
Abstract
Objective:
Angiotensin-converting enzyme (ACE) I/D polymorphism has been reported to be associated with lung cancer, but the results of previous studies are conflicting. The present study was designed to investigate the association between this polymorphism and the risk of lung cancer using a meta-analysis of the published studies.
Methods:
Two investigators independently searched the PubMed, Embase and CNKI databases. This meta-analysis covered six case-control studies, including 807 lung cancer patients and 816 healthy controls.
Results:
The results of this meta-analysis based on all the studies showed no significant association between ACE I/D gene polymorphism and lung cancer risk (DD vs II: OR = 1.18, 95% CI = 0.68–2.04; DI vs II: OR = 0.93, 95% CI = 0.56–1.53; DD+DI vs II: OR = 1.01, 95% CI = 0.68–1.50; DD vs II+DD: OR =1.11, 95% CI = 0.73–1.71). In the subgroup analysis by race and the larger studies (n > 200 participants), no significant associations between the ACE I/D polymorphism and risk of lung cancer were indicated. However, when the analyses were restricted to small studies (n ≤ 200 participants), a significantly higher risk was observed (DD vs II: OR = 2.57, 95% CI = 1.24–5.30).
Conclusions:
This meta-analysis suggests that the ACE gene I/D polymorphism may not be associated with the risk of lung cancer, and the observed increase in the risk of lung cancer may be due to small-study bias.
Introduction
According to the International Agency for Research on Cancer of the World Health Organization, lung cancer is the most common cancer in the world, with an estimated 1.6 million new cases in 2008, representing one in eight of all new cancer cases. It is also the most common form of cancer death in the world, comprising nearly one in five of all deaths from cancer. 1 There are many factors contributing to lung cancer, of which environmental exposure, primarily to smoking, is the major risk factor. However, not all lung cancers are due to smoking, and increasing evidence for the association between genetic factors and identified lung cancer risk has been accumulated in hundreds of studies. 2 Existing evidence has suggested that genetic factors also play an important role in the pathogenesis of lung cancer. 3
Angiotensin-converting enzyme (ACE) is a zinc metallopeptidase that converts angiotensin I to angiotensin II (vasoconstrictor) and degrades bradykinin (vasodilator), regulating blood pressure and cardiovascular homeostasis. 4 Approximately 90% of the physiologic conversion of angiotensin I to angiotensin II takes place in the lungs. ACE in peripheral blood is thought to be identical to the lung enzyme and is proportional to blood oxygen concentration, suggesting that serum ACE activity is closely correlated with the enzyme concentration in the pulmonary tissue. 5 ACE plasma levels depend on a 287 bp insertion/deletion (I/D) polymorphism of the ACE gene located on chromosome 17q23. 6 Homozygotes for the D allele have the highest ACE plasma levels, homozygotes for the I allele have the lowest, and ID heterozygotes have intermediate levels.
Over the past few years, many studies have shown that the ACE I/D polymorphism may be closely associated with the risk of cancer, including breast, gastric, and prostate cancer. In addition, though, several studies found an association between ACE I/D polymorphism and lung cancer while others did not, suggesting that it may serve as a possible risk factor for lung cancer. Meta-analysis can be a useful tool in the detection of associations that could otherwise remain unseen in studies with small sample sizes, especially studies evaluating rare allele frequency polymorphisms. 7 This has recently become an important part of genetic research, mainly because it can reconcile previously conducted studies that gave inconsistent results. The present study investigated, by performing a meta-analysis, whether the ACE I/D polymorphism is associated with lung cancer risk.
Materials and methods
Literature search strategy
Literature databases including PubMed, Embase and China National Knowledge Infrastructure (CNKI) databases were searched for all articles on any association between ACE I/D polymorphism and the risk of lung cancer (last search update November 30, 2013). The search strategy was designed to identify all possible studies using the following keywords: “ACE I/D,” ”lung cancer,” “polymorphism,” “single nucleotide polymorphism” and “genetic polymorphism.” The search was not restricted by language, but all included studies had to be conducted on humans. Reference lists of previous reviews and meta-analyses were searched manually. Unpublished reports were not considered. If more than one article was published by the same author using the same case series, the study covering the greater number of individuals was included.
