
Abstract
Introduction
Dementia is defined as a cognitive impairment that severely affects activities of daily living and leads to loss of independence (Pasquini et al., 2018; van der Steen, 2010). Moreover, the development of dementia is usually progressive and irreversible, getting worse over time and eventually leading to severe disability in older adults (Sousa et al., 2009, 2010). Therefore, dementia is considered one of the most burdensome diseases (Europe, 2019). Dementia is also emerging as a serious health challenge globally, with the number of people living with dementia estimated to be over 55 million worldwide (Organization, 2022) with projections that the number of people living with dementia will reach approximately around 152.8 million globally by 2050 (Nichols et al., 2022).
Dementia is associated with shorter life expectancy, making it the fifth leading cause of death globally, responsible for a staggering number of deaths each year (Scheltens et al., 2021). People with dementia are often accompanied by other comorbidities that increase their risk of death, such as impaired consciousness, pain, aspiration pneumonia, and eating disorders (Davies et al., 2021; Hum et al., 2018; Sampson et al., 2018). This also exacerbates patients’ suffering, which makes them more vulnerable in the final stages of life. Considering this predicament, end-of-life care has become a pressing issue.
People with dementia may benefit from palliative and end-of-life care, even though there is no reversible therapy for dementia illness (Piovezan et al., 2020). Palliative and end-of-life care is comfort-oriented, preventing and alleviating patients’ suffering through early treatment of pain, addressing other physical, mental and spiritual issues, and maintaining the highest quality of life until death, rather than merely prolonging life (Organization, 2018; Radbruch et al., 2020; Van der Steen et al., 2014). There are several venues where end-of-life care can be provided, including homes, nursing homes, and hospitals (Wang & Wang, 2020). However, most people express a preference for receiving end-of-life care at home (S. Shepperd et al., 2021). This is because one’s own home provides familiarity, comfort, and a more intimate atmosphere than the hospital environment, which helps patients to feel accompanied and cared for by their families in the last days of their lives (Wahid et al., 2018). This comfortable environment not only reduces patients’ anxiety and distress but also contributes to improving their quality of life (Gozalo et al., 2011). Consequently, the home is becoming the preferred place for an increasing number of terminally ill patients as it helps them to live the last stages of their lives with dignity and meaning (Higginson & Sen-Gupta, 2000).
The integration of home end-of-life care program into dementia care is a first step towards alleviating end-of-life suffering and improving the quality of death and is a key factor in helping people with dementia to achieve a ‘good death' (Hoare et al., 2015). However, despite the many advantages of home end-of-life care, which have been favorably viewed in several studies (Brumley et al., 2007; Gomes et al., 2016), current evidence shows mixed findings on the ultimate practical outcomes of end-of-life care at home, particularly as some studies have found that home end-of-life care is associated with long hospice stays (>180 days) and live discharges from hospice (Luth et al., 2020, 2021). This issue is highlighted in people living with dementia. As dementia progresses, the symptom burden and physical dependency of people with dementia increases, requiring high levels of care that are often beyond the capacity of their family caregivers (Peacock, 2013). This can lead to hospitalization, most commonly in a nursing home. It also results in people living with dementia rarely dying at home (Sleeman et al., 2014). They are more likely to die in a hospital or long-term care facility (Reyniers et al., 2015). Therefore, although one’s own home may be a satisfactory end-of-life care setting for people living with dementia, unfortunately, the lack of evidence on home-based end-of-life care for this population leaves it unclear whether home can ultimately serve as their final place of care (Miranda et al., 2019).
Aim
This review aimed to assess and identify current evidence on home-based end-of-life care for people living with dementia by synthesizing findings from quantitative and qualitative studies, as well as to identify key gaps in the existing evidence that still need to be addressed more comprehensively.
Objectives
Specifically, the purpose of this review was to identify existing evidence on (i) interventions, outcomes, and effectiveness, including cost-effectiveness, of home-based end-of-life care for people living with dementia, and (ii) the experiences of people living with dementia and their family caregivers who utilize home-based end-of-life care services, as well as the perspectives of those who provide such care services.
Method
This review used a combination of quantitative and qualitative data (Thomas et al., 2004), and was conducted in strict adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009).
Eligibility criteria
Inclusion and exclusion criteria were determined using participant, intervention, outcome, and study design methods. Only studies that met the following criteria were eligible for inclusion.
Participants
Participants with dementia, including all types of dementia or family members or informal caregivers, or healthcare professionals involved in providing end-of-life care for people living with dementia.
Interventions
Studies evaluating end-of-life care services provided in the home setting were included in this review. For the purposes of the review of evidence on home-based end-of-life care, interventions were defined as any type of data about end-of-life care services or interventions at home for people with dementia. End-of-life care is part of palliative care and includes managing symptoms as well as providing psychological, social and spiritual support and ensuring that the wishes of the patient and family are followed (Alshammari et al., 2022). Therefore, studies assessing home-based end-of-life care, home hospice or home palliative care were included in the review. Studies of palliative or end-of-life care in nursing home settings or in the community, or in hospitals were excluded.
Outcomes
Studies encompassing one or a broad range of outcomes related to home-based end-of-life care associated with people living with dementia, family caregivers, healthcare professionals, including, but not limited to, quality of life, quality of death, dementia symptoms, comfort, place of death, satisfaction with care, health care utilization, cost of care, and survival, experience and satisfaction of care were included. Studies were excluded if the outcomes related to the needs of home-based end-of-life care for people living with dementia.
Study design
Randomized and non-randomized controlled trials, non-comparative trials, and qualitative or mixed-methods studies were included in the study. Case reports, conference proceedings and books, literature reviews and unpublished and grey literature were excluded.
Search strategy
Recognizing that relatively few studies were likely to be found, and to reduce the risk of missing studies, the search terms covered only the following three domains: (i) end-of-life care, (ii) dementia, and (iii) home. No specific terms were used in the search to describe study designs, interventions, comparison groups, or outcomes. The search was conducted from June to August 2023, and 5 electronic databases (PubMed, Web of Science, MEDLINE, CINAHL and Scopus) were searched. The search strategy was adapted to the different databases. The researcher (GY) also searched the reference lists of the included studies to identify other relevant articles. Additionally, citations to the included studies were tracked through citation tracking in Google Scholar. The full text of all identified potentially relevant citations was manually reviewed to verify that they met the inclusion criteria. Additional language restrictions were used to include only English-language publications, but no geographic or year restrictions were set.
