
Abstract
Objective:
Previous case-control studies on the relation between the angiotensin-converting enzyme (ACE) gene insertion/deletion (I/D) polymorphism and lung cancer were controversial. In this study, we aimed to further evaluate the relation between the ACE gene I/D polymorphism and lung cancer.
Methods:
We selected eight case-control studies related to the ACE gene I/D polymorphism and lung cancer by searching PubMed, EMBase, Chinese Biomedical Literature Database, and Wanfang database. We utilized Q-test and I2 test to test the heterogeneity between each study. To merge the odds ratio (OR) and 95% confidence interval, we utilized the fixed-effects model during the analyses.
Results:
The present study included 1612 patients with lung cancer and 1442 cancer-free control subjects. By meta-analysis, we did not find any association between the ACE gene I/D polymorphism and lung cancer in either genotype or allele distribution (DD vs. (ID+II): OR = 0.96, 95% CI (0.80–1.14), p = 0. 61; D allele vs. I allele: OR = 1.01, 95% CI (0.91–1.13), p = 0.79).
Conclusion:
We concluded that the ACE gene I/D polymorphism was not associated with lung cancer.
Introduction
Lung cancer is the most frequently occurring cancer in the world. There are 1.3 million new patients diagnosed with lung cancer every year. 1 Recently, lung cancer has been recognized as a complex multifactorial disease resulting from the interactions between many genetic and environmental factors. 2 During the past decade, there has been increasing scientific interest in understanding the complex relationship between lung cancer and the renin-angiotensin system (RAS).3–5 The RAS plays an important role in blood pressure and cardiovascular homeostasis.6,7 However, recently published data indicated that angiotensin II, the main biologically active peptide of the RAS, contributed to lung cancer development and progression.7,8 Accruing evidence suggests that divergence from the insertion (I) allele to the deletion (D) allele of this polymorphism is correlated with a higher plasma level of angiotensin-converting enzyme (ACE) activity. 10 Some studies have attempted to investigate the association between the ACE gene I/D polymorphism with lung cancer, but the results are often not reproducible.11–15 This fact was possibly due to inadequate sample sizes, patient selection, and ethnicity of the populations studied, and a single study might be insufficient to detect a possible small effect of the polymorphism on lung cancer. Meta-analysis is a useful method for investigating the associations between diseases and risk factors because it uses a quantitative approach to combine the results of different studies on the same topic, potentially providing more reliable conclusions.16,17 Considering the extensive role of ACE in the pathogenesis of lung cancer, a meta-analysis was performed on all eligible case-control studies to estimate the association between this polymorphism and lung cancer risks.
Materials and methods
Literature collection and screening
To identify all the articles that explored the association of ACE polymorphisms with lung cancer risk, we conducted a computerized literature search of PubMed, EMBase, Chinese Biomedical Literature Database, and Wanfang database using the terms “lung cancer (Medical Subject Headings (MeSH))” or “lung neoplasm” and “angiotensin-converting enzyme” or “ACE,” “polymorphism, or [single nucleotide polymorphism] SNP, or genotype, or insertion/deletion, or I/D, or D/I, or D/D or I/I,” without any restriction on language or publication year. By means of online retrieval and literature review, references obtained using the above-mentioned databases were reviewed again to ensure that no relevant studies were missed.
The inclusion criteria for the present study are as follows: (1) independently published case-control or cohort studies on the relation between the ACE polymorphism and lung cancer; (2) similar themes and methods; (3) sufficient information had to be provided to calculate the odds ratio (OR) with 95% confidence interval (CI); and (4) the distribution of genotypes in the control groups should be consistent with the Hardy-Weinberg equilibrium (HWE). Accordingly, the following exclusion criteria were also used: (1) abstracts and reviews; (2) studies in which the genotype frequencies were not reported; and (3) repeated or overlapping publications. For studies with the same case series by the same authors, the most recently published studies or studies with the largest numbers of subjects were included.
Quality assessment and data extraction
Two reviewers (Zhenshun Cheng and Rongli Ma) independently evaluated the studies and extracted the data using a standard approach according to the above-mentioned inclusion criteria. Discrepancies were resolved through discussion. We utilized the Cochrane Handbook 5.2 quality evaluation criteria to assess the methodological quality of included studies.
