
Abstract
Background
People living with dementia often develop distressing behavioural and psychological symptoms (BPSD) that can affect their quality of life and the capacity of family carers and staff providing support at home. This systematic review of qualitative studies considers the views and experiences of people living with dementia and care providers about these symptoms and what helps to reduce their impact.
Methods
The two-stage review involved (a) An initial mapping of the literature to understand the range of BPSD, and how it is operationalised by different groups, to develop a search strategy; (b) A search of electronic databases from January 2000 to March 2015, updated in October 2016. Included studies focused on people living in their own homes. Data extraction and thematic analysis were structured to provide a narrative synthesis of the evidence.
Results
We retrieved 17, 871 records and included relevant qualitative papers (n = 58) targeting community-dwelling people with dementia and family carers around the management of BPSD. Five key themes were identified: (1) Helpful interventions/support for BPSD management, (2) Barriers to support services for BPSD management, (3) Challenges around recognition/diagnosis of BPSD, (4) Difficulties in responding to aggression and other BPSD, and (5) Impact of BPSD on family carers and people living with dementia.
Conclusions
Family carers sometimes feel that their experiences of BPSD may not be evident to professionals until a crisis point is reached. Some helpful services exist but access to support, lack of knowledge and skills, and limited information are consistently identified as barriers to their uptake. The lack of common terminology to identify and monitor the range of BPSD that people with dementia living at home may experience means that closer attention should be paid to family carer accounts. Future research should include qualitative studies to evaluate the relevance of interventions.
Keywords
Background
In the UK, around two-thirds of people with dementia live at home (Nyman, Mc Parland, & Innes, 2015). Behavioural and psychological symptoms of dementia (BPSD) is a term often used to describe a range of symptoms that can be stressful to witness or to manage by family carers. These distressing non-cognitive symptoms are estimated to affect up to 90% of people living with dementia at some stage and they often affect the family carer’s ability to provide support at home. People with dementia experiencing such symptoms have a poor prognosis, use care services more than others, and are more likely to make unwanted moves to care homes (Robinson et al., 2006; Savva et al., 2009).
There is variability about what is termed BPSD in the UK and world-wide (Cerejeira, Lagarto, & Mukaetova-Ladinska, 2012). Essentially it describes a range of symptoms that may be hard to manage or to witness by family carers and practitioners alike (often termed ‘behaviour that challenges’ or ‘distressing behaviour’ that may be a communication of unmet needs). Symptoms may include aggression, risky and apparently strange behaviours, wandering or walking, agitation, apathy or emotional distress. These can affect the ability to sustain everyday activities, and reduce quality of life (Kales, Gitlin, & Lyketsos, 2015).
While the traditional approach of reviewing research mainly focuses on quantitative data, there is growing awareness of the salience of literature reviews that explore qualitative studies as they can add important insights not found in quantitative studies (Dixon-Woods & Fitzpatrick, 2001; Hasseler, 2007). Some qualitative reviews have examined the general experiences of people living with dementia (de Boer et al., 2007; Steeman, de Casterle, Godderis, & Grypdonck, 2006), mainly emphasising memory problems and their effects on everyday life. Other reviews have been of studies in mixed (residential/community) (Sung & Chang, 2005) or residential (Bradshaw, Playford, & Riazi, 2012) settings, while a recent review of qualitative studies highlighted the general problems that occur with early onset dementia (Greenwood & Smith, 2016).
The National Dementia Strategy in England highlighted the need for more community-based personal support, reduced use of antipsychotic medication and alternative approaches to the support and management of BPSD (Department of Health, 2009). Our study aimed to inform this approach, by reviewing the views and experiences of participants in different non-pharmacological community based support programmes. The impact of the various interventions as shown by quantitative outcomes is reported separately (Trivedi et al., 2018).
Methods
A preliminary stakeholder meeting with health and social care practitioners, researchers, and family carers of people with dementia informed the review’s search terms, definitions of BPSD and home care challenges. Involving different stakeholders in the refinement and interpretation of the review process and research design has been undertaken in previous complex reviews (Goodman et al., 2010; Iliffe et al., 2010; Moriarty, Manthorpe, Wilcock, & Iliffe, 2007; Popay, 2016). In this present study the stakeholder meeting was followed by a broad mapping of the literature on BPSD, leading to the in-depth systematic review of quantitative and qualitative studies (following the approach developed by Greenhalgh & Peacock, 2005). Only findings from qualitative studies are reported in this present paper. At the end of the study, findings were discussed with people living with dementia, family carers and service providers. Our methods were pre-specified in a published protocol (Trivedi et al., 2013).
Selection criteria
In this review we included qualitative studies that had explored the views and experiences around the management of BPSD of people with dementia living at home and their family carers. There were no set limits to the qualitative methods employed in our search strategy, but selection criteria included:
Studies covered, for example, responses to BPSD, dealing with behavioural problems, and, more generally, the impact of BPSD on everyday life. A focus was on community-dwelling participants.
In terms of exclusion criteria, studies of people with dementia living in long-term care facilities were excluded as well as literature not published in the English language.
PRISMA guidance (PRISMA, 2016) was followed for the reporting of this literature review. An accompanying paper examined randomised controlled trials on the management of BPSD (Trivedi et al., 2018).
Search strategy
Studies were identified by computerised searches of PubMed, Embase, CINAHL, PsycInfo, AMED, HMIC, BNI, HEALTH BUSINESS ELITE, Scopus and Web of Knowledge (Web of Science). In addition, we searched the Cochrane Library and carried out lateral searches (checking reference lists and citation searches) and screened several reviews to identify studies that included people with dementia living at home. An example search query from PubMed is presented in the supplementary Search Box A1. Searches were conducted in October/November 2012 (from year 2000) with updates in March 2015, and with a further search in October 2016 of PubMed, Scopus, and Google Scholar. An overview of the qualitative study selection process is presented in Figure 1.
