
Abstract
Introduction:
Angiotensin II receptor type 1 mediates the major cardiovascular effects of angiotensin II to regulate blood pressure. Polymorphisms of angiotensin II receptor type 1 are associated with essential hypertension, but the results are inconsistent and conflicting. The aim of the present study is to assess the association between angiotensin II receptor type 1 polymorphisms and essential hypertension risk in Chinese Hani and Yi minorities.
Methods:
This study recruited 692 unrelated Chinese Hani subjects (case vs. control = 346:346) and 615 unrelated Chinese Yi subjects (case vs. control = 303:312). Twelve selected single nucleotide polymorphisms in the angiotensin II receptor type 1 gene were genotyped using a polymerase chain reaction-restriction fragment length polymorphism method.
Results:
Statistical analysis indicated that the GC+CC genotype of rs387967 was significantly associated with the decreased susceptibility to essential hypertension compared with GG in a Yi population (odds ratio = 0.58, 95% confidence intervals 0.41–0.83, P = 0.003). Allele C was a protective allele for essential hypertension (odds ratio = 0.78, 95% confidence intervals 0.61–0.99, P = 0.040). This association was confirmed respectively by comparing systolic blood pressure and diastolic blood pressure between different genotypes and between different alleles, which indicated that the genotype (GC+CC) had a tendency of lower systolic blood pressure and diastolic blood pressure than GG (PSBP = 3.716 × 10–4, PDBP = 1.187 × 10–3); Carriers with C had lower systolic blood pressure and diastolic blood pressure (PSBP = 7.301 × 10–3, PDBP = 9.142 × 10–4). Another single nucleotide polymorphism (rs2638360) was analysed in a Hani minority, then replicated in a Yi minority. The C allele showed a consistent risk trend for essential hypertension in two independent populations (Hani: odds ratio = 1.74, 95% confidence intervals 1.01–2.99, P = 0.046; Yi: odds ratio = 1.27, 95% confidence intervals 0.82–1.96, P = 0.277). Meta-analysis revealed that the C allele could significantly increase the risk of essential hypertension (odds ratio = 1.44, 95% confidence intervals 1.02–2.02, P = 0.037).
Conclusion:
Our findings suggest that rs387967 is associated with the susceptibility to essential hypertension in a Yi population and the tendency was replicated in systolic blood pressure and diastolic blood pressure detection. Meta-analysis revealed that C allele of rs2638360 could significantly increase the risk of essential hypertension. The two single nucleotide polymorphisms maybe play a role in the pathology of essential hypertension.
Keywords
Introduction
Essential hypertension (EH) is characterized by a complex mode of multiple environmental and genetic factors. 1 Epidemiological studies and clinical trials implied that EH is mainly caused by genetic factors. Family-based studies have shown that the genetic contribution to the variation of individual blood pressure (BP) reached 23% 2 and up to 60% in twin research. 3
The renin-angiotensin-aldosterone system (RAAS), which regulates water and salt homeostasis, plays an important role in regulating BP, an independent risk factor for cardiovascular and cerebrovascular diseases. Genes encoding RAAS components are considered as candidates for EH study, including angiotensin II receptor type 1 (AGTR1), angiotensin-converting enzyme gene, angiotensinogen gene and so on.
The human AGTR1 gene maps to chromosome 3q24 and comprises five exons. It encodes a membrane protein with 359 amino acids, which comprised well-conserved seven-transmembrane domains. 4 AGTR1 encodes the type 1 receptor, which mediates the main cardiovascular effects of angiotensin II including vasoconstriction, stimulation of Na+ reabsorption and aldosterone secretion. This gene may play a role in the generation of reperfusion arrhythmias following restoration of blood flow to the ischaemic or infarcted myocardium. 5 It is an important effector controlling BP and volume in the cardiovascular system.
Much research showed that genetic variances in the AGTR1 gene locus influenced the risk of EH. 6 The polymorphism (A1166C, rs5186) in AGTR1 was a well-studied single nucleotide polymorphism (SNP) associated with hypertension, arterial stiffness and end-stage renal disease.7–10 Rs275645 within AGTR1 was related to hypertension. 11 Rs12695895 was significantly associated with hypertension. 12 These studies indicated that the AGTR1 gene may be involved in the pathogenesis of EH. However, there have been some conflicting reports. SNPs in AGTR1 were not related to the response to antihypertensive treatment in Kazakans. 13 SNP A1166C lacked association with BP status in Japanese individuals and Indian participants.14,15 The studies above indicate that the association between AGTR1 mutations and EH is heterogeneous in area and nationality. Hence, replication of associated findings in different populations becomes inevitable. Thus, in the present study, a case–control approach was performed to explore the contribution of polymorphisms in the AGTR1 gene to the risk of EH in the Hani and Yi populations in China.
