
Abstract
Introduction:
Adrenal venous sampling is useful for discriminating unilateral and bilateral hypersecretion in patients with primary aldosteronism, but it is relatively invasive. To determine the site of hypersecretion more non-invasively, we evaluated predictors of unilateral hypersecretion.
Materials and methods:
We evaluated the baseline characteristics and the results of confirmatory tests of 123 patients with primary aldosteronism who underwent adrenal venous sampling.
Results:
Unilateral hypersecretion was identified in 22.0%. The plasma aldosterone concentration and aldosterone–renin ratio were significantly higher and serum potassium concentration and plasma renin activity were significantly lower in patients with unilateral hypersecretion. Plasma aldosterone concentrations after captopril challenge test, saline infusion test and rapid adrenocorticotropic hormone stimulation test were significantly higher among patients with unilateral hypersecretion. The plasma aldosterone concentration reduction ratio in saline infusion test and plasma aldosterone concentration elevation ratio during rapid adrenocorticotropic hormone stimulation test were significantly higher in patients with unilateral hypersecretion. However, areas under the curve for these parameters were not superior to the values after confirmatory tests.
Conclusions:
The plasma aldosterone concentration values after captopril challenge test, saline infusion test and rapid adrenocorticotropic hormone stimulation test were useful for identifying patients with unilateral hypersecretion. However, value changes or ratios during confirmatory tests are less useful for this aim.
Keywords
Introduction
Primary aldosteronism (PA) is one of the leading causes of secondary hypertension, and is considered an important cause for resistant hypertension.1,2 Patients with PA are reported to experience cardiovascular events such as stroke, coronary artery disease, heart failure and atrial fibrillation more frequently than patients with essential hypertension.3–5 The diagnosis of PA in the early stage is thus exceedingly important to avoid these complications. Aldosterone-producing adenoma (APA) is a particularly important type of PA that can reportedly be cured, at least partially, by adrenalectomy.6,7 A recent report from Japan advocated that although no differences in the incidence of cerebrovascular or cardiovascular disease existed between patients treated with mineralocorticoid receptor antagonist and adrenalectomy, oral antihypertensive agents were able to be reduced more often in patients who underwent adrenalectomy. 8 In addition, in PA patients, adrenalectomy is not only efficient for improving mortality, 9 but is also beneficial for reducing end-stage renal disease, 9 incident atrial fibrillation 10 and even the risk of sepsis. 11
Adrenal vein sampling (AVS) is the gold standard to determine the site of aldosterone hypersecretion in PA. 12 Recent guidelines have recommended performing AVS to distinguish between unilateral and bilateral forms of PA.13–15 However, AVS is expensive and invasive, and cannot be performed for all patients with PA.
Several recent reports have advocated the results of baseline laboratory data, confirmatory tests, 11 C-metomidate positron emission tomography (PET)-computed tomography, and 18-oxocortisol as reliable methods for discriminating between uni and bilateral PA,16–20 and suggesting the possibility of substituting this process for AVS. Moreover, the rapid adrenocorticotropic hormone (ACTH) test has recently been proposed as useful for determining subtypes of PA.21,22
However, few reports have examined the diagnostic significance of value changes in confirmatory testing for diagnosing the lateralisation of PA. In fact, although use of the plasma aldosterone concentration (PAC) suppression ratio in the captopril challenge test (CCT) is recommended for PA diagnosis, 13 the utility of the PAC suppression ratio has been contradicted in recent reports.23,24
We have compared patients with uni and bilateral aldosterone hypersecretion to elucidate indicators for distinguishing between these types.
