
Abstract
Objective:
The purpose of the study was to characterize changes in apoptosis and the renin–angiotensin system (RAS) in fetal growth restriction (FGR).
Materials and method:
Fetuses were collected from patients who visited our hospital to either terminate or abort their pregnancy. Kidneys of fetuses which suffered with FGR, (n=11) at gestational age of 33.4±0.5 weeks and those from non-FGR (n=12) at gestational age of 34.3±0.9 weeks were collected. TUNEL, Bax and Bcl-2 staining were examined. The number of nephrons was also counted. Both protein and mRNA levels of renin and angiotensinogen were analyzed. Ultrasound was applied to measure fetus parameters including biparietal diameter, head circumference, circumference of abdomen, and femur length.
Results:
The number of nephrons was positively correlated with fetal weight at termination. Kidneys in the FGR group presented more apoptotic cells than those in the non-FGR group. Renin and angiotensinogen both decreased in the FGR group. Ultrasound revealed that biparietal diameter, abdomen circumference, femur length, and birth weight were all reduced in the FGR group compared with the non-FGR group. Kidney size was also restricted in the FGR group as indicated by ultrasound.
Conclusion:
Renal apoptosis might contribute to the reduction of nephrons, and ultrasound plays a vital role in early diagnosis of developmental origins of health and disease (DOHAD).
Introduction
The hypothesis proposed by Barker is that intrauterine environmental exposures and events affect the fetus’ development, and thereby increase the risk of specific diseases in adult life.1,2 Many studies have shown that intrauterine malnutrition, infection, drugs, toxins and stress are all determinants for the intrauterine environment.3–10 Although, Barker mainly relates the intrauterine environment to coronary heart disease,1,11 a range of chronic diseases dubbed developmental origins of health and disease (DOHAD) have also been linked with the intrauterine environment. 2 Among all of the other factors, low birth weight (LBW), which is defined as the infant weighed under 2,500 g, is the most prominent factor for DOHAD.LBW is classified as one type of intrauterine growth restriction (IUGR) where a fetus fails to reach its genetic growth potential as a result of a compromised intrauterine environment. IUGR can be caused by maternal factors such as malnutrition, drug intake, hypertension, Type I or gestational diabetes, and persistent hypoxia due to cardiovascular disease or high altitude as well as placental insufficiency.14–16 The central dogma of DOHAD theory is known as “programming”, and this refers to the fact that stimuli such as malnutrition, when applied during early development, generate permanent effects that persist throughout one’s lifespan with changes during the process of altering the structure and function of various organs to preserve neurodevelopment and promoting survival. 17
The role of an adverse in-utero environment in the programming can also be applied to chronic kidney disease (CKD) in the adult. 18 LBW has been used as a clinical surrogate for poor intrauterine environment and is associated with an increased risk of adult-onset diseases including renal function disorder.19,20 Impaired nephrogenesis resulting in reduced nephron numbers is the postulated mechanism linking LBW with subsequent hypertension and risk of CKD. 21 Furthermore, the number of glomeruli has a positive correlation to kidney weight. 22 Up to adult life, lower glomerular filtration rate, azotemia, proteinuria, and glomerulosclerosis are all clinical manifestations.23–25 It is hypothesized that a reduced number of nephrons causes glomerular hyperfiltration and compensatory hypertrophy, possibly at the expense of increased intraglomerular pressures and subsequent glomerulosclerosis which leads to CKD through a further yet unknown mechanism.26,27 Apoptosis is known to play an important role in determining the number and pattern of nephrons, 28 so we decided to examine the role of apoptosis in Fetal Growth Restriction (FGR) to see whether it is the culprit with the consequence of smaller kidney size.
