
Abstract
Introduction:
To evaluate the influence of traditional risk factors of ischaemic heart disease and genetic factors to predict different types of acute coronary syndromes.
Materials and methods:
Five hundred and twenty-three patients with acute coronary syndromes (393 with ST elevation myocardial infarction (STEMI) and 130 with non-ST elevation myocardial infarction (NSTEMI)) comprised the study group. The control group consisted of 645 subjects free from symptoms of ischaemic heart disease and stroke. Genetic polymorphisms of MMP-2 (–735) C/T, MMP-2 (–1306) C/T, MMP-3 (–1171) 5A/6A, MMP-9 (–1562) C/T and ACE I/D were evaluated using polymerase chain reaction.
Results:
Patients with acute coronary syndromes more often had ID or II genotype than DD genotype of ACE (P = 0.04) and 5A5A or 5A6A genotype than 6A6A genotype of MMP-3 (P = 0.02) in comparison to the control group. The genotypes of other matrix metalloproteinase genes did not differ between the groups. 5A5A and 5A6A genotypes of MMP-3 (odds ratio (OR) 1.5; P = 0.021), II and ID genotypes of ACE (OR 1.7; P = 0.006) along with traditional ischaemic heart disease risk factors such as smoking (OR 4.9; P = 0.001), hypertension (OR 2.0; P = 0.001), diabetes mellitus (OR 2.9; P = 0.001) and dyslipidaemia (OR 2.1; P = 0.001) increased the risk of STEMI. However, the polymorphism of MMP-3 5A/6A and ACE I/D was not associated with the occurrence of NSTEMI.
Conclusions:
Genetic polymorphisms of MMP-3 5A/6A and ACE I/D along with conventional ischaemic heart disease risk factors increase the risk of the occurrence of STEMI, while having no influence on the pathogenesis of NSTEMI.
Introduction
The morbidity and mortality from cardiovascular diseases in Lithuania is one of the highest among the European Union member states. Ischaemic heart disease (IHD) and acute coronary syndromes (ACSs) comprise the largest portion of cardiovascular diseases.1,2 Epidemiological studies have confirmed that age, smoking, diabetes, dyslipidaemia, hypertension, obesity and gender are independent risk factors for atherosclerosis.3,4 The early detection of patients having a high risk of ACSs is a priority. Different ACS types such as ST elevation myocardial infarction (STEMI) and non-ST elevation myocardial infarction (NSTEMI) lead to a different clinical course of ACSs and outcomes and require different treatments.5,6 So far, there are no data on whether risk factors are different in particular ACS types. Also, great attention has been devoted to the evaluation of genetic variation of certain enzymatic systems, as a potential risk factor in the development of different ACS types. The renin–angiotensin–aldosterone system (RAAS) and the matrix metalloproteinases (MMPs) play a significant role in the pathogenesis of ACSs and the genetic polymorphism of enzymes of RAAS and various MMPs may affect the occurrence of ACSs.7–10 The activation of MMP and RAAS components is also regulated by genetic predisposition.7,8 This suggests that individuals carrying a higher activity allele of the certain gene have increased concentrations of the particular enzymes that play a crucial role in the atherosclerotic plaque instability and rupture, with consequent thrombus formation and the development of a greater extent of myocardial damage.
The aim of this study was to investigate genetic polymorphisms of several MMPs and angiotensin-converting enzymes (ACEs) mostly expected to play a significant role in the pathogenesis of ACSs if hypothesising that the different pathogenesis of the two conditions could be under the influence of the genotype along with traditional IHD risk factors.
Study population and methods
Subjects
Five hundred and twenty-three patients with ACS (393 with STEMI and 130 with NSTEMI) were enrolled into the study. All of them were admitted to the Department of Cardiology of the Lithuanian University of Health Sciences Hospital between 2007 and 2011. All the patients underwent coronary angiography, following percutaneous intervention of the culprit artery and conventional echocardiography.