Review articles were uploaded to Endnote reference management software (Gotschall, 2021) and duplicate studies were removed. One researcher (GY) initially screened titles and abstracts and excluded irrelevant studies. Next, two reviewers (GY & YW) independently screened the full texts of relevant studies. Studies that did not meet the inclusion criteria were deleted, and the reasons for exclusion were recorded. Discrepancies between reviewers regarding inclusion were resolved through discussion.
Data extraction
Data extraction forms were used to extract data for evidence synthesis and to assess study quality. Data extraction and analysis were carried out in stages. Data were first extracted independently by one researcher (GY) according to a pre-designed standardized data extraction form. The data extraction tool was based on the Cochrane checklist (Higgins & Green, 2008). The second researcher (HC) then verified and checked the data in the table and resolved any differences through discussion.
Data synthesis, and analysis
Due to the high degree of heterogeneity in the studies included relating to outcomes, study design and participants, neither meta-synthesis of qualitative studies nor meta-analysis of quantitative studies was applicable. Due to this situation, a narrative synthesis analysis approach was adopted, which offers flexibility in combining quantitative and qualitative data (Lipsey & Wilson, 2001).
Using the EAPC White Paper’s guidelines for optimal palliative care for people with dementia as a framework (Van der Steen et al., 2014), this review synthesized the key points of the included interventions to determine whether existing home-based end-of-life care practices meet the latest standards of best practice in palliative and hospice care for people with dementia.
Quality assessment
In this systematic review, the Mixed Methods Appraisal Tool (MMAT) (version 2018), which is a validated tool and allows for the assessment of studies of a wide range of designs, was used due to the combined review of quantitative and qualitative methodological studies (Hong et al., 2018). Quality assessment was conducted independently by two reviewers GY & LZ. Disagreements between the two reviewers were settled by discussion until agreement was reached. It is important to emphasize that no study was excluded from this systematic review based on quality assessment.
Results
Study selection
A total of 2022 studies were identified from the electronic database search. After removing 693 duplicates, a total of 24 studies were considered relevant after title and abstract screening. Fourteen studies were excluded after full-text screening. Reasons for exclusion included non-relevance to the interventions and outcomes on home-based end-of-life care for people living with dementia, non-full text or non-English and review articles. Finally, two relevant studies were identified in a citation search of 10 studies that met the inclusion criteria. The final 12 studies were included in this systematic review (Bolt et al., 2019; Brian Cassel et al., 2016; Holley et al., 2009; Hum et al., 2020; Luth et al., 2021; Miranda et al., 2021; Mitchell et al., 2004; Mogan et al., 2022; Pereira et al., 2023; Sternberg et al., 2019; Tay et al., 2020; Treloar et al., 2009). Detailed study screening, inclusion and exclusion processes are shown in Figure 1. PRISMA flow chart of literature search (Moher et al., 2009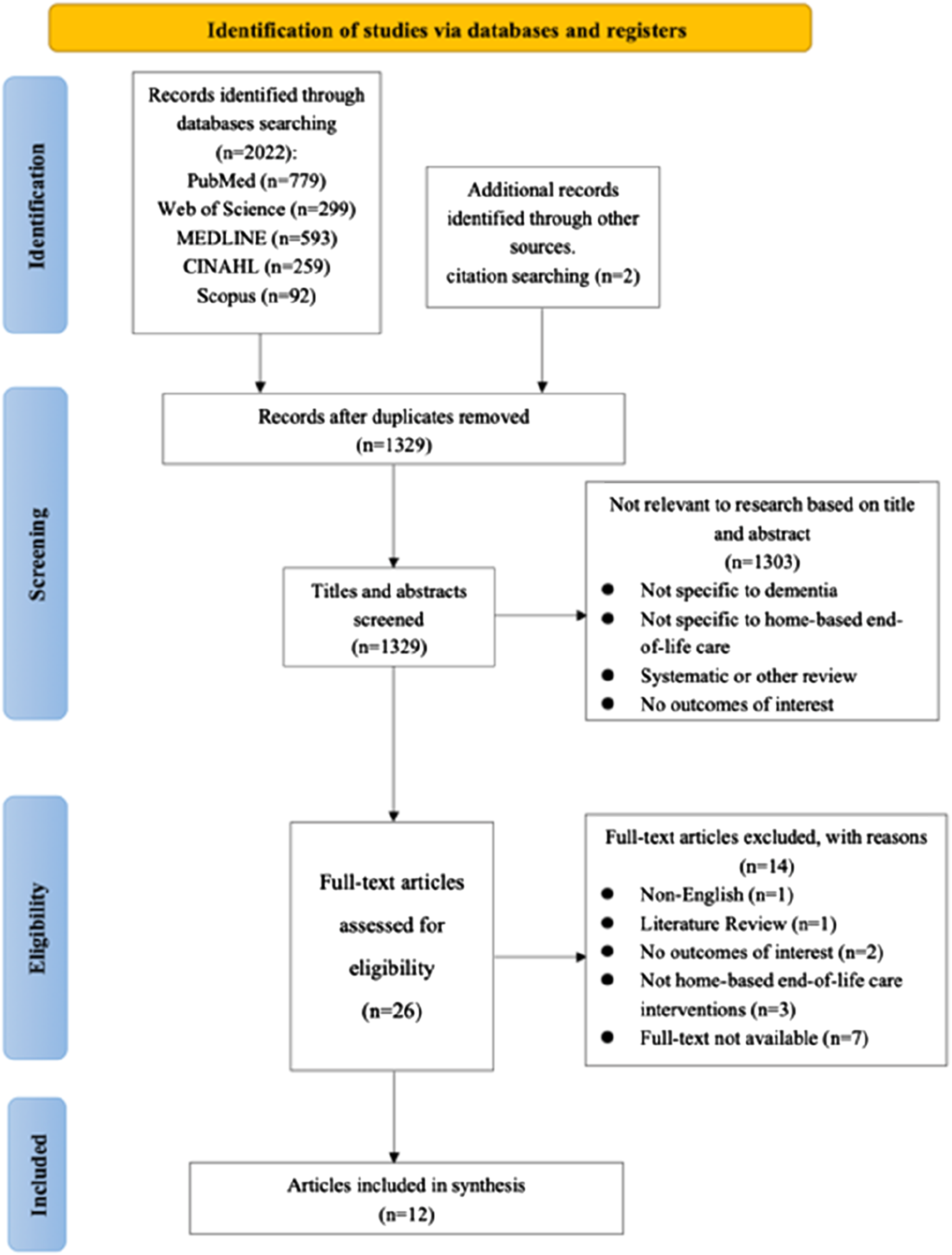
Study characteristics and quality
All 12 studies were published between 2004 and 2023. Eight studies were quantitative studies, of which two were prospective cohort (Hum et al., 2020; Tay et al., 2020) and five were retrospective cohort studies (Brian Cassel et al., 2016; Luth et al., 2021; Miranda et al., 2021; Mitchell et al., 2004; Pereira et al., 2023); with one pilot study with a pre-post design (Sternberg et al., 2019). In addition, three studies were qualitative studies (Bolt et al., 2019; Mogan et al., 2022; Treloar et al., 2009) and one study was a mixed method study (Holley et al., 2009).