Materials and methods
Study population
Participants comprised 123 patients who were finally diagnosed with PA based on the the Japanese Society of Hypertension (JSH) guideline 15 in our hospital between 2011 and 2019. In detail, all patients fulfilled the following criteria: aldosterone–renin ratio (ARR) greater than 200; PAC greater than 120 pg/ml; and at least one confirmatory test result from CCT, saline infusion test (SIT), or furosemide upright test (FUT). Our study protocol was approved by the ethics committee of the Jikei University School of Medicine (no. 31-213), and informed consent was obtained from all patients participating in the study. Baseline blood samples were collected after the patient had remained in a recumbent position for at least 30 minutes. Urine samples were obtained at the same time. As urine samples were taken at an arbitrary time, the urinary noradrenaline concentration was normalised to urinary creatinine concentration. Urinary sodium and potassium were estimated using previously described formulae.15,25 In detail, the estimated amount of creatinine excreted per day was calculated using the formula (–2.04 × age + 14.89 × body weight (kg) + 16.14 × height (cm) – 2244.45 mg/day), then the estimated amount of sodium excreted per day was calculated as 21.98 × {(urinary sodium concentration/urinary creatinine concentration) × estimated creatinine excretion}0.392. Similarly, the estimated amount of potassium excreted per day was calculated as 7.59 × {(urinary potassium concentration/urinary creatinine concentration) × estimated creatinine excretion}0.431. All blood and urine samples were examined by SRL Inc. (Tokyo, Japan). Antihypertensive agents other than calcium antagonists and α-blockers were withdrawn at least 6 weeks before baseline examination. All patients underwent computed tomography (CT) to identify the presence of adrenal adenoma. Patients who had visible adenoma on CT underwent a 1 mg dexamethasone suppression test, as previously described 26 and no patients were diagnosed with subclinical Cushing’s syndrome or Cushing’s syndrome.
Confirmatory testing
The CCT, FUT and SIT were performed as described before. 15 In the CCT, blood samples were obtained just before and 90 minutes after the patient received 50 mg of oral captopril. There are three criteria for CCT in the current guideline:13,15 (a) ARR after CCT greater than 200; (b) PAC after CCT greater than 120 pg/ml; and (c) PAC after CCT greater than PAC before CCT × 0.7. We therefore evaluated CCT in terms of these three criteria separately. In the FUT, blood samples were obtained just before and 2 hours after the patient received intravenous injection of 40 mg of furosemide. Plasma renin activity (PRA) less than 2.0 ng/ml/hour was defined as positive. In the SIT, blood samples were obtained just before the patient started intravenous infusion of 2 L of saline over 4 hours. PAC greater than 60 pg/ml was defined as positive.
With regard to CCT, FUT and SIT, the PRA and PAC after stimulation and the amount and rate of change at the confirmatory testing were evaluated. With respect to the rapid ACTH stimulation test, PAC/F ratio after stimulation and the amount and rate of change of PAC at confirmatory testing were evaluated.
Rapid ACTH stimulation test
Although not included in current guidelines, it is reported that the rapid ACTH stimulation test is useful not only for the diagnosis of PA but also discriminating APA.22,27 Therefore, the usefulness of the rapid ACTH stimulation test for discriminating unilateral hypersecretion in our cohort was also evaluated. In the rapid ACTH stimulation test, blood samples were obtained just before and 60 minutes after the patient received 250 μg of tetracosactide acetate. PAC/cortisol (F) greater than 8.5 was defined as positive as previously described. 27
Adrenal vein sampling
AVS was carried out on another day. Blood samples from the inferior vena cava (IVC) and bilateral adrenal veins were obtained before and 20 minutes after ACTH stimulation (intravenous bolus infusion of 250 μg of tetracosactide acetate). Adequate catheterisation was defined as adrenal venous cortisol concentration after ACTH stimulation of 200 μg/dl or greater, and adrenal cortisol concentration after ACTH stimulation five or more times the cortisol concentration from the IVC, as described in the guideline. 14 PAC concentration after ACTH stimulation greater than 14,000 pg/ml from the adrenal vein on at least one side was defined as aldosterone hypersecretion. In addition, after ACTH stimulation, the bilateral adrenal venous aldosterone/cortisol (A/C) ratio was calculated. A lateralised ratio (A/C ratio on the high-value side/low-value side) of 2.6 or greater and contralateral ratio (A/C ratio on the low-value side/high-value side) less than 1 was defined as unilateral aldosterone hypersecretion. 14