For each study, we abstracted the first author’s last name, year of publication, ethnicity of participants, numbers of cases and controls, and frequency of insertion or deletion genotypes. HWE was assessed using the χ2 test.
Statistical analysis
For each case-control study, the HWE of genotypes in the control group was assessed using Person’s Chi-square test. OR and 95% CI were used to assess the strength of the association between the I/D polymorphism and lung cancer risk. We calculated the OR and respective 95% CI by comparing the carriers of rare alleles with the wild homozygotes (DD vs. II+ID).We performed the present meta-analysis utilizing RevMan 5.2 software, which was provided by the Cochrane Collaboration. We utilized Q-test and I2 test to examine the heterogeneity between each study. In the present study, we selected the fixed-effects model to merge the OR. Analysis of sensitivity includes the difference of point estimation and CIs of the combined-effects value of different models to observe whether it changes the result. To test the publication bias, we utilized the RevMan 5.2 statistical software to make the funnel plot. A p < 0.05 was considered of significant difference.
Results
Study identification
As shown in Figure 1 and Table 1, a total of 223 publications were preliminarily detected; 203 publications were excluded because of the absence of RAS gene polymorphisms, the presence of gene expression analysis, and irrelevance of the study to lung cancer. Twelve studies were further excluded because they were only review papers, no ACE I/D genotype was mentioned, and publications were duplicated. Therefore, a total of eight publications,11–15,18–20 with 1612 patients with lung cancer and 1442 cancer-free control subjects, were included in this research.

The flowchart of literature selection.
Characteristics of included studies.
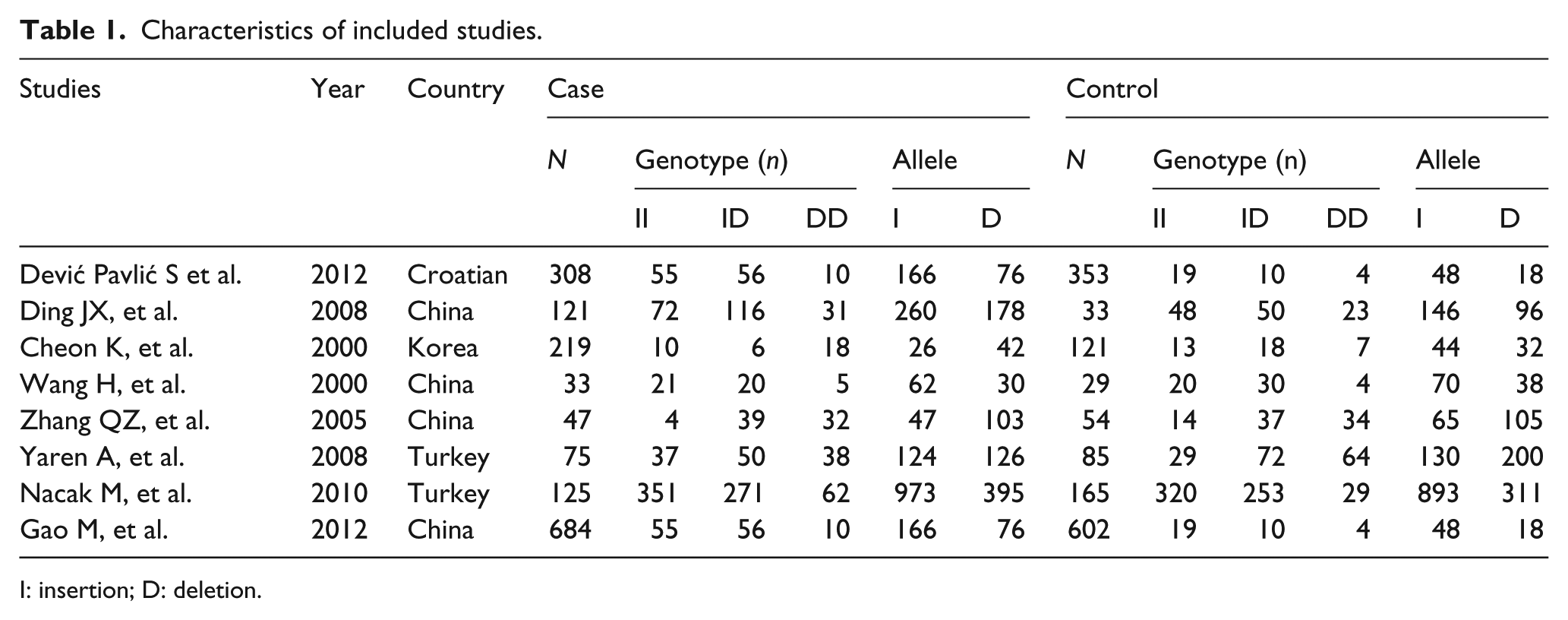
I: insertion; D: deletion.
