
Abstract
Background:
The relationship between CYP17A1 genetic polymorphisms and coronary artery disease (CAD) remains unclear. The aim of the present study was to assess the association between CYP17A1 gene polymorphism and CAD in a Chinese Uygur population.
Methods:
A total of 493 people including 266 patients and 227 controls were selected for the present study. All CAD patients and controls were genotyped for the same five single nucleotide polymorphisms (SNPs) (rs4919686, rs1004467, rs4919687, rs10786712, and rs2486758) by a real-time PCR method.
Results:
The rs4919686, rs1004467, and rs4919687 polymorphisms were found to be associated with CAD in genotypes, dominant model, recessive model, and allele frequency (rs4919686: all p<0.05, rs1004467: all p≤0.001, rs4919687: all p<0.001); the significant difference was retained (all p<0.05) after adjustment for the major confounding factors. The overall distribution of haplotypes established by SNP1–SNP4 (in total subjects and men) and SNP1–SNP4–SNP5 (in total subjects) were significantly different between the CAD patients and the control subjects (p=0.006, men: p=0.026, and p=0.030, respectively).
Conclusion:
Polymorphisms rs4919686, rs4919687 and rs1004467 were found to be associated with CAD in this Uygur population.
Introduction
Coronary artery disease (CAD) and its most severe complications, such as myocardial infarction, are leading causes of mortality worldwide.1,2 It is a complex multifactorial disorder thought to result from several susceptibility genes and multiple environmental determinants.3,4 Recently, the genetic basis of CAD has gained considerable interest; heritable factors were found to account for 40–60% of occurrence and development of CAD. 5 With the development of genome-wide association studies concerning CAD, a growing number of susceptibility genes related to CAD have been revealed, and some large-scale association analyses have identified many common, uncommon and functional variants for CAD.6,7
The cytochrome P450 proteins catalyze many reactions involved in drug metabolism and synthesis of cholesterol, steroids and other lipids. They are responsible for not only the metabolism of xenobiotics but also a host of endogenous substances whose metabolites have critical roles in the maintenance of cardiovascular health.8,9 Mounting evidence has demonstrated that CYP enzymes are involved in the pathogenesis of CAD. For example, the CYP2C19 genetic variants involved in the conversion of clopidogrel to its active metabolite are associated with an increased rate of recurrent cardiovascular events, including stent thrombosis (ST);10,11 recent reports suggest that CYP8A1, predominantly in vascular endothelial and smooth muscle cells, is a member of the CYP family and acts mainly as an enzyme that converts prostaglandin H2 (PGH2) into prostacyclin (PGI2); and some studies suggest that gene polymorphisms are associated with cardiovascular risk. 12 In addition, CYP1A1, CYP1A2 (which metabolize tobacco polycyclic aromatic hydrocarbons and aromatic amines during smoking),13,14 CYP2C8, CYP2J2 (EET synthesis),15,16 CYP3A4 (the main metabolic enzyme of fentanyl), 17 and CYP17 and CYP19 (synthesis of hormones) 18 have been demonstrated to have a relationship with CAD.
In humans, the CYP17A1 gene is located on chromosome 10q24.3, and is mainly expressed in the adrenal glands and gonads. This gene encodes a member of the cytochrome P450 superfamily of enzymes. The CYP17A1 gene produces P450c17 proteins; it has both 17alpha-hydroxylase and 17,20-lyase activities and is a key enzyme in the steroidogenic pathway that produces progestins, mineralocorticoids, glucocorticoids, androgens, and estrogens. CYP17A1 gene mutations affect the synthesis of steroids, which are the precursors of sex hormones. Some evidence has indicated that the levels of sex hormones can affect the development of cardiovascular and cerebrovascular diseases. 19 Sex hormones such as estrogens protect against oxidative stress and are known to be vasoprotective.20-22
In recent years, several studies have investigated the association between CYP17A1 heritable variation and CAD.7,23 However, the relationship between CYP 17A1 genetic polymorphisms and CAD in the Uygur population remains unclear. In the present study, we aimed to assess the association between the polymorphism of CYP17A1 and CAD in the Uygur population in Xinjiang, China.