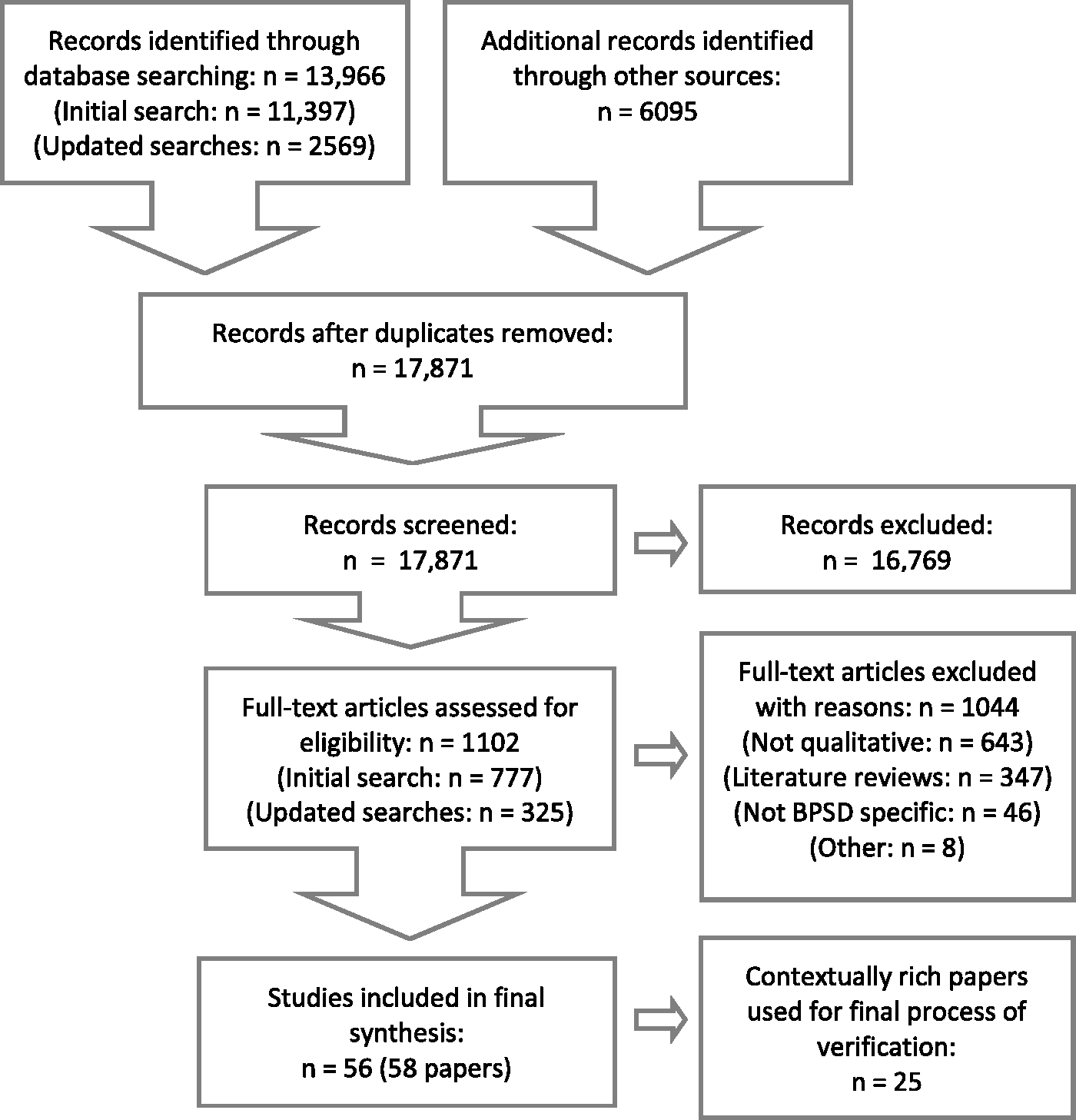
PRISMA flow diagram of qualitative study selection process.
Screening, data extraction and critical appraisal
All records were managed with Endnote version X7.5. Due to the large volume of literature, 10% were independently screened for inclusion by two reviewers to check for agreement. Hard copies of potentially relevant papers were further screened, with 20% screened independently. Relevant data, such as aims, methods, design, setting and participant characteristics, were extracted using a pre-piloted data extraction tool. Qualitative data from final included papers were imported into NVivo version 11 and coded independently by two reviewers and checked by a third.
Quality assessment was conducted independently by two reviewers and examined for consistency by a third reviewer using a checklist based on Spencer, Lewis, and Dillon’s (2003) framework for assessing quality in qualitative research. The main quality assessment principles included scope and purpose, design, sample, data collection, analysis, validity, generalisability and credibility. A summary of quality assessment domains is given in Figure 2, which shows authors’ judgements about each quality domain presented as percentages across all 58 included papers. Where necessary we sought further information from authors. All relevant studies were included regardless of their quality.
