
Abstract
Background
Two-thirds of people living with dementia live at home in the UK and many experience distressing behavioural and psychological symptoms. This systematic review evaluates the effectiveness of non-pharmacological interventions for behavioural and psychological symptoms among community-dwelling people living with dementia.
Methods
This two-stage review undertook an initial mapping of the literature followed by a systematic review of relevant randomised controlled trials. We searched electronic databases for pertinent studies reporting outcomes from interventions from January 2000 to March 2015 and updated searches in October 2016. We included studies that considered behavioural and psychological symptom management for older people living with dementia who live at home and excluded studies conducted in long-term care settings. This paper presents findings from a narrative synthesis of 48 randomised controlled trials evaluating interventions for people living with dementia alone, family carers alone and patient-carer dyads.
Results
We retrieved 17,871 de-duplicated records and screened them for potential inclusion. Evidence from 48 randomised controlled trials suggests that family carer training and educational programmes that target problem behaviours and potential triggers can improve outcomes. Nurses and occupational therapists appear to help people with dementia with behavioural and psychological symptoms, but professional comparisons are lacking and there is no shared language about or understanding of behavioural and psychological symptoms amongst professionals, or between professionals and family carers.
Conclusions
Future research should focus on the effectiveness of components of multi-faceted programmes and their cost effectiveness and include qualitative data to better target interventions for behavioural and psychological symptoms. It is important to consider family carer readiness to use non-pharmacological strategies and to develop a shared language about the inherent needs and communications of behavioural and psychological symptoms.
Keywords
Background
Two-thirds of people living with dementia in the United Kingdom (UK) live at home and most experience non-cognitive behavioural and psychological symptoms of dementia (BPSD). These symptoms may result in distress, increased service use and an unwanted move to a care home (Robinson et al., 2006; Savva et al., 2009).
Whilst the term ‘challenging behaviour’ incorporates other terms used previously such as behavioural disturbance, problematic behaviours, behavioural problems and difficult or distressing behaviour (Krishnamoorthy & Anderson, 2011), the term BPSD is still widely used in clinical settings and research (Kales, Gitlin, & Lyketsos, 2015). It is conceptually linked to challenging behaviour, as these symptoms often result in behaviour that presents others with challenges. It is important to stress that the presence of a range of symptoms and behaviours that are hard to manage for family carers and practitioners alike are invariably a way that the person with dementia communicates unmet needs (James & Jackman, 2017).
Symptoms include depression, psychosis, aggression, wandering or walking, agitation, apathy and emotional distress. These can limit the ability to sustain everyday activities and reduce quality of life (QoL) for all those affected (Kales et al., 2015). They can cause or exacerbate sleep deprivation, fatigue and eating problems (Manthorpe & Watson, 2003; Watson & Green, 2006).
The National Dementia Strategy in England (Department of Health, 2009) highlighted the need for more community-based personal support, reduced use of antipsychotic medication and alternative approaches to the support and management of BPSD. Most research has focused on long-term or mixed settings (Forbes et al., 2009; Livingston, Johnston, Katona, Paton, & Lyketsos, 2005; Logsdon, McCurry, & Teri, 2005; Robinson et al., 2006; Verkaik, van Weert, & Francke, 2005; Vernooij-Dassen, Draskovic, McCleery, & Downs, 2011; Woods, Spector, Jones, Orrell, & Davies, 2005) or on a narrow range of interventions or symptoms (Forrester et al., 2014; Livingston et al., 2014; Orgeta, Qazi, Spector, & Orrell, 2014; Reilly et al., 2015) and there is limited evidence-based guidance for managing BPSD at home. A rapid systematic overview of BPSD management (Dickson et al., 2012) was limited only to reviews, included many settings and did not evaluate primary studies.
A recent consensus narrative review of pharmacological and non-pharmacological management of BPSD covered various settings but did not employ rigorous systematic review methodology (Tible, Riese, Savaskan, & von Gunten, 2017).
This present paper systematically reviews the evidence from randomised controlled trials (RCTs) of effectiveness of interventions for BPSD specifically for community dwelling older people living with dementia. An accompanying paper examines studies reporting the views and experiences of people living with dementia and their family carers, on managing BPSD (Braun et al., 2018).
Methods
We invited 25 health and social care practitioners, researchers and carers of people living with dementia to a preliminary stakeholder meeting to gain their perspectives around managing BPSD at home and to inform the focus of the review (how BPSD is defined, search terms, challenges for family carers and strategies for support at home). A broad mapping of the literature on BPSD interventions identified studies for inclusion in an in-depth review and was followed by a systematic review of included quantitative and qualitative literature. Only evidence from RCTs is reported in this paper. The study protocol is available (Trivedi et al., 2013). Findings from the review were later discussed with people living with dementia, family carers and service providers at the end of the study.
Selection criteria
We included English language studies that investigated BPSD management in community-dwelling individuals and excluded studies set in long-term care facilities.
