
Abstract
Introduction:
Angiotensin-converting enzyme (ACE) and ACE2 are key regulators of the renin–angiotensin system, which has been shown to participate in a series of cardiovascular diseases. We hypothesized that dysregulated gene expression of ACE and ACE2 contribute to the formation of thoracic aortic dissection and aneurysm.
Materials and methods:
We assessed ACE plasma concentration in 73 patients with acute thoracic aortic dissection (n=34), aneurysm (n=18), coronary heart disease (n=21) and 13 healthy volunteers. ACE and ACE2 gene expression in available aortic tissues was also examined by using quantitative real-time polymerase chain reaction.
Results:
In patients with acute aortic dissection, ACE plasma concentration and its mRNA level in aortic tissue were markedly reduced compared with those in patients with aneurysm, coronary heart disease and healthy controls. The level of ACE2 gene expression in dissection samples was also significantly lower than that in aneurysm (8.01±7.44, p<0.01) and coronary heart disease groups (9.61±11.54, p<0.01). A strong correlation was observed between the gene expressions of ACE and those of ACE2, and ACE to ACE2 ratio was significantly elevated in dissection tissues.
Conclusions:
Imbalanced down-regulation of ACE and ACE2 mRNA expression levels may play an important role in the development and progression of thoracic aortic aneurysmal dilatation and subsequently dissection.
Keywords
Introduction
Thoracic aortic dissection (TAD) and aneurysm (TAA) are severe cardiovascular diseases and may lead to devastating events without early diagnosis and appropriate management. 1 These diseases are characterized by infiltration of inflammatory cells, depletion of vascular smooth muscle cells (VSMCs) and degradation of the extracellular matrix (ECM) within the aortic wall.1,2 Several risk factors such as smoking, hypertension, atherosclerosis and diabetes that induce these histopathological changes may predispose to the progression of aneurysmal dilatation and dissection.1–3 Furthermore, a proportion of TAD cases are closely related to inherited diseases such as bicuspid aortic valve, Marfan syndrome and Loeys–Dietz syndrome;1,2,4 however, genetic propensity associated with non-syndromic TAD and TAA remains largely unknown.
The renin–angiotensin system (RAS) has been recognized to be highly involved in disturbances in a series of cardiovascular diseases.2,5 As a key regulator in the RAS, angiotensin-converting enzyme (ACE) has considerable impact on vascular function and remodeling. It catalyzes the conversion of angiotensin (Ang) I to Ang II, a major effector of the RAS. Ang II can affect the arterial wall through modulation of the function of numerous adhesion molecules, cytokines and growth factors that may be responsible for inflammation, hypertrophy, ECM degradation and proliferation and apoptosis of dysregulated VSMCs.2,6,7 Recently, a homolog of ACE, namely ACE2, has emerged as an important player in the pathophysiology of vascular diseases due to its protective role in metabolizing pro-inflammatory, pro-proliferative and pro-hypertensive Ang I and Ang II into favorable Ang-(1-9) and Ang-(1-7), respectively.7,8
Despite a growing body of evidence on the importance of ACE family in the pathogenesis of arterial diseases, their involvement and functional roles in the setting of aortic aneurysmal dilatation and dissection are still unclear. Therefore, the present study was designed to assess the plasma ACE levels and the mRNA expression of ACE and ACE2 in aortic samples obtained from surgical patients with TAD and TAA, and to determine whether these proteinases contribute to the progression of aortic diseases.
Materials and methods
Patient enrollment and tissue collection
Between March 2011 and October 2012, a total of 86 patients’ blood specimens were collected and were divided into four groups according to the etiology of the vascular diseases: acute TAD group (n=34), TAA group (n=18), coronary heart disease (CHD) group (n=21) and control group (n=13) (Table 1). Blood specimens in control group were collected from healthy volunteers with any of the following: metabolic diseases, severe systemic diseases including malignancy, a first-degree relative with TAD or TAA, hypertension, and any other documented cardiovascular disorders. None of the TAD and TAA was caused by trauma, surgery, infection, aortitis and heritable connective tissue diseases. All patients had no history of medical treatment with ACE inhibitors or angiotensin receptor blockers. This study was approved by the Ethical Review Board of West China Hospital (No. 20101206) in compliance with the Declaration of Helsinki, and all patients gave written informed consent.