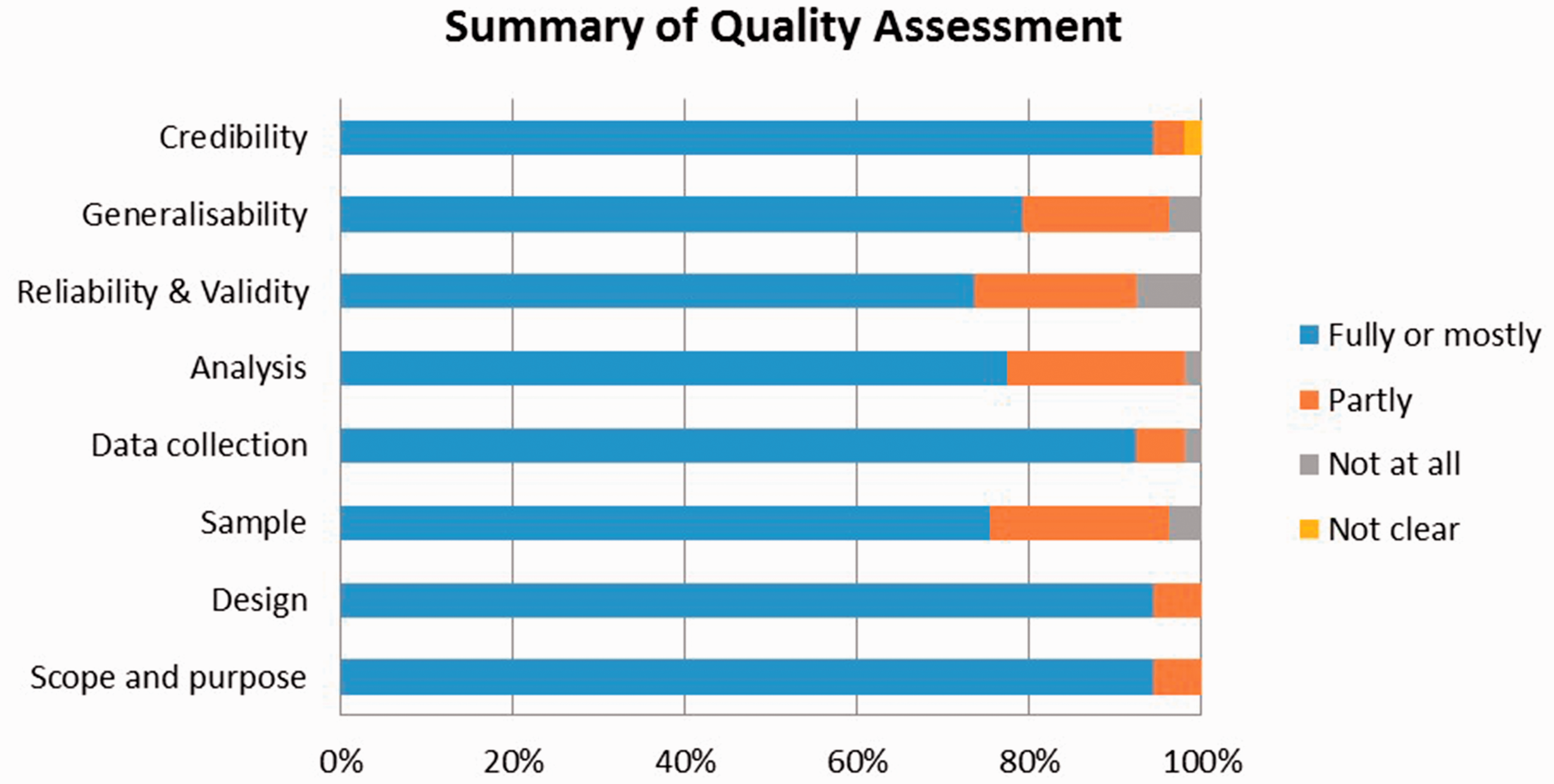
Summary of quality assessment domains.
Analysis and synthesis
By drawing on previous frameworks for thematic synthesis (Thomas & Harden, 2008), we included data from studies in form of quotations, results and findings. This process has previously been used successfully in other systematic reviews to synthesize a large number of qualitative studies (Bunn et al., 2012; Campbell et al., 2003). Thematic analysis involved the identification of prominent themes and sub-categories that emerged not only from quotations, but also from relevant text within each paper. We used qualitative data analysis software Nvivo (QSR International Pty Ltd. Version 11, 2016), which helped to facilitate the development of themes and to analyse individual studies, as well as groups of studies. In this process we analysed and coded all 58 papers to create a ‘Hermeneutic Unit’, which served as a network of associated codes and sub-codes leading to the emergence of meaningful interpretive themes (Thomas & Harden, 2008). Finally, we verified the themes using 25 papers that were contextually rich, scoring high for both reliability and usefulness, in order to conceptualise the various views and experiences about BPSD management.
Results
Preliminary stakeholder event and evidence mapping
Discussion with stakeholders revealed a lack of a shared terminology about BPSD and how symptoms are defined and prioritised by different professional groups. Practitioners and family carers suggested that there was a need to understand behaviours that they thought were commonplace (e.g. aggression) and those that were less common (e.g. sexual disinhibition). Accounts highlighted the distressing nature of these symptoms and varied knowledge of possible interventions and experiences of accessing support, underpinning the need for comprehensive and sensitive searches to capture the heterogeneity of BPSD. We retrieved 17,871 de-duplicated records in Endnote that were screened for potential inclusion (see Figure 1). The initial mapping phase helped identify relevant papers for an in-depth systematic review.