Fetal malnutrition, maternal malnutrition, as well as exposure to maternal glucocorticoid and renin-angiotensin all contribute to the reduction of nephrons during fetal development.29,30 LBW infants are defined as infants who weigh 2500 g at birth. The LBW infant population can be divided into preterm (delivered before 37 weeks from the first day of the last menstrual period), appropriate for gestational age (AGA), or small for gestational age (SGA). The cause of LBW in developed countries is normally preterm delivery while in developing countries it is IUGR. 31 Maternal under-nutrition and/or placental insufficiency are two main contributors to IUGR. 32 Placental insufficiency results from poor placentation which is usually associated with preeclampsia and maternal cardiovascular risk factors and is likely to have a greater impact on LBW than maternal malnutrition. 33
The renin–angiotensin system (RAS) plays an important role in physiological control of cardiovascular systems and body fluid homeostasis in adults. Now, a variety of evidence has demonstrated that the prenatal RAS is important. Its alteration during development in utero can cause cardiovascular disease and kidney defect in adult life. 34 In animal models, maternal calorie or protein restriction and uteroplacental insufficiency can lead to alterations in kidney development with lower numbers of nephrons. 35
In this study, we confirm the correlation between FGR with metabolism syndrome and other diseases such as CKD. We propose that renal apoptosis might contribute to the reduction of nephrons. Finally, we advocate the valuable role of ultrasound in early diagnosis.
Material and methods
Ethics statement
All experimental protocols were approved by the institutional review board of Tianjin Central Hospital of Gyne-cology Obstetrics (Tianjin, China). All participants were informed of all procedural details, including study duration, study methods, results publication, and disposal of the research samples. Signed informed consent forms were submitted. No financial incentives were offered for sample collection. We guaranteed that all research samples were used for basic scientific research and not for medical purposes.
Pathological sample collection
Pregnant women who visited the Department of Obstetrics, Tianjin Central Hospital of Gynecology Obstetrics between November 2009–December 2010 were selected and divided into the FGR (n=48) group and non-FGR group (n=72). In the FGR group, 11 women decided to terminate their pregnancy before full term while the number in the non-FGR group was 12. Among those 11 patients in the FGR group who underwent early termination of their pregnancy, eight were complicated with pre-eclampsia while the other three were not. As to the 11 aborted fetuses in the FGR group, three were stillbirths due to placental abruption; two were deformities (one cheilopalatognathus and one diaphragmatic hernia); another six were terminated as required by their patients due to FGR. The fetuses in the non-FGR group were terminated for various reasons including cheilopalatognathus (n=4), abnormal brain development (n=1), diaphragmatic hernia (n=2), dyschondroplasia (n=1), esophageal atresia (n=2), and social factors (n=2). The abnormalities of fetuses are shown in Table 1. The ages of the pregnant women were 21–32 (25.3±5.2) and 23–31 (26.3±4.2) respectively in the FGR group and the non-FGR group, with no significant difference (p>0.05). And gestational weeks were 28+6 to 38+1 (33.4±0.5) and 29+4 to 37+6 (34.3±0.9) respectively in the FGR and the non-FGR group, also with no significant difference (p>0.05). There was no abnormality in all kidneys of aborted fetuses. The left kidneys were chosen to be used in further analysis in all cases.
Fetus anomaly in the two groups.
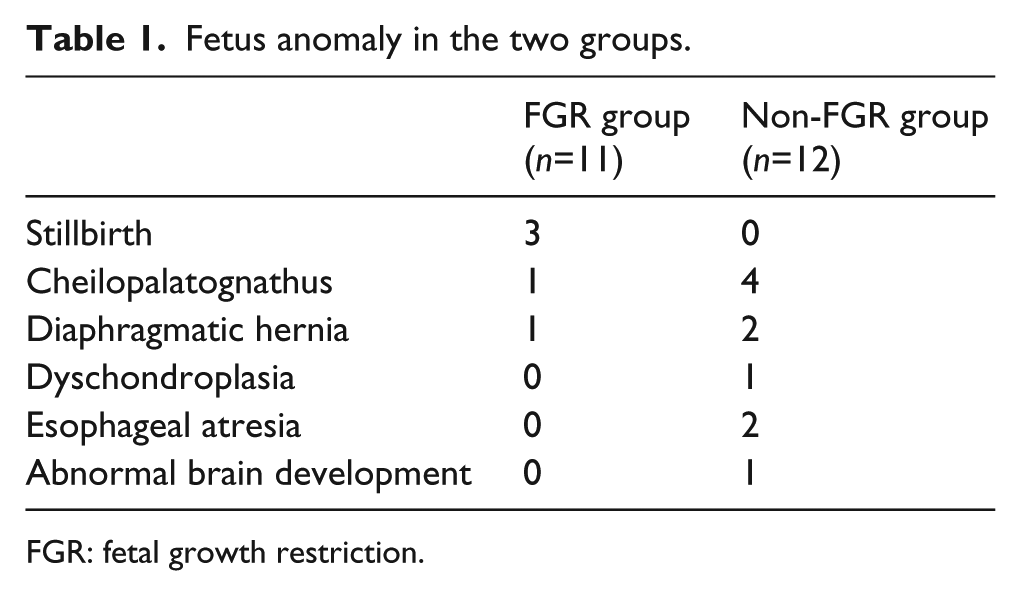
FGR: fetal growth restriction.