The included studies have a diverse international distribution, with four studies conducted in the United States (Brian Cassel et al., 2016; Holley et al., 2009; Luth et al., 2021; Mitchell et al., 2004), and three studies from Singapore (Hum et al., 2020; Pereira et al., 2023; Tay et al., 2020), two from the United Kingdom (Mogan et al., 2022; Treloar et al., 2009), one each from the Netherlands, Belgium, and Israel (Bolt et al., 2019; Miranda et al., 2021; Sternberg et al., 2019).
Details of included studies.
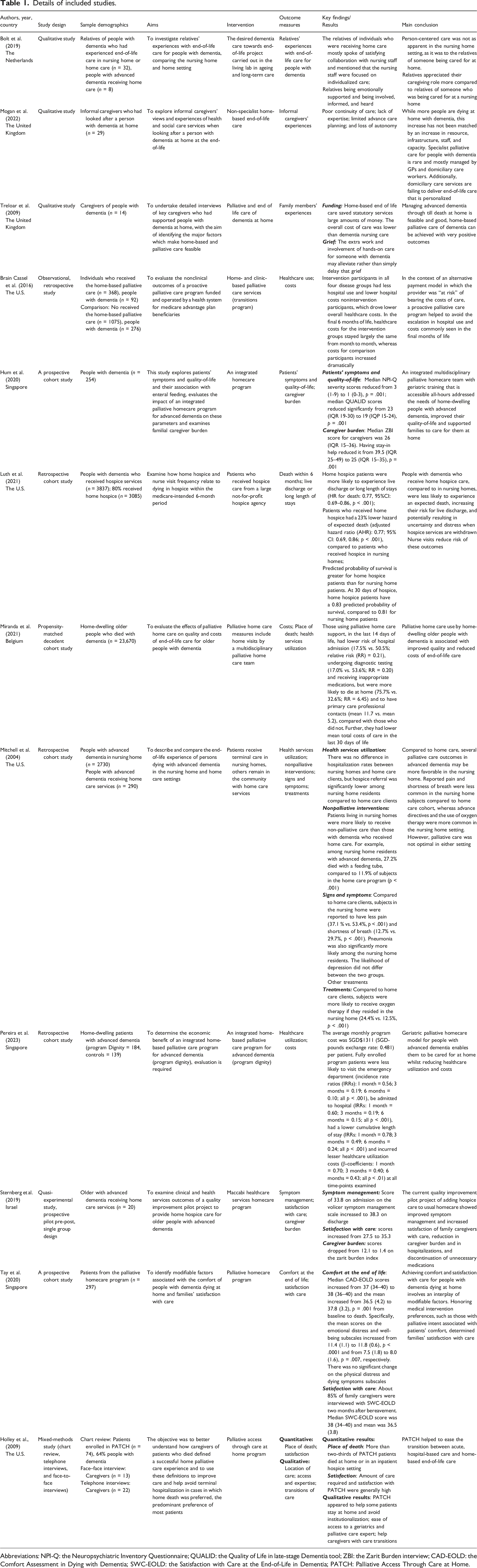
Abbreviations: NPI-Q: the Neuropsychiatric Inventory Questionnaire; QUALID: the Quality of Life in late-stage Dementia tool; ZBI: the Zarit Burden interview; CAD-EOLD: the Comfort Assessment in Dying with Dementia; SWC-EOLD: the Satisfaction with Care at the End-of-Life in Dementia; PATCH: Palliative Access Through Care at Home.
MMAT quality appraisal results.
