
Abstract
Dementia accounts for one in three deaths among people aged 65 and over, but end-of-life care for people with dementia is often sub-optimal. Palliative care for people with dementia poses particular challenges to those providing services, and current policy initiatives recommend education and training in palliative care for those working with patients with dementia. However, there are few evaluations of the effectiveness of dementia education and training. This paper presents a narrative review undertaken in 2011–2012 of evaluations of palliative care education for those working with people with dementia at the end of life. A total of eight papers were identified that described and evaluated such palliative care education; none reported benefits for people with dementia. There is a clear need to develop and evaluate educational interventions designed to improve palliative and end-of-life care for people with dementia. Some suggestions for educationally sound approaches are discussed.
Introduction
Palliative or end-of-life care for people with dementia is emerging as a healthcare priority (Evans & Goodman, 2009; Hennings, Froggatt, & Keady, 2010; Watson, Hockley, & Murray, 2010). Government initiatives in England have sought to improve both end-of-life care (Department of Health, 2008) and support for people with dementia (Department of Health, 2009, 2010). Similar policy objectives for end-of-life care have been developed in Wales (Welsh Assembly Government, 2003), Scotland (Scottish Government, 2008) and Australia (Australian Department of Health and Ageing, 2006).
Dementia accounts for one in three deaths among people aged 65 and over (Brayne, Gao, Dewey, M., Matthews, & Medical Research Council Cognitive, Function, Ageing Study Investigators, 2006), so people with dementia make up a very high proportion of all those potentially needing end-of-life care. However, end-of-life care for people with dementia is often sub-optimal (Sampson, Ritchie, Lai, Raven, & Blanchard, 2005; Engel, Kiely, & Mitchell, 2006; Hughes, Jolley, Jordan, & Sampson, 2007; Godwin & Waters, 2009; Goodman et al., 2010; Hall, Kolliakou, Petkova, Froggatt, & Higginson, 2011; Lawrence, Samsi, Murray, Harari, & Banerjee, 2011).
Palliative care for people with dementia poses particular challenges to those providing services, who report lack of confidence in their skills, a sense of helplessness and a need for training (Dening, Greenish, Jones, Manda, & Sampson, 2012). Dementia may have a fluctuating illness trajectory, in which there is a progressive deterioration (Murray, Kendall, Boyd, & Sheikh, 2005; Hennings et al., 2010), often punctuated by steeper declines caused by bouts of acute illness (Sachs, Shega, & Cox-Hayley, 2004). Moreover, recognising when a person with dementia is nearing the end of life is particularly challenging. The overall estimated median survival time from onset of dementia to death is 4.1 years for men and 4.6 years for women, with longer survival among those with early onset dementia (in their 60s) (Xie, Brayne, Matthews, & Medical Research Council Cognitive, Function, Ageing Study Collaborators, 2008). It is easy to see how the need to prepare for or recognise the end of life can so easily be missed (Sloane, Zimmerman, Williams, & Hanson, 2008; Godwin & Waters, 2009). Few people with dementia can express their preferences for end-of-life care at the time that they need it (Triplett et al., 2008; Johnson et al., 2009). Practitioners may rely on a combination of information from advance care planning documentation, their own knowledge and that of family carers and their own observations of behaviour, some of which may be conflicting.
In England both the National End of Life Care Programme (Department of Health, 2008) and the National Dementia Strategy (Department of Health, 2009) recommend education and training in palliative care for those working with patients with dementia. However, there are few evaluations of the effectiveness of dementia education and training (Hussein & Manthorpe, 2012). This paper presents a narrative review of evaluations of educational programmes for practitioners working with people with dementia at the end of life.
Methods
This paper is the product of a rapid appraisal of the literature carried out for the IMPACT study (IMplementation of quality indicators in PAlliative Care study), a European Commission study of palliative care for people with dementia and people with cancer. The search terms used were: palliative care, terminal care, attitude to death or dying, end-of-life care, comfort care, symptom control, end-stage disease, living will, advance directive, palliate, palliative and Alzheimer’s disease, dementia, neurodegenerative diseases, Parkinson’s disease and aphasia. The following databases were searched: AMED, ASSIA, BNI, CareData, CINAHL, EBMR, EMBASE, HMIC, IBSS, Medline, PsychINFO and Social Science Citation Index. Titles and abstracts were screened by two reviewers and papers were then categorised according to their subject and main themes, education and training being one category.