Methods
Study populations
This case–control study consisted of 692 independent Chinese Hani subjects and 615 unrelated Chinese Yi subjects. Among them, 692 Hani subjects include 346 cases with EH and 346 controls and 615 Yi subjects were composed of 303 cases with EH and 312 controls. All participants were selected from individuals undergoing an investigation of hypertension epidemiology in the Yunnan University from May, 2002 to May, 2003.
Samples were selected based on the criteria reported previously. 16 In this case–control study, consistent criteria of diagnosis for EH is defined as systolic BP (SBP) ≥ 140 mmHg and/or diastolic BP (DBP) ≥ 90 mmHg. Participants with diabetes mellitus, secondary hypertension, myocardial infarction, cerebrovascular accident or other serious diseases were excluded. The normotensive group was composed of subjects with SBP/DBP < 140 / 90 mmHg and without history of hypertension. The confounding factors, sex and age, are matched. This study was performed with the approval of the ethical committees of the Yunnan University (Yunnan, China). At recruitment, written informed consent was obtained from all the participants.
Selection of SNPs
Several large-scale studies based on SNPs have revealed that linkage disequilibrium (LD) patterns vary across the human genome with some regions of high LD interspersed with regions of low LD.17,18 TagSNPs representing remaining SNPs can efficiently identify most gene haplotypes. We downloaded the genotype data of the AGTR1 gene from the dbSNP database (http://www.ncbi.nlm.nih.gov) and the HapMap database (http://hapmap.ncbi.nlm.nih.gov). To ensure enough statistical power, a value of 0.10 of minor allele frequency was set as the threshold value of inclusion in this research. The tag SNPs were selected to predict the remaining common SNPs with r2 ≥ 0.8 using Haploview 4.1 software (http://www.broad.mit.edu/mpg/haploview). After screening, seven tagSNPs were identified. Another five well-studied SNPs in the promoter and 5’-UTR of AGTR1, rs5186 (A1166C), rs275653, rs387967, rs422858 and rs1492078, were selected. The AGTR1 gene structure and relative position and information of these 12 SNPs are shown in Figure 1 and Tables 1 and 2, respectively in Supplementary Material.
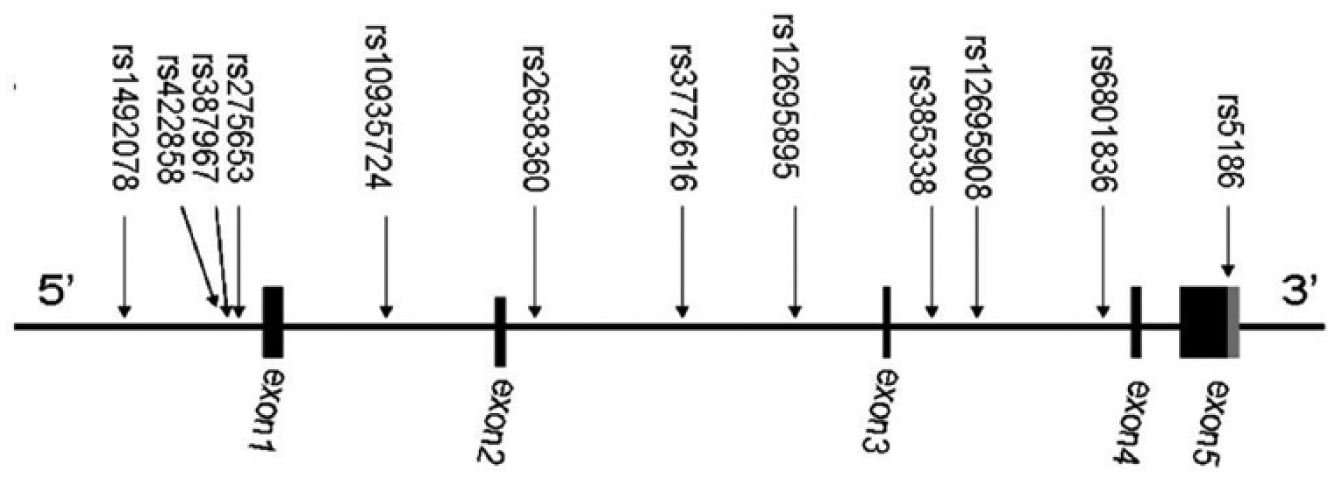
The AGTR1 structure and relative position of 12 tag single nucleotide polymorphisms. Black boxes indicate exons, lines indicate introns and a grey box indicates 3’-UTR.
