of bias for the included 22 studies was previously completed by two independent authors from the Cochrane review (Woods et al., 2018), using the Cochrane ‘Risk of bias’ tool (Higgins, 2011). Consequently, the reviewer did not complete additional methodological quality checks.
Ethical approval
The author can confirm that Ethical Committee approval was not required.
Results
The review questions were explored using the data from the 22 studies included in the Cochrane review (Woods et al., 2018). The quality of these studies was assessed (Woods et al., 2018). None of the studies were classified as a ‘high risk’ of bias in any of the following five domains; selection, detection, attrition, reporting and other bias.
Summary table of reminiscence therapy.

RYCR: Remembering Yesterday Caring for Today; LREF: Life Review Experiencing Form; DARES: Dementia Education Programme Incorporating Reminiscence for Staff; GRA-RO: Group reminiscence therapy with reality orientation.
aThose studies where it was possible to contact the authors for more details on the programme/model used.
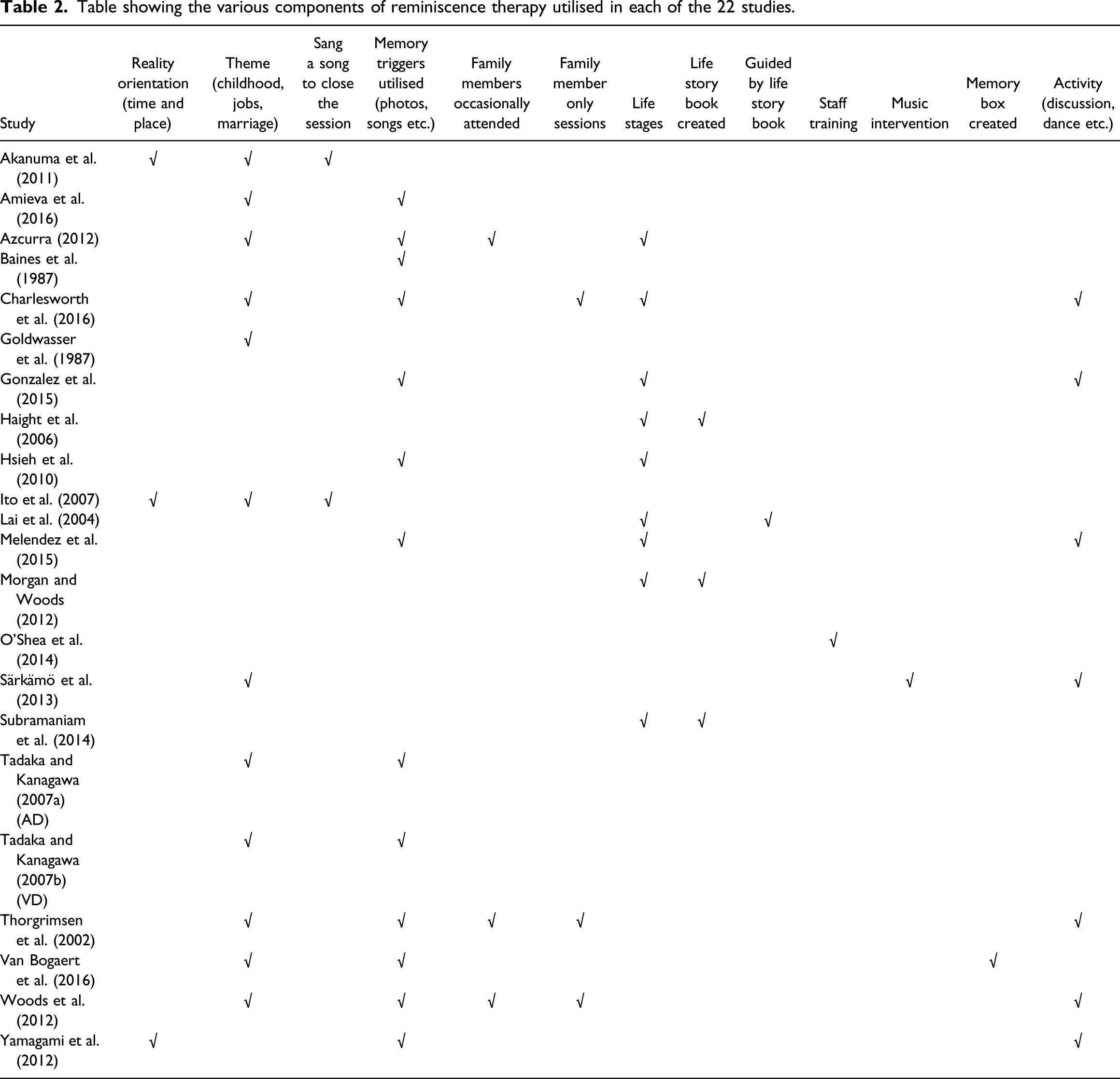
Table showing the various components of reminiscence therapy utilised in each of the 22 studies.