Acute myocardial infarction (AMI) was defined according to the standard criteria based on clinical symptoms, ECG findings and cardiac enzyme abnormalities. 11 Family history, cardiovascular risk factors and current treatment were obtained from each patient using a standard questionnaire. Hypertension was defined as the presence of elevated systolic (≥ 140 mmHg) and/or diastolic (≥ 90 mmHg) blood pressure or the current use of antihypertensive drugs. A patient was considered as a smoker if he was smoking at the current time or had been a smoker in the past. Diabetes mellitus was identified when dietary treatment and/or medical therapy was required to control blood glucose levels. Dyslipidaemia was defined as serum total cholesterol levels of 5.2 mmol/L or more, low density cholesterol more than 2.6 mmol/L, and/or triglycerides equal to or more than 1.7 mmol/L or the use of statin medication. 12
The control group consisted of 645 subjects free from symptoms of IHD and stroke matching the study group design according to their age and gender. The control group consisted of subjects from a random sample of the Kaunas population screened within the international Health, Alcohol and Psychosocial factors In Eastern Europe (HAPPIE) project, the Countrywide Integrated Non-communicable Disease Intervention (CINDI) project and an international study, the Kaunas Healthy Ageing Study.
Written informed consent was obtained from all the patients, and the study protocol was approved by the Kaunas region ethics committee.
Genetic analysis
The DNA was extracted from the venous blood of patients using the Genomic DNA Purification Kit, according to the recommendations of the manufacturer. Aliquots of purified DNA were stored at –20°C until use in real time quantitative polymerase chain reaction (qPCR) analysis.
ACE gene I/D polymorphism (NCBI SNP identification number rs4340) was performed according to Mayer et al. 13 To minimise errors introduced by the possibility of misreading, the second independent qPCR amplification with a primer pair that recognises the insertion-specific sequence (I allele) was performed in each sample from patients with the DD genotype. The qPCR products were separated on a 2% agarose gel that was stained with 1 μl (10 mg/mL) ethidium bromide. An O’GeneRuler 100 bp DNA Ladder (#SM1143; Thermo Fisher Scientific, Lithuania) was used to evaluate fragment length. Digested qPCR products were evaluated under UV light illumination with the Biometra TI 1 and BioDoc Analyze 2.0 (serial number: 41290-0; 2.26.11.4 BNA U-536) gel documentation system. ACE genotypes were determined from electrophoregrams.
The determination of MMP-2 (–735) C/T (rs2285053) and MMP-2 (–1306) C/T (rs243865) genotype was performed using commercially available genotyping kits: C_26734093 20 and C_3225943_10 (Applied Biosystems, USA). For MMP-3 (–1171) 5A/6A polymorphism genotyping primers and fluorescently labelled probes (Metabion, Germany) listed as follows, were used: forward 5′–GTGGCCAAATATTTTCCCTGTATTT–3′ and reverse 5′–GGCACCTGGCCTAAAGACATT–3′, 5′–6FAM-AAGACATGGTTTTTCCCCCCATCAAA-BBQ and 5′–YAK-AAGACATGGTTTTTTCCCCCCATCAA-BBQ. For MMP-9 (–1562) C/T polymorphism genotyping primers and fluorescently labelled probes (Metabion, Germany), listed as follows, were used: forward 5′–CAGATCACTTGAGTCAGAA–3′ and reverse 5′–GGTGTAGTATCACTCTGTCA–3′, 5′–6FAM-TGGCGCACGCCTATAATACCA-BHQ-1–3′ and 5′–Yakima YellowTM-TGGCGCATGCCTATAATACCAGC-BHQ. Genotyping was performed using a real time qPCR HT 7900 Applied Biosystems instrument, USA.
Statistical analysis
All statistical analyses were conducted using the Software Package for Social Sciences (SPSS) version 19.0 (SPSS, Chicago, IL, USA).
Continuous variables were expressed as means ± standard deviations (SD) when normally distributed, and as medians (25th, 75th percentiles) when not normally distributed. Continuous variables were assessed using the unpaired Student’s t-test and Mann–Whitney U test, as appropriate. Categorical variables are presented as absolute numbers and percentages, and are compared using the χ2 test. Allelic and genotypic frequencies were analysed with the χ2 test. In order to predict ACS in an individual patient, clinical and genetic variables were put into logistic regression analysis. Variables with statistical significance at univariate analysis were further analysed at multivariate analysis. A P value less than 0.05 was considered statistically significant.