Methods
Ethical approval of the study protocol
This study was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (Xinjiang, China). Written informed consent was obtained from each participant, and explicitly provided permission for DNA analyses as well as collection of relevant clinical data. This study was conducted according to the standards of the Declaration of Helsinki.
Study population
The subjects were from a Uygur population who lived in the Xinjiang Uygur Autonomous Region of China, and comprise 493 people (326 men, 167 women), with 266 patients and 227 ethnically and geographically matched controls. All subjects attended as inpatients in the First Affiliated Hospital of Xinjiang Medical University from 2007 to 2013. CAD group patients were defined as having the presence of at least one significant coronary artery stenosis of >50% luminal diameter on coronary angiography. Patients with congenital heart disease, valvular disease, multiple organ failure syndrome, malignancy or chronic inflammatory disease were excluded from this study. Each control subject also underwent a coronary angiogram and did not show coronary artery stenosis, and the electrocardiogram did not indicate CAD.
Biochemical analyses
Before cardiac catheterization, a 5 ml sample of fasting venous blood drawn by venipuncture in the Cardiac Catheterization Laboratory was taken from all participants. The blood samples were collected into tubes containing ethylene diamine tetraacetic acid (EDTA), and to separate the plasma content were centrifuged at 4000 ×g for 5 min. Genomic DNA was extracted using a standard phenol-chloroform method. Serum concentrations of glucose (Glu), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), blood urea nitrogen (BUN), creatinine (Cr) and uric acid (UA) were measured using standard methods in the Central Laboratory of First Affiliated Hospital of Xinjiang Medical University as described previously.24-26
Genotyping of the CYP17A1 gene
Using Haploview 4.2 software and International HapMap Project website phase II database (http://www.hapmap.org), we obtained five tag single nucleotide polymorphisms (SNPs) (SNP1: rs4919686, SNP2: rs1004467, SNP3: rs4919687, SNP4: rs10786712, SNP5: rs2486758) by using minor allele frequency (MAF) ≥0.05 and linkage disequilibrium (LD) patterns with r2≥ 0.8 as a cut off. Genotyping was confirmed by the TaqMan SNP Genotyping Assay (Applied Biosystems, Foster City, CA) according to the previous report.
Statistical analysis
Differences in categorical variables (e.g. age, body mass index (BMI), TC, TG, HDL-C, LDL-C, Glu, BUN, Cr, UA) were analyzed using means ± standard deviation (SD). The difference between the CAD and control groups was analyzed using an independent-sample t-test. Differences in frequencies of smoking, drinking, hypertension, diabetes mellitus, and CYP17A1 genotypes were analyzed using χ2 test or Fisher’s exact test where appropriate. Hardy–Weinberg equilibrium was assessed by χ2 analysis. Logistic regression analyses with effect ratios (odds ratio (OR) and 95% confidence intervals (CI)) were used to assess the contribution of major risk factors. Data analysis was carried out using the computer software Statistical Package for Social Sciences SPSS 17.0 for Windows (SPSS Institute, Chicago, USA). Statistical significance was established at a p-value <0.05. In addition, based on the genotype data of the genetic variations, we performed LD analysis and haplotype-based case-control analysis, using the expectation maximization algorithm and the software SHEsis (http://analysis.bio-x.cn/SHEsisMain.htm). The pairwise LD analysis was performed using five SNP pairs. We used|D’|values of >0.25 to assign SNP locations to one haplotype block. Single nucleotide polymorphisms with an r2 value of <0.5 were selected as tagged. In the haplotype-based case-control analysis, haplotypes with a frequency of <0.03 were excluded. The frequency distribution of the haplotypes was calculated by performing a permutation test using the bootstrap method.