A comparison, using narrative analyses, of the most commonly used reminiscence therapy components (used in 50% or more studies that evidenced either a beneficial impact or no beneficial impact on outcomes).
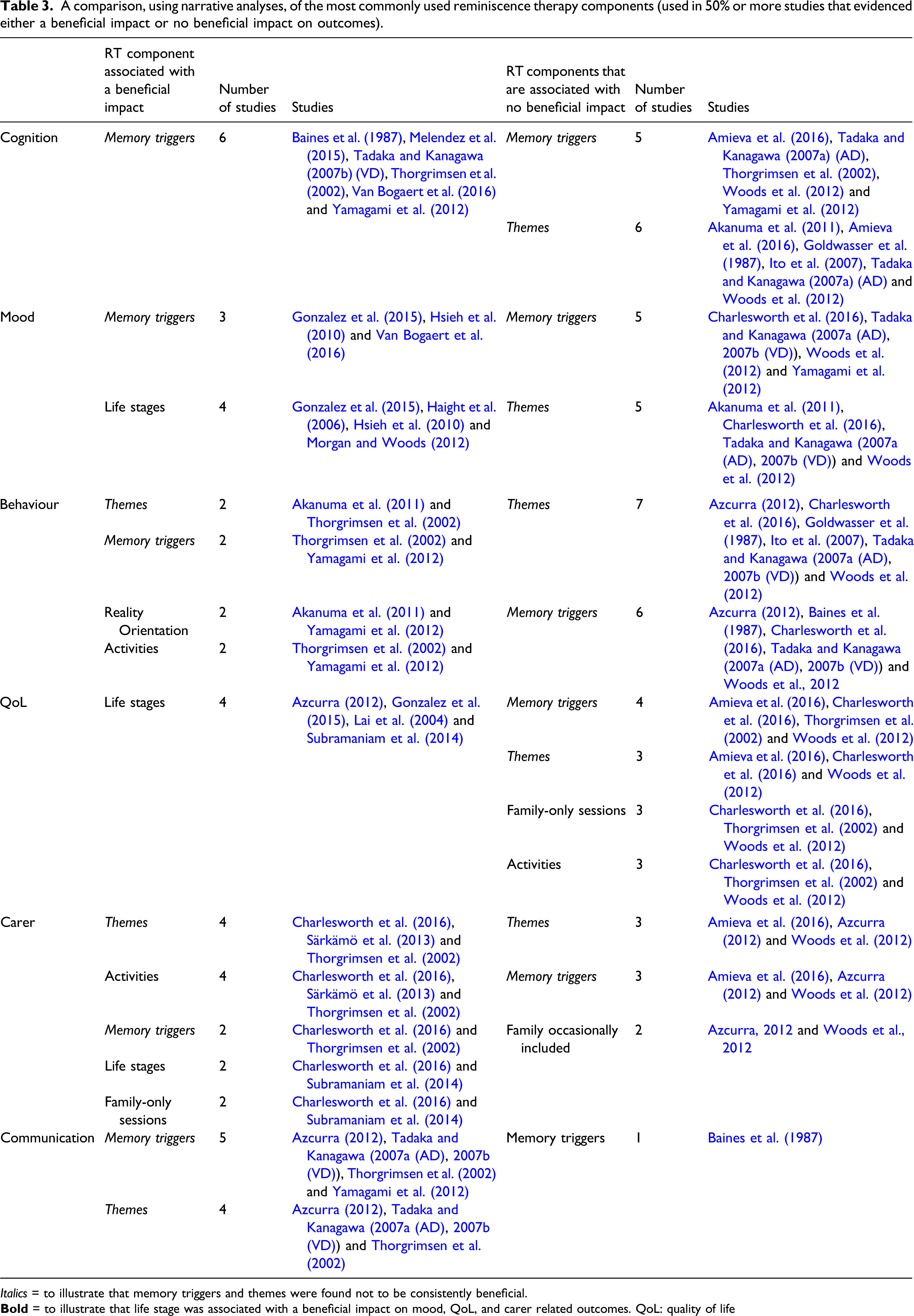
Italics = to illustrate that memory triggers and themes were found not to be consistently beneficial.