Results
Patients with ACS more frequently had arterial hypertension (P = 0.001), diabetes (P = 0.002), dyslipidaemia (P = 0.001) and were more often smokers (P = 0.001). The patients with ACS did not differ from the control group subjects according to weight and family history of IHD (Table 1).
Comparison of IHD risk factors between ACS group and control group patients.

ACS: acute coronary syndrome; AH: arterial hypertension; BMI: body mass index; IHD: ischaemic heart disease; NSD: no statistical difference.
The distribution by gender, mean age and frequency of IHD risk factors, cholesterol level did not differ between the patients with STEMI and NSTEMI (Table 2). Heart rate (P = 0.001), troponin I (P = 0.001), level of glucose (P = 0.03) and white blood cell count (P = 0.001) were higher in STEMI patients when compared to NSTEMI patients. The left circumflex coronary artery had a tendency to be a culprit artery more often in NSTEMI patients in comparison to STEMI patients. The frequency of left anterior descending artery and right coronary artery as a culprit artery was similar between both groups. STEMI patients had significantly decreased left ventricular ejection fraction and more increased wall motion score index (P = 0.001) as compared to NSTEMI patients.
Comparison of clinical characteristics of patients with STEMI and NSTEMI.
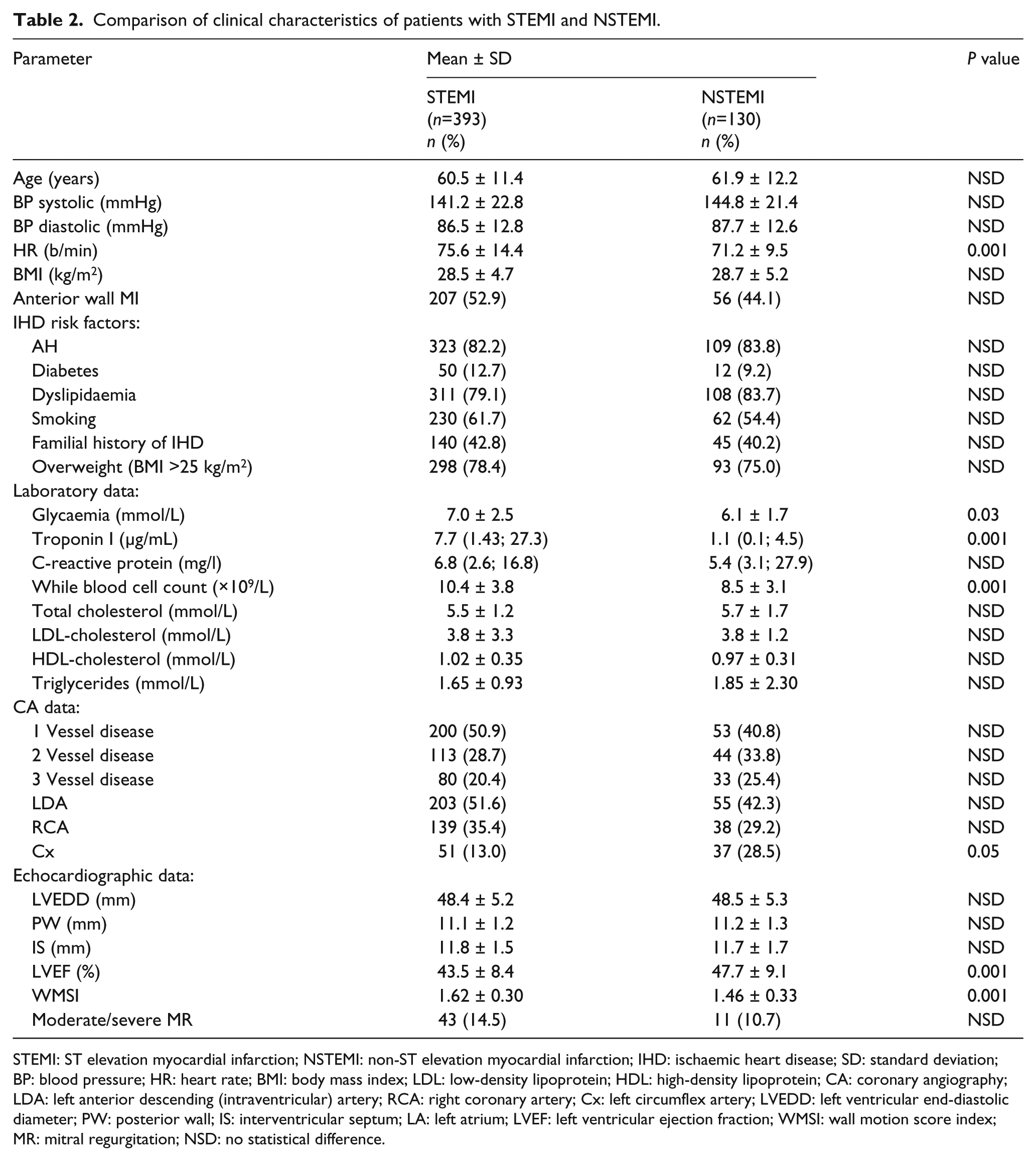
STEMI: ST elevation myocardial infarction; NSTEMI: non-ST elevation myocardial infarction; IHD: ischaemic heart disease; SD: standard deviation; BP: blood pressure; HR: heart rate; BMI: body mass index; LDL: low-density lipoprotein; HDL: high-density lipoprotein; CA: coronary angiography; LDA: left anterior descending (intraventricular) artery; RCA: right coronary artery; Cx: left circumflex artery; LVEDD: left ventricular end-diastolic diameter; PW: posterior wall; IS: interventricular septum; LA: left atrium; LVEF: left ventricular ejection fraction; WMSI: wall motion score index; MR: mitral regurgitation; NSD: no statistical difference.