Search strategy
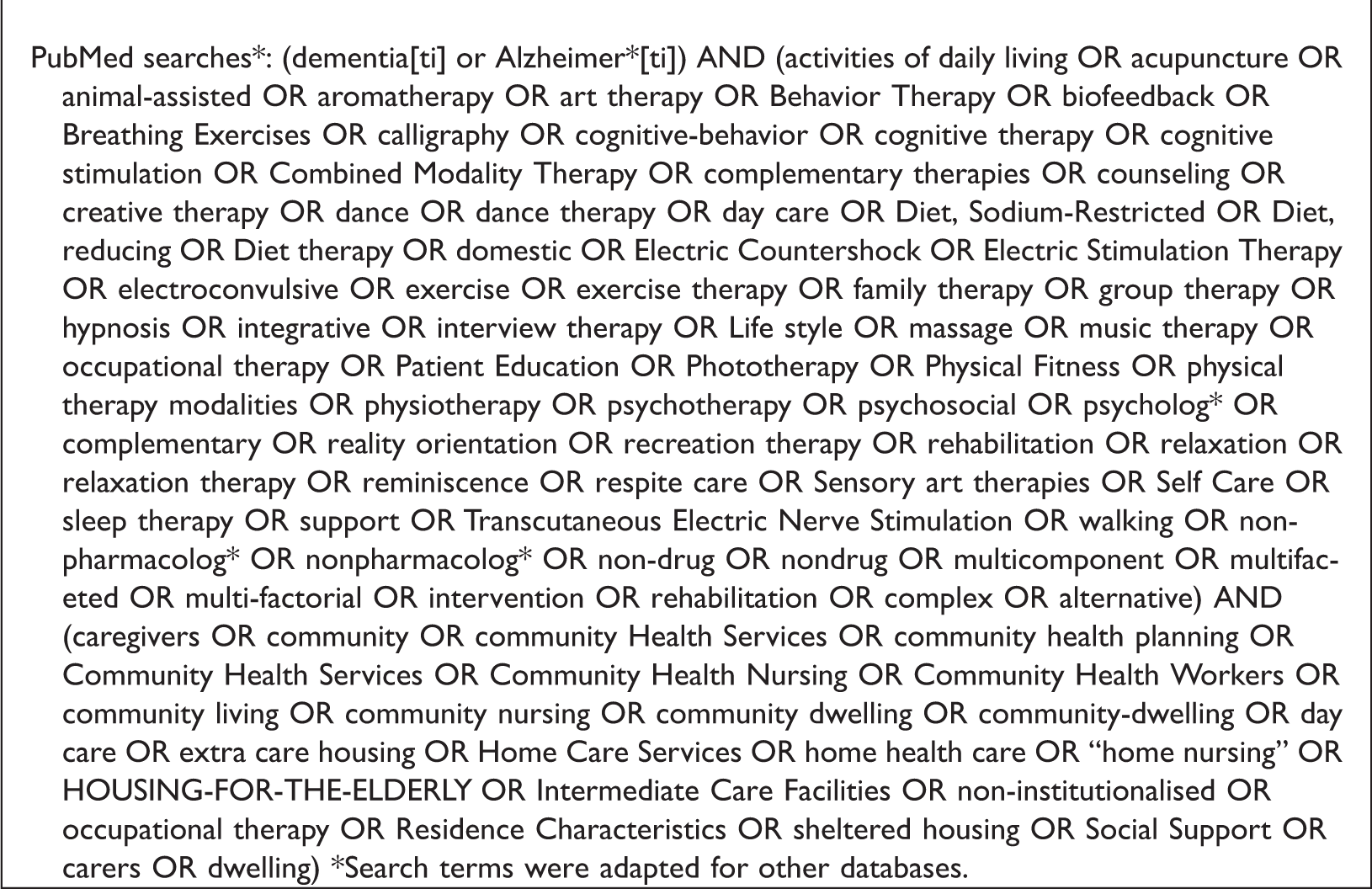
Studies were identified by computerised searches of PubMed, Embase, CINAHL, PsycInfo, AMED, HMIC, BNI, HEALTH BUSINESS ELITE, Scopus and Web of Knowledge (Web of Science). In addition, we searched the Cochrane Library (including Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, Health Technology Assessment, Economic, Systematic reviews, Trials, Method, Techno). We carried out lateral searches (checking reference lists and citation searches) and screened several reviews to identify other relevant studies. An example search query from PubMed is presented in Box 1. Searches were conducted in October/November 2012 from year 2000, with two updates (March 2015 and October 2016). The broad mapping informed the selection of studies for our in-depth systematic review, through applying additional criteria and assessing the focus of complex interventions and BPSD relevant outcomes.
Screening for inclusion in systematic review
All records from searches were retrieved in Endnote and screened for potential inclusion; 10% were independently screened by two reviewers. Hard copies of potentially relevant papers were further screened, with 20% screened independently. Studies included were RCTs describing interventions for BPSD and reporting one or more of the following as main outcomes: BPSD and QoL for people with dementia, and carer burden/strain, distress, psychological health and QoL for carers. Secondary outcomes included resource use and costs and processes of care. Uncertainties were resolved by consensus in discussion by the research team.
Data extraction and quality assessment
All quantitative data were extracted into an Excel database, using a pre-piloted data extraction tool developed in consultation with our study’s lay advisers. This included participant characteristics, intervention details, providers, clinical outcomes, resource use, costs (where available) and effect sizes. Key outcome and descriptive data for reviewing economic implications were extracted independently (HG). Data were extracted by one reviewer, with 70% extracted independently by two reviewers for in-depth systematic review. Quality assessment was conducted on all included studies independently by two reviewers using the Cochrane risk of bias tool for RCTs (Higgins & Green, 2011). Categories for seven types of non-pharmacological interventions were based on a broad classification used in the earlier review (Dickson et al., 2012), namely: behavioural, education and training, environmental, multi-component, organisational, physical and structured and support types of interventions.
Analysis and synthesis
Due to the heterogeneity of people living with dementia, follow-up periods and their outcomes, an overall meta-analysis was not considered appropriate and data are presented narratively supported by evidence tables. Findings are discussed by categories of intervention offered to people living with dementia alone, to dyads (people living with dementia and family carers) and to family carers alone.
