
Abstract
Objective:
In this article, we aim to prove the safety and effectiveness of orthotopic renal autotransplantation using ex vivo repair for the treatment of complex renovascular hypertension (RVH).
Methods:
We retrospectively reviewed five consecutive patients (three women, two men) with young-onset RVH from January 2009 to August 2014. Orthotopic renal autotransplantation using ex vivo repair was performed and perioperative data were collected for statistical analysis.
Results:
The median age at diagnosis was 20 years (range, 11 to 27 years). Technique success was achieved in all the patients with no in-hospital or late deaths. During a median follow-up of 3.4 years (range, 1.5 to 6 years), the postoperative blood pressure was decreased compared with preoperative level (204 ± 8/133 ± 8 mm Hg vs 129 ± 3/78 ± 5 mm Hg; p < 0.0001). The postoperative anti-hypertensive medications number was reduced (3.4 ± 0.4 vs 0.2 ± 0.2; p < 0.0001). Early and late renal functions were both well preserved as measured by no changes in serum creatinine level (p > 0.05). The primary patent rate was 100% (5/5) at one-year follow-up.
Conclusion:
In our small series, orthotopic renal autotransplantation using ex vivo repair was safe and effective for the resolution of complex young-onset RVH.
Keywords
Introduction
Renal artery stenosis (RAS) is a recognized cause of secondary hypertension, renal dysfunction, and flash pulmonary edema (Pickering syndrome). Atherosclerotic renal artery stenosis (ARAS) is the most common cause of RAS, accounting for more than 90% of cases. 1 Other nonatherosclerotic causes include fibromuscular dysplasia (FMD) and Takayasu arteritis (TA), both of which are important causes of pediatric renovascular hypertension (RVH). 2 Additionally, congenital dysplasia, dissection and other causes have also been reported. Management of RVH consists of proper control of severe hypertension and preservation of the renal parenchyma. Nonatherosclerotic RAS treatment paradigms vary from angioplasty for FMD to anti-inflammatory treatments for TA. Renal artery repairs, whether surgical or endovascular, are essential when hypertension is resistant to antihypertensive medication.
The prognosis of RVH is favorable in young-onset populations, especially in children. The short duration of elevated blood pressure (BP), the absence of atheromatous changes of the arterial system and the usual lack of renal or visceral lesions secondary to hypertension explain the good results of renal artery repair with respect to control of hypertension and preservation of renal function. Long-term results show that the repairs are durable with time and support an aggressive surgical approach toward RVH for the young-onset patient. Percutaneous transluminal renal artery angioplasty (PTRA) and open management of nonatherosclerotic renal artery disease (NARAD) confer long-term benefit for BP, renal function, renal artery/graft patency, and survival. Open revascularization results in superior one- and five-year outcomes compared with endovascular management and provides the most durable outcome for NARAD. 3
A number of studies have demonstrated the safety, durability and clinical benefits on BP and renal function of open reconstructive and renal parenchymal protective techniques in the treatment of complex renal artery disease involving the distal renal artery, segmental branch vessels, or renal hilum.4–8 Management of such lesions, however, is a surgical challenge both in ARAS and NARAD. Kidneys with disease involving segmental branch vessels that were once threatened by nephrectomy have been successfully treated with a myriad of reconstructive techniques and adjuncts, such as ex vivo repair, in situ repair with or without cold preservation, and orthotopic autotransplantation of the repaired kidney.5,9,10 However, thus far few studies have shown that this technique could be effective for the treatment of RVH in young-onset patients.
This retrospective study examined the efficacy of orthotopic renal autotransplantation in young-onset patients by reviewing the short-term and long-term outcomes of five consecutive patients in a single institution.
Methods
Five patients up to 30 years of age who had undergone orthotopic renal autotransplantation, performed by the same senior surgeon (YHZ), for NARAD RVH between January 2009 and August 2014, at the Peking Union Medical College Hospital (PUMCH), China, were included. The duration of hypertension and details of antihypertensive therapy were recorded, as was the presence of comorbidities (as shown in Table 1). All patients had undergone substantial preoperative computed tomography angiography (CTA) (as shown in Figure 1(a)) and renogram as well as intraarterial digital subtraction angiography (DSA) if required to learn the anatomic features of the arterial lesions. For Patient 1, there were severe stenosis located at the orifice of the left renal artery, aneurysm immediately after the narrowing segment, and stenosis at the origin of the right renal artery, and the artery bifurcated into two branches immediately after the dilation. For Patient 2, there was severe stenosis located at the right renal artery caused by the fractured stent (as shown in Figure 1(a)). The bifurcation of the renal artery started from the distal end of the stent. For Patient 3, there was severe stenosis located at the orifice of the right renal artery, and an aneurysm at the right renal hilum involving the first bifurcation of renal artery. For Patient 4, there were coarctation of the abdominal aorta, bilateral renal artery stent, and both of the renal arteries bifurcated into two branches very proximal to the stent. For Patient 5, there was a 1.9 cm aneurysm at the left renal hilum involving the first bifurcation of the renal artery. Pre- and early postoperative data were collected from patients’ records and all patients were invited for a current follow-up examination. The results of three of these patients (Patients 1, 11 4 12 and 5 13 ) have been published elsewhere. The hospital records, imaging studies, and clinic records for all patients were reviewed with the approval of the ethics committee of PUMCH.