Statistical analysis
Data are described as mean ± standard deviation. Values of P<0.05 were considered significant. The comparison between uni and bilateral hypersecretion was evaluated by the Mann–Whitney U test. Multivariate logistic regression models were employed to elucidate factors predicting unilateral hypersecretion. Associations between parameters were analysed by Pearson’s product-moment correlation coefficient. Receiver operating characteristic (ROC) analysis was performed to compare diagnostic abilities for the purpose of discriminating unilateral from bilateral aldosterone hypersecretion of each baseline characteristic and results from each confirmatory test. The cut-off value was set on the basis of the point closest to the upper left corner of the ROC curve. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R (the R Foundation for Statistical Computing, Vienna, Austria). More precisely, EZR is a modified version of R Commander designed to add statistical functions frequently used in biostatistics. 28
Results
Patient characteristics
A total of 123 patients were included. Mean age was 49.9±10.7 years, and 58.3% of patients were men. All patients underwent CT, and visible adenoma was identified in 40.7% of patients. Unilateral hypersecretion was shown in 22.0% of patients by AVS. In terms of pharmacotherapy, 62.6% of patients received only calcium antagonists, and 4.1% of patients received calcium antagonists and α-blockers. Baseline values of PRA, PAC and ARR were 0.46±0.34 ng/ml/hour, 228.8±155.8 pg/ml and 876.6±1566.1, respectively. Estimated sodium intake was 146.4±41.4 mEq/day. Among 123 patients, for CCT, 75.2%, 64.1% and 56.1% of patients were positive for each criterion that: (a) ARR after CCT greater than 200; (b) PAC after CCT greater than 120 pg/ml; and (c) PAC after CCT greater than PAC before CCT × 0.7. Besides, 84.9%, 74.8% and 88.0% of patients showed positive results for the FUT, SIT and rapid ACTH stimulation tests.
Difference in characteristics between uni and bilateral hypersecretion
We compared patients with uni and bilateral hypersecretion with respect to various baseline characteristics (Table 1). Visible adenoma was more likely to be apparent in patients with unilateral hypersecretion. Serum sodium concentration tended to be higher and serum potassium concentration was significantly lower in patients with unilateral hypersecretion. PRA was significantly lower and PAC and ARR were significantly higher in patients with unilateral hypersecretion.
Comparison between uni and bilateral hypersecretion.

ACTH: adrenocorticotropic hormone; ARR: aldosterone–renin ratio; PAC: plasma aldosterone concentration; PRA: plasma renin activity.
We subsequently compared the positive rate, PRA and PAC values after confirmatory tests, and PRA and PAC value change during confirmatory tests (Table 1). The positive rate of CCT (other than criterion (c), SIT and rapid ACTH stimulation test were significantly higher in patients with unilateral hypersecretion. In addition, PAC value after CCT, PAC value after SIT and PAC and PAC/F value after rapid ACTH testing were significantly higher in patients with unilateral hypersecretion. The positive rate of FUT and PRA value after FUT did not differ between uni and bilateral hypersecretion. Although PAC change value and ratio in CCT and PRA change value and ratio in FUT did not differ between uni and bilateral hypersecretion, PAC reduction ratio in SIT, and PAC/F elevation value and ratio in the rapid ACTH stimulation test were significantly higher in patients with unilateral hypersecretion.
In patients with visible adenoma, serum potassium concentration and PRA were significantly lower and PAC and ARR were significantly higher in patients with unilateral hypersecretion. Although positive rates for each confirmatory test did not differ between uni and bilateral hypersecretion, PAC value after CCT, PAC value after SIT and PAC and PAC/F value after rapid ACTH test were significantly higher in patients with unilateral hypersecretion as compared to patients with bilateral hypersecretion. With regard to the value change and ratio of PRA and PAC in confirmatory tests, only PAC reduction rate in SIT differed significantly between the two groups (Table 2).
Comparison between uni and bilateral hypersecretion in patients with visible adenoma on CT.