Results
Evidence mapping
We retrieved 17,871 de-duplicated records. Following screening, 301 records were selected (all study types) for an initial mapping exercise (Trivedi et al., 2015). Records retrieved and screened for final inclusion of quantitative studies are shown in Figure 1. Non-pharmacological interventions identified were heterogeneous, with over 50 different formats of varying content and duration. A range of different terminologies was used to describe BPSD, and the evaluations were based on a variety of different outcomes and instruments. The interventions targeted people living with dementia and family carers, were delivered at home or in community or out-patient settings and were often multi-faceted and multidisciplinary. Many studies addressed symptoms as one component of a complex intervention for dementia (including behavioural management, various types of support, education and training) whilst others did not specifically target BPSD but reported BPSD-relevant findings as secondary outcomes. Findings from the analysis of 48 RCTs where BPSD management was one of the components of the intervention and reported BPSD as either a primary or secondary outcome are reported in this paper.
PRISMA flow diagram of RCT study selection process.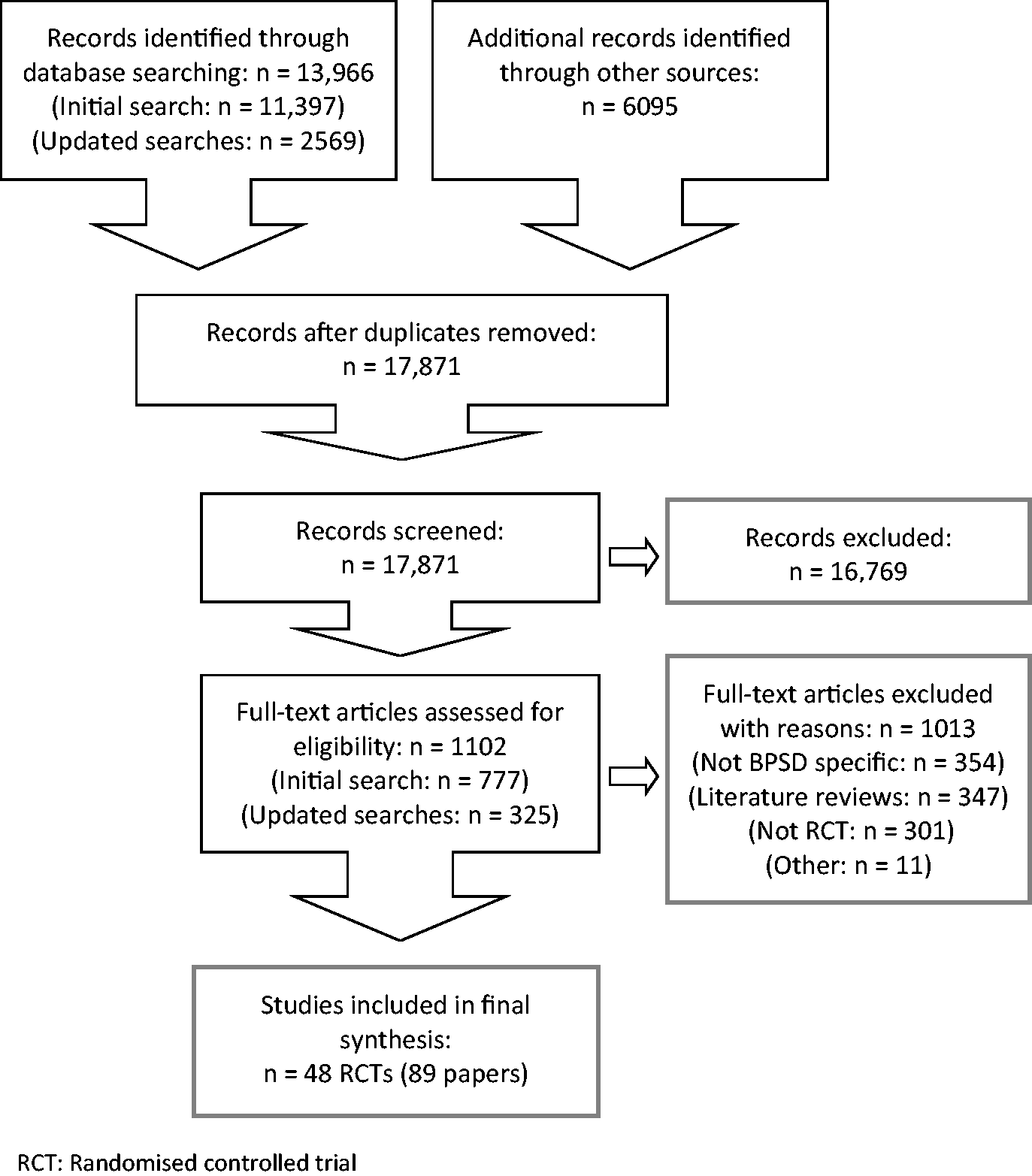
Example of search query.
Evidence synthesis
Due to the heterogeneity of interventions, outcomes and follow-up, a narrative synthesis was constructed according to the ‘target’ group (interventions offered to people living with dementia alone, to dyads (people living with dementia and family carers) and to family carers alone and broad intervention groups and outcomes.
Seven studies (10 papers) reported evidence on interventions that focused on people living with dementia only, 18 studies (33 papers) on dyads and 23 studies (46 papers) related to family carers only. Studies took place in the United States (US) (n = 27), mainland Europe (n = 7), United Kingdom (UK) (n = 6), Japan (n = 2), Hong Kong (n = 3); one report came from a collaborative UK/US/Australia study, one from Canada and one from a joint Russia/Peru study. Most studies targeted the mild-moderate stages of dementia and included all dementia types. The quality of the studies was mixed, with 20 having low risk of bias (ROB) (5 or more domains of low or good quality); 8 low/unclear risk (4/6 domains of low or moderate quality), 15 unclear and 5 at high risk. They used various instruments for BPSD-related outcomes, most validated or based on previous research. Less than half the studies reported theoretical frameworks. Details of these and effect sizes are shown in evidence Tables S1 to S3 (see supplementary tables). Comparison groups mostly included ‘usual care’ or interventions that did not include specific components of a complex intervention.