Patient characteristics.

CHD: coronary heart disease; NA: not applicable; TAD: thoracic aortic dissection; TAA: thoracic aortic aneurysm.
In acute TAD cases, samples were obtained from the outer wall of the false lumen; the mean interval between the onset of dissection and open surgery was 6.8±3.6 days. During aneurysm repair, samples of the anterior-lateral aortic wall were excised from the site of maximal aortic dilatation. In patients from the CHD group, samples were collected from aortotomy tissues excised by the aortic wall punch before suturing the proximal end of the graft to the aorta. Each fresh tissue sample was snap-frozen in liquid nitrogen and stored at -80°C.
Plasma ACE assessment
All blood specimens were taken after 12-hour fasting. The samples were centrifuged for 10 minutes at 3000 rpm within 15 minutes of sampling and stored at -80°C until assay. Plasma ACE analysis was made from freshly thawed samples via a spectrophotometric procedure (Roch P800 automatic biochemical analyzer).
Quantitative real-time polymerase chain reaction
Total RNA was extracted from aortic tissues (while on ice) with Trizol (Invitrogen, Carlsbad, CA) according to manufacturer’s protocol. The mRNA from each tissue sample was reverse-transcribed with an iScript™ cDNA Synthesis Kit (BioRad, Hercules, CA), and quantitative real-time polymerase chain reaction was performed with the iCycler IQ Real-Time PCR Detection System (BioRad, Hercules, CA). The primers used were as follows: ACE forward 5′ - T G G T G A C T G A T G A G G C T G A G - 3′ and reverse 5′ - T C T T G C T G G T C T C T G T G G T G - 3′, ACE2 forward 5′ - C A T T G G A G C A A G T G T T G G A T C T T - 3′, reverse 5′ - G A G C T A A T G C A T G C C A T T C T C A - 3′, β-actin forward 5′ - A C T A T C G G C A A T G A G C G G T T C - 3′, reverse 5′ - A T G C C A C A G G A T T C C A T A C C C - 3′. Levels of mRNA were acquired by normalizing the threshold cycle to that of 18S. The relative levels of mRNA were normalized with the mRNA level of an internal reference sample.
Statistical analysis
Continuous variables are presented as the mean ± standard deviation and categorical data as percentages unless otherwise specified. Differences between groups were analyzed by Chi-square, Fisher’s exact or other nonparametric tests as appropriate. Statistical significance was determined by χ2 or one-way analysis of variance followed by Bonferroni tests when more than two groups were compared. Since the distribution of the ACE and ACE2 mRNA levels was deviated (kurtosis=7.53, skewness=2.80, Kolmogorov–Smirnov test z=0.33, p<0.001), Spearman’s correlation was used to evaluate the relationship between variables. A two-tailed p-value less than 0.05 was considered statistically significant.
Results
Aortic tissues from 12 patients with acute TAD, 16 aneurysm patients and 16 CHD patients undergoing open surgery were available for mRNA analysis. Demographic characteristics are summarized in Table 1. Apart from the aortic diameter at sample site, no significant differences between groups were observed.
Plasma ACE concentrations were significantly lower in patients with acute TAD compared with those in patients with TAA, CHD and healthy controls (17.90±7.88 vs. 25.26±9.05*, 33.51±8.11#, 38.39±4.75# IU/l, *p<0.01, #p<0.001, respectively). Moreover, significantly reduced ACE values were also observed in TAA patients compared with those in CHD patients and healthy controls (Figure 1).