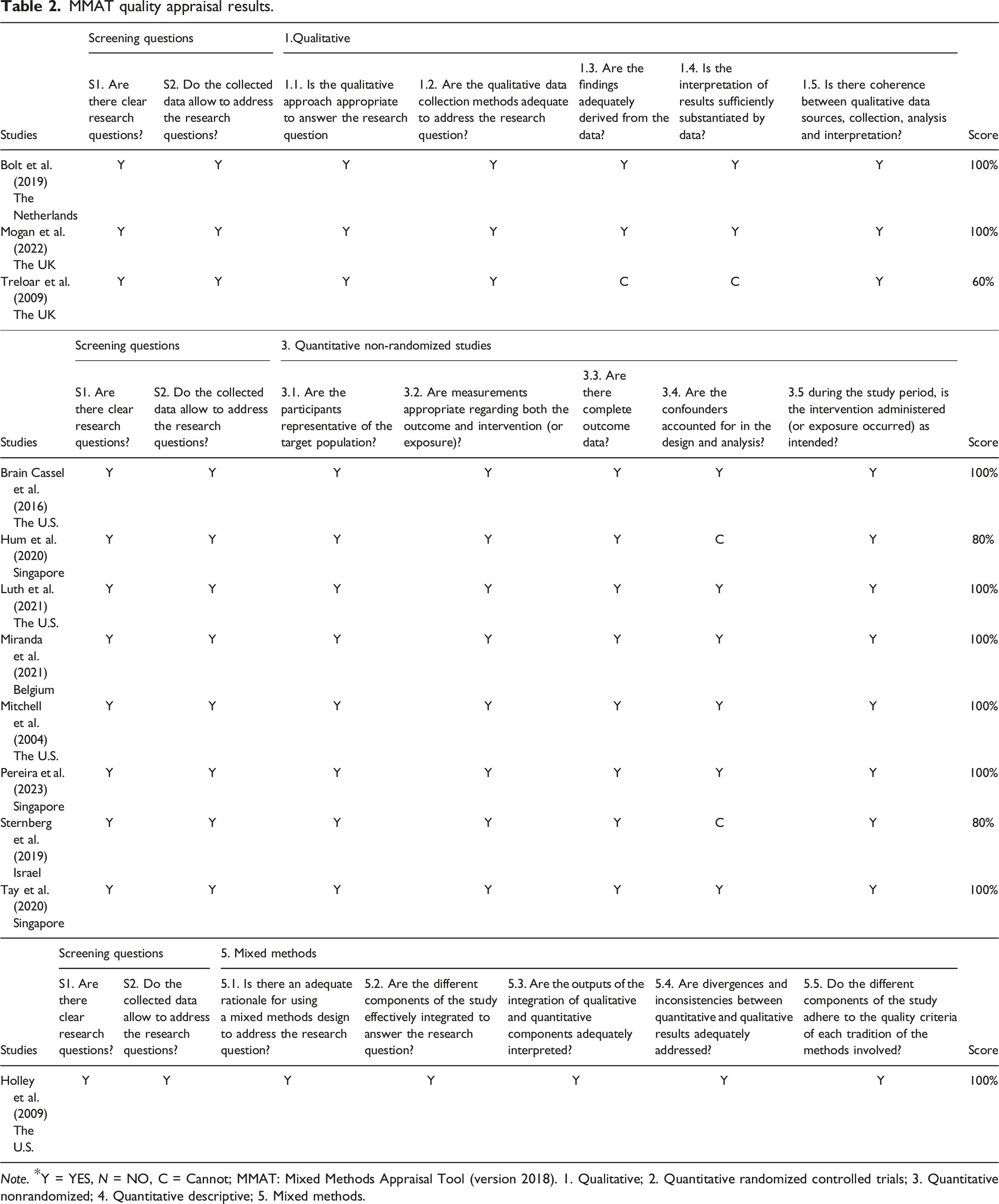
Note. *Y = YES, N = NO, C = Cannot; MMAT: Mixed Methods Appraisal Tool (version 2018). 1. Qualitative; 2. Quantitative randomized controlled trials; 3. Quantitative nonrandomized; 4. Quantitative descriptive; 5. Mixed methods.
Description of home-based end-of-life care interventions
Home-based end-of-life care services and interventions for people living with dementia in certain studies lacked clear definitions, especially in qualitative and retrospective studies. This can be attributed to differences in the nature and focus of studies. Qualitative studies prioritize subjective experiences and perspectives (Bolt et al., 2019; Mogan et al., 2022; Treloar et al., 2009), Retrospective studies use pre-existing data from patient electronic medical records and databases, which may have obscured intervention specifics (Luth et al., 2021; Mitchell et al., 2004). Consequently, while these studies all examined home-based end-of-life care for people living with dementia, some emphasized detailed intervention descriptions, while others explored various outcomes and effects.
Key components of home-based end-of-life care services (n = 7).

Home-based end-of-life care interventions mapped to the EAPC White Paper domains.
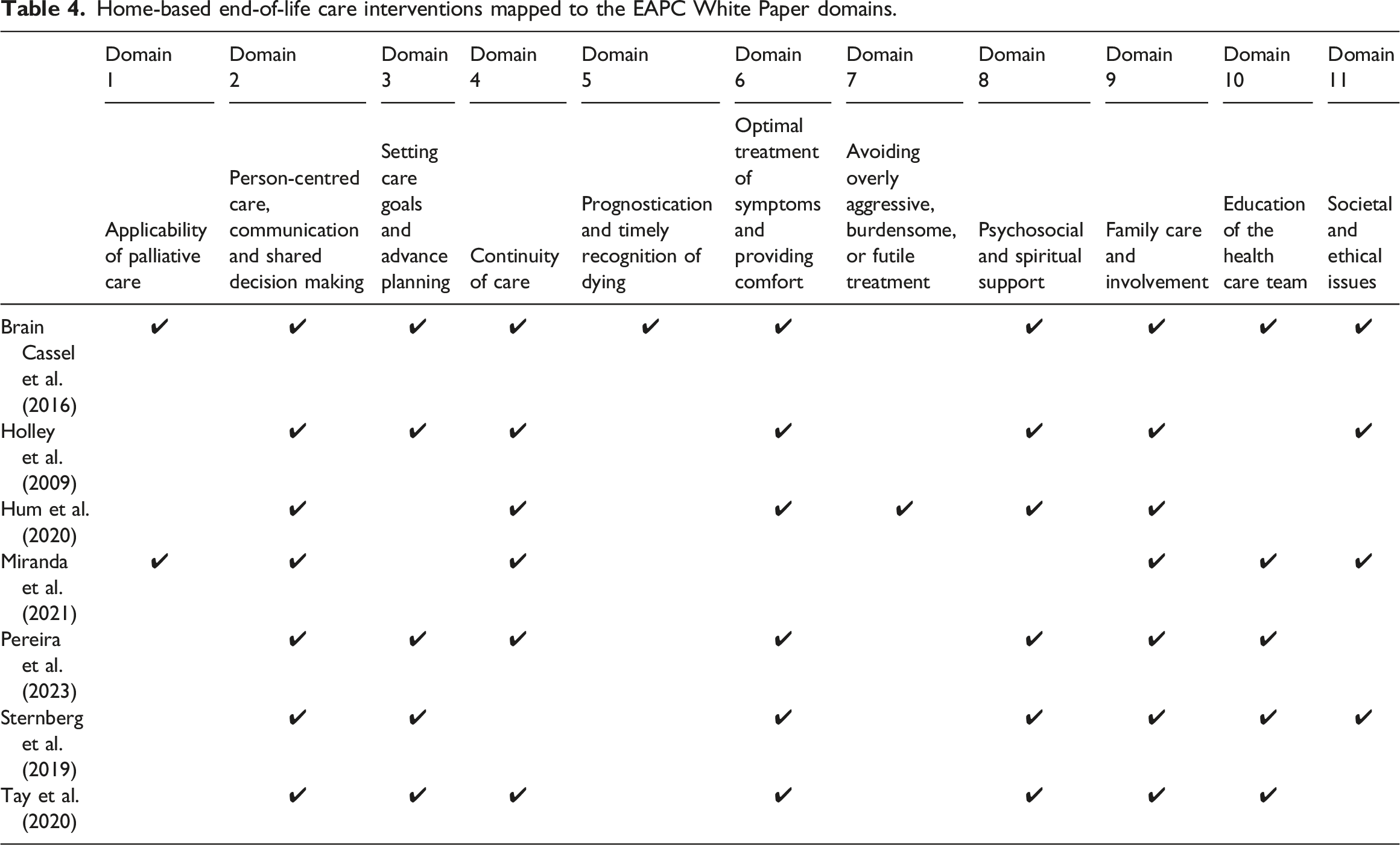
It is important to note that due to the lack of detail in the reporting of care interventions across studies, there is little or no identifiable supporting evidence for several domains of intervention for optimal palliative care for people with dementia, which included applicability of palliative care, avoid overly burdensome treatment, prognostication, and timely recognition of dying. In addition, few studies (Sternberg et al., 2019) reported the timing and duration of home-based end-of-life care for people living with dementia. Only one study (Sternberg et al., 2019) limited the time of end-of-life care, and patients were only allowed to participate in the home-based end-of-life care program for a maximum of six months.