Interventions for people with dementia (supplementary evidence Table S1)
Interventions for people living with dementia alone are shown in Evidence Table S1. Evidence of the effectiveness of interventions (from seven small studies) was weak with unclear or high risk of bias (overall low quality). Providers and duration of interventions varied and included intensive sessions with trained individual or group therapists with short-term follow-up. Tadaka and Kanagawa (2007) reported reductions in withdrawal and disorientation in people with vascular dementia. In another study, participants with mixed dementia in the early stage were likely to engage well in mentally stimulating activities to reduce apathy and depression (Buettner, Fitzsimmons, Atav, & Sink, 2011; Fitzsimmons, Barba, & Stump, 2014). Likewise, multisensory stimulation, such as Snoezelen seemed to help people with dementia be more attentive to environment and improved mood (Baker, Holloway, et al., 2003; Baker, Wareing, et al., 2001), but larger studies are required to examine its effect on agitation in community dwelling older people (Baillon et al., 2004; van Diepen et al., 2002). Other interventions, such as art therapy and multimodal interventions (Taiji, cognitive therapy with support) may reduce apathy and improve QoL (Hattori, Hattori, Hokao, Mizushima, & Mase, 2011; Lam, Lui, et al., 2010) and improve mental stability (Burgener, Yang, Gilbert, & Marsh-Yant, 2008), but larger high-quality studies with longer follow-up are required to establish effectiveness.
Interventions for dyads (supplementary evidence Tables S2.1–2.2)
We identified 18 relevant dyadic interventions (targeted at both people living with dementia and family carers) of which only 10 were of good quality and four were of moderate quality; the interventions are described in detail in Table S2.1 and the outcomes in Table S2.2.
Mode of intervention involved individual or group sessions, home or clinic visits or telephone sessions or in combination. The intensity, duration and follow-up varied across all studies. The number of sessions of interventions varied from brief (<6 sessions, n = 5), to medium (around 8–14 sessions, n = 10) and long (≥16 n = 3); follow-up periods varied from short (≤6 months, n = 9) to longer term (>6 months, n = 9). Duration of interventions ranged from less than 8 weeks to over 12 months or for duration of the study.
Behavioural interventions
Person living with dementia outcomes
Of four dyadic studies (Burns, Nichols, Martindale-Adams, Graney, & Lummus, 2003; Gormley, Lyons, & Howard, 2001; Spector, Charlesworth, et al., 2015; Spector, Orrell, et al., 2012; Teri et al., 2000; Weiner et al., 2002), one good quality pilot study from the UK reported that cognitive behavioural therapy (CBT) (10 weekly one-hour sessions) can improve anxiety and may be cost neutral (Spector, Charlesworth, et al., 2015), although substantial family carer involvement in the earlier stages of dementia might be required.
Carer outcomes
Only one study (with unclear risk of bias) that largely included people living with severe dementia reported improved long-term psychological health for family carers but the study had high attrition (Burns et al., 2003). The intervention included managing patient behaviour together with family carer stress management and coping with specific behaviours. Another less intensive programme showed no effect on patient or family carer outcomes (Teri et al., 2000; Weiner et al., 2002).
Education and training
Four psychosocial education and training interventions ((1) Belle et al., 2006; Nichols et al., 2008, (2) Gitlin, Winter, Dennis, Hodgson, & Hauck, 2010a, (3) Gitlin, Winter, Dennis, Hodgson, & Hauck, 2010b; Gitlin, Winter, Dennis, & Hauck, 2007; Gitlin & Rose 2016) and (4) Judge, Yarry, Looman, & Bass, 2012; Judge, Yarry, & Orsulic-Jeras, 2010) were included.
Person living with dementia outcomes
Evidence from two good quality US studies suggests that training family carers to support people living with dementia’s capabilities by reducing environmental stressors, and enhancing family carers’ psychosocial skills, had no effect on agitation or QoL, but improved engagement and functional dependence at four months’ follow-up, although not in the longer term (Gitlin et al., 2010a). Advancing caregiver training (ACT) to target problem behaviours and potential triggers can improve problem behaviour in the short term (Gitlin et al., 2010b).
Carer outcomes
ACT can also reduce family carer burden and upset (Gitlin et al., 2007; Gitlin et al., 2010b). Carer readiness to use non-pharmacological strategies predicts BPSD outcomes. ‘Activated’ family carers (those actively using intervention strategies) reported greater reduction in distressing behaviours than non-activated participants, although activation did not predict family carer burden or well-being (Gitlin & Rose, 2016). These interventions were intensive, used telephone calls for maintenance, and involved ‘advanced practice’ nurses and occupational therapists (OTs).
Another intervention trained mental health professionals in systematic assessment of family carers’ competencies and in strategies to deal with a range of problems that predict moves to long-term care. There was no effect on any patient or family carer outcomes at 12 months, but results showed family carers treated by professionals adhering to the intervention protocol had a better sense of competence, suggesting that intensity and adherence can influence outcomes (Spijker, Teerenstra, et al., 2013; Spijker, Verhey, et al., 2009; Spijker, Wollersheim, et al., 2011).
Multicomponent interventions
Two good quality studies from the US and Denmark involved multifaceted Alzheimer’s disease programmes for dyads, which included home-based exercise with behavioural management and multifaceted semi-tailored counselling, information and support programmes, respectively.