What are the components of reminiscence therapy?
Thirteen reminiscence therapy components (reality orientation (RO), discussed themes, sang a song to close, memory triggers, family members occasionally attend, family member only sessions, life stages covered, life story book created, guided by life story book, staff training, music intervention, memory box created and activities implemented) were identified. ‘Memory triggers’ was identified as the most commonly used reminiscence therapy component (n = 13), closely followed by ‘themes’ (n = 12) (Table 2). The number of reminiscence therapy components used ranged between one and five. All 22 studies utilised between one to five reminiscence therapy components.
Who delivers reminiscence therapy?
Nineteen studies reported who delivered reminiscence therapy (Table 1). Reminiscence therapy was delivered by volunteers (Van Bogaert et al., 2016), care staff (Haight et al., 2006), allied health and clinical professionals (including occupational therapists, speech therapists, mental health/geriatric nurses, clinical psychologists, arts workers and community support workers), accompanied by volunteers (Akanuma et al., 2011; Woods et al., 2012) or accompanied by care staff (Ito et al., 2007; Lai et al., 2004; O’Shea et al., 2014; Tadaka & Kanagawa, 2007a (AD), 2007b (VD)), clinical psychologists (Subramaniam et al., 2014), clinical psychologists accompanied by staff (Baines et al., 1987), psychologists (level of training not specified) (Amieva et al., 2016; Azcurra, 2012; Gonzalez et al., 2015; Melendez et al., 2015), graduate student in clinical psychology who was working in the care home as a clergyman and a volunteer social worker (Goldwasser et al., 1987), a final year trainee clinical psychologist (Morgan & Woods, 2012) and a music teacher/therapist (Särkämö et al., 2013).
What level of training is provided to those who deliver reminiscence therapy?
Eight studies reported the level of training provided. Training varied from 2 hours (Haight et al., 2006), 4 hours (Yamagami et al., 2012), 6 hours (Baines et al., 1987), 2 × 0.5 days (Woods et al., 2012), 4 (care workers) to 19.3 (research assistants) hours (Lai et al., 2004), 3 days (Amieva et al., 2016; O’Shea et al., 2014), 30.4 hours (Azcurra, 2012) and 3 months (Subramaniam et al., 2014).
What level of supervision is provided to those who deliver reminiscence therapy?
Only one study reported a measurable level of supervision (Haight et al., 2006) – weekly supervision totalling 10 hours. An additional seven studies referenced components which are typically considered supervision but did not report a measurable level (Table 1), weekly supervision with a consultant clinical psychologist (Subramaniam et al., 2014), supervision by an ‘experienced’ clinical psychologist (Morgan & Woods, 2012), support and advice (Van Bogaert et al., 2016), telephone support and one on-site visit (O’Shea et al., 2014), recorded reminiscence therapy sessions reviewed by experts (Lai et al., 2004), and consultations (frequency not reported) (Amieva et al., 2016; Woods et al., 2012).
How is reminiscence therapy delivered?
Reminiscence therapy was most commonly delivered in a group setting (Akanuma et al., 2011; Amieva et al., 2016; Azcurra, 2012; Baines et al., 1987; Charlesworth et al., 2016; Goldwasser et al., 1987; Gonzalez et al., 2015; Hsieh et al., 2010; Ito et al., 2007; Lai et al., 2004; Melendez et al., 2015; Särkämö et al., 2013; Subramaniam et al., 2014; Tadaka & Kanagawa, 2007a (AD), 2007b (VD); Thorgrimsen et al., 2002; Woods et al., 2012; Yamagami et al., 2012), with a small number being delivered on an individual basis (Haight et al., 2006; Morgan & Woods, 2012; O’Shea et al., 2014; Van Bogaert et al., 2016) (Table 1).