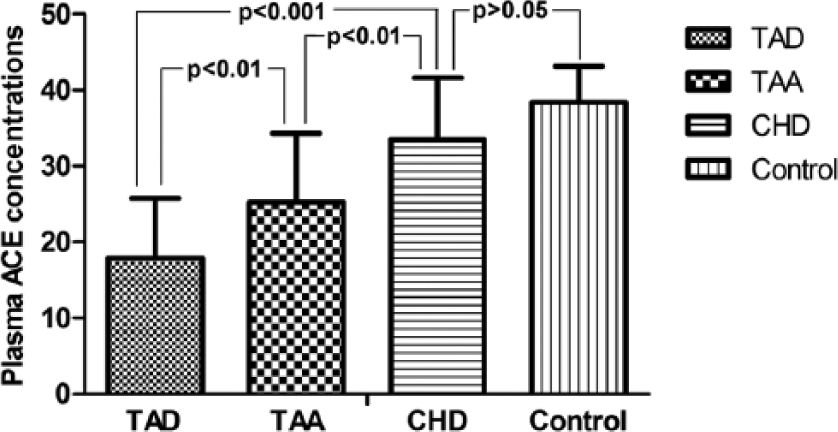
Comparison of plasma ACE concentrations among patients with acute thoracic aortic dissection (TAD) (n=34), thoracic aortic aneurysm (TAA) (n=18), coronary heart disease (CHD) (n=21) and heathy controls (n=13).
Strongly correlated with its plasma concentrations (r=0.643, p=0.003), ACE mRNA levels were remarkably reduced in TAD tissues compared with those in samples from patients with TAA and CHD (0.23±0.39 vs. 0.99±0.96*, 7.09±7.69 *p<0.05, respectively). ACE mRNA expression in TAA tissue was also significantly lower than that in aortic tissues from CHD patients (Figure 2(a)). Similarly, the expression level of ACE2 mRNA in aortic tissues was the lowest among the three groups (0.77±0.86 vs. 8.01±7.44*, 9.61±11.54#, *p<0.01, #p<0.05, respectively); however, no significant difference in ACE2 mRNA levels in aortic tissues between TAA and CHD patients was observed (Figure 2(b)). A significant correlation between ACE and ACE2 gene expressions (r=0.759, p<0.001) was observed (Figure 3). Moreover, it is noted that the ACE to ACE2 gene expression ratio in aortic tissue was significantly higher in subjects with TAD than subjects with TAA (p=0.025). No significant relationship was observed between the ACE to ACE2 ratio and other clinical variables (Table 2).

Quantitative real-time polymerase chain reaction analysis of ACE

Relationship between ACE and ACE2 mRNA levels in aortic tissues (r=0.759, p<0.001).
Clinical variables and the aortic ACE to ACE2 gene expression ratio.

NS: not significant; TAD: thoracic aortic dissection; TAA: thoracic aortic aneurysm; SD: standard error.
Discussion
The present study revealed a significant down-regulation of ACE and ACE2 mRNA levels within the aortic wall from patients with acute TAD. Moreover, the ACE to ACE2 gene expression ratio was remarkably higher in aortic tissues collected from patients with TAD compared with those in TAA tissues. In addition, we demonstrated that the plasma ACE concentrations were significantly reduced in patients with dissections and aneurysms, and correlated well with its mRNA levels in aortic tissues. Our findings might suggest an important role of imbalanced down-regulation of ACE and ACE2 gene expression in the progression of aortic aneurysmal dilatation and dissection.
Several clinical and experimental studies have suggested that dysregulated expression of ACE may contribute to the development of vascular disease.2,5 This enzyme is highly expressed in the vasculature and mainly catalyzes the conversion of angiotensin I to Ang II, which acts as a strong vasoconstrictor through angiotensin II receptor 1 (ATR1) and is involved in VSMCs’ proliferation, ECM degradation, excessive production of reactive oxygen species and subsequent inflammatory cascades. Such an increase of Ang II level was shown to promote aneurysm and dissection formation in apolipoproteins E-deficient (ApoE-/-) mice.9,10 However, recent studies have also demonstrated that Ang II may also activate the angiotensin II receptor 2 (ATR2), resulting in vasodilation, anti-proliferative and anti-inflammatory actions, antagonizing the ATR1-mediated effects.11–13 In the present study, we observed a significant reduction of plasma ACE concentrations and its mRNA level in aortic tissues from TAD patients compared with those in TAA patients. Given the evidence that Ang II may have a role in inducing or attenuating dissection formation, our findings indicate a close relationship between the down-regulation of ACE levels and the formation of aortic aneurysm and dissection, and we speculate that ACE and its downstream effector Ang II may have varied effects via different signaling pathways during the TAA and TAD-related disease process.