Person living with dementia outcomes
Intensive behaviour management aiming to improve patient–carer interactions, affect and behavioural distress can improve depression and reduce moves to a long-term care facility in people living with moderate to severe dementia (Teri et al., 2003). Intensive counselling and support (>12 months) aiming to prevent depression in people with mixed dementia types had no effect on behaviours or related QoL in the long term (three years), although participants benefitted in coping, competence and seeking further support (Phung et al., 2013; Waldemar et al., 2011; Waldorff et al., 2012; Waldorff, Nielsen, & Waldemar, 2010).
Carer outcomes
These interventions had no significant effect on family carer distress, despite good adherence to programme recommendations and family carers reporting better awareness, ability to cope and seeking appropriate support. Cost implications of intensive sessions of long duration are unclear.
Organisational interventions
Person living with dementia outcomes
Of three dyadic studies (Callahan et al., 2006; Chien & Lee, 2008; Lam, Lee, et al., 2010), one good quality US study suggests that collaborative care planning and delivery using structured behavioural protocols and individualised plans targeting people living with moderate dementia exhibiting symptoms such as repetitive behaviour and aggression can improve BPSD (Callahan et al., 2006) over 18 months. The model aims to identify, monitor and treat BPSD, through behavioural interventions, education on communication skills, coping skills and lifestyle advice. The 12 months intervention had a long follow-up and involved a primary care physician and a geriatric nurse practitioner.
Carer outcomes
Reduced family carer depression and improved quality of care were reported, with increased clinician visits and increased drugs, but without increasing use of antipsychotics (Callahan et al., 2006). In another study (moderate quality), OTs working as case managers improved family carers’ psychological health and increased their use of external support (Lam, Lee, et al., 2010). This involved regular home and out-patient visits and telephone calls over 12 months. The model included mobilisation and optimum use of local services in addition to advice on coping, skills training and behavioural management. The strength of these interventions lies in the comprehensive and integrated approaches with designated care/case managers and individual targeting of problem behaviours.
Physical and structured interventions
Person living with dementia outcomes
Of three dyadic studies, one (moderate quality pilot study) showed that tailored activity programmes (TAP) delivered by OTs (six 90-minute home visits, two telephone sessions over four months) can improve engagement and reduce shadowing, repetitiveness and agitation (Gitlin et al., 2008; Gitlin et al., 2009), although a larger trial is required to confirm the reported benefit. There is no evidence from two good quality studies that prescribed exercise or sleep therapy is effective for BPSD, although better adherence can reduce time awake ((1) Cerga-Pashoja et al., 2010; Lowery et al., 2013 and (2) McCurry et al., 2011; McCurry, Gibbons, Logsdon, Vitiello, & Teri, 2005; McCurry, Logsdon, Gibbons, Vitiello, & Teri, 2003).
Carer outcomes
TAPs can improve family carer objective burden and skills, with good understanding of strategies by dyads but larger studies are required (Gitlin et al., 2008).
Support interventions
Person living with dementia outcomes
One good quality study from UK, US and Australia of dyads showed that tailored individual and family counselling for emotional support combined with drug treatment had no effect on problem behaviours at 24 months. The study was not, however, adequately powered to measure this change (Mittelman, Brodaty, Wallen, & Burns, 2008).
Carer outcomes
The intervention reduced family carer depression and distress when the people living with dementia were taking Donepezil. This effect was maintained over two years. The counselling occurred in the first three months and was followed by continuous available telephone counselling on demand over 24 months duration. Although costs are not reported, the authors refer to the intervention’s costs as ‘modest’.
Interventions for family carers alone (supplementary evidence Tables S3.1–3.2)
Of 23 studies directed at family carers alone, 10 were of good quality, three were of moderate quality and the rest were unclear or of low quality. For family carer interventions, the number of sessions and duration of interventions varied from brief (<6 sessions, n = 5), to medium (around 8–14 sessions, n = 9), to long (≥16 sessions weeks, n = 9); and follow-up periods varied from short (≤6 months, n = 11) to longer term (>6 months, n = 12) (Evidence Table S3.2 reports studies by intervention whilst Table S3.3 shows outcomes).
Behavioural interventions
One moderate quality study evaluating intensive CBT-based telephone intervention (TeleTanDem) focused on managing behavioural problems, promoting competence and coping strategies for challenging behaviour, personality changes of care recipient, enhancing coping skills for reducing social isolation and help with accessing professional and informal support. This 12-week intervention reduced family carer depression but with no effect on QoL. However, it did not specifically target clinically depressed family carers (Schinköthe & Wilz, 2014; Wilz, Schinköthe, & Soellner, 2011; Wilz, Meichsner, & Soellner, 2016; Wilz & Soellner, 2016).
Education and training
Sixteen studies evaluated education and training programmes targeted specifically at family carers. These included six psychoeducational ((de Rotrou et al., 2011), (Gallagher-Thompson et al., 2003; Gallagher-Thompson, Gray, Dupart, Jimenez, & Thompson, 2008), (Gallagher-Thompson et al., 2010), (Buckwalter, Gerdner, & Kohout, 1999; Gerdner, Buckwalter, & Reed, 2002; Garand, Buckwalter, & Lubaroff, 2002), (Hebert et al., 2003) and (Martin-Carrasco et al., 2009)), six psychosocial ((Burgio, Stevens, Guy, Roth, & Haley, 2003), (Czaja, Loewenstein, Schulz, Nair, & Perdomo, 2013), (Farran et al., 2004; Farran et al., 2007), (Moniz-Cook et al., 2008), (Tremont et al., 2014; Tremont et al., 2013; Tremont, Davis, Bishop, & Fortinsky, 2008) and (Ulstein, Sandvik, Wyller, & Engedal, 2007)) and four other training programmes ((Gavrilova et al., 2009; Guerra, Ferri, Fonseca, Banerjee, & Prince, 2011), (Hepburn, Tornatore, Center, & Ostwald, 2001; Ostwald, Hepburn, & Caron, 1999), (Teri, McCurry, Logsdon, & Gibbons, 2005; Logsdon et al., 2005) and (Wright, Litaker, Laraia, & DeAndrade, 2001)).