Description of included studies
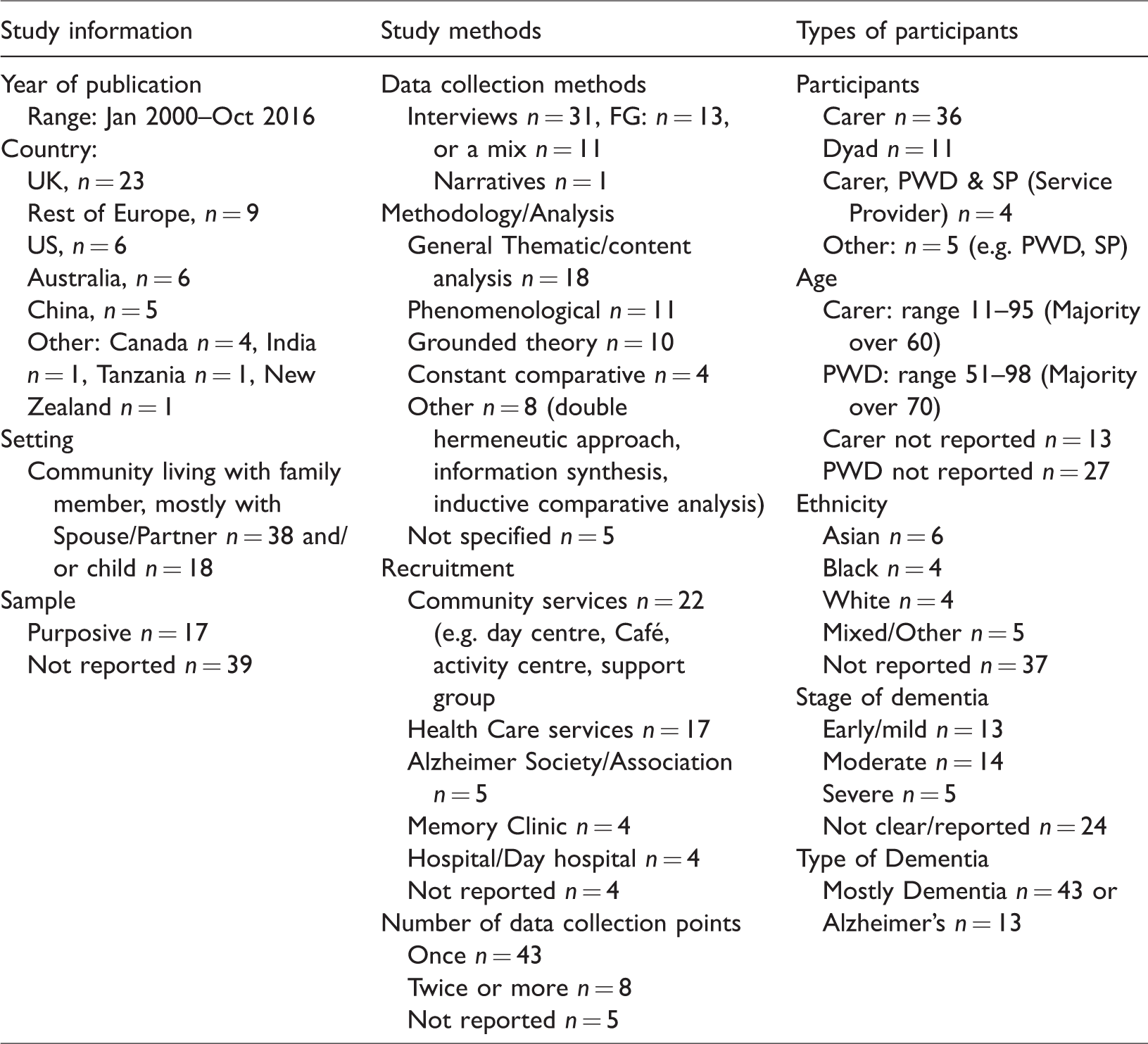
We identified 58 qualitative papers (56 studies) that met our inclusion criteria, spanning a total of data collected from, 1326 family carers, 182 people living with dementia, and 89 health professionals/practitioners. Most were conducted in the UK (n = 23), the rest of Europe (n = 9), the United States (US) (n = 6) or other countries. Participants were recruited mostly via community organisations (n = 22) or health care services (n = 17). The majority of people living with dementia in these studies resided with a spouse/partner and had early/mild or moderate dementia. General Thematic/Content Analysis was the most common methodology used to analyse the qualitative interview data (n = 18), followed by Phenomenological approaches (n = 11), Grounded Theory (n = 10), and others. An overview of the study characteristics is presented in Table 1.
Overview of qualitative studies.
Study quality
The overall reliability and usefulness of the included papers were classified as low, medium or high (Spencer et al., 2003). Overall, 47% of the papers scored high for reliability, 41% medium and 12% low. For usefulness, 52% scored high, 38% medium and 10% low. Nearly half, 25 papers (43%), scored high for both reliability and usefulness. These were contextually rich papers that explored the management of BPSD well, supported by convincing evidence of quotes or statements. The other 33 papers, which were of lower quality, supported or illustrated the overall findings of this study. Evidence is summarised from all 58 papers, while the contextually rich 25 papers were used to verify our findings. A record of individual quality assessment scores and other details of all 58 papers are presented in the supplementary Table S1.
Findings from the thematic synthesis
We identified five overarching themes to illustrate the general impact and experiences of BPSD of people living with dementia and their family carers. Figure 3 illustrates the key themes and subthemes supported by quotes. Themes 1 and 2 represent the key points about managing BPSD in different contexts and where there are system based enablers or barriers, while the last three themes emphasise the difficulties in responding to certain symptoms and the impact on family carers and people living with dementia. All themes are interlinked and reflect the dynamic process of BPSD, starting with the occurrence of one or more mild symptoms until they escalate and may become unmanageable by family carers. A list of quotations linked to each theme is given in the supplementary Table S2.