The searches yielded 6167 papers. Papers were included only if they: a) described education or training for healthcare and social care professionals or practitioners already in post (that is, in-service training or continuing professional development); b) reported an educational intervention that had been evaluated; or c) were reviews of educational interventions. Where the substance of the paper was not clear from the title and abstract, the full paper was read. A broad selection of papers was chosen at first and a third reviewer reviewed papers if there were doubts over inclusion.
We excluded papers about the education of those working in palliative care that focused on conditions other than dementia (e.g. cancer); papers published before 2000; and papers covering aspects of dementia not related to palliative care, for example medical treatments, social activities or diagnosis.
Findings
A total of eight papers were identified which described and evaluated palliative care education or training for professionals caring for patients with dementia (see Figure 1). One paper described psychiatric nurses’ impressions and experiences of education for palliative care, five were evaluations or descriptions of educational interventions and two were reviews of current knowledge.
PRISMA diagram.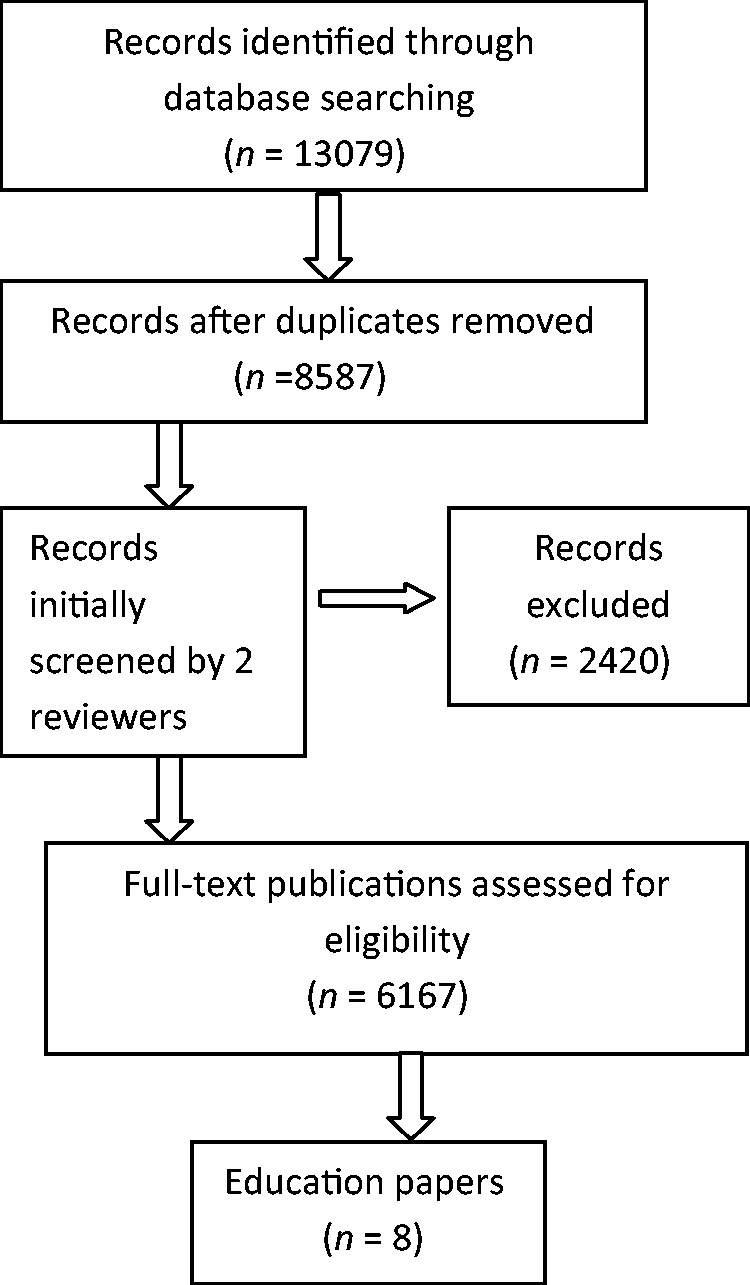
Summary of papers on education and training for end-of-life care in people with dementia.