Description of home-based end-of-life care outcomes
Outcomes related to people with dementia
Quality of life
Outcomes of home-based end-of-life care interventions for people with dementia.
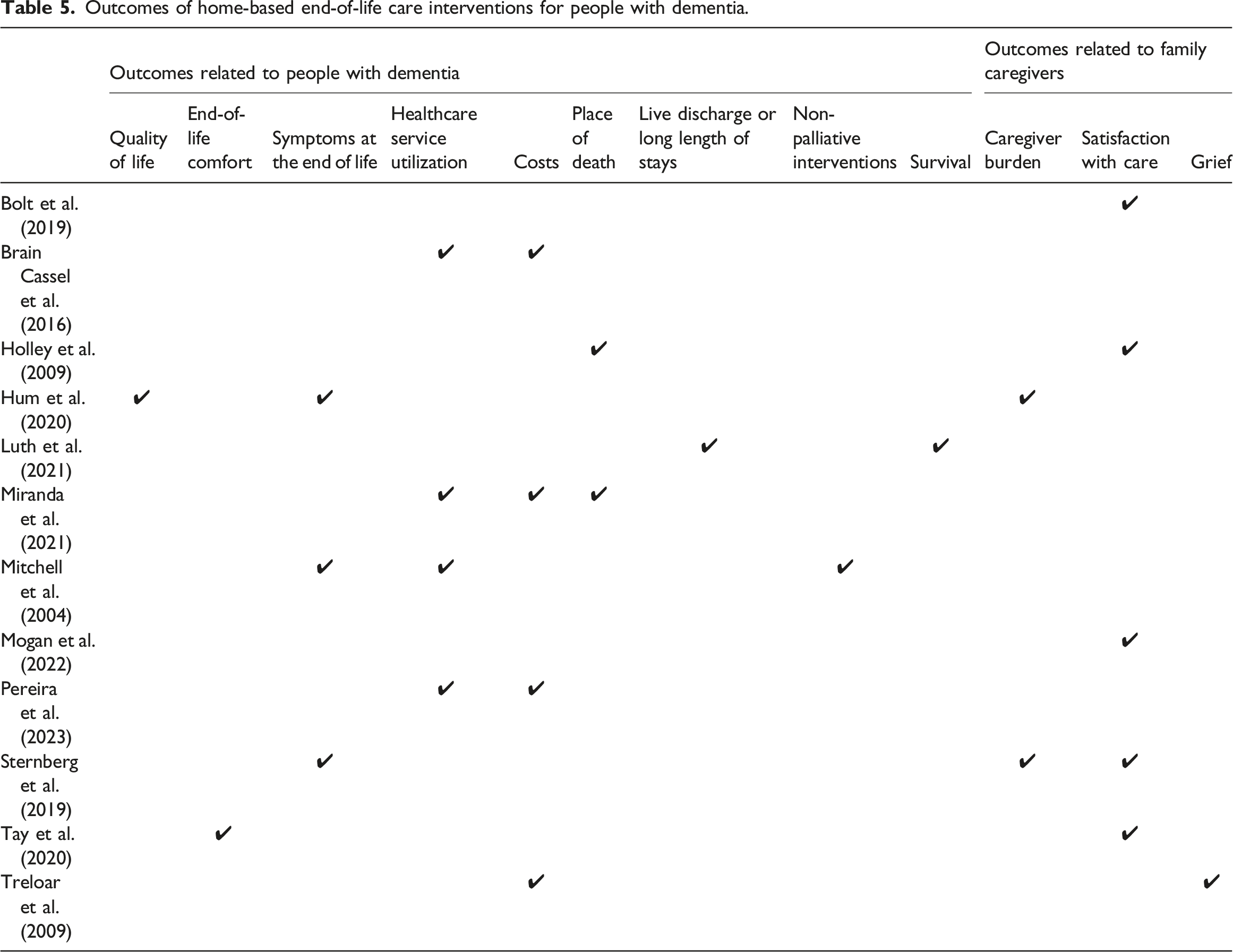
End-of-life comfort
Only Tay et al., (2020) assessed the comfort of dying during end-of-life care in the home for people living with dementia. This study found an improvement in comfort at the end of life for this population at home (p = .001). Notably, emotional distress and well-being exhibited marked improvements, with patients’ scores increasing from 11.4 (1.1) to 11.8 (0.6), p < .0001, and from 7.5 (1.8) to 8.0 (1.6), p = .007, respectively (Tay et al., 2020).
