
Abstract
Introduction:
Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers are widely used in congestive heart failure and chronic kidney disease, but up to 40% of patients will experience aldosterone breakthrough, with aldosterone levels rising above pre-treatment levels after 6–12 months of renin-angiotensin-aldosterone system blockade. Aldosterone breakthrough has been associated with worsening congestive heart failure and chronic kidney disease, yet the pathophysiology remains unclear. Breakthrough has not been associated with elevated peripheral blood pressure, but no studies have assessed its effect on central blood pressure.
Methods:
Nineteen subjects with well-controlled peripheral blood pressure on stable doses of angiotensin-converting enzyme inhibitor/angiotensin receptor blocker had aldosterone levels checked and central blood pressure parameters measured using the SphygmoCor system. The central blood pressure parameters of subjects with or without breakthrough, defined as serum aldosterone >15 ng/dl, were compared.
Results:
Of the 19 subjects, six had breakthrough with a mean aldosterone level of 33.8 ng/dl, and 13 were without breakthrough with a mean level of 7.1 ng/dl. There was no significant difference between the two groups in any central blood pressure parameter.
Conclusions:
We found no correlation between aldosterone breakthrough and central blood pressure. The clinical impact of aldosterone breakthrough likely depends on its non-genomic, pro-fibrotic, pro-inflammatory effects rather than its regulation of extracellular volume.
Keywords
Introduction
Angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) are widely used in patients with congestive heart failure (CHF) and chronic kidney disease (CKD) due to their impact on long-term outcomes, including overall mortality,1,2 but approximately 30–50% of patients on angiotensin-converting enzyme (ACE) inhibition experience aldosterone breakthrough, 3 a phenomenon where aldosterone levels increase up to or above pre-treatment levels after 6–12 months of ACE inhibition. 4 Aldosterone breakthrough is not merely a function of inadequate ACE inhibition, 5 but the details of its underlying mechanism remain unknown. Aldosterone is primarily regulated by angiotensin II (ATII), serum potassium levels, and to a minor extent by serum adrenocorticotropic hormone (ACTH). Breakthrough has been shown in patients on ARBs, 6 indicating that ATII derived from non-ACE catalysis of angiotensin 1 (AT1) to ATII is unlikely to play a role in breakthrough. Additionally, hyperkalemia does not appear to be contributory, as potassium levels are not significantly different between patients with and without breakthrough. 7 There may be a role for the AT2 receptor, as experiments in hypertensive rats with breakthrough on ACEi subsequently showed reduced aldosterone levels after receiving an AT2 antagonist. 8
Observational studies have shown that aldosterone breakthrough is associated with increased morbidity in patients with chronic heart and kidney diseases, including increased left ventricular hypertrophy (LVH), 7 reduced exercise tolerance, 9 increased albuminuria in CKD, 10 and accelerated decline in glomerular filtration rate (GFR). 11 Two hypotheses could explain the clinical impact of aldosterone breakthrough: (a) activation of pro-fibrotic and pro-inflammatory pathways by aldosterone leading to glomerulosclerosis12,13 and LVH, 14 or (b) increased systemic pressure due to increased sodium absorption and potassium excretion. The former hypothesis implies that the deleterious effects of breakthrough are based primarily in aldosterone’s non-epithelial effects, while the latter hypothesis implies that aldosterone’s classic effects at the epithelial sodium channel are responsible for injury.
Studies of aldosterone breakthrough, to date, have not shown that breakthrough leads to elevated peripheral blood pressure (PBP).4,10,15 Central blood pressure (CBP) and PBP often do not correlate, 16 exemplified by the reduced CBP with amlodipine/perindopril compared to atenolol/thiazide in the CAFÉ subgroup of the ASCOT trial despite statistically equivalent PBP. 17 CBP parameters have also been shown to be incrementally superior to PBP in predicting carotid hypertrophy and LVH, 18 time to first cardiovascular event, 19 microalbuminuria, 20 and progression to end stage renal disease (ESRD). 21 Given that PBP may not accurately represent CBP and that CBP has independent value in predicting cardiovascular (CV) and renal outcomes, we investigated whether aldosterone breakthrough was associated with elevated CBP parameters in a cohort of patients on long-standing ACEi and ARB therapy with well-controlled PBP.
Methods
Participants
This cross-sectional study recruited volunteers from the nephrology clinics at New York Presbyterian Hospital. All subjects signed an informed consent before enrollment. The study was approved by the Institutional Review Board of Columbia University Medical Center.