Evaluations of educational interventions
Arcand and colleagues described an educational intervention for staff caring for residents with moderate to severe dementia in a 387-bed nursing home in Quebec, Canada (Arcand et al., 2009). This was a pre- and post-intervention study, where the intervention included awareness-raising meetings to explain the project as well as educational sessions. The awareness-raising meetings were aimed at physicians, head nurses, other professionals, members of the residents’ committee, members of the ethics committee and administrators. The educational sessions were aimed at nursing staff and separate sessions were arranged for the physicians. The sessions lasted 45 minutes and were provided on a number of occasions to enable staff working different shifts to attend. Their content covered topics deemed relevant to palliative care for people with advanced dementia. Nursing staff of all levels, including nursing assistants, attended. The physician education sessions lasted 60 minutes, covering topics in more detail, although not all physicians attended. A relevant medical article for further reading was supplied to the physicians.
Booklets on ‘comfort care’ were developed from a literature review and qualitative research. These were given to nursing staff and physicians, who could give these to family members whenever they felt it appropriate. The researchers assessed levels of satisfaction among the family members of residents who had died with advanced dementia before and after the educational intervention (sessions and booklets) provided to staff. The researchers interviewed 27 family members of residents who had died between January and August 2005 (pre-intervention – Time 1) and 21 family members of residents who had died between January and August 2006 (post-intervention – Time 2).
Of the relatives invited, 60% invited participated at Time 1 and Time 2, with lack of time being the main reason cited for not taking part. The characteristics of deaths among the nursing home residents were similar in both groups, with pneumonia being the main reported cause. Family satisfaction with end-of-life care was assessed using the ‘After-death bereaved family member interview/ Nursing home version’. Pre- and post-intervention group scores were compared using a 2-sample t test. Although the trend was for higher scores in the post-intervention group (T2), indicating higher satisfaction with the care provided among family members, the difference did not reach statistical significance.
This study was conducted in one voluntary sector nursing home facility where residents (and family members) were Jewish, so the results may not be generalisable to different populations; no comment was made regarding whether this group might have any special needs or cultural considerations about end-of-life care. The staffing levels at the facility were considered by the authors to be comparable to standard public facility norms, but they were supplemented by additional volunteers and ‘companions’ paid for by residents’ families. Post-intervention interviews took place many months after death (mean 10 months post-intervention) and recall at this point may have been distorted, although this did have the advantage of possibly avoiding provoking distress among bereaved relatives. One limitation is that the staff were not interviewed, nor was their practice observed to ascertain any benefit from the intervention. Furthermore, as this study was based in one nursing home, a larger, multi-site study would be needed to explore the impacts of such an educational programme.
Another study from a not-for-profit nursing home in Canada (Gnaediner, Robinson, Murray, & Vandergoot, 2008) described the development of an education programme for staff on end-of-life care for residents with dementia. Consultants in hospice palliative care and adult learning, together with a clinical nurse specialist from the nursing home, developed and offered a two-day workshop to approximately 90 staff members (nurses, occupational and physical therapists, social workers and dieticians) with the expectation that this would improve their understanding of end-of-life care for people with dementia. A clinical nurse specialist, a consultant and five senior members of staff were selected as trainers and participated in two train-the-trainer days. Staff members were asked by a clinical nurse specialist about what they wanted to know and family members were interviewed by another senior nurse to find out what was important to them when their relative was dying. The two-day workshop covered disease progression, the ‘ambiguous dying syndrome’ (the time before dying in which the likelihood of dying can best be described as uncertain; Bern-Klug, 2004), support for families, symptom management, making moments meaningful, last days and hours and staff care. As well as PowerPoint presentations, participants were given a work-book, discussed case studies to prompt problem solving and participated in role play. The educational intervention was carried out by either the clinical nurse specialist and the hospice palliative care consultant or the consultant and a trainer. However, very little detail is given about the participants, the content of the course and the training given to the trainers.
Preliminary results of the above trial were later published separately in Gnaedinger et al. (2010). A sample of 17 staff members from a range of disciplines and positions was interviewed in three groups and an additional group interview was undertaken with the workshop facilitators/clinical educators. All groups were asked the same question: ‘What changes have you made or observed in your practice because of or that you would attribute to new perspectives, new knowledge, and new skills learned during the dementia difference workshop?’