Symptoms at the end of life
Three studies examined the impact of home-based end-of-life care on symptoms in people living with dementia (Hum et al., 2020; Mitchell et al., 2004; Sternberg et al., 2019). Specifically, Hum et al. (2020) revealed a positive impact on reducing behavioral severity and improving nutritional status and pain (p < .05; p = .001; p < .05) (Hum et al., 2020). Sternberg et al. (2019) also supported this positive impact (p < .001) (Sternberg et al., 2019). However, Mitchell et al. (2004) found that pain symptoms and shortness of breath symptoms were less commonly reported by patients living in nursing homes relatively to those receiving home-based end-of-life care (37.1 % vs. 53.4 %, p < .001; 2.7% vs. 29.7%, p < .001). This may be partially attributable to the fact that patients living in nursing homes are relatively less exposed to pain-causing opportunities due to functional impairment and reduced mobility (AOR, 1.46; 95% CI, 1.04–2.03). Additionally, the use of oxygen therapy was more common in the nursing home setting (24.4% vs. 12.5%, p < .001) (Mitchell et al., 2004).
Healthcare service utilization
Four studies demonstrated significant positive effects of home-based end-of-life care interventions in reducing health care service utilization including reduced inappropriate medication use, surgeries, hospitalizations, admissions to the intensive care unit, and deaths in the hospital (p < .001) (Brian Cassel et al., 2016; Miranda et al., 2021; Pereira et al., 2023). In particular, Mitchell et al. (2004) also found that nursing home patients were more likely to be hospitalized compared to people with dementia receiving home-based care (31.5% vs. 43.7%, p < .001) (Mitchell et al., 2004).
Costs
Four studies examined the cost of providing end-of-life care for people living with dementia at home and all strongly support its potential for reducing healthcare costs (Brian Cassel et al., 2016; Miranda et al., 2021; Pereira et al., 2023; Treloar et al., 2009). Brian Cassel et al., (2016) study highlighted that this was due to patients who received home end-of-life care interventions requiring fewer hospitalizations and lower hospitalization costs, thereby reducing overall healthcare costs (Brian Cassel et al., 2016).
Place of death
Two studies have used place of death as an indicator to assess the effectiveness of home-based end-of-life care for people living with dementia (Holley et al., 2009; Miranda et al., 2021). The results of one study showed that people with dementia who used home end-of-life care support were more likely to choose to spend the last stages of their lives at home (75.7% vs. 32.6%; RR = 6.45) (Miranda et al., 2021). This finding is supported by another study (Holley et al., 2009).
Live discharge or long length of stays
Patients live discharged from hospice to seek treatment, or the condition of patients is stable and no longer eligible for hospice services, is known as “live discharge” (Russell et al., 2017). “Long length of stays” means long hospice stays exceeding 180 days (Luth et al., 2021). Only one study had explored live discharge and long length of stays in people with dementia during end-of-life care (Luth et al., 2021). Results showed that 39% (n = 1485) of people with dementia experienced a live discharge or long length of stays during end-of-life care, while patients receiving end-of-life care at home were more likely to experience live discharge or long length of stays compared to those in nursing homes (30% vs. 26%, p < .001).
Non-palliative interventions
Findings from one study (Mitchell et al., 2004) suggested that home end-of-life care programs appear to favor less invasive forms of care that may be more focused on patient comfort and quality of life. Findings (Mitchell et al., 2004) indicated that 27.2% of nursing home residents with dementia ultimately died from nonpalliative care measures of feeding tubes. In contrast, among people with advanced stages of dementia at home, this percentage was only 11.9% (p < .001).
Survival
One study focused on exploring the survival rates of people who received home-based end-of-life care compared to nursing home end-of-life care settings (Luth et al., 2021). The study showed that the predicted probability of survival for home hospice patients was higher than nursing home hospice patients at both 30 days and 90 days in hospice (0.83 vs. 0.81; 0.67 vs. 0.63). In addition, patients who received home-based end-of-life care had a 23% lower expected risk of death (p < .001).
Outcomes related to family caregivers of people with dementia
Caregiver burden
Two studies assessed caregiver burden when providing end-of-life care to people living with dementia at home (Hum et al., 2020; Sternberg et al., 2019), and provided inconsistent results. One of the studies indicated that family caregivers experienced mild to moderate burden (Hum et al., 2020). In contrast, another study showed that the home-based end-of-life care program had a positive effect on easing caregiver burden (p < .001) (Sternberg et al., 2019).
Satisfaction with care
Five studies reported outcomes of satisfaction with care (Bolt et al., 2019; Holley et al., 2009; Mogan et al., 2022; Sternberg et al., 2019; Tay et al., 2020). The results showed that not all studies consistently found that relatives of people living with dementia were satisfied with home end-of-life care. One qualitative study found that home care provided more personalized and emotionally supportive experiences compared to nursing homes (Bolt et al., 2019). In contrast, another study criticized home care services for failing to provide personalized end-of-life care, with an overemphasis on task-centered approaches and neglecting individual preferences due to resource and infrastructure inadequacies (Mogan et al., 2022). The generation of inconsistent findings also highlights the complexity of the field of home end-of-life care.
Grief
The existing literature on the impact of home-based end-of-life care on family caregivers’ grief is limited, with only one qualitative study providing relevant insights (Treloar et al., 2009). Specifically, family caregivers may alleviate their grief to some extent by taking on additional caregiving tasks and responsibilities, rather than simply delaying their grief experience. However, this study lacked further exploration of this result and failed to reveal in detail how family caregivers can regulate and relieve grief through their caregiving roles. In addition, the research results section lacks adequate quotations or specific examples to enhance its credibility, which to some extent limits the in-depth understanding of the research conclusions and may lead to misinterpretation or research bias. Therefore, in order to ensure the credibility and authority of the findings, further comprehensive studies are needed to validate this finding and remove potential biases.