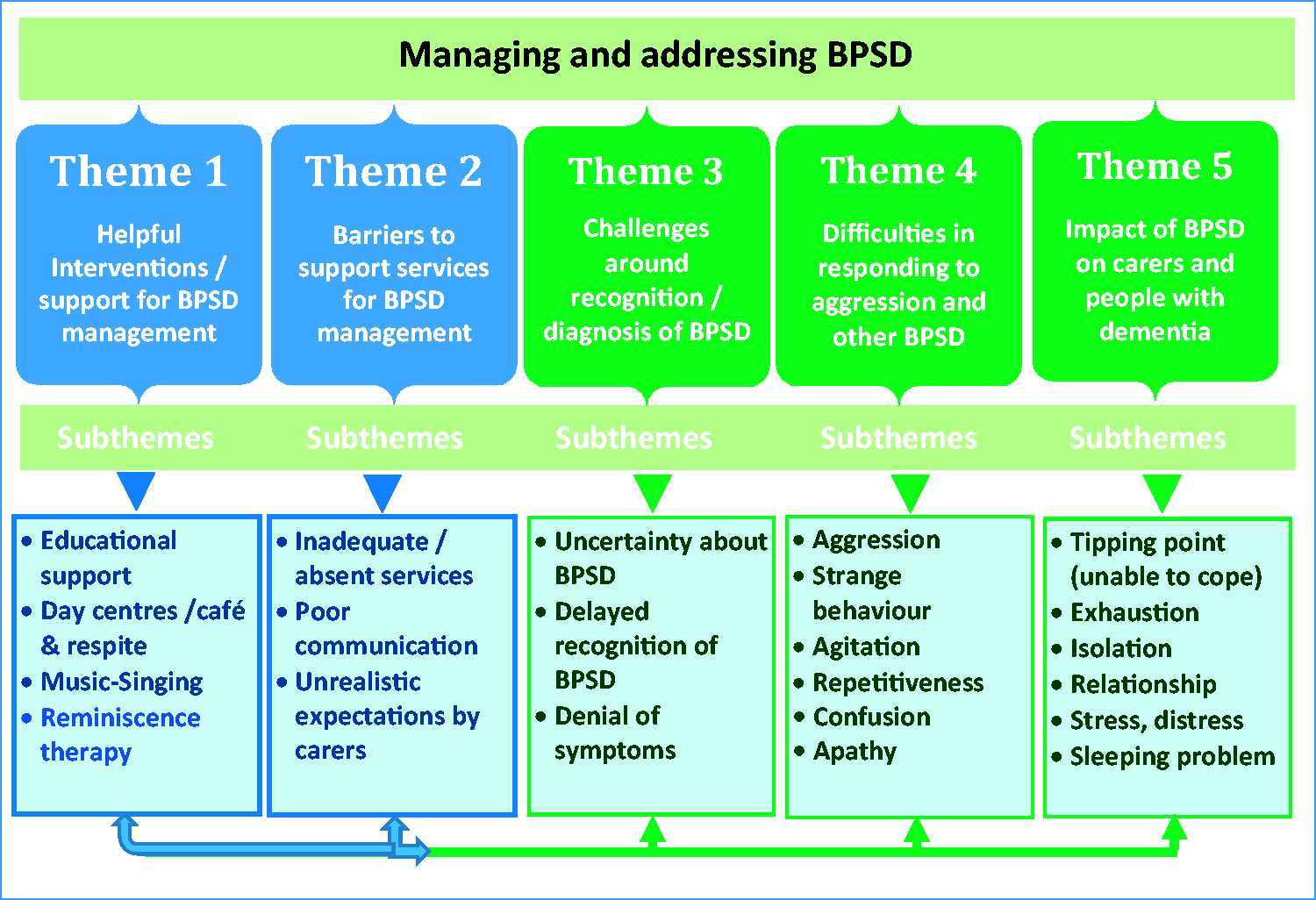
Overarching themes and subthemes.
Theme 1: Helpful interventions/support for BPSD management
The literature identified many interventions that were thought to support family carers and people living with dementia. The most frequently mentioned interventions or programmes were education, respite, day centres, music and reminiscence.
Educational support
Enhancing family carer skills and educational support (training) can assist with managing BPSD. These may include dealing with emotional and physical responses to care, unexpected changes, competing responsibilities and other stressors (Farran, Loukissa, Perraud, & Paun, 2003, 2004; Landmark, Aasgaard, & Fagerström, 2013; Milne, Guss, & Russ, 2014; Samia, Hepburn, & Nichols, 2012).
Day centres and respite
Additional beneficial support included attending day centres or meeting centres and Dementia Cafés (Capus, 2005; Ivey et al., 2013; Meiland, Droes, de Lange, & Vernooij-Dassen, 2005; Perraud, Farran, Loukissa, & Paun, 2004; Phillipson & Jones, 2012). These centres ‘freed up’ family carers by providing respite from care responsibilities. They also reduced isolation and generally helped by offering the opportunity to share experiences with other carers (Ivey et al., 2013; Robinson, 2012; Toot et al., 2013; Xiao, De Bellis, Habel, & Kyriazopoulos, 2013).
Music
Furthermore, there was a cumulative narrative about the benefits of music, including singing and dancing, to relieve some symptoms for people living with dementia and improve mood or becoming less withdrawn and more communicative (Camic, Williams, & Meeten, 2013; Hamill, Smith, & Rohricht, 2012; McDermott, Orrell, & Ridder, 2014; Osman, Tischler, & Schneider, 2016).
Joint reminiscence therapy
Family carers described the benefits of joint reminiscence therapy (Samia et al., 2012) as drawing on others’ experiences (Marshall, Bucks, & Mander, 2005). A daughter said: ‘It (reminiscent group) gave us the time to talk about any problems we had and to talk with others and found out how they managed; their coping strategies and how they felt about how things were going with their people’ (Melunsky et al., 2015, p. 852).
Additional support
Other support programmes included, for example, the use of narratives (Benbow & Kingston, 2016), carer networks (Egdell, 2012; Forbes et al., 2012; Powell et al., 2010), counselling (Sorensen, Waldorff, & Waldemar, 2008; Vernooij-Dassen, Joling, van Hout, & Mittelman, 2010), art gallery visits (MacPherson, Bird, Anderson, Davis, & Blair, 2009) and assistive technologies (GPS, Telephone, cameras) (Lindqvist, Nygard, & Borell, 2013; McCabe & Innes, 2013; Meiland et al., 2014; Salfi, Ploeg, & Black, 2005; White & Montgomery, 2014; White, Montgomery, & McShane, 2010). These programmes were mostly described as ‘helpful’ for family carers in coping with the daily tasks of supporting people living with dementia.