Five studies incorporated caregivers to varying degrees (Azcura, 2012; Charlesworth et al., 2016; Subramaniam et al., 2014; Thorgrimsen et al., 2002; Woods et al., 2012).
Length of sessions
Twenty studies reported length of sessions. Length varied from; 0.5 hour (Baines et al., 1987; Goldwasser et al., 1987; Lai et al., 2004; Melendez et al., 2015), 40–50 minutes (Hsieh et al., 2010), 0.5–1 hour (Morgan & Woods, 2012), 0.75 hour (Van Bogaert et al., 2016), 1 hour (Akanuma et al., 2011; Azcurra, 2012; Gonzalez et al., 2015; Haight et al., 2006; Ito et al., 2007; Subramaniam et al., 2014; Yamagami et al., 2012), 1.5 hours (Amieva et al., 2016; Särkämö et al., 2013), 1–1.5 hours (Tadaka & Kanagawa, 2007a (AD), 2007b (VD)) and 2 hours (Charlesworth et al., 2016; Woods et al., 2012).
Frequency of sessions
All 22 studies reported the frequency of reminiscence therapy sessions. Frequency of sessions varied as follows; three to four sessions per week for a mean of 14 weeks (42–56 sessions) (O’Shea et al., 2014), five daily sessions a week for 4 weeks (20 sessions) (Baines et al., 1987), one session a week for 6 weeks (six sessions) (Haight et al., 2006; Lai et al., 2004), one session a week for 8 weeks (eight sessions) (Tadaka & Kanagawa, 2007a (AD), 2007b (VD)), one session a week for 10 weeks (10 sessions) (Gonzalez et al., 2015; Särkämö et al., 2013), one session a week for 12 weeks (12 sessions) (Akanuma et al., 2011; Amieva et al., 2016; Charlesworth et al., 2016; Hsieh et al., 2010; Ito et al., 2007; Morgan & Woods, 2012; Subramaniam et al., 2014; Woods et al., 2012), one session a week for 18 weeks (18 sessions) (Thorgrimsen et al., 2002), two sessions a week for five weeks (10 sessions) (Goldwasser et al., 1987), two sessions a week for 8 weeks (16 sessions) (Van Bogaert et al., 2016), two sessions a week for 10 weeks (20 sessions) (Melendez et al., 2015) and two sessions a week for 12 weeks (24 sessions) (Azcurra, 2012; Yamagami et al., 2012).
Follow-up (top-up) sessions
Four studies reported follow-up sessions. One study reported that follow-up sessions were provided but did not specify the frequency (Morgan & Woods, 2012), two studies provided monthly maintenance sessions for 7 months (Charlesworth et al., 2016; Woods et al., 2012) and one study provided maintenance sessions every 6 weeks for 21 months (Amieva et al., 2016).
Where is reminiscence therapy delivered?
Fourteen out of 22 studies were conducted in a residential care setting (nursing home, care home etc.) (Akanuma et al., 2011; Azcurra, 2012; Baines et al., 1987; Goldwasser et al., 1987; Gonzalez et al., 2015; Haight et al., 2006; Hsieh et al., 2010; Ito et al., 2007; Lai et al., 2004; Morgan & Woods, 2012; O’Shea et al., 2014; Subramaniam et al., 2014; Van Bogaert et al., 2016; Yamagami et al., 2012). The remaining eight studies were conducted in a community setting (including day centres, memory centres, reminiscence centres and museums) (Amieva et al., 2016; Charlesworth et al., 2016; Melendez et al. 2015; Särkämö et al., 2013; Tadaka & Kanagawa, 2007a (AD), 2007b (VD); Thorgrimsen et al., 2002; Woods et al., 2012).
Is reminiscence therapy underpinned by a theoretical framework?