Inclusion and exclusion criteria
The studies included in the meta-analysis met all of the following inclusion criteria: (1) case-control studies conducted to evaluate the association between the ACE I/D polymorphism and the risk of lung cancer; (2) sufficient genotype data to calculate the odds ratios (ORs) and 95% confidence intervals (CIs); and (3) the paper clearly described the sources of cases and controls. Major exclusion criteria were as follows: (1) studies lacking case-control evaluation of the association between ACE I/D polymorphism and risk of lung cancer; (2) case reports, letters, reviews, meta-analyses and editorial articles; (3) studies based on incomplete raw data or for which no usable data were reported; and (4) duplicate studies.
Data extraction
Data were independently extracted by two investigators (Nan Wang and JianYou Li), and a consensus was reached on all of the items. To ensure quality, the most recent and complete articles were chosen if a study was published more than once. First author, year of publication, country, nationality, number of patients and controls, gene polymorphisms and evidence of Hardy-Weinberg equilibrium (HWE) were documented. Any encountered discrepancies were adjudicated by a discussion and a 100% consensus was reached.
Statistical analysis
We assessed HWE in the controls for each study using the goodness-of-fit test (chi-square or Fisher exact test) and p < 0.05 was considered as significant disequilibrium. ORs were used as a measure of the association between the ACE I/D polymorphism and risk of lung cancer under a homozygote comparison (DD vs II), a heterozygote comparison (DI vs II), a dominant model (DD+DI vs II) and a recessive mode (DD vs II+DI) between groups. 8 Both the Cochran’s Q statistic to test for heterogeneity and the I2 statistic to quantify the proportion of the total variation due to heterogeneity were calculated. A p value of more than the nominal level of 0.10 for the Q statistic indicated a lack of heterogeneity across studies, allowing for the use of a fixed-effects model; otherwise, the random-effects model was used. We examined the following study characteristics: ethnicity and study sample size (≤200 and >200 individuals). Sensitivity analysis was performed to assess the stability of the results. Publication bias was investigated with a funnel plot, which is the main graphical method of assessing bias. To supplement the funnel plot approach, the Begg’s test was adopted (p < 0.05 was considered statistically significant). Data analysis was performed using STATA version 12.0 (StataCorp LP, College Station, TX, USA).
Results
Study characteristics
A total of 151 articles were gleaned by a literature search of PubMed, Embase and CNKI databases, using different combinations of key terms. As shown in Figure 1, a final total of six case-control studies met our inclusion criteria,9 –14 including 807 cases and 816 controls. The genotype distributions in the controls of all studies were in agreement with HWE. There were three studies of Europeans12 –14 and three of Asians.9 –11 The information from these six studies and the numbers of cases and controls with II, DI and DD genotypes reported in each study are all presented in Table 1.

Flow diagram of the study search and selection process.
Characteristics of the included studies for meta-analysis.