Evidence from seven good quality family carer studies suggests that psychoeducation programmes focusing on problem solving techniques, emotion-centred coping (de Rotrou et al., 2011), enhancing skills in handling disruptive behaviours, cognitive appraisal with coping strategies (Hebert et al., 2003) and identifying triggers, planning to manage as symptoms change and ‘anticipating’ stressful situations (Gallagher-Thompson et al., 2008) improve family carer health including depression, distress and reactions to disruptive behaviours. Psychosocial interventions report that enhancing behaviour management skills reduced emotional stress related to agitated behaviours over 18 months (Farran et al., 2004). The intervention involved 12-weekly sessions (group and individual) with booster sessions and ‘as needed’ telephone calls over 12 months.
Intervention training for community mental health nurses (CMHN) (Moniz-Cook et al., 2008) improved coping with problem behaviours, although long interventions are required. CMHNs received both group and individual in-service supervision sessions, weekly, fortnightly and then monthly over 18 months. This study suggests that the intervention effect depended on the CMHN who delivered it. Highly accessible, intensive telephone contacts of longer duration between therapists and family carers and potentially low-cost interventions to enhance coping reduced family carer depression and improved reactions to care recipient behaviours at six months (Tremont et al., 2014).
Training community consultants (master’s level healthcare professionals) to teach family carers behavioural management plans was found to improve both behaviours and carer burden, depression and reactions to behaviours at six months following a brief intervention (Teri et al., 2005).
Environmental interventions
One good quality US study examining home environment skill-building interventions (Gitlin, Corcoran, Winter, Boyce, & Hauck, 2001; Gitlin et al., 2003; Gitlin, Hauck, Dennis, & Winter, 2005) aimed to help family carers develop a supportive environment which reduced disruptive behaviours and functional decline. The intervention involved intensive training by OTs, home visits and telephone contacts. It reduced family carer burden and enhanced carer well-being, sustaining carer affect over a year but was resource intensive. More frequent professional contact and ongoing skills training may be necessary to maintain other important outcomes such as reduced carer distress in managing problem behaviours. Although the intervention can be adapted to other cultural/ethnic groups, more work is required on level of intensity and on dyad interactions, according to the researchers. People in the severe stage of dementia are not likely to benefit from this type of intervention, in the researchers’ view.
Multi-component interventions
REACH carer interventions (Resources for Enhancing Alzheimer’s Caregiver Health) from various sites in the US aimed to assist family carers to manage disruptive behaviours in care recipients. They were overall intensive, with long durations and of unclear risk of bias. They offered multiple components which included behaviour management, stress-coping mechanisms, family-based therapy with access to community support, telephone systems and skills training. Evidence from REACH studies suggests that family therapy using computer-mediated automated interactive voice response targeted at culturally different groups in five US sites has the potential to reduce ‘bother’ and upset about BPSD and carer depression (Eisdorfer et al., 2003; Elliott, Burgio, & Decoster, 2010; Mahoney, Tarlow, & Jones, 2003; Mahoney, Tarlow, Jones, Tennstedt, & Kasten, 2001). Wives who exhibited low mastery and high anxiety benefitted most from the automated telecare intervention. Differential responses to psychosocial interventions according to race and relationship to care recipients may be important (Burgio et al., 2003; Czaja et al., 2013). Although the effects of racial or ethnic concordance between carers and interventionists on carer depression and burden were not significant, they need to be examined systematically in further studies (McGinnis et al., 2006). Offering multiple components with flexibility for participants to choose component, frequency, duration and timing appears to be important. No costs are reported.
REACH II offered skills training, systematically targeting problem areas, in-home family therapy, access to resources for managing BPSD and engagement with family carers in the intervention process (see Evidence Tables S2.1–2.2, S3.1–3.2). Whilst it reported positive benefits for family carers from ethnically diverse populations, particularly when outcome domains were closely linked to intervention components (Belle et al., 2006), it was resource intensive. However, the intervention significantly reduced family carer hours per day compared with controls at one site (Nichols et al., 2008).
Clinical application and implementation of the REACH II programme in the US Veterans health care system resulted in positive family carer benefits (Nichols, Martindale-Adams, Burns, Graney, & Zuber, 2011), although REACH studies were of mixed quality and involved intensive individualized home visits and telephone sessions. The implementation programme was structured and individualized through risk assessment, targeted education, support and skills training to address family caregiving risk areas of safety, social support, problem behaviours and management of depression (Belle et al., 2006; Martindale-Adams, Nichols, Burns, Graney, & Zuber, 2013).
Support interventions
Of four family carer studies ((1) Knapp et al., 2013; Livingston et al., 2013, (2) Mittelman, Haley, Clay, & Roth, 2006; Mittelman, Roth, Clay, & Haley, 2007; Mittelman, Roth, Coon, & Haley, 2004; Mittelman, Roth, Haley, & Zarit, 2004, (3) Martindale-Adams et al., 2013 and (4) Pillemer & Suitor, 2002), the ‘Strategies for relatives’ programme (START) manual based coping support included psychoeducation, counselling, relaxation, behaviour management for carers with high burden improved carer mood (depression and anxiety) and reported less abusive behaviour of family carers towards care recipients (Livingston et al., 2013). Eight sessions were delivered over 8–14 weeks during eight months’ follow-up. An economic evaluation showed that START had a greater than 99% chance of being cost effective compared with usual treatment alone, at a willingness to pay threshold of £30,000 per Quality Adjusted Life Year gained, and a high probability of cost effectiveness in reducing anxiety and depression (Knapp et al., 2013; Livingston et al., 2013).