Discussion
Main findings
This review systematically summarizes the existing evidence on home-based end-of-life care for people living with dementia, offering valuable insights into its viability as an end-of-life care option. Consistent evidence demonstrated from the findings is that home-based end-of-life care for people living with dementia reduces healthcare utilization and costs by decreasing the frequency and length of hospitalization, which is supported by the findings of previous studies (Brumley et al., 2007; Gomes et al., 2013; Gonzalez-Jaramillo et al., 2021). However, the advantages of home-based end-of-life care in terms of the overall cost of care for people living with dementia are uncertain. Due to the current focus of research primarily on assessing healthcare costs. This limited perspective prevents a full understanding of the overall costs of home-based end-of-life care. Candy et al. (2011) have suggested that if the cost analysis of end-of-life care at home encompassed all societal costs, then the cost differences between types of care might be smaller (Candy et al., 2011). For instance, the time and expenses associated with home visits may offset the cost savings from reduced healthcare utilization (Smith et al., 2024).
The place of death for terminally ill patients is often the focus of home-based end-of-life care (Shepperd et al., 2021). The findings of this review support that home-based end-of-life care increases the likelihood of people with dementia dying at home. However, dying at home is not considered a quality indicator of good end-of-life care (O'Leary et al., 2017), consistency between preferred and actual place of death is a better quality indicator (Hammer et al., 2023; Mansoor et al., 2023). Patients and caregivers participating in home-based end-of-life care programs suggests a strong inclination towards spending final days at home (Holley et al., 2009). This suggests that the outcome of the place of death is largely influenced by voluntary choices made by patients or their families. However, it also indicates that home-based end-of-life care can help people with dementia realize their wish to die at home.
While this review acknowledges the benefits of home-based end-of-life care on pain and symptom management, the results suggest that nursing home settings may better meet the needs of people living with dementia in this regard. Nursing home settings provide greater access to medical and nursing resources, which facilitates more effective management of pain and symptoms, such as oxygen therapy is more common in this setting (Mitchell et al., 2004). Despite pain and symptom management are recognized as crucial aspects of end-of-life care for people with dementia (McCaffrey et al., 2016), fewer reports of pain and symptoms in this review could indicate gaps in assessment and research coverage concerning these aspects for people with dementia. Indeed, existing literature suggests that pain is prevalent among people living with dementia during the end-of-life stage, but is often underdetected and undertreated (Thakur et al., 2017). This gap in comprehensive research on pain and symptom management during the home-based end-of-life care for people living with dementia limited understanding and response to this critical aspect.
Significantly, although home-based end-of-life care shows positive effects on people living with dementia, its effectiveness in supporting family caregivers remains inconclusive. Specifically, controversial findings exist regarding family caregivers’ burden and satisfaction. While some evidence suggests caregivers feel safer with the support of home-based end-of-life care services (Sarmento et al., 2017), they encounter numerous challenges in actual implementation. Limited face-to-face care from hospice workers often leaves family members as primary caregivers when workers are unavailable (Luth et al., 2021). Rowland et al. (2017) indicates patients in home-based end-of-life care required nearly 10 hours of care per day from family caregivers in their final three months, without which many patients would not be able to die at home (Rowland et al., 2017). Furthermore, a review finds that even with support, family caregivers inevitably face emotional and psychological stress (Becqué et al., 2019). Caregivers may feel pressure from professionals to act as professionals rather than loving relatives (Neergaard et al., 2008).
The review also examined the characteristics of home-based end-of-life care interventions for people living with dementia. Several elements of optimal palliative and end-of-life care are also well represented in this review of studies on end-of-life care at home for people living with dementia, as noted in the EAPC white paper (Van der Steen et al., 2014), although no single intervention can comprehensively address all of the 11 areas of optimal palliative and end-of-life care. In contrast to previous findings (Kochovska et al., 2020), this review suggests that current research placed a widespread emphasis on the continuity of care. This may reflect an improving focus on end-of-life care in the home for people with dementia and the recognition that transition to hospital may sometimes be in the best interests of the patient (Kochovska et al., 2020). However, the applicability of palliative care, avoiding overly treatment, prognostication, and timely recognition of dying has rarely been considered an area of interest by current research. This may be due to the uncertainty and difficulty in predicting survival, as well as the focus of care interventions on addressing unmet needs in this population rather than being model-driven (Kochovska et al., 2020). Davies et al. (2017) proposed that high-quality end-of-life care for people living with dementia does not need to be highly complex but should be tailored to individual needs (Davies et al., 2017). Furthermore, Round-the-clock access to care is considered a key component to be addressed when developing home-based end-of-life care services (Malcolm et al., 2020; Shepperd et al., 2021). However, it appears that the studies included in this review did not take this critical component into account, which also suggests potential areas for further research and development in home-based end-of-life care for people living with dementia.
Although some attributes of home-based end-of-life care for people with dementia have been described, the process of identifying best practices remains complex and elusive. As a previous systematic review of end-of-life care (Malcolm et al., 2020), there are few well-designed randomized controlled trials in this filed. The lack of high-quality randomized controlled trials hampers the identification of definitive, widely recognized best practice methods or models (Kaur & Li, 2024). Most of the studies included in this review were non-randomized controlled studies (Brian Cassel et al., 2016; Luth et al., 2021; Miranda et al., 2021; Mitchell et al., 2004; Pereira et al., 2023), these prospective and retrospective studies often reflect real-world rather than experimental situations (Saturni et al., 2014). Therefore, these studies can also provide valuable insights into service delivery. Unfortunately, these studies often lack comprehensive descriptions of the content of end-of-life care services and how service is delivery in practice, thereby introducing uncertainty into the actual implementation of care models. As noted previously, the lack of comprehensive descriptions of these interventions also hinders the ability to establish meaningful comparisons (Smith et al., 2014).
Applicability, completeness and quality of the evidence
Because of the academic challenges within pertaining to the terminologies of palliative care and end-of-life care in this field, these studies used the broader term “palliative therapy” instead of “end-of-life care”, although the interventions in these studies exhibited characteristics of the end-of-life care service (Brian Cassel et al., 2016; Holley et al., 2009; Pereira et al., 2023). This issue appears to be a common occurrence in research within the palliative and end-of-life care domains (Malcolm et al., 2020), potentially leading to ambiguity in the interpretation and application of study findings.