Baseline characteristics of Hani and Yi minorities.

Hani: Hani minority, Yi: Yi minority, EH: essential hypertension, Non-EH: non-essential hypertension, BMI: body mass index, SBP: systolic blood pressure, DBP: diastolic blood pressure.
P < 0.001.
Association of rs387967 with EH in the Yi minority.

OR: odds ratio, CI: confidence interval, EH: essential hypertension, Non-EH: non-essential hypertension.
ORs, 95% CIs and P values were calculated by logistic regression while adjusting for age, sex and BMI.
The Yi population consists of 277 patients with EH and 287 subjects with non-EH, respectively. The number of genotyped samples varies due to genotyping failure.
Genotyping of SNPs
Genomic DNA was extracted from peripheral blood by standard phenol-chloroform protocols and stored at −80°C. The 12 SNPs selected were genotyped by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). The primers, annealing temperature, length of PCR products, related restriction endonuclease and digested bands are shown in Tables 3 and 4 in Supplementary Material.
The difference of blood pressure between rs387967 genotypes in the Yi minority.
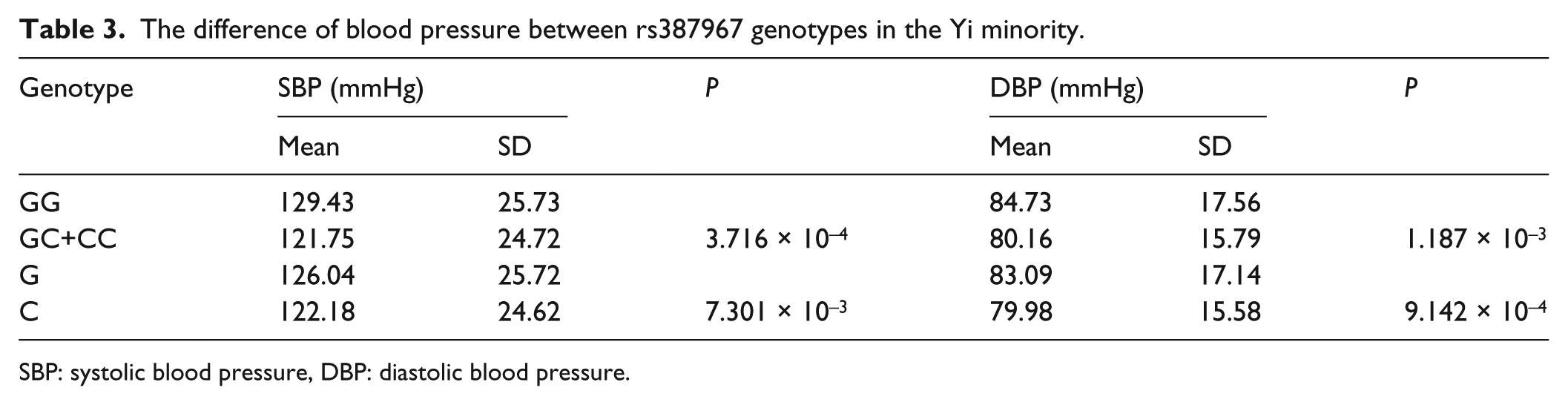
SBP: systolic blood pressure, DBP: diastolic blood pressure.
Association of rs2638360 with EH.

OR: odds ratio, CI: confidence interval.
ORs, 95% CIs and P values were calculated by logistic regression while adjusting for age, sex and BMI.
Hani and Yi populations consist of 325 and 277 patients with EH and 330 and 287 patients with non-EH, respectively. The number of genotyped samples varies due to genotyping failure.
A meta-analysis combining two independent case–control studies. The P values for heterogeneity among sample sets are 0.282 for TC+CC vs. TT group and 0.375 for C vs. T group.
Nested PCR technology was employed to amplify the target SNP fragments. Genomic DNA underwent the first run of PCR with the long primers, then the product underwent a second run with the nest primers (see Table 3 in Supplementary Material). Each 15 μL reaction volume contained 0.5 units of Taq DNA polymerase (TaKaRa Biotechnology Co. Ltd., Japan), 1.5 μL of 10 × buffer supplied (containing 25 mM MgCl2), 0.2 μL of 10 mM each primer, 1 μL of 2 mM dNTPs and 1 μL of genome DNA or PCR product. The PCR products were digested with corresponding restriction enzymes listed in Table 4 in Supplementary Material. Digested fragments were separated on 2% agarose gel and stained with ethidium bromide. For quality control, 5% of the samples were randomly selected to perform direct sequencing.