Staff identified seven key changes to their practice since their participation in the workshop. First, staff felt that there was more spontaneous and formal discussion about end of life and death. They described a decreased focus on the clinical nature of dying, with a stronger focus on quality of life, rather than sticking to a strict hospital routine. Staff believed they had increased their knowledge, understanding and confidence, and had gained a greater sense of ‘team-ness’. In turn, the increase in knowledge and confidence allowed improved communication with family members, in their perception. Within the care facility there was also a change in the language that was used: for example, staff used the terms ‘actively dying’ or ‘imminently dying’ as opposed to ‘palliative’. Finally, the staff reported increased attention to self-care: for example, they would now tell their colleagues to ‘eat well, rest, laugh, pray, talk to others’.
The educators also reported several lessons from the teaching that enabled them to develop their own understanding and knowledge. For example, the palliative care consultant who helped develop the workshop said she had increased her knowledge of dementia.
From an acute hospital setting, Formiga, Vidaller, Mascaro, and Pujol (2005) evaluated the effect of an educational intervention on health professionals’ decision making when caring for patients who were dying with dementia in a hospital in Barcelona, Spain. They scrutinised the case notes of 365 patients who had died in hospital with dementia. Case notes analysis was used to assess DNAR (do not attempt resuscitation) orders, step-down treatment decisions, decisions not to transfer to critical care units and decisions not to initiate antibiotics or to do additional tests, and to identify any mention of whether information on prognosis had been provided to family members. An educational programme was then initiated, comprising one 45-minute-long session open to doctors and nurses, PhD students in Geriatrics and undergraduate students in their fourth or fifth year. This session included making decisions, discussions with families, palliative care interventions and ways to manage the palliative care needs of patients who are dying with dementia, as well as the importance of documenting all discussions and decisions in the notes.
There is little detail on the content and structure of the brief educational intervention and little about the assessment of the intervention’s effectiveness. The scrutiny of case notes may not give a reliable picture of the discussions that have been held. Formiga and colleagues noted a low percentage of patients with DNAR documented. Even after the educational intervention, however, there were no significant differences in the management of patients dying with dementia. Formiga and colleagues measured five indicators: number of DNAR orders, gradation of therapeutic decisions, information provided to relatives about prognosis, total withdrawal of routine drug therapy and the provision of ‘terminal’ care in the last few days of life. Both before and after the intervention, in about 70% of cases for which there were documentary records, the researchers judged that there had been appropriate care in terms of prognosis information provided to the family, withdrawal of inappropriate medications and initiation of palliative treatment.
This educational intervention did not significantly alter five indicators at the end of life. The authors concluded that the educational programme needed to be more specific about the needs of patients with dementia. Formiga et al. (2005) considered it important to record prognosis to facilitate co-ordination between medical professionals. They advised that health care planning should include policy directed at improving the end-of-life experience of hospital patients with dementia.
Robinson and Sudbury (2009) conducted a two-day workshop for an unknown number of health professionals from a range of disciplines and backgrounds at a 229-bed complex care facility in Canada with 115 priority access beds, 110 community beds and four respite care beds for veterans. A purposeful sample of 17 workshop participants was invited to join a subsequent focus group to discuss any ways their practice might have changed since the workshop. Participants overall reported increased understanding and acceptance of the dying process and death, and felt this had affected their practice. They said that they were more likely to communicate with each other, with residents and with families about death and dying. This, they felt, improved staff stress levels and helped with advance decision making and planning.
Valente and Saunders (2010) reported the findings of a survey of 190 psychiatric nurses who were attending the American Psychiatric Nurses Association’s annual conference in 2006. The survey briefly asked about the conference attendees’ knowledge and skills, their interest in end-of-life care, their perceptions of their potential roles in end-of-life care and their recommendations for end-of-life care. This was not specific to dementia; however, some psychiatric or mental health nurses may work with patients with dementia. The opportunistic survey found that 30% of nurses thought they had some end-of-life skill, 46% had moderate end-of-life skill, 30% had some end-of-life knowledge and 49% had moderate knowledge. Less than 10% reported excellent skills or knowledge. Most of the nurses expressed some interest or were very interested in end-of-life care, which may be a bias inherent in such a convenience sample.