Enhanced counselling and support for family members (involving regular sessions with carers and a family support group of unlimited sessions with ad-hoc counselling available over a long follow-up period) can lead to sustained benefits in reducing carer depression and less than half as many nursing home placements compared with usual care (Mittelman et al., 2006; Mittelman et al., 2007; Mittelman, Roth, et al., 2004; Mittelman, Roth, Haley, et al., 2004). The authors suggest that in order to be maximally effective, structured components of longer duration should be widely available to provide effective, evidence-based interventions for family carers.
Overview
Intensity, duration and follow-up varied across all studies. Of the better quality studies, those that delivered more than 8–14 sessions of longer duration (over 16 weeks or more) reported one or more positive outcomes for person living with dementia and family carers. These included psychosocial dyadic and carer interventions environmental, multicomponent dyadic and carer interventions, REACH studies, collaborative care and case management, physical and structured dyadic support, e.g. OT-led interventions; supportive dyadic and carer interventions such as counselling with behaviour management plus long-term follow-up. Examples of brief sessions but given over longer duration which improved one or more outcomes include CBT and psychosocial skills programme. Follow-up periods varied, although many of these had six months or more follow-up periods. However, cost implications are not known. Although most papers described (to some extent) the resources involved in delivering the interventions (staffing, number of sessions, facilities and materials), these were rarely converted to a cost.
Other lesser or unclear quality studies targeted at dyads or family carers suggest a few potentially effective interventions, such as family interventions targeted for diverse low/middle income settings using existing resources (Gavrilova et al., 2009; Guerra et al., 2011), culturally sensitive models using case managers (Chien & Lee, 2008), acquiring new skills whilst enhancing strengths (Judge et al., 2012; Judge et al., 2010), and intensive targeted behaviour programmes with triggers for coping with BPSD and family carer strategies (Burns et al., 2003; Martin-Carrasco et al., 2009). Less intensive behaviour and educational programmes showed no effect (Garand et al., 2002; Gerdner et al., 2002; Gormley et al., 2001; Ulstein et al., 2007), whereas other low-quality studies of skills training and peer support gave mixed results (Hepburn et al., 2001; Pillemer & Suitor, 2002; Wright et al., 2001). Larger good quality evaluations are required to establish effectiveness, cost implications and their applicability.
Discussion
We evaluated evidence from 48 RCTs describing seven broad groups of non-pharmacological interventions that addressed the management of BPSD for both people living with dementia and their family carers living in the community. We synthesised the evidence according to intervention types, target groups and outcomes for persons living with dementia and family carers. The literature highlights the multiplicity of terms and tools used to describe and measure BPSD as well as multiple components of interventions and programmes. By considering broad groups of interventions, their key characteristics and delivery and relevant outcomes in target groups, we offer a way of evaluating effectiveness of differing interventions for a complex range of behaviour changes and symptoms. Evidence supports the development of multi-faceted interventions that include enhancing family carer skills and educational support for them in coping and managing BPSD.
Helping family carers through efforts such as training to focus on problem behaviours and potential triggers (anticipate stressful situations) and helping them to plan to manage changing symptoms is important in developing effective interventions (Gitlin et al., 2007; Gitlin et al., 2010b). Furthermore, family carers’ level of readiness to engage in such activities impacts on behavioural symptom outcomes (Gitlin & Rose, 2016) and it is important to consider this. Programmes involving trained health professionals to provide highly accessible and potentially low-cost interventions to enhance coping can be effective. Whilst training professionals can improve family carer competence, intervention effects are influenced by adherence to protocol (Moniz-Cook et al., 2008; Spijker, Teerenstra, et al., 2013; Spijker, Wollersheim, et al., 2011).
Behavioural interventions such as CBT require high-quality adequately powered studies to confirm their effectiveness for dyads and family carers. Multicomponent programmes that include intensive counselling, support and behavioural management can improve family carer outcomes (REACH studies; Mittelman et al., 2006). High levels of OT input in organisational interventions (such as integrated care with case management) mobilising access to support, as well as physical and structured tailored activity programmes, have the potential to reduce BPSD. However, cost implications of long, intensive interventions delivered by nurses and OTs are unclear.
Recent reviews have included mixed or long-term settings and many studies of the of BPSD focus on one type of intervention or symptom, or on a narrow range of either (Brasure et al., 2016; Forrester et al., 2014; Holle et al., 2016; Livingston et al., 2014; Orgeta et al., 2014; Vernooij-Dassen et al., 2011; Reilly et al., 2015; van der Steen et al., 2017). A recent overview of systematic reviews also highlighted the heterogeneity of non-pharmacological interventions, but it was limited only to systematic reviews in mixed settings and did not evaluate primary studies (Abraha et al., 2017).
Our up-to-date evidence synthesis describes the effectiveness of support for people with dementia living at home with a diverse collection of distressing behaviours. It complements other overviews that emerged during the course of our study (e.g. Laver, Clemson, Bennett, Lannain, & Brodaty, 2014). Our review adds to knowledge with its synthesis of evidence on a broad group of interventions. Despite the large volume of research, this review demonstrates the lack of clarity around what BPSD entails or the diverse behaviours that it can encompass, as highlighted by our preliminary stakeholder consultation.
Implications for practice
For commissioners or service funders, there are difficult decisions about how to fund multicomponent programmes for symptom management. These decisions may now be better informed by the evidence that practitioners with specific skills in managing BPSD (specific behavioural intervention protocols with individualised plans and input from primary care professionals) can improve behavioural symptoms and family carer outcomes. It is important to consider family carer involvement and their readiness to participate in such interventions. More evidence is needed about what training and skills development are most cost-effective.