Demographic and patient characteristics.
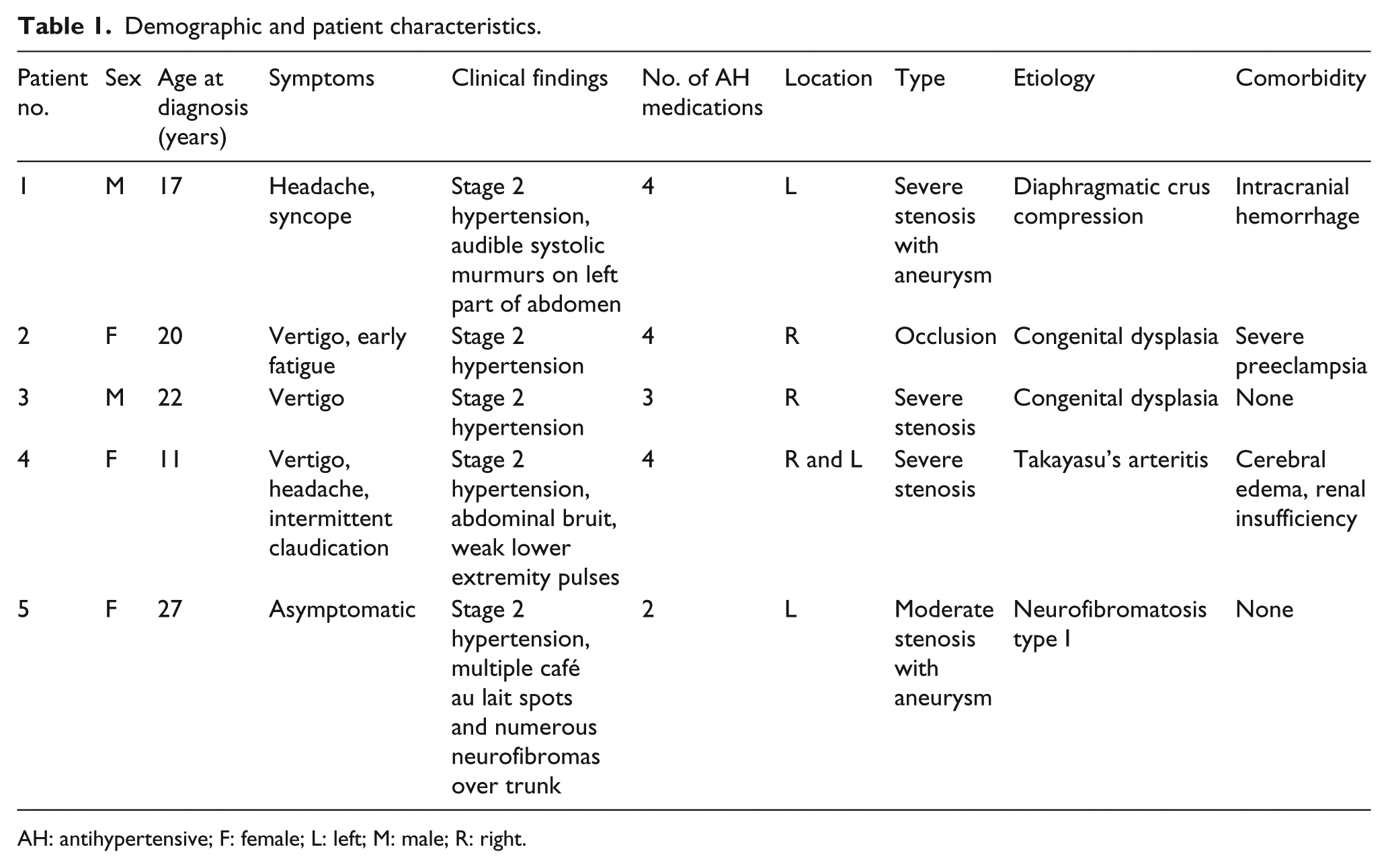
AH: antihypertensive; F: female; L: left; M: male; R: right.