Theme 2: Barriers to support services for BPSD management
Barriers to services often prevented individuals from potentially benefiting from the interventions designed to reduce or ameliorate the impact of BPSD (Gorska et al., 2013; Oyebode, Bradley, & Allen, 2013; Phillipson & Jones, 2012; Samia et al., 2012; Stokes, Combes, & Stokes, 2014; Toot et al., 2013). The three main barriers described are inadequate/absent services, poor communication and unrealistic expectations.
Inadequate/absent services
Some services, when offered, were not helpful, inadequate or absent altogether (Nichols et al., 2013), such as respite for family carers (de la Cuesta-Benjumea, 2010; Oyebode et al., 2013; Phillipson & Jones, 2012; Samia et al., 2012). Few studies appear to have investigated whether problems of access or eligibility criteria are associated with inadequate services (Gorska et al., 2013). Other argued that services should provide person centred-care to meet the individual needs of people living with dementia and their family carers (Soderhamn, Landmark, Eriksen, & Soderhamn, 2013).
Poor communication
Poor communication about existing services or the lack of right and timely information was another barrier to the uptake of appropriate services. Some health professionals were thought to be unaware of services at the time of dementia diagnosis (Stokes et al., 2014; Toot et al., 2013). ‘My idea was to have that signpost available, a first port of call, rather than going in several different directions at the same time’ (Stokes et al., 2014, p. 65). In one study, the authors pointed out that dementia service helplines ‘were only accessed by those who knew about them and who were fluent in English’ (Xiao et al., 2013, p. 7). Bilingual care coordinators may be helpful in identifying support for behaviour management in some settings (Xiao et al., 2013).
Unrealistic expectations
Some family carers had unrealistic expectations about the trajectory of dementia. It was reported that some believed that a person living with dementia may become ‘normal’ again (Paton, Johnston, Katona, & Livingston, 2004). Moreover, some family carers were unwilling or unable to accept support, perhaps reflecting dementia’s stigma or their distorted expectations (Au, Shardlow, Teng, Tsien, & Chan, 2013; Mushi et al., 2014; Oyebode et al., 2013).
Theme 3: Challenges around recognition/diagnosis of BPSD
The literature suggests that the detection of early signs of BPSD is not easy for practitioners. This can result in delay of interventions and increased burdens for family carers (Ducharme, Kergoat, Antoine, Pasquier, & Coulombe, 2013). Three subthemes were identified within Theme 3:
Uncertainty about BPSD
Uncertainty about the significance of BPSD among General Practitioners (GPs) and other health professionals may delay intervention (Bruce & Paterson, 2000; Chan et al., 2010; Ducharme et al., 2013; Gorska et al., 2013; Ivey et al., 2013; Scott, Lewis, & Loughlin, 2005). While most health professionals were reportedly helpful in identifying dementia, some GPs were thought not to recognise BPSD symptoms early enough (Ducharme et al., 2013; Toot et al., 2013; Xiao et al., 2013). Possibly as a result, interventions were not initiated, increasing stress for family carers and for people living with dementia.
Delayed recognition
Some UK studies of family carers suggest that the dismissal of concerns by some health professionals was the reason for delayed recognition of BPSD (Gorska et al., 2013; Stokes et al., 2014; Toot et al., 2013). Others felt that care pathways managed by a single service would provide better monitoring of escalating symptoms and timely action. A daughter who cared for her mother suggested: ‘I think it (service) maybe needs checklist that are not there. Just to tick off, right, this is where we are’ (Gorska et al., 2013, p. 1111).
Denial
Some family carers and older people living with dementia were thought to ‘play down’ the severity of BPSD (Au et al., 2013), by relating the symptoms to old age.
Theme 4: Difficulties in responding to aggression and other BPSD
The literature identified family carer accounts of a number of problem behaviours among people living with dementia, especially aggression, but also repetitiveness, agitation, confusion or apathy.
Aggression
The most commonly mentioned problems in the studies identified were aggressive and abusive behaviour (Au et al., 2013; Ducharme et al., 2013; Farran et al., 2003; Ivey et al., 2013). A wife reported: ‘He just lost it that morning … he tried to smash the windows … it was about $1,500 damage to the car. Then he smashed the TV, he tried to smash the computer…’ (Samia et al., 2012, p. 604). Family carers reported that new behaviours, particularly aggression, became more difficult to understand and address as the person living with dementia gradually deteriorated. A male family carer reflected: ‘It [aggression] was new…I’d never experienced it and so that was something completely new: that was very, very difficult to cope with’ (Stokes et al., 2014, p. 69). Some believed that symptoms were temporary and might disappear over time (Paton et al., 2004).
Other symptoms
The literature mentioned additional symptoms affecting basic activities of daily living, such as eating, hygiene or social engagements. These included risky, strange or embarrassing behaviour (Au et al., 2013; Ducharme et al., 2013), repetitiveness (Au et al., 2013; Farran et al., 2003), agitation (Melunsky et al., 2015; Moore, Ozanne, Ames, & Dow, 2013), confusion (Ducharme et al., 2013; Farran et al., 2003; Oyebode et al., 2013; Stokes et al., 2014), apathy (Gorska et al., 2013; Moore et al., 2013) or passive behaviour (Colling, 2004). Often people living with dementia experienced multiple symptoms, which added to the burden of family carers.
Theme 5: Impact of BPSD on family carers and people with dementia
Findings from the literature suggest that BPSD has a direct cumulative effect on people with dementia and their family carers, affecting matters such as stress, inability to cope (with crises leading to a possible tipping point), isolation or relationship problems.
Tipping point
The experience of BPSD over time can build up tension, desperation and exhaustion in family carers, sometimes reaching a ‘tipping point’ when they cannot cope anymore (Ducharme et al., 2013; Scott et al., 2005; Shaji, Smitha, Lal, & Prince, 2003; Stokes et al., 2014; Toot et al., 2013; Vaingankar et al., 2013). ‘Every day, when I am back home, she calls my name over and over for [the] whole night. How can I bear it? I just put up [with] it’ (Au et al., 2013, p. 1431). This can be the point when family carers seek external support as they feel overwhelmed by the increasing problem behaviours exhibited by the person living with dementia.