Strengths and limitations of the review
We used systematic and rigorous methods to review RCT evidence. Despite our efforts to identify all available studies, some may have been missed. However, we used a comprehensive approach to ensure that a broad evidence base from the first mapping stage enabled us to select appropriate studies for the evidence synthesis. In order to manage the literature for dyads and family carers, we prioritised RCTs that aimed to address BPSD management as a component of a complex intervention, reported BPSD relevant outcomes and excluded poor quality pilot studies. Our findings might have been less tenuous if we had taken a narrower focus to studies that included only people living with dementia, or only dyads, or only family carers, but this would have excluded many studies and not reflected the heterogeneity of the population.
Several methodological issues may have had an important bearing on the findings of this review. Some studies were of limited quality, with short-term follow-up and high attrition. There was a considerable heterogeneity in interventions and in the measurement of outcomes, making comparisons difficult. The tools for measuring BPSD and related symptoms and family carer outcomes varied across the studies. Although participants’ satisfaction and process measures from several studies and carers’ reports from qualitative studies relating to RCTs were generally reported to be good, with only modest effects on other outcomes, it is possible that the intervention studied was ineffective due to methodological limitations or it may be that these evaluations did not capture the complexity of BPSD. People living with dementia may exhibit more than one symptom and different symptoms may need different treatments or interventions. Not all studies reported their theoretical basis, although some were based on models from previous research. We categorised studies in what we judged to be the main components of non-pharmacological interventions, as defined by previous research. Although we located a broad range of material, we excluded studies that did not specifically address BPSD management in the intervention or did not provide adequate detail for us to judge this. Despite the inherent complexity of BPSD management and the limitations of our study, evidence highlights the benefit to people living with dementia and family carers of some interventions for BPSD management.
The resource implications of delivering interventions (staffing, number of sessions, facilities and materials) varied considerably and were often incompletely reported. Costs were rarely calculated. Future evaluations of interventions would ideally provide robust evidence to funders or service commissioners through a full cost-effectiveness analysis. Where impact on BPSD is incidental rather than the primary outcome and when interventions are multicomponent, issues associated with attributing input to effects need to be considered at the research design stage.
Implications for research
Large-scale complex intervention studies with in-built economic evaluations and long follow-up periods are required to clarify which interventions are effective and cost-effective. Standardisation of definitions and measures of BPSD across the research community including family carer perspectives would aid better targeting of interventions and aid meta-analysis of data. Research should also explore the components of multifaceted interventions that contribute to effectiveness for both people living with dementia and family carers, as well as examining intensity, dose, duration and format of effective interventions to assess ‘value for money’. Research designs that are more appropriate for complex interventions and examine active ingredients of such interventions need to be developed (Craig et al., 2008).
Future trials should collect qualitative data to explore how to better target interventions and contain a process analysis to identify features of adoption beyond research initiatives. Cultural and linguistic specific interventions may be required to support people from diverse populations. Future research needs to consider the effectiveness of tailoring interventions to improve family carer readiness to use non-pharmacological interventions.
Conclusions
This review identified RCT interventions for the management of BPSD among people living with dementia in the community and evaluated their effectiveness. The study findings provide a benchmark for the development of an evidence base for practice and research.
Supplemental Material
Evidence Table S2.1 Dyads Interventions -Supplemental material for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions
Supplemental material, Evidence Table S2.1 Dyads Interventions for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions by Daksha P Trivedi, Andreas Braun, Angela Dickinson, Heather Gage, Laura Hamilton, Claire Goodman, Kunle Ashaye, Steve Iliffe and Jill Manthorpe in Dementia
Supplemental Material
Evidence table S2.2 Dyads Outcomes -Supplemental material for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions
Supplemental material, Evidence table S2.2 Dyads Outcomes for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions by Daksha P Trivedi, Andreas Braun, Angela Dickinson, Heather Gage, Laura Hamilton, Claire Goodman, Kunle Ashaye, Steve Iliffe and Jill Manthorpe in Dementia
Supplemental Material
Evidence Table S3.1 Carer Interventions -Supplemental material for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions
Supplemental material, Evidence Table S3.1 Carer Interventions for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions by Daksha P Trivedi, Andreas Braun, Angela Dickinson, Heather Gage, Laura Hamilton, Claire Goodman, Kunle Ashaye, Steve Iliffe and Jill Manthorpe in Dementia
Supplemental Material
Evidence table S3.2 Carer Outcomes -Supplemental material for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions
Supplemental material, Evidence table S3.2 Carer Outcomes for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions by Daksha P Trivedi, Andreas Braun, Angela Dickinson, Heather Gage, Laura Hamilton, Claire Goodman, Kunle Ashaye, Steve Iliffe and Jill Manthorpe in Dementia
Supplemental Material
Evidence Table S1 People with dementia -Supplemental material for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions
Supplemental material, Evidence Table S1 People with dementia for Managing behavioural and psychological symptoms in community dwelling older people with dementia: 1. A systematic review of the effectiveness of interventions by Daksha P Trivedi, Andreas Braun, Angela Dickinson, Heather Gage, Laura Hamilton, Claire Goodman, Kunle Ashaye, Steve Iliffe and Jill Manthorpe in Dementia
Footnotes
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Acknowledgements
We are grateful to Dr Jennifer McLaughlin who conducted the initial screening, data extraction and quality assessment, the project steering group and Reinhard Wentz who conducted the initial searches.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference Number RfPB PB-PG-0211–24078).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.