Only one study (Azcurra, 2012) explicitly stated their theoretical position: person-centred principles (Nolan et al., 2008). Another study made brief reference to Kitwood’s (1997) concept of personhood (Haight et al., 2006). A further seven studies made brief reference to Butler’s (1963) ‘Life Review’ model (Akanuma et al., 2011; Amieva et al., 2016; Goldwasser et al., 1987; Ito et al., 2007; Morgan & Woods, 2012; Tadaka & Kanagawa, 2007a (AD), 2007b (VD)), with one also making reference to Erikson’s (1950) life-span development model (Morgan & Woods, 2012) in their introductory literature reviews.
Is reminiscence therapy delivered according to a programme/model?
A ‘simple reminiscence’ approach was adopted by 16 studies (Akanuma et al., 2011; Amieva et al., 2016; Baines et al., 1987; Charlesworth et al., 2016; Goldwasser et al., 1987; Gonzalez et al., 2015; Hsieh et al., 2010; Ito et al., 2007; Melendez et al., 2015; O’Shea et al., 2014; Särkämö et al., 2013; Tadaka & Kanagawa, 2007a (AD), 2007b (VD); Thorgrimsen et al., 2002; Woods et al., 2012; Yamagami et al., 2012). Ten of these studies reported a programme/model used, accounting for six different approaches: (1) GRA-RO protocol (Akanuma et al., 2011; Ito et al., 2007), (2) Reminiscence therapy programme based on the format suggested by Norris (1986) and Bains et al. (1987), (3) Reminiscence therapy programme based on the principles of brain-activating rehabilitation (Yamaguchi et al., 2010), (4) Reminiscence therapy programme based on earlier research by Melendez et al. (2013) (Gonzalez et al., 2015; Melendez et al., 2015), (5) The Dementia Education Programme Incorporating Reminiscence for Staff (O’Shea et al., 2014) and (6) Remembering Yesterday Caring for Today (Charlesworth et al., 2016; Thorgrimsen et al., 2002; Woods et al., 2012). A ‘life review’ approach was adopted by five studies (Table 1) using two different approaches: (1) Life story book proposed by Hellen (1998), which did not lead to the creation of a life story book (Lai et al., 2004), (2) Life Review Model and Life Review Experiencing Form leading to the creation of a life story book (Haight et al., 2006; Morgan & Woods, 2012; Subramaniam et al., 2014). The remaining study (Van Bogaert et al., 2016) used the SolCos reminiscence programme, which was not considered by the Cochrane review (Woods et al., 2018) to be either a simple reminiscence approach or a life review approach.
Are there commonalities in the reminiscence therapy components utilised?
Table 3 provides a comparison of the reminiscence therapy components utilised in studies that evidenced a beneficial impact in six domains (cognition, mood, behaviour, QoL, carer and communication) with those studies that did not evidence a beneficial impact. Reminiscence therapy components were considered the most frequently used if they were utilised by 50% or more of the studies. The reminiscence therapy component memory triggers, and to a lesser degree themes, were found not to be consistently beneficial (highlighted in italics). The reminiscence therapy component, life stages, was associated with a beneficial impact on mood, QoL and carer related outcomes (highlighted in bold). The reminiscence therapy component, activities, was associated with a beneficial impact on behaviour and carer related outcomes. In addition to the reminiscence therapy components, life stages and activities, the narrative analysis identified family-only sessions, as a beneficial reminiscence therapy component for carer related outcomes.
Discussion
This review set out to better understand reminiscence therapy for people with dementia. The analysis focussed on the 22 studies included in the most recent Cochrane review of reminiscence therapy (Woods et al., 2018). This review completed multiple narrative analyses of reminiscence therapy to explore six questions that can be subdivided into two distinct but related areas. The first focussed broadly on reminiscence therapy content and delivery by exploring and analysing the following areas: (1) What are the components of reminiscence therapy? (2) Who delivers reminiscence therapy (including level of training and supervision provided) (3) How is reminiscence therapy delivered (including length, frequency, follow-up sessions and delivery location) (4) Is reminiscence therapy underpinned by a theoretical framework? (5) Is reminiscence therapy delivered according to a programme/model? The second focussed specifically on exploring and analysing reminiscence therapy components by asking the following question: (6) Are there commonalities in the reminiscence therapy components utilised?