Statistical analysis
Statistical software SPSS 16 (SPSS Inc., Chicago, USA) was used to carry out the analysis. Genotype and allele frequency were determined by direct counting. The significance of deviation from the Hardy–Weinberg equilibrium was assessed by the Chi-square test. Binary logistic regression analysis was used to estimate the independent effect of each genetic variant on the risk of EH adjusted for gender, age and body mass index (BMI). The association between polymorphisms and EH risk was estimated by P value, odds ratio (OR), and 95% confidence interval (95% CI). T-test was used to assess the BP difference between genotypes. Bonferroni’s correction was used to assess the probability of a spurious association due to multiple comparisons. A P value less than 0.05 was considered statistically significant and all tests were two-sided.
Results
Clinical characteristics
A summary of baseline characteristics of the EH and non-EH subjects is presented in Table 1. The majority of the EH and non-EH groups in the Hani minority is male and the same with the Yi minority. The ratios of male to female were similar in the two minorities. The average age is 49.3 and 50.2 years in the EH and non-EH groups of the Hani minority, respectively. It is 44.2 and 42.8 years in the Yi minority. There was no significant difference between cases and controls for age. Hypertensive patients exhibited significantly higher SBP, DBP and BMI compared with non-EH subjects. Confounding factors, gender, age and BMI, have been adjusted in the subsequent association analysis.
Genetic association between SNPs and EH
In the present study, 12 SNPs were genotyped in Hani (case = 346, control = 346) and Yi (case = 303, control = 312) populations using the PCR-RFLP method. Rs387967 in the Hani minority and rs3772616 in the Yi minority were not in agreement with those predicted by Hardy–Weinberg equilibrium in a control group (see Table 5 in Supplementary Material), so the two SNPs were excluded in the next analysis. For other polymorphisms in control subjects, no significant deviation from the Hardy–Weinberg equilibrium was found. The 12 SNPs genotype and allele distributions are shown in Tables 6 and 7 in Supplementary Material.
Difference of blood pressure between rs2638360 genotypes in Hani and Yi minorities.
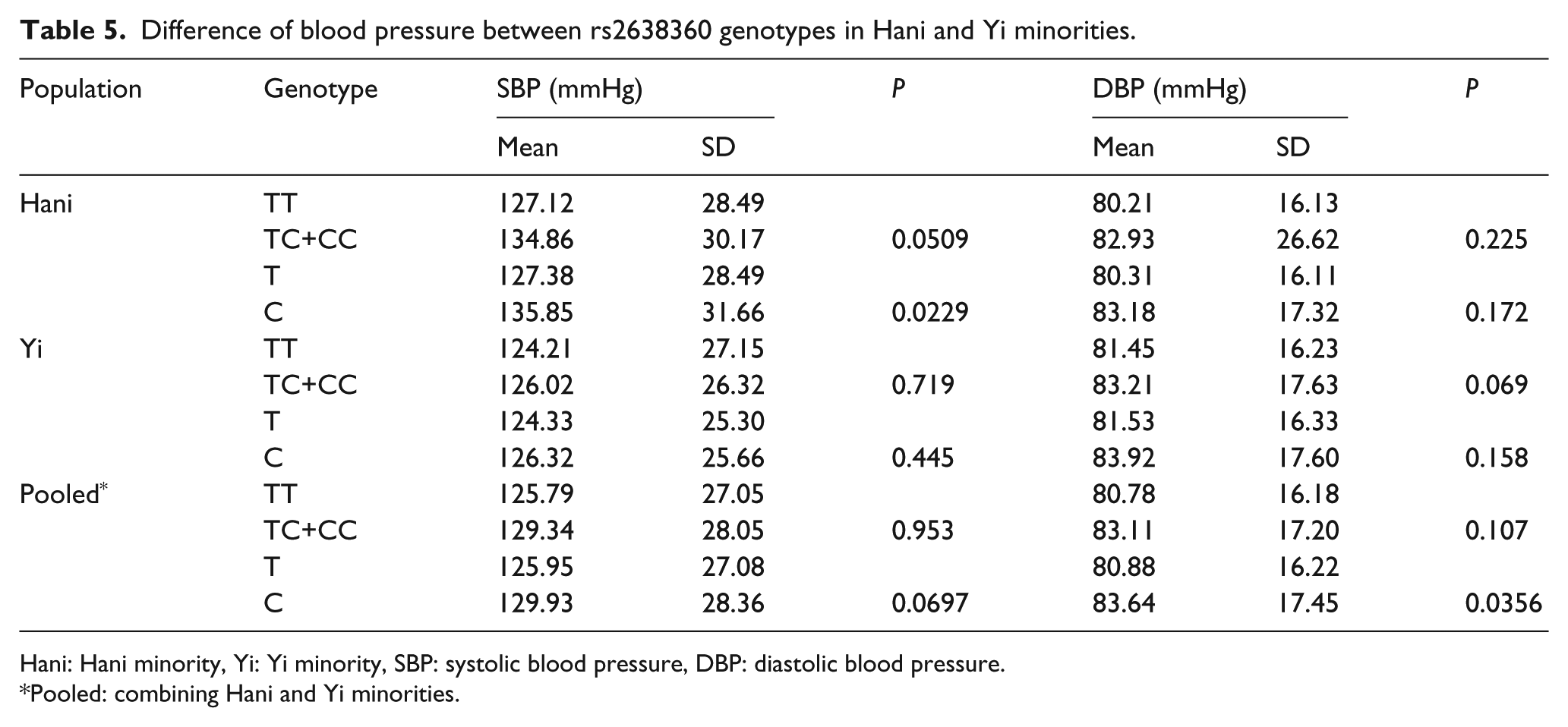
Hani: Hani minority, Yi: Yi minority, SBP: systolic blood pressure, DBP: diastolic blood pressure.
Pooled: combining Hani and Yi minorities.