Immunohistochemistry of pathological samples
Part of kidney samples included both medulla and cortex, and were fixed in 10% formalin and embedded in paraffin, then sectioned onto slides with a thickness of 4 µm. After rehydration, slices were blocked in 5% Bovine serum albumin (BSA) and incubated with primary antibody (B-cell lymphoma 2 (Bcl2) and Bcl-2-associated X protein (Bax)) at 4°C overnight then with secondary antibody at room temperature for 20 min. 3,3’-Diaminobenzidine (DAB) was used for chromogenic reaction using commercial available kits (Beijing Golden Bridge Biotechnology Ltd). Antigen was retrieved by 0.1% trypin and endogenous peroxidase was blocked by 3% H2O2. Terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) staining was performed using a commercially available kit (Boehringer Mannheim) according to the manufacturer’s instructions.
Quantitative polymerase chain reaction (PCR) of pathological samples
Total RNA was extracted by Trizol (Invitrogen) and quantified using optical density (OD260) then cDNA were synthesized by reverse transcriptase Moloney Murine Leukemia Virus Reverse Transcriptase (M-MLV) (Promega).
Primers of target genes (renin and angiotensinogen) as well as internal reference gene (Glyceraldehyde 3-phosphate dehydrogenase (GAPDH)) were as follows:
Renin
Sense: 5’-CCAACTACATGGACACCCAG-3’
Antisense: 5’-ATCCGAAGCATCGAAGAG-3’
Angiotensinogen
Sense: 5’-AACTATCTCCCCGGACCA-3’
Antisense: 5’-CCTGATGCGGTCATTGCT-3’
GAPDH
Sense: 5’-CCTTCCgTgTTCCTACCC-3’
Antisense: 5’-AAgTCgCAggAgACAACC-3’
Finally, real-time polymerase chain reaction (PCR) was performed using Synergy Brands, Inc (SYBR) Green PCR kit from Takara Da Lian. And RNA was analyzed using the 2−ΔΔct method, which was standardized to GAPDH.
Western blot of pathological samples
The kidney samples were cut into small pieces and homo-genized, then quantified using BCA Protein Assay Kit (Pierce). Each sample (100 µg) was run on sodium dodecyl sulfate Polyacrylamide gel electrophoresis (SDS-PAGE) and transferred into nitrocellulose and blocked by 5% skimmed milk. Primary antibodies such as renin, angiotensinogen and GAPDH were incubated for 2 h at room tem-perature while secondary goat anti rabbit Immunoglobulin G (IgG) were incubated for 1 h at room temperature. enhanced chemiluminescence (ECL) (Millipore) was used to develop luminescence.
Quantitation of nephrons in pathological samples
Nephron numbers can be estimated by stereology based analysis.36–38 In short, each kidney was fixed in 10% formalin and cut into small pieces, then incubated in 1% NH4Cl for 2 h. Kidney pieces were then incubated in 1 mol/l HCl for 30 min and homogenized in Phosphate Buffered Saline (PBS). An amount of 1/500 of total homogenate was used to count the number of nephrons in three independent experiments. Finally, the number of nephrons in each kidney was calculated through the proportion of kidney that was homogenized.