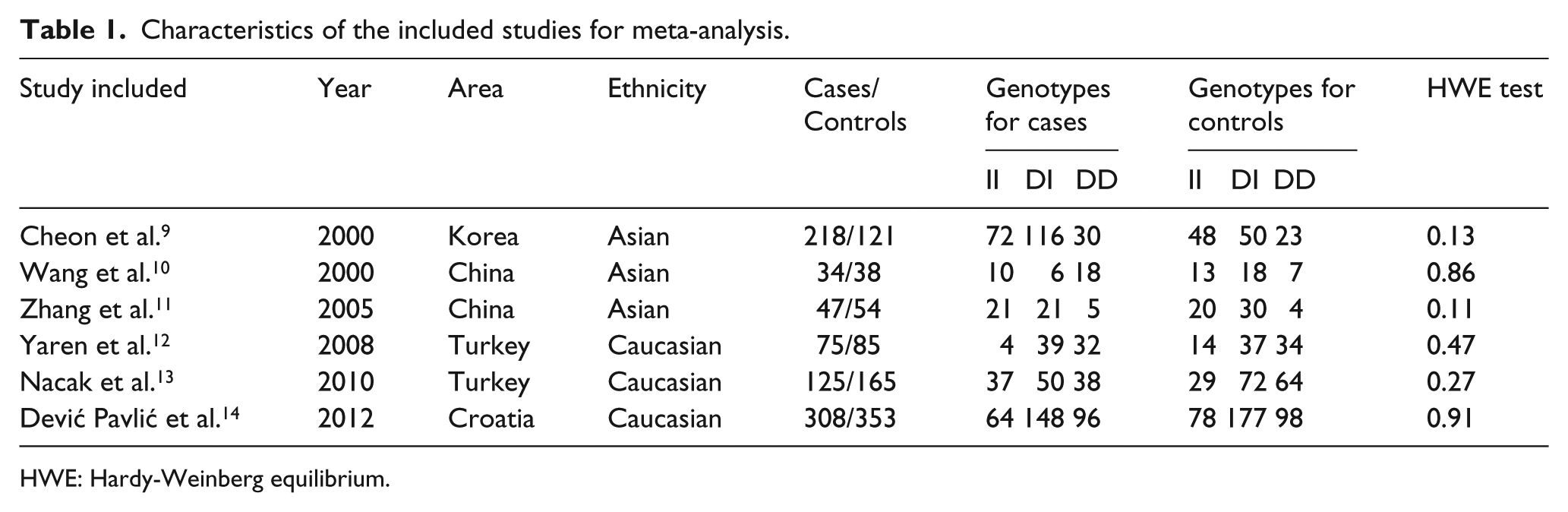
HWE: Hardy-Weinberg equilibrium.
Quantitative synthesis
The evaluation of an association between the ACE I/D polymorphism and the risk of lung cancer is displayed in Table 2. The results of this meta-analysis showed no significant association between the ACE I/D polymorphism and lung cancer risk in any of the genetic models (Figure 2, DD vs II: OR = 1.18, 95% CI = 0.68–2.04; DI vs II: OR = 0.93, 95% CI = 0.56–1.53; DD+DI vs II: OR = 1.01, 95% CI = 0.68–1.50; DD vs II+DI: OR = 1.11, 95% CI = 0.73–1.71). In a subgroup analysis by ethnicity, the studies included were divided into Asian and Caucasian populations, and no significant association was found between the ACE I/D polymorphism and lung cancer risk in Asians (DD vs II: OR = 1.20, 95% CI = 0.71–2.03; DI vs II: OR = 0.76, 95% CI = 0.30–1.92; DD+DI vs II: OR = 1.07, 95% CI = 0.74–1.54; DD vs II+DI: OR = 1.64, 95% CI = 0.45–6.01) and in Caucasians (DD vs II: OR = 1.09, 95% CI = 0.45–2.66; DI vs II: OR = 1.08, 95% CI = 0.50–2.35; DD+DI vs II: OR = 1.08, 95% CI = 0.50–2.42; DD vs II+DI: OR = 1.01, 95% CI = 0.79–1.30). However, when the analyses were restricted to three small studies (n ≤ 200 participants), meta-analysis results showed a significant association with the risk of lung cancer (DD vs II: OR = 2.57, 95% CI = 1.24–5.30). Sensitivity analyses were conducted by altering the statistic models. No material alteration was detected, indicating that our results were statistically robust (DD vs II: OR = 1.05, 95% CI = 0.79–1.39; DI vs II: OR = 0.97, 95% CI = 0.77–1.26; DD+DI vs II: OR = 1.00, 95% CI = 0.79–1.26; DD vs II+DI: OR = 1.05, 95% CI = 0.84–1.31).
Stratified analyses of the ACE I/D polymorphism and risk of lung cancer.

N = number of comparisons; p value of the Q-test for heterogeneity test. Random-effects model was used when p value for heterogeneity test <0.1; otherwise, fixed-effects model was used. ACE: angiotensin-converting enzyme; I: insertion; D: deletion; OR: odds ratio; CI: confidence interval.