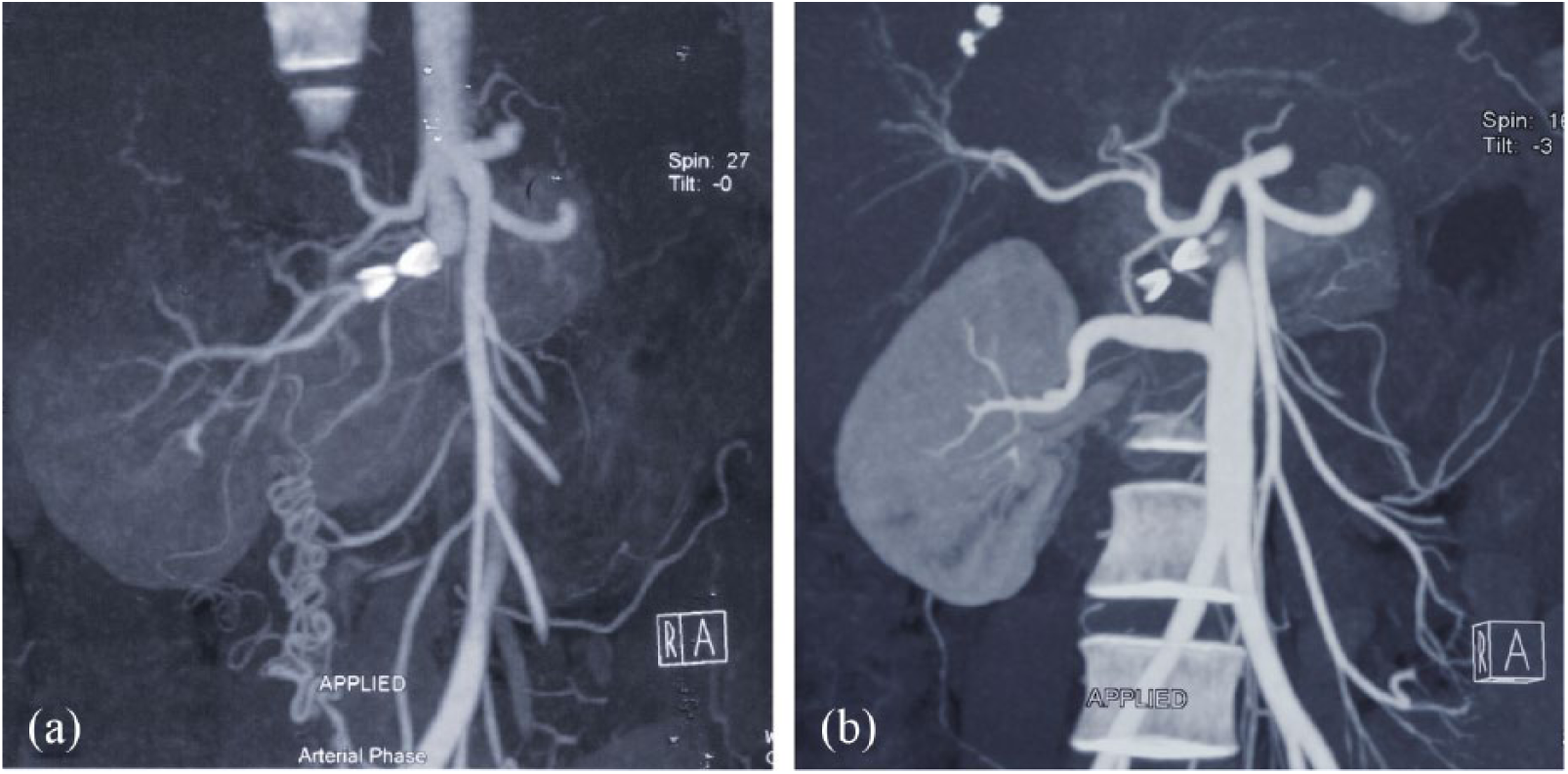
Computed tomography angiography (CTA) of the right renal artery in a 28-year-old patient. (a) Preoperative CTA of the right renal artery in Patient 2. The CTA demonstrating the right renal artery with severe stenosis estimated at more than 80% caused by the fractured stent, the involvement of the bifurcation of renal artery, and the establishment of collateral circulations from the right internal iliac artery. The right kidney showing signs of malperfusion. (b) Preoperative CTA at two-year follow-up showing the saphenous vein graft was patent, the right kidney was well perfused and the collateral circulation disappeared.