Statistics
All data were analyzed by SPSS 16.0 and results were annotated as
Results
All patients in the FGR group and the non-FGR group underwent an ultrasound scan before delivery. There is no significant difference in the gestation weeks when they were scanned (Table 2). Furthermore, pregnant women in the two groups were no different in age, previous pregnancy, and gestational hypertension background, although body mass index (BMI) in the non-FGR group was higher than that in the FGR group (Table 3).
Comparison of fetal characteristics between the two groups using ultrasound (US).

FGR: fetal growth restriction.
Data are shown as x¯±s, ap<0.01.
Comparison of basic characteristics of patients in fetal growth restriction (FGR) and non-FGR groups.
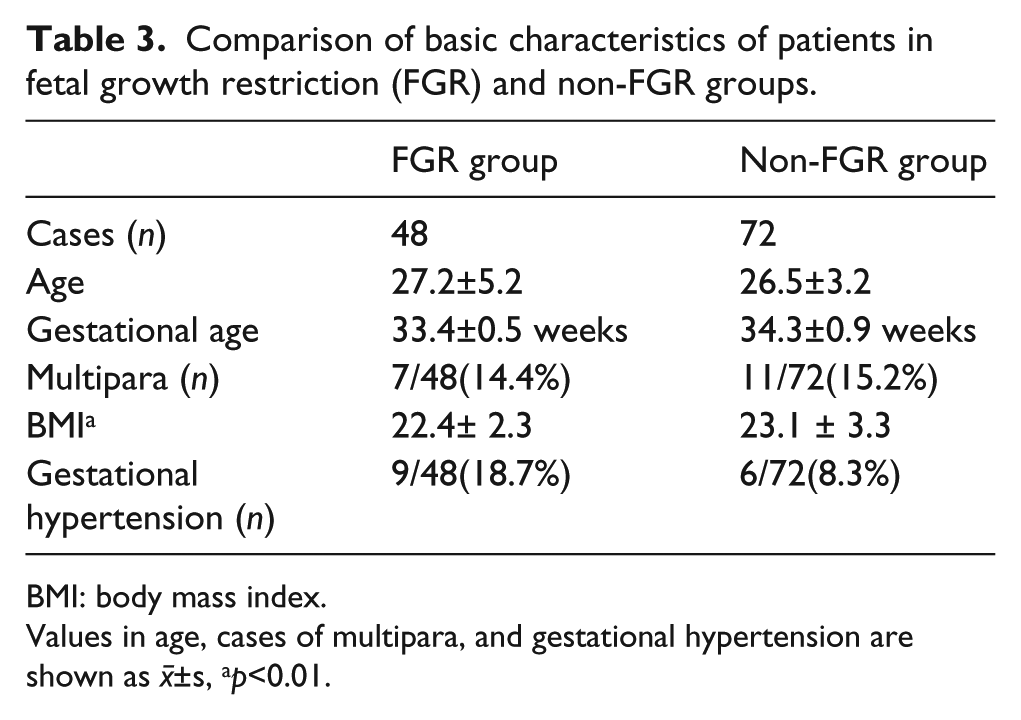
BMI: body mass index.
Values in age, cases of multipara, and gestational hypertension are shown as x¯±s, ap<0.01.
Ultrasound revealed that biparietal diameter, abdominal circumference, femur length, and birth weight all reduced in the FGR group compared with the non-FGR group (Table 2). This finding again confirmed FGR in the FGR group.
As part of the fetal body, kidney growth was also restricted in FGR group. Shown in ultrasound, both kidneys were smaller and their kidney lengths were shorter than their counterpart in non-FGR group (Table 4).
Comparison of size of fetal kidneys in two groups through ultrasound.

FGR: fetal growth restriction.
Data are shown as x¯±s, ap<0.01.
There was no significant difference in the gestation weeks at termination between patients in the FGR group and the non-FGR group. The number of nephrons was positively related to the corresponding fetal weight at termination. On average, the number of nephrons increased by 170,042 per kg of fetal weight (data not shown). Therefore, reduced numbers of nephrons mainly account for the smaller kidney size.