Meta-analysis of the relationship between the ACE I/D polymorphism and lung cancer risk.
Publication bias
The publication bias of the meta-analysis of the association between the ACE I/D polymorphism and lung cancer risk was detected by Begg’s funnel plot; all graphical funnel plots of the included studies appeared to be symmetrical. Results showed that there was no publication bias (DD vs II: Begg’s test, p = 1.00, Egger test; DI vs II: Begg’s test, p = 1.00; DD+DI vs II: Begg’s test, p = 1.00; DD vs II+DI: Begg’s test, p =1.00, all p > 0.05, Figure 3).

Begg’s funnel plot for publication bias test (DD vs II).
Discussion
Genetic polymorphisms that alter the amount of protein expressed may have a substantial influence on disease activity. 15 Lung cancer is a complex disease, and many factors, including environmental and occupational exposure, cigarette smoking, and genetics, contribute to its progression. The I/D polymorphism accounts for 20% to 50% of the variance in ACE expression or activity in blood and tissues among individuals. 16 The relationship between ACE I/D polymorphism and risk of lung cancer has been addressed in several studies, and the results are controversial. An apparent discrepancy in the results may be due to ethnic differences, or to insufficient sample size. The aim of meta-analysis is to combine the same kinds of studies to increase the sample size and statistical power, thereby producing more authentic results.
This is the first meta-analysis to consider ACE I/D polymorphism and the risk of lung cancer. In the current meta-analysis, the association between ACE I/D polymorphism and the risk of lung cancer was examined by critically including all published studies. Ultimately, only six case-control studies were included, comprising a total of 807 patients and 816 healthy controls. The final results of this meta-analysis did not show any significant association between ACE I/D polymorphism and the risk of lung cancer. Because results may be affected by ethnicity, a race-related subgroup analysis was performed, and no significant association was found between ACE I/D polymorphism and susceptibility to lung cancer in either Caucasian or Asian populations. When stratifying by sample size (≤200), this meta-analysis detected a significant association between ACE I/D polymorphism and lung cancer. However, this conclusion was drawn using a small number of samples, which suggests that the observed associations between ACE I/D polymorphism and an increased lung cancer risk reflect chance observations rather than true associations, which is a small-study bias. Further sensitivity analysis confirmed the significance of the association between ACE I/D polymorphism and risk of lung cancer. No evidence collected in this meta-analysis indicated publication bias (p > 0.05).
The potential influence of ACE I/D polymorphism may be affected by gene-gene and gene-environment interactions. The effects of ACE I/D polymorphism on lung cancer may be attributable to linkage disequilibrium with the ACE gene A-240T and A2350G polymorphisms. 17 In addition, nicotine and its metabolites increase the expression and activity of ACE in human endothelial cells, 18 and higher levels of circulating ACE, which are associated with the ACE I/D polymorphism, are found in male smokers. 19 This suggests that the ACE I/D polymorphism may be correlated with tobacco smoking and with an increased risk of lung cancer development. However, one study could not be included in this meta-analysis, and further studies of gene-gene and gene-environment interactions must be taken into consideration for assessment of the risk of lung cancer.
The current meta-analysis has some limitations in this meta-analysis: 1) Only published studies were included, so publication bias may be an issue, even though the use of a statistical test did not indicate any; 2) because of incomplete raw data or publication limitations, some relevant studies could not be included in our analysis; and 3) gene-gene and gene-environment interactions were not tested in the present study because of the lack of information from the original studies.
In conclusion, this meta-analysis indicates that the ACE I/D polymorphism may be not associated with lung cancer risk, and the observed increase in the risk of lung cancer may be due to small-study bias. Because few studies are available in this field and because current evidence remains limited, large studies of adequate methodological quality, properly controlling for possible confounding factors, are greatly needed.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by a grant from Zhejiang Science and Technology R&D Fund (2014C33245), the Medical Scientific Research Foundation of Zhejiang Province (2012RCB039), and the Huzhou Science and Technology R&D Fund (2012YS02).