Patients with ACS (STEMI or NSTEMI) had a higher frequency of ID genotype and lower frequency of DD genotype of ACE I/D than the control group patients (Table 3). Lower activity genotypes (ID and II) were more frequent in the ACS patient group and STEMI patients than in the control group overall (respectively, 83.6% vs. 78.1%, P = 0.03 and 83.3% vs. 78.1%, P = 0.03).
Comparison of ACE I/D and MMPs genotypes’ distribution among STEMI, NSTEMI and control group patients.

P<0.05 if comparing between ACS patients (STEMI and/or NSTEMI) and control group.
P<0.005 if comparing between STEMI and NSTEMI patients. ACE: angiotensin converting enzyme; ACS: acute coronary syndrome; STEMI: ST elevation myocardial infarction; NSTEMI: non-ST elevation myocardial infarction; I: insertion; D: deletion; MMP: matrix metalloproteinase; T: thymine; C: cytosine; A: adenine.
The genotypes of the MMPs are also presented in Table 3. The genotype distribution was in Hardy–Weinberg equilibrium. There were no differences in frequencies of MMP-2 (–735) C/T, MMP-2 (–1306) C/T and MMP-9 C/T genotypes among the control group, STEMI and NSTEMI patients. Higher enzymatic activity of 5A5A and 5A6A genotypes of MMP-3 were more frequent in STEMI patients than in the NSTEMI group (81.5% vs. 72.3%, P = 0.027) or in the control group (81.5% vs. 73.6%, P = 0.009).
Multivariate logistic regression analysis revealed that smoking (P = 0.001), arterial hypertension (P = 0.001), diabetes (P = 0.001), dyslipidaemia (P = 0.001), 5A5A and 5A6A genotypes of MMP-3 and ID and II genotypes of ACE are independent predictors of STEMI (Table 4).
Univariate and multivariate logistic regression analysis to predict STEMI occurrence.

STEMI: ST elevation myocardial infarction; OR: odds ratio; CI: confidence interval; AH: arterial hypertension; MMP: matrix metalloproteinase; ACE: angiotensin-converting enzyme.
Independent predictors of NSTEMI development were as follows: smoking (P = 0.001), arterial hypertension (P = 0.002) and dyslipidaemia (P = 0.005) (Table 5).
Univariate and multivariate logistic regression analysis to predict NSTEMI occurrence.

NSTEMI: non-ST elevation myocardial infarction; OR: odds ratio; CI: confidence interval; AH: arterial hypertension; MMP: matrix metalloproteinase; ACE: angiotensin-converting enzyme.