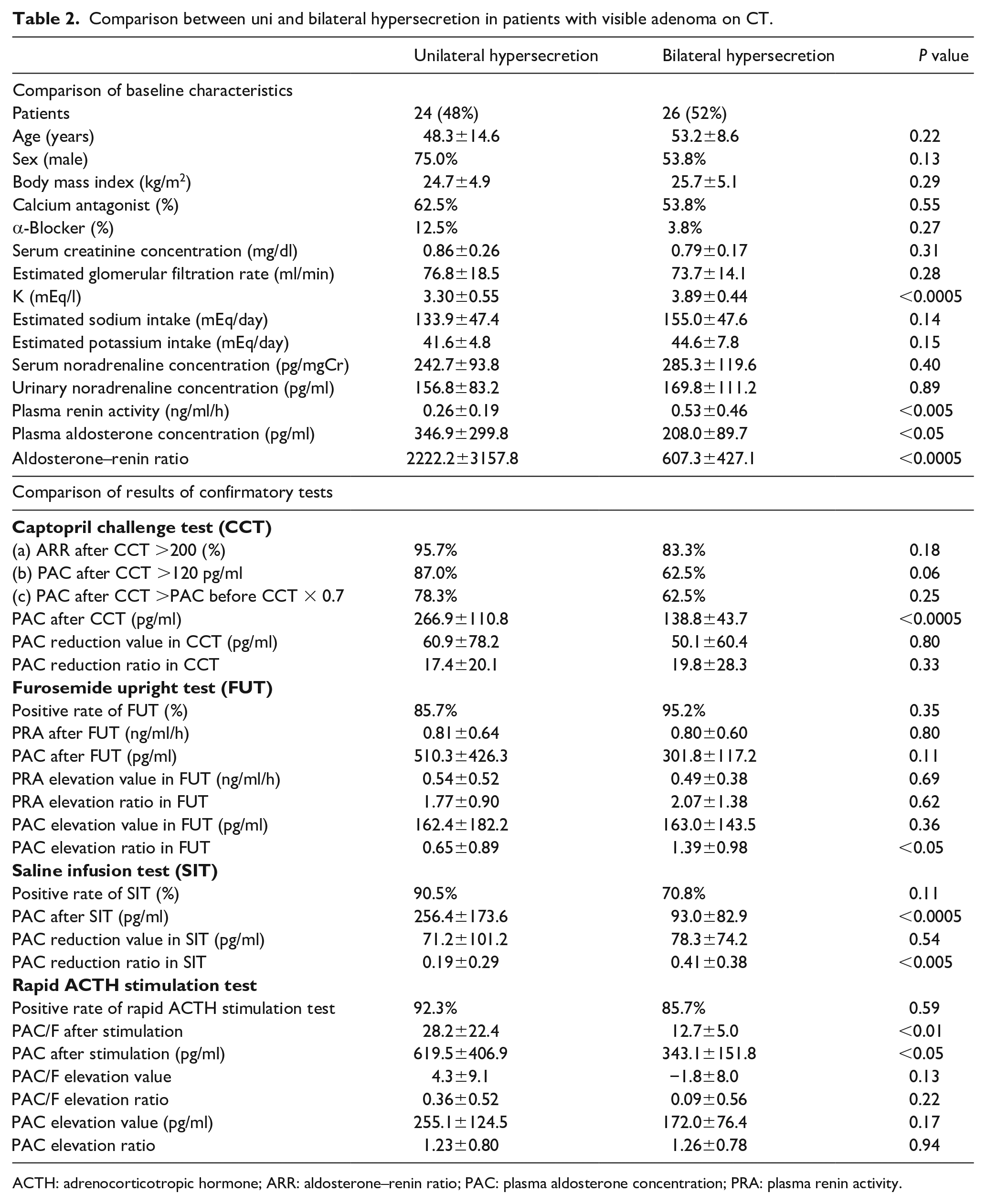
ACTH: adrenocorticotropic hormone; ARR: aldosterone–renin ratio; PAC: plasma aldosterone concentration; PRA: plasma renin activity.
In patients without adenoma, baseline characteristics of patients with uni and bilateral hypersecretion showed no significant difference. Positivity rates for each confirmatory test also did not differ significantly between groups. With regard to value changes and ratios of PRA and PAC in confirmatory tests, only PAC value after the rapid ACTH stimulation test was significantly higher in patients with unilateral hypersecretion (Table 3).