Results
Characteristics of the study participants
As shown in Table 1, there was no significant difference in age between patients with CAD and control subjects, which indicated that the study was an age-matched case-control study. For total and female subjects, the systolic blood pressure (SBP), serum concentration of glucose, TG, UA, Cr, and the incidence of diabetes were significantly higher in subjects with CAD than in the controls, and the serum concentration of HDL-C was significantly lower for patients with CAD than for control participants. For all, the diastolic blood pressure (DBP) was significantly higher in CAD subjects than in the controls. For women, the serum concentration of BUN was significantly higher for the CAD patients than in the control subjects. There was no significant difference in the following variables between the CAD patients and the control participants in total and female subjects: the incidence of hypertension, smoking, drinking, BMI, plasma concentration of TC, and LDL-C. For men, the incidence of smoking, SBP, and glucose were significantly higher for the CAD patients as compared with the control subjects, and HDL-C was significantly higher for control participants than for patients with CAD; for other variables there was no significant difference in men.
Demographic and clinical characteristics of study participants.

Continuous variables are expressed as mean ± SD. Categorical variables are expressed as percentages.
BMI: body mass index; BUN: blood urea nitrogen; Cr: creatinine; DBP: diastolic blood pressure; DM: diabetes mellitus; Glu: glucose; TG: triglyceride; TC: total cholesterol; HDL: high-density lipoprotein; LDL: low-density lipoprotein; EH: essential hypertension; SBP: systolic blood pressure; UA: uric acid.
The p-value of the continuous variables was calculated by independent t-test. The p-value of the categorical variables was calculated by Fisher’s exact test.
Distributions of CYP17A1 genotypes
As shown in Table 2, the genotype distributions for each SNP were in good agreement with the predicted Hardy–Weinberg equilibrium values (data not shown). For total, male and female subjects, the distribution of SNP4 (rs10786712) and SNP5 (rs2486758) genotypes did not show a significant difference between CAD and control subjects (p>0.05 respectively). For total subjects, distribution of rs4919686 genotypes, dominant model (AC + CC vs. AA), recessive model (AA+AC vs. CC) and allele frequency showed significant difference between CAD and control subjects (p=0.034, p=0.030, p=0.047 and p=0.011, respectively); the dominant model, recessive model, and allele frequency of rs4919686 were significantly higher in subjects with CAD than in controls (37.7% vs. 28.2%, 5.3% vs. 1.8%, and 21.5% vs. 15.0%). Distribution of rs1004467 genotypes; dominant model (CC + CT vs. TT), recessive model (CT+TT vs. CC) and allele frequency showed significant difference between CAD and control subjects (p<0.001, p=0.001, p<0.001 and p<0.001), and the dominant model, recessive model, and allele frequency of rs1004467 were significantly higher in controls than in CAD subjects (83.8% vs. 70.9%, 32.0% vs. 18.1%, and 57.9% vs. 44.5%). Distribution of rs4919687 genotypes; dominant model (AA + AG vs. GG), recessive model (AG+GG vs. AA) and allele frequency showed significant difference between CAD and control subjects (all p<0.001), and the dominant model, recessive model, and allele frequency of rs4919687 were significantly higher in CAD patients than in controls subjects (58.4% vs. 41.7%, 19.6% vs. 7.6%, and 39.0% vs. 24.7%).
Genotype and allele distributions in patients with CAD and control participants.

CAD: coronary artery disease; n: number of participants; SNP: single nucleotide polymorphism.