To explore the mechanism behind the FGR phenotype, apoptotic markers were examined in the two groups. Under a high power field of 200× magnification, 10.5 apoptotic cells were found in each 1000 kidney cells in the FGR group, much higher than the 5.7 cells found in the non-FGR group which was also confirmed by expression levels (Figure 1(a) and Table 5). Furthermore, the anti-apoptotic protein Bcl2 was down-regulated while the pro-apoptotic protein Bax was up-regulated in fetal renal samples from the FGR group compared to those in the non-FGR group, both in transcription level shown by q-PCR (Table 6) and in translation level shown by Western blot (Table 1). These were also confirmed in expression levels in the kidneys (Figure 1(b)). So, apoptosis partially contributes to the reduced kidney size in the fetus.

Comparison of apoptotic protein expression levels of Bcl2 and Bax between two groups: (a) comparison of TUNEL expression levels between two groups; (b) comparison of Bax and Bcl2 between two groups. FGR: fetal growth restriction.
Comparison of TUNEL staining between two groups.

FGR: fetal growth restriction; HPF: high powered field.
Data are shown as x¯±s, ap<0.01,
Comparison of apoptotic protein RNA levels in fetal kidneys of the two groups.
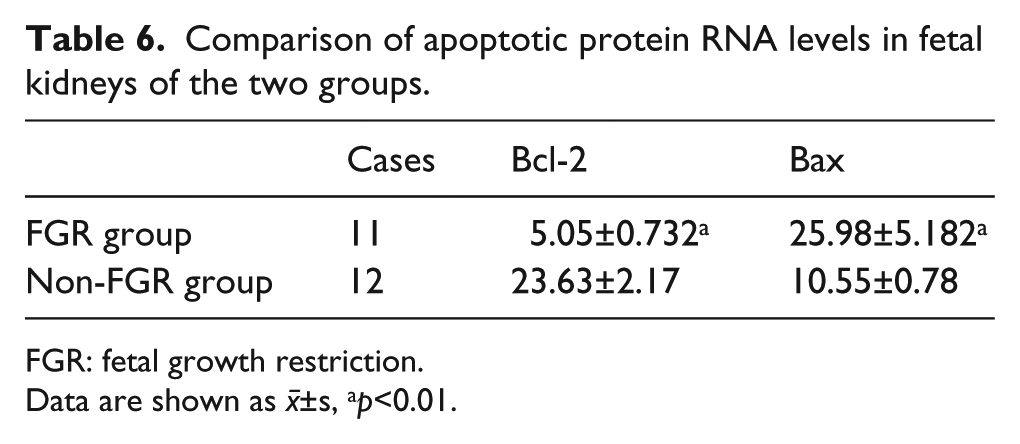
FGR: fetal growth restriction.
Data are shown as x¯±s, ap<0.01.
Finally, the RAS plays a role in fetal kidney development too. Both renin and the angiotensin precursor, angiotensinogen, were reduced in kidney samples in fetuses from the FGR group compared to those from the non-FGR group, both in transcription level shown by q-PCR (Table 7) and in translation level shown by Western blot (Table 8).
Comparison of renin and angiotensinogen RNA levels in fetal kidneys of the two groups.

FGR: fetal growth restriction.
Data are shown as x¯±s, ap<0.001.
Comparison of protein expression levels of renin and angiotensinogen between the two groups.

FGR: fetal growth restriction.
Data are shown as x¯±s, ap<0.001.
Discussion
Besides the conventional two factors, genetic and environmental, which contribute to the etiology of diseases, more and more evidence points to the far-reaching effects of prenatal (intrauterine) programming on subsequent organ function and adult diseases. 39 IUGR was recently known to be associated with increased rates of cardiovascular disease (CVD) and non-insulin dependent diabetes in adult life and the induced animal model demonstrates a variety of diseases in target organs. 40 This was further certified in clinical research that showed IUGR leads to persistent aortic wall thickening and significantly higher microalbuminuria during infancy which might cause adult renal and cardiovascular disease.41,42 Taking these findings into consideration, it is no surprise to see that eight women in the FGR group terminated their pregnancy due to preeclampsia.