Several areas of psychiatric nurses’ expertise relevant to end-of-life care were identified from the survey, including therapeutic communication and discussion of difficult topics, screening, assessing mood disorders, grief work, suicide evaluation and mental status examinations. With further education, the nurses felt they could apply their skills and knowledge to dying patients to improve patient care. To achieve this, they wanted education about communication, legal issues and cultural issues surrounding death, and patient education on death and dying.
Reviews of educational interventions
Chang et al. (2005) discussed recent research focusing on the educational needs of staff caring for people with dementia at the end of life and explored some of the challenges in providing palliative care. Their review paper discussed ways to enhance skills among key providers of care through education of health professionals and, specifically, aged-care facility (care home) staff. They outlined the benefits of a palliative approach in end-stage dementia (ESD), discussing why such an approach seems often to be lacking – for example, because of fragmented services, lack of recognition of dementia as a terminal illness, challenges in prognostication and communication difficulties with patients.
The latter part of this paper focuses on the educational needs of care home and nursing home staff, including care workers, registered nurses, clinical nurse specialists and general practitioners (family doctors). The authors identified six studies reporting a lack of education among care home staff, mainly covering nursing staff, but also including evidence of educational needs identified among registered nurses and GPs. These included pain and symptom management, counselling skills, the physiology of death and knowing when to withhold routine care.
Chang and colleagues (2005) also identified a lack of debriefing for nursing staff and poorly resourced bereavement support for family members and noted some interventions aimed at addressing these deficits, including an education package for GPs in Australia and training of clinical nurse specialists in the UK. They observed that some studies had positive results in terms of increasing staff understanding of dementia and increased awareness of residents’ discomfort. The authors also addressed the importance of educating family members. They recommended the development and implementation of educational programmes for multidisciplinary staff caring for people with end-stage dementia and training within generalist settings.
Chang and colleagues commended the work of Grbich et al. (2003) in calling for minimum palliative care competencies for care providers which, they argued, should be funded by government. They also recommended the development of a learning package for general practitioners based on the results of a survey of residential care facilities in South Australia.
Later, Mittman summarised several conceptual or theoretical frameworks for quality improvement that may be relevant to palliative care services for people with dementia (Mittman 2006). One framework was based on the chronic care model, an approach used in depression management, and the main features of this approach were summarised. Other programmes discussed briefly in Mittman’s review included giving training to patients and carers to educate their physicians and other healthcare providers, a ‘train-the-trainer’ approach for physicians to teach clinical skills to their colleagues and a case study method for clinicians to present the principles of high-quality dementia services.
Mittman also emphasised the important role of non-physician clinicians and support staff, and the role of patients in managing their own condition, even though this may be limited for people with dementia whose symptoms are severe. Mittman concluded that patients and carers may benefit from ‘consumer education’ programmes.
In terms of outcomes, Mittman noted that such approaches have yet to demonstrate significant benefits for the quality of care. This review suggests that multi-level approaches are needed that ‘require a sustained, coordinated campaign of inter-related efforts by a broad spectrum of leaders and stakeholders in dementia, research, practice, and policy, modelled after similar efforts targeting other chronic diseases and requiring significantly increased levels of commitment, energy and effort’ (Mittman 2006, p. 61).
Mittman concluded by suggesting initiatives for improving dementia care, including the building of new dementia coalitions to establish commitment and collaboration, as undertaken in relation to diabetes and heart disease in the US. This approach could also generate business interest and the sort of public and private funding programmes that other chronic disease research attracts. A single set of authoritative clinical practice guidelines was suggested, instead of the multiple and uncoordinated guidelines currently in existence, with dementia included in quality monitoring systems.
Mittman’s paper contains insights that are relevant to other cultures and countries. Many of the programmes and recommendations for success stem from North America, but not all, and there are several messages that are potentially applicable to health quality improvement in other countries.
Discussion
There are as yet few published evaluations of educational programmes for improving palliative care for people with dementia, yet there are many calls for training and education to be provided. Overall, the few studies found did not show positive effects. There was weak evidence (see Valente & Saunders, 2010) that nurses caring for patients with dementia felt they needed more training on the subject of palliative care, death and dying and some suggestions that learners felt education changed their attitudes (Robinson & Sudbury, 2009), but where outcomes were evaluated, the educational interventions failed to show benefits for patients.