Discussion
The results of our study revealed that genetic polymorphisms of MMP-3 5A/6A and ACE I/D along with conventional IHD risk factors such as diabetes, dyslipidaemia, hypertension and smoking increase the risk of the occurrence of STEMI, while genetic factors have no influence on NSTEMI development. The state of knowledge about IHD and its relation to the inflammation process and genetic predisposition are established.14–16 However, the manifestation of IHD remains very complicated, unexpected and is not so far completely explained. Furthermore, there are not many data analysing the association of traditional IHD risk factors with the different ACS forms such as STEMI and NSTEMI. To our knowledge, genetic factors were not evaluated between the different ACS types at all.
The epidemiological studies revealed unquestionable risk factors of atherosclerosis and IHD such as smoking, diabetes mellitus, dyslipidaemia, arterial hypertension and physical inactivity.2–5 The exposure to different risk factors disrupts the endothelial function of a blood vessel, determining the beginning of the atherosclerotic process and formation of the atherosclerotic plaque. An inflammatory process regulates the process of atherosclerosis 16 and is the most important decisive factor of instability of an atherosclerotic plaque. 15 Data and results from the pathological, autopsy and angiographic studies revealed that plaque vulnerability, plaque morphology, thin fibrous cap, smaller lumen diameter account for the clinical presentation of myocardial infarction (MI).17,18
The results of our research confirm the influence of traditional risk factors on ACS occurrence. Patients with ACS more frequently were smokers and more frequently had arterial hypertension, diabetes mellitus and dyslipidaemia. Our study revealed that smoking, diabetes, dyslipidaemia and arterial hypertension increase the risk of STEMI development. However, diabetes mellitus has no associations with NSTEMI development while smoking, arterial hypertension and dyslipidaemia may be important in NSTEMI occurrence. The results of other researchers are quite contradictory. According to the data of Montalescot et al., patients with STEMI more frequently had arterial hypertension and diabetes mellitus than patients with NSTEMI while the patients with NSTEMI more frequently were smokers. 19 On the contrary, the results of Di Stefano et al. demonstrated that patients with STEMI more frequently have been smoking, and arterial hypertension has been more frequent for those who had NSTEMI. 20 Research by Ino et al. did not reveal any differences in IHD risk factors between the STEMI and NSTEMI patients at all. 21
The present study also demonstrated the differences in the basic clinical and biochemical parameters between STEMI and NSTEMI patients. Patients with STEMI had a higher heart rate and white blood cell count, higher levels of troponin I and glucose, as well as more severe heart dysfunction assessed than in patients with NSTEMI. This indicates that a higher activity of inflammation, more extensive myocardial necrosis and disbalance of glucose metabolism are more common in STEMI patients. Our results confirm the data of other studies reporting that the pathogenesis of STEMI is associated with a more active inflammation process and STEMI may lead to more extensive myocardial damage and necrosis.22–24 The research data of Di Stefano et al. demonstrated obvious differences in inflammation markers between patients with STEMI and NSTEMI. Patients with STEMI had a higher concentration of leukocytes and a higher activity of other markers of inflammation such as high sensitivity C-reactive protein, interleukin-6 and serum amyloid A. 20 The patients with NSTEMI had a lower concentration of leukocytes, and other inflammation markers were not increased at all. 20
Furthermore, in STEMI patients a more severe disturbance of glucose metabolism is present. According to our data, patients with STEMI had a higher level of glycaemia as compared to patients with NSTEMI at baseline and patients with STEMI also more frequently had diabetes in the past. Hyperglycaemia is a predictor of adverse outcomes in STEMI patients 25 as hyperglycaemia increases the amount of free fatty acids which may reduce vasodilation of small blood vessels, stimulate leukocyte adhesion and increase procoagulant action of thrombocytes, 26 and worsen myocardial perfusion and contractility. 27
Our results demonstrate that the concentration of troponin I at baseline is higher in STEMI patients than in NSTEMI patients. As we know, troponin I is the main marker of necrosis and death of myocytes during AMI and its level is an important predictor of a bad prognosis after AMI. 28 The results of other authors also show that a higher concentration of troponin I is detected in STEMI patients. An increased concentration of troponin I at the acute period of AMI not only reflects the size of the area of myocardial necrosis, but also demonstrates a higher probability of repeated ischaemic cardiac events and repeated hospitalisation because of ACS or a greater probability of death.29,30 According to the data of Di Stefano et al. the troponin I concentration correlates with the level of C-reactive protein in patients with STEMI suggesting that activation of the inflammatory system is closely related to the size of necrotic area of myocardium after MI. 20