For men, the distribution of rs4919687 genotypes, dominant model (AA + AG vs GG), and recessive model (AG+GG vs. AA) showed significant difference between CAD and control subjects (p<0.001, p=0.001, and p<0.001), and the dominant model and recessive model of rs4919687 were significantly higher in CAD patients than in control subjects (63.3% vs. 44.7%, 24.9% vs. 8.5%, respectively). For women, the distribution of rs1004467 genotypes, dominant model (CC + CT vs. TT), recessive model (CT+TT vs. CC) and allele frequency showed significant difference between CAD and control subjects (p<0.001, p<0.001, p=0.001 and p<0.001), and the dominant model, recessive model, and allele frequency of rs1004467 were significantly higher in controls than in CAD subjects (98.8% vs. 70.5%, 51.9% vs. 25.6%, and 75.3% vs. 48.1%).
Logistic regression analyses
Multiple logistic regression analysis for CAD patients and control subjects (rs1004467).
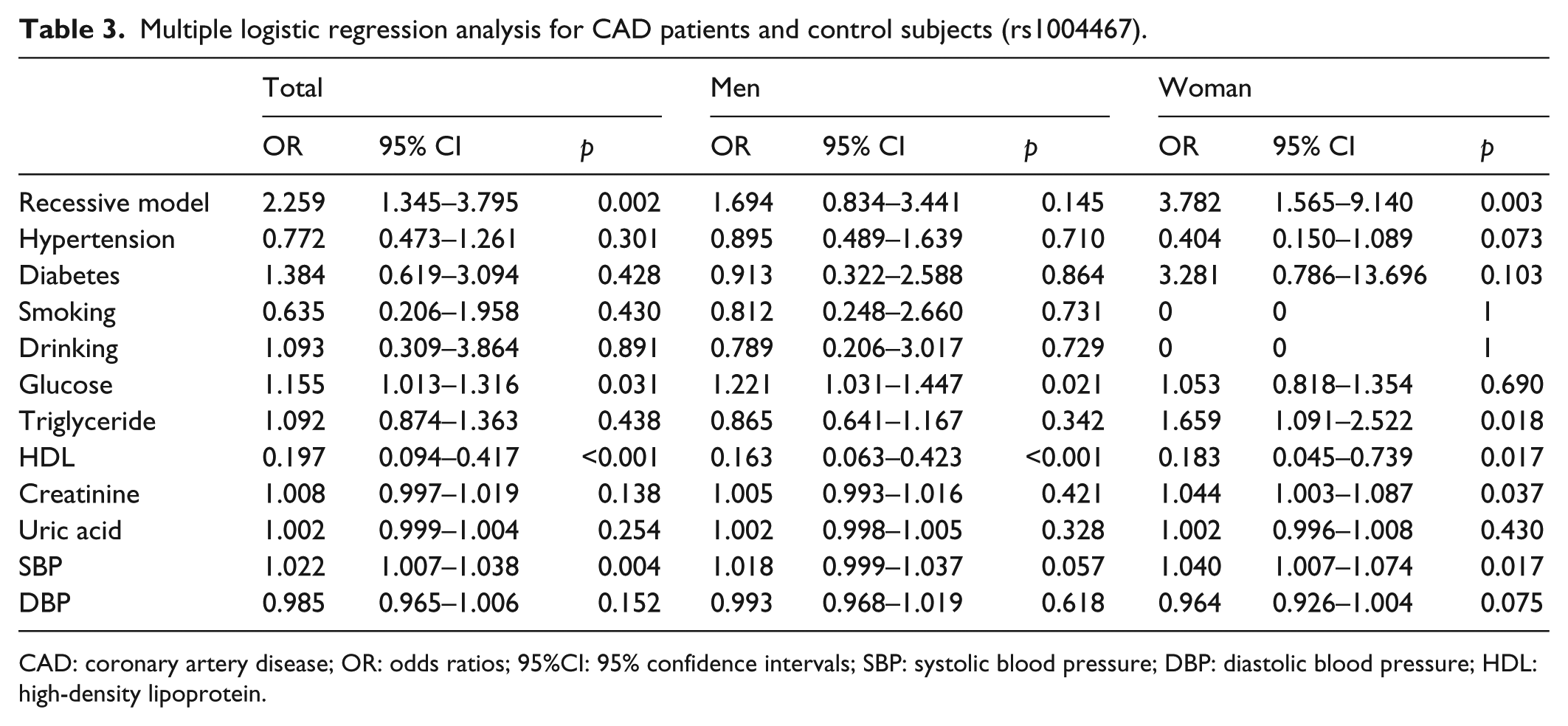
CAD: coronary artery disease; OR: odds ratios; 95%CI: 95% confidence intervals; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein.