SNP (rs387967) was analysed only in the Yi population for deviation from the Hardy–Weinberg equilibrium in the Hani population. After adjustment for gender, age and BMI in the dominant model (GC+CC vs. GG), logistic regression analysis showed that the combined genotype (GC+CC) significantly reduced the risk of EH (OR = 0.58, 95% CI 0.41–0.83, P = 0.003, Table 2) and the C allele played a protective effect for EH (OR = 0.78, 95% CI 0.61–0.99, P = 0.040) in the Yi population. The hereditary effects were consistent. After Bonferroni’s correction, the P value was still less than 0.05 in the dominant model (P = 0.036, 0.003 × 12).
The associated results were replicated by the SBP and DBP distribution between genotypes and alleles, respectively (shown in Table 3). The SBP and DBP of subjects with GC+CC genotype were lower than those with CC genotype (PSBP = 3.716 × 10–4, PDBP = 1.187 × 10–3). Accordingly, carriers with C allele had lower SBP and DBP compared with those with G allele (PSBP = 7.301 × 10–3, PDBP = 9.142 × 10–4). The results implied that rs387967 was associated with EH. Individuals who carried the combined genotype GC+CC or allele C more easily suffered from EH.
Another SNP (rs2638360) was analysed in the Hani minority, then replicated in the Yi minority. Logistic regression analysis indicated that the combined genotype of rs2638360, TC+CC, was associated with the risk of EH (OR = 1.79, 95% CI 1.00–3.20, P = 0.049, Table 4). Meanwhile, gender, age and BMI were adjusted in the Hani population. Carriers with C allele were more likely to suffer from high BP (OR = 1.74, 95% CI 1.01–2.99, P = 0.046, Table 4). A follow-up analysis detected that rs2638360 was associated with EH in the same direction in the Yi minority, although there was no significant difference between EH and non-EH for genotype distribution (OR = 1.19, 95% CI 0.75–1.90, P = 0.457) and allele frequency (OR = 1.27, 95% CI 0.82–1.96, P = 0.277). Meta-analysis can more powerfully estimate the true effect size than a single population-based study. To increase power, meta-analysis was done and revealed that the P value of association between genotype and the EH risk was marginally significant (OR = 1.40, 95% CI 0.97–2.01, P = 0.072) and the C allele can significantly increase the risk of EH (OR = 1.44, 95% CI 1.02–2.02, P = 0.037). C allele of rs2638360 showed a consistent risk trend for EH in two independent populations and the subsequent meta-analysis in spite of no significant association in the Yi population.
SBP and DBP tended to be higher in subjects with rs2638360 C allele than those with the T allele in the pooled populations (P < 0.05, Table 5). Especially, the P value in a DBP test has exceeded the significant level (P = 0.0356).