Synthesis of reminiscence therapy content and delivery
What are the components of reminiscence therapy?
A narrative analysis of the 22 studies identified 13 reminiscence therapy components (RO, themes, sang a song to close the session, memory triggers, family occasionally attended, family-only sessions, life stages, development of a life story book, guided by a life story book, staff training, music intervention, memory box and activities) (Table 2). ‘Memory triggers’ (59% studies) and ‘themes’ (55% studies) were identified as the most commonly utilised reminiscence therapy components in the 22 studies. The analysis indicates inconsistencies in the reminiscence therapy components utilised by each study. The number of reminiscence therapy components used by each study ranged from one to five (Table 2).
Who delivers reminiscence therapy?
Reminiscence therapy was delivered by a wide range of individuals (Table 1). When considering level of training, the analysis was limited by the level of information reported by studies. Sixty-four percent of studies did not report the level of training provided. Of those studies that did, there was no consistency in the level of training provided (2 hours to 3 months) (Table 1). Only one study reported a measurable level of supervision (Haight et al., 2006). A further seven studies reported variations of what would typically be considered supervision components (support and advice, video feedback, consultations) but did not explicitly report that supervision was provided and did not specify the level provided (Table 1). Given the insufficient information available to the author, it was not possible to make a judgement on supervision provided. This review highlights the need for greater transparency in study methods (Table 1). Based on the available data the review identified that reminiscence therapy is delivered by any type of health care worker, ranging from care worker to psychologist. Expertise, training, supervision and experience will vary considerably. Therefore this review can conclude that there are no consistencies in who delivers reminiscence therapy.
How is reminiscence therapy delivered?
The review identified that reminiscence therapy is typically conducted in a care setting (64% studies), using a group approach (73% studies) and on occasion, carers are incorporated to varying degrees (23% studies). Despite length of reminiscence therapy sessions being well reported (91%), inconsistencies were identified (Table 1). Length varied from 0.5 hours to 2 hours, with 1 hour sessions being the most common (35% studies). It was not possible to calculate a mean session length as several studies reported length as a range. Similarly, although frequency of sessions was well reported (Table 1), inconsistencies in the number of reminiscence therapy sessions delivered per week (one to five sessions) and the duration of the intervention (4–18 weeks) were identified. Based on the available data, this review can conclude that reminiscence therapy tends to be delivered in a care setting using a group approach. Occasionally carers are incorporated to varying degrees. Huge discrepancies in session and duration length were noted. Thus, this review highlights the many apparent inconsistencies in how reminiscence therapy is delivered.
Is reminiscence therapy underpinned by a theoretical framework?
Reminiscence therapy places importance on the personal history of individuals. Butler’s (1963) life review model is widely considered to be the theoretical foundation of reminiscence therapy, along with Erikson’s (1950, 1959) developmental life stage model. Because reminiscence therapy provides a greater understanding of a person, it is considered a helpful tool when providing person-centred dementia care, as it supports the preservation of personhood (Kitwood, 1997). With this in mind, one might expect that the reminiscence therapy approaches utilised in the 22 studies would have been informed by Butler’s (1963) and Erikson’s (1950, 1959) theories. However, this was not the case. None of the 22 studies reported that the reminiscence therapy approach used was underpinned by either Butler’s (1963) life review model or Erikson’s (1950) life span development model. However, 32% of studies briefly referenced Butler’s (1963) model in their literature reviews, with one also making reference to Erikson’s (1950) model. Only one study (Azcurra, 2012) explicitly reported that the reminiscence therapy approach used was underpinned by a theoretical framework and this was person-centre principles (Table 1). The author would argue that ‘person-centred principles’ are more akin to a framework of care and a holistic and personalised ethos, rather than a theoretical framework. It may be that this study was referring to Kitwood’s (1997) principles of personhood, which informs person-centred dementia care, but this cannot be confirmed with the available information. The lack of a theoretical underpinning is surprising given the theoretical foundation of reminiscence therapy and the governmental direction on developing ‘…programmes, policies and interventions that are underpinned by evidence and theory…’ (Public Health England, 2018). In summary, the review evidenced that there is no clear operationalisation of theory in reminiscence therapy.