Comparison between uni and bilateral hypersecretion in patients without visible adenoma.
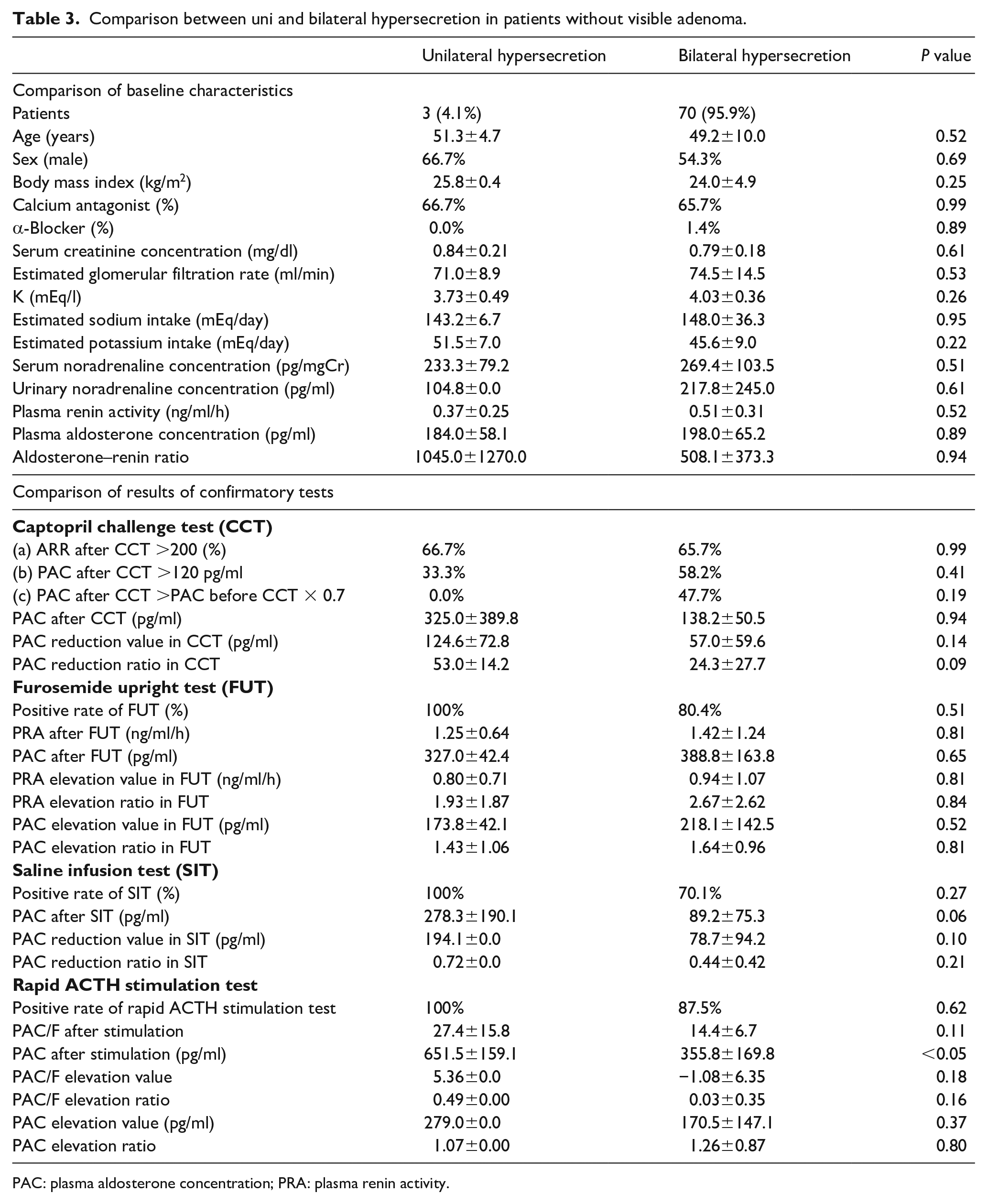
PAC: plasma aldosterone concentration; PRA: plasma renin activity.