Furthermore, it is necessary to interpret the findings of this review considering certain limitations. Due to ethical and methodological challenges (Akdeniz et al., 2021; Chen et al., 2014; Sampson et al., 2018), the number of studies eligible for inclusion in this review is relatively limited. This limitation resulted in many key outcome indicators receiving attention from an extremely limited number of studies. For example, quality of life, end-of-life comfort, survival, non-palliative interventions, and grief among family caregivers are all areas where only one study has focused (Hum et al., 2020; Luth et al., 2021; Mitchell et al., 2004; Tay et al., 2020; Treloar et al., 2009). While the review finds these results all demonstrate positive outcomes, some marginally significant outcomes may be the consequence of chance. For example, the results of a previous review clearly indicated that end-of-life care at home did not have an impact on caregivers’ grief (Gomes et al., 2016).
It is also important to note that many factors contributed to the heterogeneity of the results. In particular, some retrospective reporting may be affected by recall bias after the patient’s death, family members’ recall aspects are more generally limited (Song et al., 2016). Studies conducted at different times after patient death also contribute to heterogeneity in results (Claxton-Oldfield et al., 2010). Because patient end-of-life outcomes are more likely to be proxy-reported by family caregivers, the goals and values of family members are subject to change with time, resulting in their inability to accurately recall perceptions at a given point in time, which generates variability in measurement outcomes (Ernecoff et al., 2021). The diversity in study designs, outcome measurements, and the complexity of instruments used for outcome assessment in the studies included in this review also contributed to the heterogeneity of the study results. As a result, effectiveness assessments of home-based end-of-life care services has many methodological limitations, which hindered the ability to provide a definitive answer on the effectiveness of home-based end-of-life care services for people with dementia.
The absence of clear interventions and the variability in outcome measures also posed challenges in establishing associations between specific end-of-life care processes and outcomes in this review. These factors hindered the comparison of outcomes and synthesis of evidence, potentially impacting the generalizability of the findings. As described in previous studies the existing evidence base is too weak to robustly assess the effectiveness of home-based end-of-life care interventions for people with dementia (Miranda et al., 2019). Consequently, drawing accurate conclusions about the evidence of end-of-life care at home for people living with dementia proved to be a challenging task. Indeed, the lack of certainty in the evidence reflects the difficulties of conducting research in this area. Many studies examining home hospice and palliative care have struggled to draw specific conclusions (Hammer et al., 2023; Miranda et al., 2019; Shepperd et al., 2021).
Although the evidence supporting home-based end-of-life care for people living with dementia is limited, most of the studies reviewed reported positive results. This supports the intuitive hypothesis that home-based end-of-life care is beneficial for people with dementia, and that home-based end-of-life care services provide better opportunities for this population who want to die at home.
Implications for research and practice
This review provides multiple insights that point to current research and evidence gaps in home-based end-of-life care for people living with dementia. To promote the development of this field, it is imperative for future studies to focus on the following aspects. Firstly, there is an urgent need for more research to develop and evaluate home-based end-of-life care services for people living with dementia. Considering the ethical challenges in conducting randomized controlled trial studies can be complex, future study designs such as case control studies could prioritize large samples with carefully matched intervention and control groups. Furthermore, future research endeavors to prioritize the utilization of consistent, standardized, and validated outcome measures are used to ensure accuracy and comparability of findings. Finally, it is crucial to consider the perspectives and needs of people with dementia, family caregivers, and healthcare professionals when delivering home-based end-of-life care. Addressing these stakeholders’ expectations will not only improve care services but also advance research in optimal home-based end-of-life care for people living with dementia.
It is also worth considering that the current lack of research may reflect a broader reality that while remaining at home until the end of life is often idealized, many people with dementia either choose not to stay at home at the end of life (Gott et al., 2004) or are forced to transition to other care settings due to the increasingly complex and demanding nature of their care needs (Seamark et al., 2014). The progressive nature of dementia often requires a level of intensive support and specialized medical attention that may surpass the capacity of home environments, even with family involvement (Mogan et al., 2018). This potential disconnect between the idealized vision of home-based end-of-life care and the practical realities faced by people with dementia and their families highlights an area worthy of further research. Consequently, future studies should also explore the barriers and facilitators that affect home-based end-of-life care for people with dementia, which could further illuminate the intricacies of providing effective home-based end-of-life care and is critical to improving care outcomes and advancing the overall understanding of optimal home-based end-of-life care for people living with dementia.
What this review adds?
This review adds new insights into home-based end-of-life care for people with dementia. This review highlights that feasible and favorable outcome associated with such care, including reduced healthcare service utilization and costs, along with increased opportunities for patients to spend their final days at home. While the findings of this review consistent with previous systematic reviews (Candy et al., 2011; Grossoehme et al., 2020; Shepperd et al., 2021), this consistency is not surprising because it reflects the consensus in the field. But this review is unique in that it focuses on people living with dementia, drawing on the latest literature to shed light on the interventions and effectiveness of home-based end-of-life care services for people with dementia, filling a gap in previous evaluations of home-based end-of-life care services for this population. In addition, to provide a comprehensive assessment of home-based end-of-life care for people with dementia by combining quantitative and qualitative evidence, thereby adding variety and depth to the findings. This review also points out the limitations of existing research on home-based end-of-life care for people living with dementia and clear directions for future research.
Conclusion
Home-based end-of-life care services provide better opportunities for people with dementia who want to die at home. However, interpretation of the evidence for home-based end-of-life care interventions for people living with dementia is constrained by the number of studies and methodological limitations. Additionally, the ambiguity of the study interventions and the heterogeneity of the outcome measures and outcome metrics, further complicate the interpretation of results. Therefore, although this review found other positive outcomes for home-based end-of-life care for people living with dementia, it cannot be conclusively assumed that these findings offer a definitive answer to the impact of home-based end-of-life care services. Given the urgent need for home-based end-of-life care for people with dementia and their family caregivers, there is still a need for more rigorous research to generate stronger evidence.
Footnotes
Author’s note
The protocol was registered in the PROSPERO international Prospective Register of Systematic Reviews database (No. CRD42023454547).
Authors’ contributions
GY: Conceptualization and design; Writing – original draft and final version; LM: Review and editing; Formal analysis; Supervision; DS: Review and editing; Formal analysis; Supervision; YW: Article selection; Data curation; Validation; LZ: Data curation; Validation; HC: Data curation; Validation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.