Patients were eligible for inclusion if they had well-controlled PBP (<140/90 mm Hg) on stable doses of ACEi or ARB for >1 year, as well as no changes to other anti-hypertensive medications for >1 year, including diuretics. Patients were excluded if they had atrial fibrillation, a diagnosis of secondary hypertension, known structural vascular abnormalities, potassium >5.5, or a prescription for a mineralocorticoid receptor blocker. It was not deemed necessary that a patient be on maximal doses of ACEi to be included in the study, since no association has been found between the dose of ACEi and the incidence of breakthrough. 22
Non-invasive hemodynamic data acquisition
Participants were studied in the seated position, brachial systolic and diastolic blood pressures were obtained using an aneroid sphygmomanometer, and those pressures were in turn used to calibrate the SphygmoCor AtCor central arterial pressure device. 23 Applanation tonometry of the radial artery provided waveforms that were processed with pulse wave analysis according to the manufacturer’s guidelines to derive a waveform of the ascending aorta. Systolic and diastolic CBP were measured directly from this derived central waveform, central pulse pressure (CPP) calculated as the difference between systolic and diastolic CBP, augmentation pressure (AP) calculated as the difference between the second and first systolic peaks, and augmentation index (AI) as the ratio of AP to CPP, normalized for a HR of 75. Estimations of CBP using applanation tonometry have been well validated, and non-invasive measurements of CBP using this technique correspond closely to those obtained through catheterization, with a mean error of only 1.1 mm Hg in one meta-analysis. 24
Definition and measurement of aldosterone breakthrough
A variety of different cutoffs have been used to define aldosterone breakthrough including the mean value in the studied population (ranging from 6–10 ng/dl). For this study, aldosterone breakthrough was defined using the strictest available criteria for a cross-sectional study: an aldosterone level above the upper limit of normal, 22 defined as >15 ng/dl at our institution. Sample acquisition for aldosterone levels was conducted in a seated, upright posture along with routine laboratory testing ordered at each participant’s outpatient nephrology clinic visit. No restrictions were imposed on participants regarding diet or fluid intake prior to sample acquisition.
Statistical analysis
Data analysis was conducted using Student’s t-test to evaluate for difference between those patients with and without aldosterone breakthrough, with significance set at p<0.05. Analyses were also performed separately for quartiles of aldosterone levels.
Results
Patient characteristics
The mean age of participants in the study was 53±18 years, with roughly equal representation of ACEi and ARB in their medication lists (Table 1). Diuretics were over-represented in the breakthrough group, but had been stably dosed for >1 year as per our inclusion criteria so that they would be without dynamic effect on the renin-angiotensin-aldosterone system (RAAS) axis. CBP and AP are known to increase with age, 16 but no significant difference was found between the mean age of individuals with and without breakthrough. Women comprised only 26% of individuals, and the majority of the participants were either Hispanic or Caucasian by ethnicity. No significant difference in body mass index (BMI) could be seen between the two groups. Of the 19 subjects evaluated, six were found to have aldosterone levels >15 ng/dl, classifying them as having aldosterone breakthrough as per our pre-defined criteria. Between those with and without aldosterone breakthrough, there was no difference in serum potassium levels but a significant difference was found in terms of the severity of CKD. In addition to an increased prevalence of macroalbuminuria, individuals with aldosterone breakthrough had a mean serum creatinine (Cr) 3.2±1.9 mg/dl, significantly higher than those without breakthrough, who had Cr of 1.4±0.5 mg/dl (p<0.006). A broad range of etiologies leading to CKD were represented in our study group (Supplementary Material, Table 1).
Patient characteristics.

ACEi: angiotensin-converting enzyme inhibitor; Am: American; ARB: angiotensin receptor blocker; BMI: body mass index.
Central hemodynamics in aldosterone breakthrough
None of the central hemodynamic parameters we measured had any significant difference according to aldosterone breakthrough status (Table 2). Mean CBP, CPP, AP, and AI were all without statistically significant differences between the two groups. Categorizing the subjects in terms of quartiles for serum aldosterone levels 0–6 ng/dl (n=5), 6–9 ng/dl (n=5), 9–20 ng/dl (n=5), and >20 ng/dl (n=4), created four groups each with statistically significant differences in mean serum aldosterone level (Table 3). However, this grouping by quartiles did not reveal any statistically significant differences between the first and fourth quartiles nor any statistically significant trends in the overall dataset.
Central hemodynamics in aldosterone breakthrough.

AI: augmentation index; AP: augmentation pressure; CBP: central blood pressure; CPP: central pulse pressure.
Aldosterone quartiles and central hemodynamics.
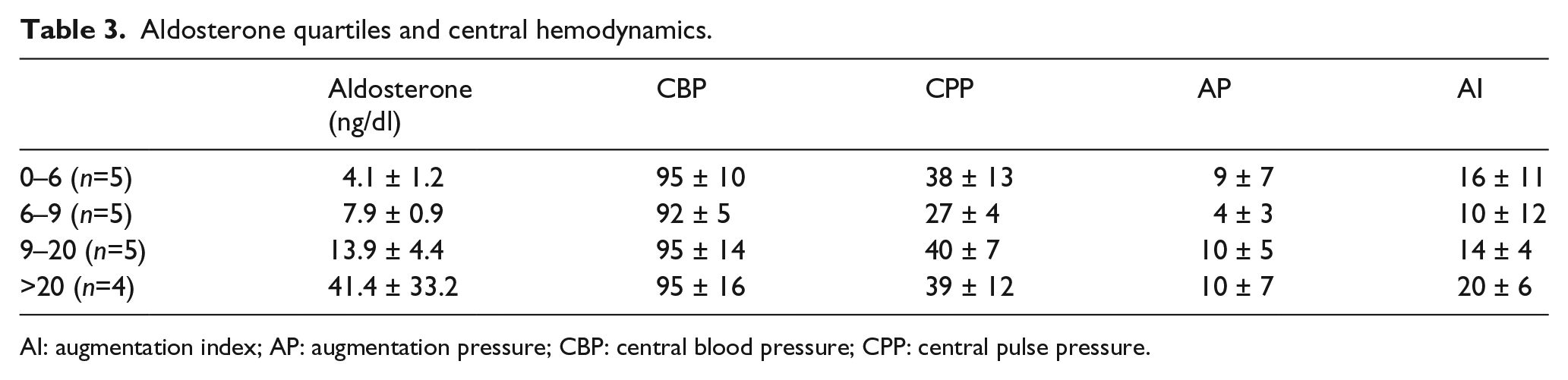
AI: augmentation index; AP: augmentation pressure; CBP: central blood pressure; CPP: central pulse pressure.