Predictors of unilateral hypersecretion
We performed logistic regression analysis for baseline variables predicting unilateral hypersecretion. We included sex, visible adenoma, serum potassium concentration, estimated sodium intake, baseline PRA and baseline PAC in the model, and revealed visible adenoma (odds ratio 17.1, 95% confidence interval (CI) 3.3–89.0; P<0.0001) and serum potassium concentration (odds ratio 0.037, 95% CI 0.007–0.205; P<0.0005) as independent predictors of unilateral hypersecretion.
Consequently, with regard to the result and value change and ratio of confirmatory tests, we included baseline PRA, baseline PAC, PAC after CCT, PAC reduction value and ratio in CCT, PRA after FUT, PRA elevation value and ratio in FUT, PAC after SIT, PAC reduction value and ratio in SIT, PAC/F and PAC after rapid ACTH stimulation test, and PAC elevation value and ratio in rapid ACTH stimulation test in our model. This analysis revealed only PAC after SIT as an independent predictor of unilateral hypersecretion (odds ratio 1.02, 95% CI 1.01–1.03; P<0.005).
Finally, ROC curve analyses were performed to evaluate the diagnostic abilities of baseline characteristics and results of each confirmatory test (Table 4). Among the baseline characteristics, baseline ARR showed the highest area under the ROC curve (AUC) (AUC 0.791, 95% CI 0.678–0.903, optimal cut-off 903.3, sensitivity 66.7%, specificity 89.6%). Moreover, the AUC for serum potassium concentration was 0.829 (optimal cut-off 3.50 mEq/l, sensitivity 70.4%, specificity 88.5%). For PRA and PAC after confirmatory tests, PAC after SIT showed the highest AUC (AUC 0.825, 95% CI 0.711–0.938, optimal cut-off 130.0 pg/ml, sensitivity 75.0%, specificity 85.7%). Among PRA or PAC change values or ratios from confirmatory tests, the AUC for PAC reduction ratio in SIT was highest (AUC 0.742, 95% CI 0.614–0.869, optimal cut-off 41%, sensitivity 76.2%, specificity 65.2%). However, none of these indices showed superiority to the value after confirmatory tests.
ROC curves for predictors of unilateral hypersecretion.

ACTH: adrenocorticotropic hormone; ARR: aldosterone–renin ratio; CI: confidence interval; PAC: plasma aldosterone concentration; PRA: plasma renin activity; ROC: receiver operating characteristic.
Combination of two confirmatory tests for diagnosis of unilateral hypersecretion
We compared combinations of two confirmatory tests based on the cut-off value derived from the ROC curve described above for the diagnosis of unilateral hypersecretion (ARR after CCT >380.0, PRA after FUT <0.70 ng/ml/hour, PAC after SIT >130 pg/ml, and PAC/F after ACTH stimulation >16.2) (Table 5). Among the six combinations of diagnostic criteria, the combination of CCT and SIT (AUC 0.815, 95% CI 0.714–0.915, sensitivity 65.2%, specificity 97.7%) and CCT and rapid ACTH stimulation test (AUC 0.844, 95% CI 0.719–0.968, sensitivity 71.4%, specificity 97.3%) showed relatively high AUC.
Diagnostic value of dual confirmatory tests for the diagnosis of unilateral hypersecretion.