Multiple logistic regression analysis for CAD patients and control subjects (rs4919686).

CAD: coronary artery disease; OR: odds ratios; 95%CI: 95% confidence intervals; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein.
Multiple logistic regression analysis for CAD patients and control subjects (rs4919687).

CAD: coronary artery disease; OR: odds ratios; 95%CI: 95% confidence intervals; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: High-density lipoprotein.
LD analysis
Table 6 shows patterns of LD analysis in the CYP17A1 gene. For all five SNPs the r2 values were below 0.5; for one haplotype block |D’| values were beyond 0.25. Because the |D’| for SNP2–SNP3 was <0.25, this meant that SNP2 and SNP3 could not be used to construct haplotypes. We constructed haplotypes using SNP1, SNP4, and SNP5.
Pairwise linkage disequilibrium for five SNPs.
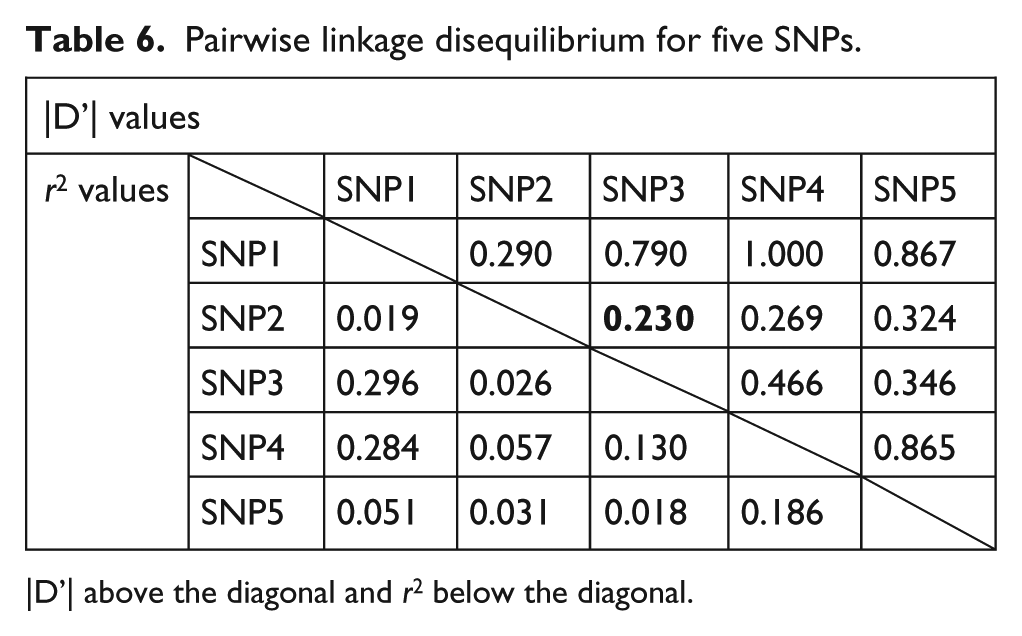
|D’| above the diagonal and r2 below the diagonal.