Exposure was performed with a midline transperitoneal approach in four operations (4/5), and a subcostal incision in one (1/5). The preferred conduit was the autogenous saphenous vein. Prosthetic material was used for abdominal aortic reconstruction. For adequate exposure, we preferentially perform ex vivo renal exposure and vascular reconstruction with orthotopic replacement (as shown in Figure 2) as described by Ham and Weaver. 10

Intraoperative pictures illustrating the key steps of ex vivo renal artery reconstruction and orthotopic autotransplantation. (a) Cold perfusion of the right kidney with University of Wisconsin solution. (b) Autogenous saphenous vein bypasses connect the renal artery to the abdominal aorta. IVC: inferior vena cava; RV: renal vein; SVG: great saphenous vein graft.
Hypertension was graded by systolic (SBP) and diastolic (DBP) levels of three or more clinical measurements and the number of antihypertensive drugs. Patients’ BP levels were evaluated by the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure classification. 14 BP response was defined as follows: 15
(1) Cured: if an SBP of <140 mm Hg and a DBP of <90 mm Hg were obtained without medication.
(2) Improved: if an SBP of <140 mm Hg and a DBP of <90 mm Hg were obtained with less than the number of medications used preprocedure, or if the patient was uncontrolled with an SBP of >140 mm Hg and/or a DBP of >90 mm Hg before the intervention that improved to an SBP of <140 mm Hg and DBP of <90 mm Hg with the same number of antihypertensive medications used before the intervention.
(3) Failed: if an SBP of >140 mm Hg and a DBP of >90 mm Hg occurred after intervention and there was either no change or an increase in the number of antihypertensive medications.
All appropriate variables were analyzed for normality before descriptive statistics were applied. Continuous variables were summarized as mean ± SEM and compared by two-tailed t tests. Categorical variables were expressed as frequency and percentage. A p < 0.05 was considered statistically significant. Statistical analysis was performed with SPSS version 17.0 (SPSS Inc, Chicago, IL, USA).
Results
During the study period, orthotopic renal autotransplantation using ex vivo repair was performed in five consecutive patients (three women, two men). The median age at diagnosis was 20 years (range, 11 to 27 years). Patient demographics, comorbid characteristics and characteristics of repaired renal artery diseases are summarized in Table 1. All patients had received PTRA but ultimately failed. Therefore, they underwent renal artery reconstruction for alleviation of uncontrolled hypertension and two of them for simultaneous resolution of the renal artery aneurysm.
Perioperative complications that extended the hospital stay occurred in one patient (1/5) as summarized in Table 2. No renal failure or cardiovascular events occurred. Preoperative hypertension was present in all of the five patients (BP, 204 ± 8/133 ± 8 mm Hg; medications, 3.4 ± 0.4; both expressed as mean ± SEM). During a median follow-up of 3.4 years (range, 1.5 to 6 years), three (3/5) were cured, two (2/5) were improved, and none were considered failed after renal artery repair among the five hypertensive patients (Table 2). Considered collectively, hypertensive patients had decreased SBP and DBP (129 ± 3/78 ± 5 mm Hg; p < 0.0001) as well as decreased medication requirements for adequate BP control (medications, 0.2 ± 0.2; p < 0.0001). Early renal function was improved in one patient and preserved in all the other patients after the operations. The mean preoperative serum creatinine (SCr) had no significant changes compared with mean discharge SCr (1.52 ± 0.85 vs 0.76 ± 0.09; p > 0.05). During the follow-up, all patients underwent periodic CTA (as shown in Figure 1(b)) to learn the morphology of the reconstructive graft. All grafts remained patent at last follow-up. No reintervention was required during the follow-up.
Outcome of treatment on patients with renovascular hypertension caused by NARAD.

AH: antihypertensive; BP: blood pressure; NARAD: nonatherosclerotic renal artery disease; SCr: serum creatinine.
Discussion
The clinical features of RVH are remarkable because the tolerance of the elevated BP may extend over a long period of time. 16 It is well known that severe hypertension is an independent predictor of major adverse cardiac events and premature death in patients with NARAD.17–19 Unlike hypertension in the senior population, a large proportion of young-onset hypertension is potentially correctable. In general, the younger the patient and the more severe the hypertension, the more likely a secondary or correctable cause exists. RVH is one of the common causes. The lesions of the renal artery are mostly congenital such as extrinsic compression by the diaphragmatic crus, congenital dysplasia and neurofibromatosis type I, as mentioned above.