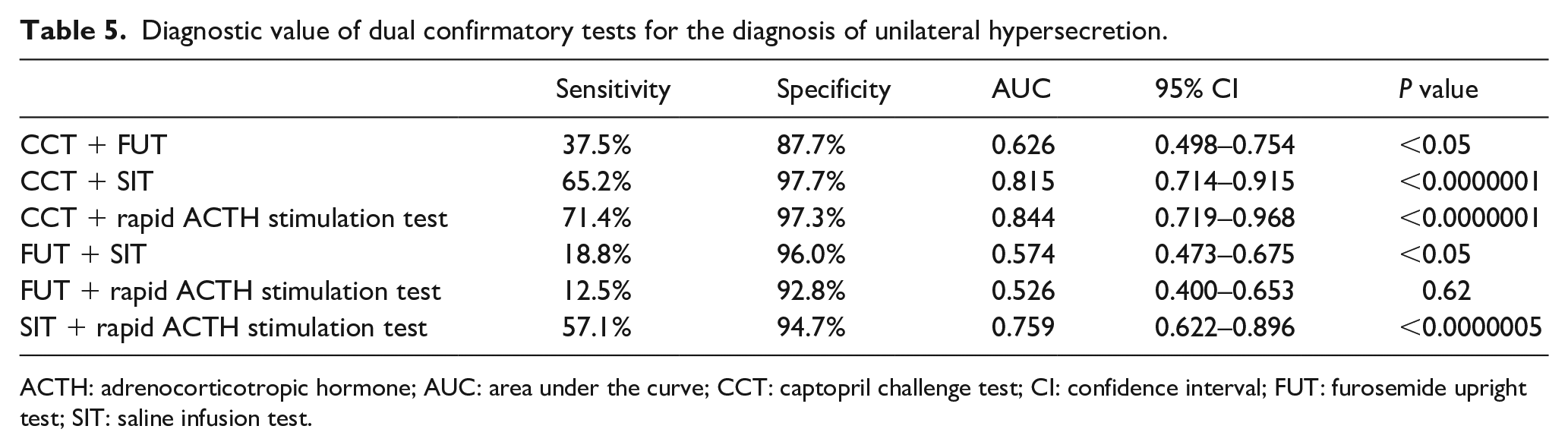
ACTH: adrenocorticotropic hormone; AUC: area under the curve; CCT: captopril challenge test; CI: confidence interval; FUT: furosemide upright test; SIT: saline infusion test.
Discussion
First, we demonstrated that PAC and ARR were higher, and serum potassium concentration and PRA were lower in patients with unilateral hypersecretion. With regard to serum concentrations of electrolytes, our findings support a previous report describing the frequency of hypokalemia as higher in APA than in idiopathic hyperaldosteronism (IHA) (APA 48.0%; IHA 16.9%). 29
In addition, a recent report demonstrated that serum potassium concentration was useful for discriminating APA from IHA (optimal cut-off 3.45 mEq/l, sensitivity 62.5%, specificity 93.0%). 18 Similarly, some reports have described baseline ARR as useful for the diagnosis of APA. ARR is generally considered useful for PA diagnosis. 30 Moreover, a supine ARR at a cut-off value of 32 ng/ng is proposed to be useful for APA diagnosis with 92% sensitivity and 92% specificity. 31 Therefore, as in previous reports, we demonstrated that baseline serum potassium concentration and ARR value are important predictors of unilateral hypersecretion. However, in the present study, although the cut-off value for serum potassium concentration was similar to previous studies (3.5 mEq/l in our study), the cut-off value for ARR was markedly different (903.3 in our study). Given this discrepancy, we further examined other factors that could be estimated to determine the site of hypersecretion non-invasively.
In our study, patients with unilateral hypersecretion were more likely to show positive results for the CCT and SIT. Likewise, PAC and ARR after CCT, PAC after SIT, and PAC/F ratio after rapid ACTH stimulation test were significantly higher in patients with unilateral hypersecretion. Various confirmatory tests are recommended to confirm PA diagnosis in the current guidelines.13–15 PACs after CCT, SIT and the fludrocortisone suppression test (FST) are reportedly significantly higher in PA, 24 and the FUT, which was not evaluated in this report, is frequently used in Japan due to the high prevalence of low-renin hypertension associated with high sodium consumption. 32 These confirmatory tests are therefore considered equally useful for the diagnosis of PA. However, few reports have described these confirmatory tests as useful for differentiating between unilateral and bilateral hypersecretion.
Recently, ARR after CCT, PRA after FUT and PAC after SIT have been demonstrated as equally useful for discriminating APA from IHA. 18 In another recent report, PRA after FUT was significantly lower in APA than in IHA, 22 representing a difference from our report. Although we could not elucidate the precise reason for this discrepancy, they applied a 1 mg/kg dose of furosemide for the FUT, which is much more than the dose adopted in our study, which might have contributed to this difference. Moreover, although we lack data for direct comparison, the results of FUT might be influenced by sodium intake.