Haplotype analyses
As shown in Table 7, in the haplotype-based case-control analysis, haplotypes were established through the use of different combinations of the three SNPs. For total subjects, the overall distribution of the haplotypes established by SNP1–SNP4 and SNP1–SNP4–SNP5 were significantly different between the CAD patients and the control subjects (p=0.006, and p=0.030, respectively). In total, frequencies of the C–T haplotype established by SNP1–SNP4, the C–T haplotype established by SNP1–SNP5, and the C–T–T haplotype established by SNP1–SNP4–SNP5 were significantly higher for the patients with CAD as compared with the control subjects (p=0.007, p=0.024, and p=0.013, respectively). The frequency of the A–T haplotype established by SNP1–SNP4, and the A–T–T haplotype established by SNP1–SNP4–SNP5 was significantly higher for the control subjects as compared with the CAD patients (p=0.017, and p=0.046). For men, the overall distribution of the haplotypes established by SNP1–SNP4 was significantly different between the subjects with CAD and the controls (p=0.026). In men, the frequency of the A–T haplotype established by SNP1–SNP4, and the A–T–T haplotype established by SNP1–SNP4–SNP5 was significantly lower for the control subjects as compared with the CAD patients (p=0.022 and p=0.039). The frequency of the C–T haplotype established by SNP1–SNP4 was significantly higher for CAD patients than for controls (p=0.043). For women, the overall distribution of haplotypes was not significantly different between the CAD patients and the control subjects.
Haplotype analysis in patients with CAD and in control subjects.

CAD: coronary artery disease; SNP: single nucleotide polymorphism.
Haplotypes with frequencies >0.03 were estimated using SHEsis software; the p-value was calculated by permutation test using the bootstrap method.
Discussion
An association with CYP genetic polymorphism has been established in numerous diseases such as hypertension, CAD, heart failure, stroke, cardiomyopathy and arrhythmias. 9 In our study, we found the variation in CYP17A1 gene is associated with CAD in a Chinese Uygur population, and after multivariate adjustment the associations between CYP17A1 gene polymorphisms and CAD are still maintained. The etiology and pathogenesis of CAD include disorders of lipoprotein metabolism, 27 hypertension, 28 insulin resistance or diabetes, 29 the impairment and inflammation of vascular endothelium,30,31 and the disturbance of blood coagulation and the fibrinolytic system. 32
As previously mentioned, CYP17A1 has two kinds of enzyme activity: 17alpha-hydroxylase and 17,20-lyase activities convert 17-alpha OH pregnenolone to dehydroepiandrosterone, which is a precursor to sex hormones. P450c17 protein is an important enzyme that catalyzes the formation of all endogenous androgens. Therefore, CYP17A1 genetic mutations potentially reduce androgen biosynthesis. In the clinical setting, countering androgen biosynthesis by inhibition of CYP17A1 is a rational approach for therapeutic intervention in castration-resistant prostate cancer. 33
In recent years, many clinical studies have shown that testosterone levels play an important role in the progress of CAD among elderly men, 34 whereas lower testosterone levels promote CAD. 35 In addition, some evidence has indicated that testosterone is also related to CAD risk factors, for example, disorders of lipoprotein metabolism is also one of the primary mechanisms of CAD, 27 and research shows a positive correlation between the levels of testosterone and HDL-C and a negative correlation between the levels of testosterone and TG, TC, LDL-C and VLDL. Malkin et al. confirmed that the low levels of testosterone can lead to lipid disorders, and supplementing testosterone can correct dyslipidemia. 36 Insulin resistance and diabetes are significant independent risk factors for CAD. 29 Selvin et al. indicated that there is a relationship between diabetes and low free or low bioactive testosterone levels. 