Is reminiscence therapy delivered according to a programme/model?
The review indicates that a ‘simple reminiscence’ approach was most widely used (16/22 studies), followed by a ‘life review’ approach (5/22 studies). The analysis identified nine different reminiscence therapy programmes/models (Table 1). There was no consistency in the programme/model used. Exploring whether a relationship exists between programme/model and beneficial outcomes extends beyond the scope of this review.
Reminiscence therapy component analysis
Are there commonalities in the reminiscence therapy components utilised?
The 22 studies reviewed represent a heterogeneous sample. Given the heterogeneity of the data and the many inconsistencies regarding for example reminiscence therapy content, who delivers reminiscence therapy and how reminiscence therapy is delivered, it is difficult to succinctly identify commonalities in reminiscence therapy. However, based on the available data, ‘memory triggers’ and to a lesser extent ‘themes’, were found not to be consistently beneficial (Table 3). Furthermore, based on the available data this review could not reliably determine what was used as ‘memory triggers’ and could not determine if the same ‘memory triggers’ and ‘themes’ were used between studies (Table 1).
Secondly, given that reminiscence therapy is based on reflecting back on a life once lived (Butler, 1963; Erikson, 1950, 1959), it was surprising that less than half of the 22 studies examined utilised the reminiscence therapy component ‘life stages’ (9/22 studies) (Table 2). Importantly, this review identified that this reminiscence therapy component was used in studies that evidence beneficial mood, QoL and carer outcomes, future research may wish to explore this reminiscence therapy component further.
In 75% of studies that evidenced beneficial carer outcomes and 50% of studies that evidenced beneficial behaviour–related outcomes in people with dementia, ‘activities’ were used. The progressive nature of dementia impacts negatively on an individual’s social connectedness and typically relationships become care-driven and are characterised by unidirectional interactions (Pearlin et al., 1990). The review makes the tentative suggestion that the inclusion of the reminiscence therapy component ‘activities’, may offer carers new opportunities to engage with their loved ones on a personal/human level, rather than based on a needs driven response and in doing so, support more meaningful connections for both the person with dementia as well as the carers (Gilliard et al., 2005).
Another interesting finding can be illustrated when reminiscence therapy components in studies that evidenced beneficial carer outcomes are compared with studies that did not evidence beneficial carer outcomes. ‘Family-only sessions’ were used in 50% of studies evidencing a beneficial outcome and ‘family occasionally included’ sessions were used in 50 percent of studies that did not evidence a beneficial outcome. Although family were incorporated in both sets of studies, their incorporation differed. While it was not always clear what ‘family-only sessions’ involved, unlike ‘family occasionally attended’ sessions, this particular reminiscence therapy component provided carers with a unique opportunity to meet others with similar and shared experiences. In doing so, carer connectedness rather than isolation is nurtured. This is supported by a meta-analysis of caregiver support groups (Chein et al., 2011) which evidenced significant positive effects on caregiver depression, burden, psychological well-being and social outcomes.
Strengths and limitations of the review
The importance of this review is that it is the first of its kind to complete in-depth narrative analyses of reminiscence therapy content and delivery from those 22 studies included in the Cochrane review (Woods et al., 2018). Secondly, although each study varied in terms of what they were investigating and measuring, the findings of this review suggests a consensus around measuring a core set of six domains (cognition, mood, behaviour, QoL, communication and carer). While the heterogeneity of the data along with inconsistent and limiting reporting of data limited the author’s ability to address and answer the research questions set out in the review, the findings that can be offered remain important. As a result of this review, 13 reminiscence therapy components were identified. Reminiscence therapy is typically delivered in a care setting using a group approach. This review evidenced inconsistencies between studies with respect to the extensive reminiscence therapy components used, session composition (length, frequency, follow-up) and intervention duration. Furthermore, this review identified that reminiscence therapy does not appear to be underpinned by expected theories and is not routinely delivered according to a programme/model. Based on a small number of studies this review identified that the reminiscence therapy components, ‘life stages’, ‘activities’ and ‘family-only sessions’, were used in studies that evidenced beneficial outcomes. However, until more studies confirm these reminiscence therapy components as beneficial, these findings should be considered with caution. Furthermore, the studies examined in this review typically included participants with either AD or VD, limiting the generalisability of the findings. Finally, by only reviewing the 22 studies from the Cochrane review (Woods et al., 2018), newer studies were not considered in this review.