Haplotype analysis and interaction between SNPs failed to pass multiple testing (data not provided).
Discussion
To our best knowledge, this is the first report of the genetic association between the polymorphisms of AGTR1 and EH in Chinese minorities. We found that the rs387967 in the promoter of AGTR1 was associated with the susceptibility to EH in the Yi minority after adjusting for multiple testing. Another rs2638360 may be an EH-related SNP for the same direction association in two independent populations and subsequent meta-analysis. Association results were confirmed by SBP and DBP distribution between different genotypes and then between different alleles.
Rs387967 is located in the promoter of AGRT1. A function prediction tool for SNPs, TF SEARCH (http://www.cbrc.jp/research/db/TFSEARCH.html), implied that a sequence containing G allele could be captured by transcription factor ADR1, which might promote AGRT1 transcription. 19 Our study also found that the G allele had a risk effect for EH. Increased G allele was significantly associated with higher SBP and DBP in the Yi minority. Hazen and his co-workers suggested taking the rs387967 as one of the markers to predict the development of hypertension. 20
Another associated SNP rs2638360 is located in the second intron of AGRT1. Intronic SNPs can change mRNA splicing and transcription of different spliceosomes. Transcriptional regulation prediction tool, TF SEARCH (http://www.cbrc.jp/research/db/TFSEARCH.html) and Consite (http://asp.ii.uib.no:8090/cgi-bin/CONSITE/consite/), pointed out that this SNP was a transcription factor binding site. Sequence with T allele could bind the transcription factor C/EBP α and β. C/EBP β was reported to be continuously elevated in porcine stromal-vascular. 21 The rs2638360 may be a transcript variant that occurred in an intron of a non-coding transcript. Further researching data are needed.
In all Hani and Yi subjects not receiving the anti-hypertension therapy, the SBP and DBP presented a natural process of EH. Interference of drugs on EH was effectively controlled. Further BP analysis verified our associated findings. The combined genotype (GC+CC) of rs387967 significantly decreased SBP and DBP levels. Individuals with C allele were not susceptible to hypertension. Risk effect of rs2638360 C allele on EH corresponded to the higher SBP and DBP level. Thus, these data strongly supported our molecular epidemiological findings that polymorphisms in the AGRT1 were associated with susceptibility to EH. They either directly altered AGTR1 expression or were in LD with the causative variant, which was directly involved in hypertension susceptibility. Although the exact mechanism by which rs387967 and rs2638360 influenced the AGTR1 gene required further investigation, the genetic association between AGTR1 polymorphisms and susceptibility to EH was biologically plausible. It has been reported that AGTR1 polymorphisms are related to susceptibility to EH.7–9,22 AGTR1 played an important role in vasoconstriction, aldosterone and vasopressin release and salt and water retention. RAAS was implicated as one major effector of EH. Blockade of RAAS with AGTR1 antagonists can provide a beneficial therapeutic approach for the treatment of hypertension. 23
Some SNPs within AGTR1, which were reported to be associated with EH, were not replicated in our study. This could be attributed mainly to multiple hypothesis testing, heterogeneous study populations and inadequate power. 24 The rs387967 derived from the Hardy–Weinberg equilibrium in the Hani minority but not in the Yi minority, which confirmed that Chinese minorities were genetic heterogeneous.
In reviewing the results of this study, several potential limitations should be kept in mind. First, our case–control study is preliminary and limited because information of risk factors such as chronic disease status and pathogens infected was not completely obtained. Second, some association studies have reported identification of the genes that may relate to the susceptibility to EH. Most of the results, however, could not be replicated in subsequent studies in other populations. Although we found a significant association between rs387967 and the risk of EH, our initial findings should be independently verified in other populations. Further investigations in a larger sample size on the level of gene–gene or gene–environment interaction were necessary to confirm the results of the present study. Without rigorous replication, we cannot exclude the possibility that these findings are due only to chance. Although our study population was small, the cohort design enabled us to investigate the impact of genetic markers. This could help in identifying those SNPs that are at greatest risk. Therefore, any association reported in the present study should be interpreted with great caution.
We have shown that AGTR1 polymorphism may be a genetic risk factor for EH in Chinese Hani and Yi minorities. Knowledge of the genetic factors involved in the pathogenesis of EH as presented here could deepen our understanding on BP regulation. It will improve the treatment and prevention of EH.
Footnotes
Acknowledgements
We thank all the patients participating in this study.
Declaration of Conflicting Interests
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the National Natural Science Foundation of China (No. U0932603 and U81460076).