According to the pathophysiological mechanisms of STEMI and NSTEMI that we ascribed earlier, we had a hypothesis that some genetic factors can also be important in the process of atherosclerosis and may cause the development of ACS. The results of our previous study confirmed that genetic polymorphism of the AGT gene is associated with left ventricular remodelling after AMI, suggesting that genes of the RAAS definitely play a role in the pathogenesis of ACS. 31 Experiments from genetic studies with engineered mice suggest that the expression of MMPs influences atherosclerotic burden in animal models. In in vivo studies, genetic polymorphism has an influence on the differential expression of MMPs. 32 More than a few polymorphisms of MMPs seem to be associated with atherosclerosis and the onset of AMI. The components of the RAAS may also be important in ACS development as they have an influence on the function of the endothelium disturbing the balance between vasodilation and vasoconstriction. Angiotensin II increases oxidative stress and apoptosis of the endothelial cells, affects the migration of adhesion molecules, chemotactic and anti-inflammatory cytokines causing the formation of myocardial fibrosis and production of extracellular matrix. In certain conditions, angiotensin II can cause acute rupture of the atherosclerotic plaque and a hyperthrombotic condition.33–35 Moreover, the elements of MMPs and RAAS systems interact and may influence the activity of each other.36,37
Our results demonstrate that 5A5A and 5A6A genotypes of MMP-3 are associated with STEMI development while they have no importance in NSTEMI development.This may be explained by the higher enzymatic activity of the 5A allele if compared to the 6A allele. 38 Patients with a more active genotype (5A5A or 5A6A) of MMP-3 have a higher expression of MMP-3 in the serum and tissues, have smaller atherosclerotic plaques with a small amount of connective tissue and a thin fibrous cap which is more frequently prone to rupture.17,18 The results of other research confirm that MMP-3 5A5A genotype is important in AMI development,39–41 especially for people from the Asian population. However, the value of the 5A allele in AMI occurrence is not so important in the European population.42–44 The research data from the Germans and Italians did not show any associations between the MMP-3 5A/6A polymorphism and IHD.
ACE I/D definitely takes part in the pathogenesis of some cardiovascular diseases such as arterial hypertension, cardiomyopathies and aortic pathology. The association of this gene with AMI development is disputable. Our study shows that ID and II genotypes of ACE are associated with STEMI development. However, other researchers provide quite conflicting data. Some scientists declare that particularly the D allele of ACE may be important in ACS occurrence, while others demonstrate that ACE polymorphism does not account for ACS development at all.45–47 Functionally the D allele of ACE is more active and determines a higher enzymatic expression of ACE in tissues and blood causing its deleterious effects as described earlier. It is difficult to explain the data of our research as we have found that genotypes II and ID of ACE with lower activity are more valuable in the prediction of STEMI. It may be explained by that fact that polymorphism of ACE I/D influences the development of STEMI indirectly through the other enzymatic systems (MMPs, etc.) or affecting the pharmacokinetics of the medication used.
In conclusion, smoking, diabetes, dyslipidaemia and arterial hypertension are undoubted risk factors for IHD and can cause STEMI and NSTEMI in which the metabolism of glucose is more important in STEMI pathogenesis rather than NSTEMI. Pathogenetic differences between STEMI and NSTEMI, different morphology of the atherosclerotic plaque and its rupture can be determined by genetic predisposition. The polymorphism of MMP-3 and ACE may be important in STEMI development. According to our data these genotypes are not valuable in association with NSTEMI development. However, traditional IHD factors have a superior role over the genetic factors in STEMI prediction.
Footnotes
Acknowledgements
All authors contributed equally to this work. The authors would like to thank all the participants in the research. They also thank the students and nursing staff at their hospital for their dedication to this study.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.