Isolation
Family carers’ reports of the impact of BPSD on themselves included loneliness, helplessness, feeling trapped, and being overwhelmed by their role, isolation from friends and family, and reduced social engagement (Samia et al., 2012; Scott et al., 2005; Toot et al., 2013). ‘You become isolated, whether it’s by choice, by design or by exclusion. The exclusion may be friends and relatives who no longer know how to treat you both. You isolate yourselves because of the difficulties in behaviour in going anywhere’ (Stokes et al., 2014, p. 70). Social isolation can lead to family carers feeling alone and disengaged from life outside their home (Farran et al., 2003; Ivey et al., 2013; McHugh, Wherton, Prendergast, & Lawlor, 2012; Stokes et al., 2014).
Other impacts
Further problems comprised stress (Au et al., 2013; Moore et al., 2013; Sun, 2014), sleeping difficulties (Gibson, Gander, & Jones, 2014; Mahoney, La Rose, & Mahoney, 2015; Martin et al., 2013; Samia et al., 2012; Toot et al., 2013), strained relationship with a partner (Malthouse & Fox, 2014; Meyer, Mc Cullough, & Berggren, 2016; Oyebode et al., 2013; Quinn, Clare, & Woods, 2015) and general coping difficulties (Au et al., 2013; Stokes et al., 2014; Wang, Xiao, He, & De Bellis, 2014). Early recognition of BPSD and use of services (Theme 3) and other interventions (Theme 1) may help to manage these problems (Mahoney et al., 2015; Toot et al., 2013).
Discussion
This review highlights the concerns of people with dementia and family carers living at home, in managing BPSD. Through Thematic Analysis of the included papers, important factors were identified for consideration in the management of BPSD. These factors are summarised in five emerging themes, which are interlinked in their description of the complexity and variety of BPSD (see Figure 3). The starting point seems to be the timely initiation and availability of support for people with dementia and their family carers (Themes 1 & 3), although some of this was not always helpful, while for others it was absent altogether (Samia et al., 2012) (Theme 2). While the importance of early recognition of dementia is generally reported in other reviews (e.g. Bunn et al., 2012; de Boer et al., 2007), it appears that the specific challenges of BPSD in the trajectory of dementia have received less attention in the literature. Thus, our review adds to the understanding of a more holistic picture, which emphasises the early diagnosis or recognition of certain behavioural and psychological symptoms. If support is timely and available, the impact of BPSD on the quality of life of people living with dementia and their family carers may be reduced or at least managed appropriately. For example, qualitative studies have indicated that training can help family carers to deal with symptoms early on (see also paper 1, Trivedi et al., 2018). Existing services were not always thought to be well signposted (Gorska et al., 2013), making it difficult to get the right help, such as respite breaks or education.
On the other hand, some family carers appeared to ignore or delay seeking professional help because that might be seen as a ‘defeat’ (Mushi et al., 2014; Oyebode et al., 2013). This may have added further burdens to family carers when trying to cope with the various stressors associated with possible round-the-clock care for a person with dementia. Sleep deprivation is only one of many effects of BPSD on family carers mentioned (Gibson et al., 2014; Mahoney et al., 2015; Martin et al., 2013; Samia et al., 2012; Toot et al., 2013). Family carers experienced a diminished quality of life over time as the dementia progressed, as mentioned in other reviews (Bunn et al., 2012; de Boer et al., 2007), although some family carers adopted strategies to successfully cope with dementia as part of life. Among the qualitative studies reviewed we found indications that family carers and people with dementia would have appreciated professional advice on how to cope with BPSD. Enhancing family carer skills and providing educational support with coping and managing BPSD were reported to be generally the first and most accessible resources for family carers. This finding is supported by some RCT evidence presented in paper 1 (Trivedi et al., 2018), which found that training can help to improve outcomes.
Furthermore, the qualitative literature describes several people who experience a continual build-up of BPSD until crisis point (Ducharme et al., 2013; Scott et al., 2005; Shaji et al., 2003; Stokes et al., 2014; Toot et al., 2013). This was a prominent subtheme of theme 5, interlinking with early recognition of BPSD, impact on family carers and people with dementia and appropriate and timely interventions. These findings lead to some helpful pointers for health and care providers to include family carers in care planning and to ensure that they are supported and educated. Raising awareness of early signs of BPSD may allow a timelier initiation of support for both family carers and people living with dementia.
It seems that there is a limited shared terminology around BPSD between professionals, and between some professionals and family carers (Ducharme et al., 2013; Toot et al., 2013; Xiao et al., 2013). As a result, certain behaviours may not be recognised in time, or their possibility raised by professionals or seen as relevant (Ducharme et al., 2013; Toot et al., 2013; Xiao et al., 2013). Early recognition of BPSD (Theme 3), especially at primary care level, may help family carers get to the right services in time, if they exist. Early support interventions perceived to be of benefit (e.g. reminiscence therapy, music and singing activities or training), might help family carers to cope better with BPSD before they become unmanageable. However, larger studies are required to examine the effects of these perceived supportive interventions on BPSD-related carer burden.
It appeared that professional help was usually not sought until BPSD had become very problematic. Certain symptoms (Theme 4) had greater impact on family carers and people with dementia than others, leading to feelings such as distress, isolation or embarrassment (Theme 5). The qualitative literature most commonly described aggression, strange behaviour, repetitiveness and confusion, while RCTs more often measured depression and anxiety (Trivedi et al., 2018). A few recent reviews have included qualitative data, but they are largely from residential settings. We identified one additional relevant recent qualitative study, which also reported that aggression is the behaviour that gives rise to most concerns (Tyrrell, Hilleras, Skovdahl, Fossum, & Religa, 2017, p. 8). ‘‘On Christmas day he started to kick me and then dragged me by the legs through the house. The beatings started when we were abroad to celebrate our 70th birthdays.’ Some symptoms started in mild form but became more severe as the dementia progressed. Particularly aggression was mentioned by family carers as becoming the breaking point where they needed help. This review highlights that BPSD can be experienced at any part of the trajectory, which needs to be recognised early on, long before the ‘tipping point’ is reached.