Multiple animal models have demonstrated the association of LBW with adult hypertension, which is partially mediated by an associated congenital nephron deficit occurring with IUGR.43–45 A recent autopsy study on Caucasians revealed that those with a history of essential hypertension had significantly fewer glomeruli per kidney, and greater glomerular volume than matched normotensive controls. This report established a connection of adult hypertension with nephrogenesis in humans. 46 Then Hinchliffe et al. linked the reduction of nephron numbers with IUGR through comparing nephron numbers in stillbirths and infants dying at one year of age with and without IUGR. 47 LBW and reduced nephron numbers are strongly associated with future kidney diseases including end-stage renal disease (ESRD). Reduced nephron numbers lead to compensatory adaption of increasing single nephron glomerular filtration rate (SNGFR) and hyperfiltration. Hyperfiltration may be clinically detected as microalbuminuria. This at least contributes partially to adult renal diseases.48–52 In this study, we confirmed the causation relationship of LBW with nephrogenesis using aborted fetuses which better represent physiological status. Furthermore, we established a direct linear relationship between the number of nephrons with “birth” weight, with an average of decreasing 170,042 nephrons per kg of reduced fetal weight. Additionally, the kidney volume shown in ultrasound is positively related with the number of the nephrons and the corresponding “birth” weight. These findings provide a potential theoretical base for using ultrasound to predict fetal origin of kidney diseases in adulthood.
Telomere integrity, mitochondria dysfunction, and apoptosis all play roles in the process of DOHAD. 46 Nephron development in humans begins in the ninth week of gestation and ceases during the 36th week. During the last trimester, there is a rapid rise in nephron number and glomerulogenesis stops 40 days after birth.53–55 As in other organ systems, the cellular mass of nephrons during development depends on a careful balance between cell proliferation and apoptosis. In animal models, IUGR was associated with evidence of higher levels of renal cellular apoptosis. 56 IUGR could lead to increased expression of pro-apoptotic factors such as p53 and Bax. Heightened p53 activity induced the downregulation of anti-apoptotic factors, such as Bcl-2. As a consequence, an increase in the ratio between pro-apoptotic and anti-apoptotic factors promotes renal cellular apoptosis, possibly leading to low nephron numbers in the offspring. 57 This change in apoptosis balance was certified in this study in human samples, both in transcription levels and translation levels. Apoptosis was shown by other researches to play a role in DOHAD. Using a high-fat diet during pregnancy to correct intrauterine malnutrition leads to increased pancreatic gene expression of Igf2. Igf2 is a mitogen and inhibitor of apoptosis that can prevent pancreatic lesions in adult life. 58 Another study showed that antioxidant quercetin increased interdigital webbing of mice through inhibiting apoptosis. 59
In the nephron-deficient rat, urinary sodium excretion was lower, and tissue sodium content was higher. 60 Then renin and angiotensin activity was reduced, possibly consistent with a degree of volume expansion secondary to sodium retention.61,62 The RAS and the paired homeobox 2 gene (Pax-2) are critical factors in nephrogenesis. Angiotensin II was shown to increase Pax-2 gene expression, a process that might be important in renal development and repair.63–65 This impaired nephrogenesis further. The down-regulation of RAS was also observed in our study too, using human samples, both in transcription level and translation level.
Consistent with our results, Alexander revealed that inappropriate suppression or activation of the RAS and/or activation of the sympathetic nervous system leading to marked increases in oxidative stress and endothelin production are implicated in the etiology of hypertension that has its origins in fetal life.66 Insulin resistance and hypertension can both be traced to blunted kidney development and RAS activation in growth-restricted offspring.67,68
Conclusion
In this study, we confirmed the down-regulation of RAS and activation of apoptosis cascade in human samples under IUGR. We also used aborted fetus to verify the connection between LBW with lower nephron numbers. In particular, we established a connection between kidney volumes on ultrasound with nephron numbers, therefore providing a new diagnostic approach for fetal origin of kidney disease apart from tissue-specific DNA methylation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the key research program of the Tian Jin Healthcare industry (12KG128).