It may be that the conclusions of Moriarty, Kam, Coomber, Rutter, & Turner (2010) about care home staff are relevant to health care professionals more broadly. They commented that although there has been considerable investment in training for staff working in care homes in the UK in the past decade, little attention has been paid to the quality of such training, adding: It has even been suggested that poor quality training is counterproductive. For example, where trainers identify inadequacies in care provision but do not provide examples of alternative strategies, this may leave staff feeling demoralised and deskilled (Moriarty et al., 2010, p. 2).
There is evidence that for an educational process to change professional activity, practitioners need to identify their own learning needs and follow through by initiating the learning process themselves (Grant, Stanton, Flood, Mack, & Waring, 1998). We do not know in detail what educational tools were used in the studies described above. For example, practitioners may have chosen to learn about the aspects of palliative care education that they already knew about or were comfortable with, or they may have had no choice in what was delivered to them. Knowles’ principles of andragogy state that adult learners should be involved in diagnosing their own learning needs, formulating their own objectives, identifying resources and evaluating their learning (Knowles, 1980). If educational interventions do not have a driver, the learner is unlikely to gain from them. The driver could be a personal learning agenda or an external force requiring them to achieve specific learning goals as part of their learning. Learning should be about enhancing performance, emphasising both the resolution of clinical concerns and better outcomes for patients (Nowlem, 1988). If the teaching is part of a known and required curriculum or agenda it is more likely to have an impact, as the learner has an incentive, apart from a personal learning need, to participate in and apply knowledge from the educational intervention.
In the case of palliative care for dementia – a sensitive and possibly controversial subject – learning could be integrated with practice to make it more relevant to the learner (Harden & Laidlaw, 1992). Kolb’s experiential learning theory concludes that learning is best achieved by relating concrete practice to conceptual models (Kolb, 1984).
The studies identified provided little detail on the type of educational tools used in the programmes, which ranged from two-day workshops to 45-minute sessions. We know that problem solving is useful for learning (Brookfield, 1986), and the more complex the problems are to solve, the more realistic practitioners’ ‘illness scripts’ (templates for disease processes; Feltovich & Barrow, 1984) become, allowing the accurate allocation of cases to scripts through pattern recognition and the enrichment of the scripts as case memory increases with experience.
Some of the papers described the teachers as peers or senior colleagues. We know that peers and colleagues can be the most effective educators.. We did not find examples of families and people with dementia being included in the educational intervention either at the time or in its planning or follow up, and care home staff appeared to be the subject of teaching from professionally qualified staff rather than being engaged in the production and ownership of the learning.
An educational intervention designed to improve practitioners’ practical and emotional capabilities in caring for a patient with dementia at the end of life must meet many theoretical requirements, as outlined above. These studies do not tell us how well constructed the interventions were, or how much the learners were involved in the process of deciding on their learning needs. Many factors may affect evidence uptake and implementation, but the interplay between evidence, the context of practice and facilitation of learning around case studies appears to be a potentially powerful lever for change (Kitson, Harvey, & McCormack, 1998).
The review papers of Mittman (2006) and Chang et al. (2005) identify the need to improve education for palliative care in dementia and note that the educational programmes current at the time gave low priority to palliative care. In England, the National Dementia Strategy (Department of Health, 2009) provides an initial set of quality indicators for good end-of-life care which could be the basis for professional development grounded in educational theory.
Limitations of this review
This review has drawn on material published in peer-reviewed journals since 2000 in English. Given the dearth of evaluations of education for end-of-life care for people with dementia, we do not think that searching from an earlier date would be fruitful. Similarly, there may be evaluations in other languages, or in the literature not indexed on the databases we selected.
Conclusion
There are few published evaluations of educational interventions about palliative care for people with dementia. Where educational impact has been measured, no positive effects for people with dementia have been demonstrated. New programmes designed to improve end-of-life care for people with dementia need to be based on sound educational methods and rigorously evaluated.
Footnotes
Funding
This research has been funded by the European Union’s Seventh Framework Programme ([FP7/2007-2013] under grant agreement n°[258883], The views expressed in this paper are those of the authors alone and should not be interpreted as those of the European Union.