Discussion
In this cross-sectional study of 19 patients with CKD on long-standing ACEi or ARB therapy with well-controlled PBP, we found no evidence that aldosterone breakthrough, manifest in one-third of the study population, was associated with elevations in any CBP parameters. The absence of correlation between aldosterone breakthrough and central hemodynamics in our cross-sectional study suggests that aldosterone’s non-genomic effects, especially its upregulation of pro-inflammatory and pro-fibrotic pathways, are likely responsible for the pathophysiology associated with aldosterone breakthrough.
Aldosterone’s effects on fibrosis and inflammation are well documented: transforming growth factor-beta (TGF-b)-β and Type I collagen expression are increased in rats with chronically elevated aldosterone levels, 25 aldosterone induces superoxide production, 26 as well as apoptosis through free radical production, 27 while spironolactone reduces glomerulosclerosis in rat models. 12 These mechanisms are believed to underlie aldosterone’s deleterious effects on left ventricular function and GFR. The absence of any hemodynamic alteration associated with aldosterone breakthrough, either in PBP as documented in prior studies,4,10,15 or in CBP as presented here, suggests that the pathophysiology of aldosterone breakthrough is driven primarily by its pro-inflammatory and pro-fibrotic effects.
On first pass, it would seem surprising that there is no effect on central hemodynamics from aldosterone breakthrough, especially in light of the differential effect of RAAS inhibition on central hemodynamics: ACEi/ARB have been shown to reduce CBP to a greater degree than PBP17,28 and, in general, vasodilators inclusive of calcium channel blockers and alpha-blockers are more potent at reducing central pressures when compared to non-vasodilators. 29 But it should be borne in mind that aldosterone levels in aldosterone breakthrough are not a function of ATII activity and do not correlate with upregulated RAAS pathway activation. In a study of 34 patients with CHF on maximal recommended doses of ACEi, aldosterone breakthrough occurred despite maximal ACE inhibition as confirmed by measurement of ATII/ATI ratios, 5 and the proportion of individuals experiencing aldosterone breakthrough remained the same whether on either ACEi or ARB alone or on combined ACEi/ARB therapy. 30 Since elevated aldosterone levels in aldosterone breakthrough are independent of ATII and its effect on vasoconstriction, it could be reasonably expected that central hemodynamics remain unchanged following aldosterone breakthrough as seen in this study.
Our study is notable for being the first to examine the impact of aldosterone breakthrough on CBP. In addition, this study and its CKD subject population provide interesting new data for the field of breakthrough. We report here a 32% prevalence of aldosterone breakthrough in patients with CKD on ACEi or ARB therapy, using a very conservative definition of breakthrough, but also found that those with breakthrough had significantly worse kidney function compared to those without breakthrough. Reduced estimated glomerular filtration rate (eGFR) has previously been shown in a multivariate regression analysis to be predictive of the likelihood of aldosterone breakthrough in a longitudinal study of patients with diabetic nephropathy, mean eGFR=45, and macroalbuminuria. 31 Our data likewise may suggest that reduced glomerular filtration or impaired renal handling of sodium, potassium, or the hormones of the RAAS in CKD could predispose individuals to aldosterone breakthrough. Although elevated Cr has in turn been correlated with increased CPP, 21 our data show no such evidence of statistically significant differences in CPP between the groups.
Limitations to our study include its inability to assess causality given its cross-sectional design. The study’s small size additionally may leave it underpowered to assess for statistically significant differences in hemodynamic parameters between individuals with and without aldosterone breakthrough. Finally, given the unequal gender and race distribution of the participants in our cohort, further study is necessary before these data can be applied to the population as a whole.
In conclusion, we show here that aldosterone breakthrough, in a cohort of CKD patients with well-controlled PBP, occurs in approximately one-third of patients on long-standing ACEi or ARB therapy. We detected significantly worse renal function in those who demonstrated breakthrough compared to those who did not. However, we demonstrated no differences in CBP parameters between these groups, suggesting that aldosterone breakthrough does not appear to mediate an effect via the hormone’s classical, epithelial actions.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This project was funded with departmental resources from the Division of Nephrology at Columbia University Medical Center. Andrew Beenken was additionally funded by NIH training grant, 5T32DK108741.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.