Implications for practice
The qualitative literature suggests that some family carers feel that their concerns are dismissed. Improved information, access and education for family carers are likely to be beneficial but the specifics of this vary and at what stages it will prove most useful and effective remain open to question. Qualitative data highlighted possible benefits of assistive technologies in very general terms (Lindqvist et al., 2013; McCabe & Innes, 2013; Meiland et al., 2014; Salfi et al., 2005) or music and singing programmes (Camic et al., 2013; Hamill et al., 2012; McDermott et al., 2014; Osman et al., 2016). For commissioners or service funders there are difficult decisions about how to fund these and other technologies and programmes for symptom management. These decisions may now be better informed by practitioners with specific skills in managing BPSD (collaborative care planning and delivery, specific behavioural intervention protocols with individualised plans, and input from primary care professionals) who can ameliorate behavioural symptoms and improve carer outcomes.
Implications for research
Although there is an increasing body of research around behavioural or distressing problems in people living with dementia, there is not much qualitative data reporting the escalating nature of BPSD that sometimes accompanies the dementia trajectory. Qualitative literature often mentions BPSD in the context of support but not explicitly around diagnosis, so we do not know if and how the subject is potentially raised and why. There is a need for qualitative and quantitative studies that elucidate the recognition of specific BPSD symptoms, such as aggression or agitation, in order to develop timely and workable strategies. This may help family carers to better manage such behaviours, which might delay unwanted moves to care homes. Furthermore, qualitative research usually relates to people who are supported by a carer, most commonly a spouse, but research with minority ethnic groups and those who live alone is less frequently conducted. Nonetheless, the qualitative data show that people will have different needs at different points on the dementia trajectory, which should be considered individually. Adequately meeting the needs of both family carers and people living with dementia is challenging for service providers and what works should be investigated further.
Strengths and limitations of the review
In order to identify all available studies, systematic and rigorous methods for reviewing qualitative literature were used to synthesis views about BPSD management. Although in this process some studies may have been overlooked, our comprehensive approach identified relevant studies. In furtherance of managing the literature, we prioritised contextually rich papers for verification of our results and we reached thematic saturation. We did not exclude studies from our review on grounds of quality, but we attempted to ‘weight’ studies by giving greater prominence in our analyses to qualitative studies that scored highly for both reliability and usefulness. All participants in the reviewed studies were recruited through services and had already received a diagnosis; less is known about those who have not sought help and how their BPSD are interpreted and potentially come to the attention of others.
Despite the inherent complexity of BPSD management, and the limitations of our study, qualitative evidence highlights the potential benefit to people living with dementia and family carers of some interventions and their barriers that need to be addressed in their uptake and funding.
Conclusions
This paper has reported on qualitative studies, mainly interviews, with family carers of people with dementia living in their own homes and how BPSD affected them and the person for whom they were caring. The literature mentioned BPSD in the context of dementia, but it is not always explicitly clear whether BPSD or dementia was recognised. There remains a lack of clarity around definitions of BPSD and approaches to effective management. This review found that for family carers aggression is often reported a problem. Most research has so far focused on people with mild-moderate dementia, and some addressed the ‘tipping points’ that arise when family carers feel they can no longer live with the person with dementia’s BPSD. The inability to cope with dementia and the relating escalating nature of the symptoms pose great challenges for both family carers and the person living with dementia.
GPs are usually the first point of contact, but they are sometimes thought to fail to perceive the extent of the difficulties people living with dementia experience and therefore support may not be offered early enough. For some family carers support is not acceptable. This review provides a comprehensive account of the management of BPSD as portrayed in the qualitative studies, which consisted of five main aspects: interventions, barriers to interventions, recognition of symptoms, the effect of symptoms on people with dementia, and on family carers. The study findings, therefore, provide a benchmark for practice, local dementia specific commissioning decisions and research.
Supplemental Material
Box A Example of Search Query -Supplemental material for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 2. A systematic review of qualitative studies
Supplemental material, Box A Example of Search Query for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 2. A systematic review of qualitative studies by Andreas Braun, Daksha P Trivedi, Angela Dickinson, Laura Hamilton, Claire Goodman, Heather Gage, Kunle Ashaye, Steve Iliffe and Jill Manthorpe in Dementia
Supplemental Material
Supplementary Table S1 Details of included qualitative studies -Supplemental material for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 2. A systematic review of qualitative studies
Supplemental material, Supplementary Table S1 Details of included qualitative studies for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 2. A systematic review of qualitative studies by Andreas Braun, Daksha P Trivedi, Angela Dickinson, Laura Hamilton, Claire Goodman, Heather Gage, Kunle Ashaye, Steve Iliffe and Jill Manthorpe in Dementia
Supplemental Material
Supplementary Table S2 Quotations to support themes -Supplemental material for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 2. A systematic review of qualitative studies
Supplemental material, Supplementary Table S2 Quotations to support themes for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 2. A systematic review of qualitative studies by Andreas Braun, Daksha P Trivedi, Angela Dickinson, Laura Hamilton, Claire Goodman, Heather Gage, Kunle Ashaye, Steve Iliffe and Jill Manthorpe in Dementia
Footnotes
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Acknowledgements
We are grateful to Dr Jennifer McLaughlin who conducted the initial screening, data extraction and quality assessment, the project steering group and Reinhard Wentz who conducted the initial searches.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference Number RfPB PB-PG-0211-24078).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.