Quantitative synthesis
The result of meta-analysis of the association between lung cancer and the ACE gene polymorphism in eight case-control studies is shown in Figures 2 and 3. The heterogeneity test of the various studies did not reveal heterogeneous results (DD vs. (ID+II): I2 = 0%, p = 0.79; D allele vs. I allele: I2 = 0%, p = 0.97); therefore, we used the fixed-effects model in the analysis. No significant association between the ACE I/D polymorphism and susceptibility to lung cancer was identified in any of the genetic models (DD vs. (ID+II): OR = 0.96, 95% CI (0.80–1.14), p = 0. 61; D allele vs. I allele: OR = 1.01, 95% CI (0.91–1.13), p = 0.79).

Forest plot of lung cancer risk associated with the angiotensin-converting enzyme insertion/deletion (ACE I/D) polymorphism (DD vs. ID+II). The squares and horizontal lines correspond to the study-specific odds ratio (OR) and 95% confidence interval (CI), respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95% CI. In this analysis, a random-effects model was used.

Forest plot of lung cancer risk associated with angiotensin-converting enzyme insertion/deletion (ACE I/D) polymorphism (D allele vs. I allele). The squares and horizontal lines correspond to the study-specific odds ratio (OR) and 95% confidence interval (CI), respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of OR and 95% CI. In this analysis, a random-effects model was used.
Publication bias analysis
We utilized RevMan 5.2 software to analyze the publication bias; the funnel plot (Figure 4) shows that the points are evenly distributed and symmetrical, and most of the points are within the 95% CI. In addition, the shape of the funnel plots showed no obvious asymmetry and the result of Egger’s test did not show statistical evidence for bias. It indicates that there is no publication bias, and the result of the study is credible.

Begg’s funnel plot for publication bias test. Each circle denotes an independent study for the indicated association. Log(OR), natural logarithm of odds ratio (OR). The horizontal line represents mean effect size.
Sensitivity analysis
We deleted one single study from the overall pooled analysis each time to check the influence of the removed data set to the overall ORs. The pooled ORs and 95% CIs were not significantly altered when any part of the study was omitted, which indicated that any single study had little impact on the overall ORs.
Discussion
In the present study, we performed a meta-analysis to evaluate the association between the ACE gene I/D polymorphism and lung cancer. We did not find any such association.
The lungs have an important role in the synthesis of ACE, and evidence is increasing that ACE activity may have some prognostic value in lung cancer patients. 21 Because the gene-encoding ACE is highly polymorphic and lung cancer is a complex syndrome caused by ill-defined genetic factors, it is interesting to determine which genetic variants of the ACE gene have the functional potential to affect the bioavailability of ACE, and thus, the development of lung cancer. Previous reports indicated that plasma ACE levels were partly regulated by I/D polymorphism in intron-16, with DD homozygotes having roughly twice the ACE levels of II homozygotes. 22 In recent years, more and more publications suggested that the ACE I/D polymorphism is related to lung cancer risk.11–15,18–20 Cheon et al. 11 were the first to report the association of the ACE I/D polymorphism with lung cancer. From then on, there have been many papers published.12–15,18–20 However, these publications used a small number of samples, and thus, the results may reflect chance observations rather than true associations.
The present study, which included eight independent case-control studies, has shown that the ACE gene I/D polymorphism was not associated with the susceptibility to lung cancer. However, there is still a need for further research and screening of etiological relations between the functional polymorphism loci of the ACE gene and the susceptibility to lung cancer.
In addition, there were several limitations in the present study. First, we included publications that reported only on the ACE gene I/D polymorphism and lung cancer. Second, we did not divided lung cancer patients into small-cell lung cancer and non-small-cell lung cancer. Finally, we did not investigate the interaction between genetic polymorphism and environmental factors in the present study.
In conclusion, the present study suggested that there is no association between the ACE gene I/D polymorphism and lung cancer.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.