The treatment of renal artery lesions includes three complementary methods. Medical treatment is usually the first applied to hypertensive patients, especially in severe cases. Renovascular hypertension is, however, sometimes resistant to antihypertensive therapy. It is estimated that patients with TA and severe hypertension treated with pharmacologic therapy alone have a five-year survival rate of less than 60%. 18 Therefore, the value of surgical revascularization has been recognized for patients with TA. Similarly, NARAD such as extrinsic compression by the diaphragmatic crus, congenital dysplasia and neurofibromatosis type I also needs surgical revascularization to resolve the anatomic abnormity.
PTRA has taken a prominent place in the treatment of renal artery stenoses since the 1980s and it is often performed as the initial therapeutic procedure. However, indications of PTRA in young-onset patients, especially in children, must be carefully discussed. First, angioplasty is not always technically feasible when applied to tight stenosis or the tortuous arterial lumen as in some extensive fibrodysplasia. Second, angioplasty may be unsuccessful in severely fibrotic lesions or in cases of developmental stenosis. Third, angioplasty may be responsible for severe complications such as arterial dissection or rupture. 20 Fourth, the primary patency rate of PTRA is up to 50% to 100%, and decreases with longer follow-up.3,21 Fifth, the presence of a dysplastic aneurysm associated with the stenosis is a contraindication of angioplasty because of the risk of aneurismal rupture. For all these reasons mentioned by Chobanian et al., 14 the indications of PTRA must be reserved in very young, severely hypertensive children as a waiting solution to an age and a size compatible with surgery or to restenoses after surgical repair.
A recent study shows that though endovascular and open management of NARAD confer long-term benefits for BP, renal function, renal artery/graft patency, and survival, open revascularization results in superior one- and five-year outcomes compared with endovascular management and provides the most durable outcome for NARAD. 3 In patients with complex renal artery disease, endovascular management may be unsuccessful and even hazardous as in our series. Because there is a close relationship among the arterial, venous, and collecting system structures in the renal hilus, management of lesions involving the distal renal artery, segmental branch vessels, or renal hilum is a surgical challenge, which demands safe performance of the extensive dissection, precise identification of the involved segments, and meticulous arterial repair while satisfactorily preserving renal function. To solve this problem, renal autotransplantation, which is highly effective for treatment of complex renovascular lesions related to FMD and TA, has been used as an alternative treatment for aneurysmal or complex occlusive disease of the renal artery for more than 40 years. 3 Since the majority of our patients are relatively young, we performed ex vivo reconstructions considering durability a crucial factor.
Some reports have advocated pelvic autotransplantation after ex vivo renal artery repair for several reasons including allowance of a minimum of operative dissection, easier surveillance of the rejection, and facilitating later transplant nephrectomy. There are several conceptual disadvantages of pelvic autotransplantation, however, including the possibility of late failure in patients from progression of atherosclerotic disease, complex subsequent management of the progressive peripheral vascular disease for the location of the autotransplanted kidney, and potential influence on future pregnancy for female patients. Taking these into consideration, for diseases affecting the renal hilar vessels, we favored the theoretical advantages of returning the kidney to the renal fossa at the completion of reconstruction. Because the retrocolic anterolateral exposure of the hilar vessels typically provides adequate visualization for the recognition that an ex vivo reconstruction will be required, the preferred approach for ex vivo reconstruction with autotransplantation is the extended subcostal incision carried to the posterior axillary line combined with a midline xiphoid-to-pubis incision. 4
As the splenic artery is usually of similar diameter to the renal vessel, it can usually be easily spatulated for a direct end-to-end anastomosis to the transected left renal artery. Routine technique often uses splenic vessels to revascularize the left renal artery to reperfuse the kidney graft. However, Benjamin and Dean 22 demonstrated that extraanatomic procedures might not be comparable to direct reconstruction of the renal arteries for the treatment of vascular lesions involving the renal hilum, which is similar to our experience. As to direct reconstruction, a branched segment of the greater saphenous vein is the most commonly employed bypass conduit because it would slightly influence the patients without changing the anatomic features of the renal artery. Therefore, we chose the greater saphenous vein to reconstruct the renal artery.
The results were satisfactory, showing the technique was able to achieve beneficial outcomes, especially in regard to BP response and durability. Owing to the relative rarity of the studied entities, however, there are some limitations to this study, including the relatively small sample size, the retrospective nature of a single institution’s experience and the absence of long-term follow-up data. Nevertheless, more experience and further studies are still required to obtain more information.
Conclusion
NARAD is a common cause of RVH in young-onset patients. Both PTRA and open revascularization confer long-term benefits for patients with NARAD. However, open revascularization results in superior long-term results. For complex renal artery disease, orthotopic renal autotransplantation using ex vivo repair proved safe and effective, in our small series, for medical treatment-requiring complex renovascular hypertension, especially in young-onset patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.