One of the key novel results from the present study is that ACE2 mRNA expression is significantly reduced in human TAD tissues compared with those in aortic samples from TAA and CHD patients. This finding sits well with the growing evidence that ACE2 plays a protective role in cardiovascular diseases. Indeed, previous studies have identified ACE2 as a negative regulator of the RAS by converting Ang II into Ang-(1-7), which, by acting via its own receptor Mas, can inhibit platelet adhesion and thrombosis formation, suppress inflammation, stabilize atherosclerotic plaques, promote myocardial remodeling and lower blood pressure.8,14–16 More recently, Ohshima et al. found that elevated Ang-(1-7) expression could in turn up-regulate the mRNA levels of ACE2 and ATR2 in the injured artery. 17 Their results suggested novel interactions between ACE2-Ang-(1-7)-Mas axis and ACE-Ang II-ATR2 axis in vascular remodeling and further revealed the multiple functions of ACE2 in protecting against the development and progression of vascular diseases.
Although ACE and ACE2 have opposite effects on the generation of Ang II, a significant positive correlation between ACE and ACE2 gene expressions was detected in our study. With regard to current evidence, it is very likely that the expression of ACE and ACE2 genes is regulated in a balanced manner, or synergistically, which might be mediated by the local Ang II concentration or via other interrelated mechanisms.11,17,18 Despite a downward trend of the ACE and ACE2 gene expressions in aortic tissue in patients with TAD compared with those in TAA ones, we found a significantly higher ACE to ACE2 ratio in TAD tissues, implicating a more prominent reduction of ACE2 level in TAD patients. On the one hand, decreased ACE mRNA level and subsequently weakened vasoconstriction effects mediated by the ACE-Ang II-ATR1 axis may implicate the fact that down-regulation of ACE gene expression also has a role in promoting aortic aneurysmal dilatation. On the other hand, this finding further confirms a more important role of ACE2 in protecting against vascular aneurysmal diseases. Thus our results indicated that an imbalanced down-regulation of the ACE and ACE2 gene expression may contribute to the development and progression of TAD and TAA.
There are several limitations in the current work. First, because of the absence of serial tissue samples spanning the period of disease progression, it is difficult for us to fully elucidate the dynamic changes of ACE and ACE2 expression and their functional roles in the initiation and formation of TAA and TAD. In addition, although decreased ACE and ACE2 mRNA levels were associated with aortic pathological changes, the crosstalk between the ACE-Ang II- AT1/AT2 receptor axis and the ACE2–Ang-(1-7)–Mas axis at different stages of aortic diseases is unknown. Furthermore, the present study is based on in vitro analysis of human aortic tissues with a modest sample size. Therefore, we cannot exclude the possibility that the duration and status of aortic pathological changes, as well as other oral anti-hypertensive and vasoactive drugs may affect ACE and ACE2 expressions.
In summary, our study demonstrates a marked decrease of ACE plasma concentration and ACE and ACE2 gene expression in aortic samples from TAD patients, and a significantly higher ACE to ACE2 ratio was observed in TAD tissues compared with those in TAA samples. These findings have provided new evidence that may help to understand RAS-related mechanisms in the pathogenesis of aortic disease. Additional studies are required to determine the role of imbalanced ACE and ACE2 expression in the formation of TAA and TAD and whether maintaining the balanced status of these proteinases represent a potential therapeutic strategy for the treatment of aortic disease.
Footnotes
Acknowledgements
We gratefully acknowledge the Cardiovascular Research Institute of Sichuan University West China Hospital for providing the experimental facilities and Bengui Zhang for assistance with data analysis.
Conflict of interest
None declared.
Funding
This study was supported by the support projects of the Science and Technology Office in Sichuan Province (No. 2010FZ0025) and National Natural Science Foundation of China (No.81300155, 81370413,81470481 and 81170288).