37 The dysfunction of vascular endothelium is a key mechanism in the occurrence and development of CAD,30,31 the levels of physiological testosterone can promote endothelial cells to release nitric oxide through improved vascular endothelial function, and low levels of testosterone can decrease vascular endothelial function and promote the occurrence of CAD. 38 Blood coagulation and the fibrinolytic system is an important mechanism in CAD; 32 physiological levels of testosterone can improve the function of endothelial cells 39 promote expression of tissue-plasminogen activator and inhibit the secretion of plasminogen activator inhibitor; and low levels of testosterone can increase the levels of proteins related to clotting factor VIII, cause endothelial dysfunction and vascular inflammatory reaction, and increase the incidence of CAD. Normal estrogen signaling is also dependent on CYP17A1. Estrogen plays a very important role in many physiological and pathological process, such as mediation of vasoconstriction, vascular endothelium repair, lipid metabolism, glucose metabolism and insulin-related signal transduction pathways, etc., which directly or indirectly affect the function of cardiovascular system. In women, estrogen seems to be protective for the cardiovascular system.20-22 Wellons et al. thought early menopause is associated with an increased risk of CAD, 40 and high levels of endogenous estrogen may explain the low prevalence of CAD in premenopausal women. 41
In our study, we found that polymorphisms of the CYP17A1 gene were associated with CAD in a Uygur population. For rs4919686, in total, the frequency of the C allele is higher in CAD patients than in control subjects; there were significant differences in genotypes, dominant model, and recessive model. After multivariate adjustment of confounding factors such as plasma concentration of TG, UA, HDL, Glu, Cr, incidence of hypertension, diabetes, drinking, and smoking, the significant difference was retained. This indicated that the C allele is a risk factor for CAD. For rs1004467, compared with men, in total subjects and women, the frequency of C allele was higher in control subjects than in CAD patients, and there were significant differences in genotypes, dominant model, and recessive model. The significant difference was retained after multivariate adjustment of confounding factors for CAD, and there was no difference for the C allele between CAD patients and control subjects in men. This indicated that the C allele might be protecting against for CAD in total subjects and in women. For rs4919687, compared with women, in total subjects and men, the genotypes, dominant model, and recessive model were significantly higher in CAD patients than in control subjects. The significant difference was retained after multivariate adjustment of confounding factors for CAD, in total; the frequency of the A allele is higher in CAD patients than in control subjects, there is no difference for the A allele between CAD patients and control subjects in women. This indicated that the A allele is a risk factor for CAD in total subjects, and the AA genotype of rs4919687 could be a risk genetic marker of CAD in total subjects and in men. In addition, based on these findings, we hypothesized that haplotype analysis would be useful for the assessment of associations between haplotypes and CAD. For total subjects and men, we succeeded in identifying two susceptible haplotypes, the C-T of SNP1-SNP4 as well as the C-T-T of SNP1-SNP4-SNP5, and two protective haplotypes, the A-T of SNP1-SNP4 as well as the A-T-T of SNP1-SNP4-SNP5. These haplotype analysis results are consistent with the genotype analysis results of SNP1 (rs4919686), that the C allele confers risk and the A allele is protective. For the total subjects we discovered a susceptible haplotype, the C-T of SNP1-SNP5; however, the overall distribution of this haplotype was not significantly different between the CAD patients and the control subjects (p=0.057).
In conclusion, this is first study to investigate the differences between the human CYP17A1 gene and CAD in the Chinese Uygur population, and is the first haplotype-based case-control study to correlate its association with CAD. The C allele of rs4919686 in the CYP17A1 gene could be a genetic marker for susceptibility. The C allele of rs1004467 could be a protective genetic marker, and the T allele could be a genetic marker for risk of CAD in total subjects and women. The A allele of rs4919687 may be a genetic risk marker and the G allele may be a genetic protective marker of CAD in total subjects. The AA genotype of rs4919687 could be a genetic risk marker of CAD in total subjects and men. Additional studies will need to be undertaken in order to isolate the functional mutations which associate polymorphisms of the CYP17A1 gene with CAD.
Limitation of the study
The present study was limited by the relatively small sample size. This may have led to weak statistical significance and wide CIs when estimating OR.
Footnotes
Conflict of interest
None declared.
Funding
This study was supported by National Natural Science Foundation of China (81160017 and 81470014) and Xinjiang Science and Technology Projects (201491181).