Future directions & clinical implications
Reminiscence therapy is a therapeutic approach for people with dementia that draws upon past memories from people’s lives. It is widely considered to be underpinned by Butler’s (1963) life review model and Erikson’s (1950, 1959) developmental life stage model. There is some evidence that reminiscence therapy can improve QoL, communication, cognition and possibly mood (Woods et al., 2018). However, the benefits evidenced were small (Woods et al., 2018). This review set out to identify and provide an overview of reminiscence therapy content, delivery and identify commonalities. The heterogeneity and limitation of the data somewhat prevented the author doing this in a meaningful and conclusive way. Definitive conclusions will only become a possibility when there is transparent and consistent reporting of reminiscence therapy content (including theory and programme/model), delivery and theory. Given that ‘memory triggers’ and ‘themes’ were found not to be consistently beneficial and the review could not reliably determine what was used as ‘memory triggers’ and could not determine if the same ‘memory triggers’ and ‘themes’ were used between studies, future research may wish to consider developing evidence based ‘memory triggers’ and ‘themes’. Additionally, ‘activities’, and ‘family-only sessions’, were identified in a small number of studies that evidenced carer benefit. Given that a reduction in caregiver stress can improve the quality of care received by individuals with dementia (Laidlaw et al., 2003, p. 144), future research would benefit from exploring the carer component of reminiscence therapy in greater detail. A recent meta-analysis (Abrahams et al., 2018) advocates for a multicomponent caregiver intervention consisting of support groups, stress and mood management, counselling, telephone support and education components. Future research may wish to consider including an evidence based caregiver only programme run alongside reminiscence therapy.
Conclusion
This review set out to provide a comprehensive and conclusive overview of reminiscence therapy content, delivery and commonalities. However, this was not possible. The 22 studies reviewed represent a heterogeneous sample. However, based on the available data, the main tentative findings are as follows: 13 reminiscence therapy components were identified. ‘Memory triggers’ and ‘themes’ were the most commonly used reminiscence therapy components but were found not to be consistently beneficial. Reminiscence therapy was typically delivered in a care setting using a group approach. There was no consistency in reminiscence therapy session composition, intervention duration, who delivers reminiscence therapy or the training and supervision provided to those who deliver reminiscence therapy. Reminiscence therapy delivered according to a programme/model was the exception rather than the norm. There was no clear operationalisation of theory within reminiscence therapy. Lastly, as a result of a small number of studies, the reminiscence therapy components ‘life stages’, ‘activities’ and ‘family-only sessions’ showed beneficial promise. In summary, this review highlights that reminiscence therapy needs more consistency in content and delivery, in addition to a clear theoretical framework.
Supplemental Material
DEMA_10.1177_1471301220941275_1 – Supplemental Material for Towards an increased understanding of reminiscence therapy for people with dementia: A narrative analysis
Supplemental Material, DEMA_10.1177_1471301220941275_1 for Towards an increased understanding of reminiscence therapy for people with dementia: A narrative analysis by Fiona Macleod, Lesley Storey, Teresa Rushe and Katrina McLaughlin in Dementia
Supplemental Material
DEMA_10.1177_1471301220941275_2 – Supplemental Material for Towards an increased understanding of reminiscence therapy for people with dementia: A narrative analysis
Supplemental Material, DEMA_10.1177_1471301220941275_2 for Towards an increased understanding of reminiscence therapy for people with dementia: A narrative analysis by Fiona Macleod, Lesley Storey, Teresa Rushe and Katrina McLaughlin in Dementia
Supplemental Material
DEMA_10.1177_1471301220941275_3 – Supplemental Material for Towards an increased understanding of reminiscence therapy for people with dementia: A narrative analysis
Supplemental Material, DEMA_10.1177_1471301220941275_3 for Towards an increased understanding of reminiscence therapy for people with dementia: A narrative analysis by Fiona Macleod, Lesley Storey, Teresa Rushe and Katrina McLaughlin in Dementia
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.