We revealed that PAC after SIT showed the highest AUC among several confirmatory tests, along with relatively high specificity. Some reports have examined the diagnostic significance of SIT for PA or APA diagnosis. Mulatero et al. proposed the SIT as easier to apply than the FST, suggesting it as a good alternative to the FST for PA diagnosis. 33 Furthermore, Nanba et al. proposed that SIT is also useful for discriminating APA from IHA, and a cut-off of 311 pg/ml provides 100% specificity (50% sensitivity), 17 providing utility in the definitive diagnosis of APA. We therefore assume that the SIT offers one of the most reliable tools to discriminate unilateral hypersecretion from bilateral hypersecretion.
Recently, the ACTH stimulation test has been proposed as a reliable tool for PA diagnosis. 34 In fact, some reports support the utility of this test for discriminating APA from IHA.20,35,36 In our study, ACTH stimulation proved as useful as other confirmatory tests such as the CCT or SIT. The ACTH stimulation test is easier to perform than other confirmatory tests, and so might offer a good alternative to those examinations.
We also demonstrated that although some of the PRA or PAC change values and ratios are useful for discriminating unilateral hypersecretion from bilateral hypersecretion, they are inferior to assessment of baseline characteristics and the results of confirmatory tests. Several reports have evaluated PAC changes between before and after confirmatory tests. Although a percentage PAC suppression in CCT less than 30% has been recommended as a criterion for the CCT in the Endocrine Society clinical practice guideline, 13 two recent reports suggested PAC value after the CCT rather than the degree of PAC decline as better suited to PA diagnosis.23,24 Although both reports were relatively against using the reduction rate of PAC for PA diagnosis, discrimination between APA and IHA was not mentioned. On the other hand, patients with APA have previously been shown to display a smaller reduction in PAC on the SIT compared to IHA patients. 33
In this study, PAC reduction ratio in CCT and PRA augmentation rate in FUT did not differ significantly between uni and bilateral hypersecretion. On the other hand, PAC reduction rate in SIT was significantly lower in patients with unilateral hypersecretion. Recently, Nagano et al. demonstrated that the combination of PAC reduction rate in SIT and PAC after SIT is a useful criterion for discriminating unilateral hypersecretion from bilateral hypersecretion, 37 which is consistent with our study. Although not only our study but their study did not purely compare the diagnostic significance of each value after confirmatory tests and the value changes in the confirmatory tests, in our study, the PAC value after CCT or SIT tends to be superior to the value change of PAC in SIT.
In contrast, alterations to PAC and PAC/F value by ACTH stimulation were significantly higher in patients with unilateral hypersecretion, meaning that patients with unilateral hypersecretion were more sensitive to ACTH stimulation than IHA patients. This could be useful for discriminating unilateral hypersecretion from bilateral hypersecretion. However, as none of the AUCs for the PAC change during confirmatory tests were superior to AUCs of baseline characteristics and values after confirmatory tests, value changes during confirmatory tests might be less useful.
Nevertheless, AVS is a gold standard for definitive diagnosis of unilateral hypersecretion and is necessary for considering partial excision of the adrenal gland. However, consideration about the result of various confirmatory tests which we demonstrated to be applicable for discriminating the patients with unilateral hypersecretion might be useful at least for selecting the candidates for AVS, or recommending AVS for the patients not willing to undergo AVS.
Conclusion
In conclusion, the CCT and SIT are beneficial methods for differentiating unilateral hypersecretion from bilateral hypersecretion even when used alone, and combination of the CCT and SIT or CCT and rapid ACTH stimulation test may prove valuable for differentiating these pathologies. Moreover, PAC changes during confirmatory tests were useful for discriminating unilateral hypersecretion from bilateral hypersecretion in our study. These factors should be taken into account when trying to diagnose unilateral hypersecretion of aldosterone without performing AVS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.