
Abstract
Introduction:
We aimed to determine the association between plasma aldosterone and renin levels as well as their ratios with carotid plaques in patients with coronary artery disease (CAD).
Materials and methods:
Carotid intima-media thickness (IMT) and plaque score were evaluated in 111 patients with stable CAD. Plasma renin and aldosterone levels were measured in all patients. Aldosterone to renin ratio (ARR) was calculated. All patients were categorized into: Group 1 (normal coronary angiography), Group 2 (patients had CAD but without carotid plaque) and Group 3 (patients had CAD and at least one carotid plaque).
Results:
Renin levels are significantly higher in Group 3 than in Group 1 and 2. ARR was significantly lower in Group 3 than in Group 1 and 2. Renin levels were found to be positively correlated with carotid IMT and plaque score but ARR was inversely associated with carotid IMT and plaque score. Renin levels and ARR are independently associated with presence of carotid plaque in CAD patients (OR 1.124, CI 1.021–1.237, p = 0.017 and OR 0.906, CI 0.839–0.978, p = 0.011, adjusted for age, respectively).
Conclusions:
Plasma renin and ARR but not aldosterone are independently associated with presence of carotid plaques in CAD patients. Hence, the linkage between aldosterone and renin plays a more important role than aldosterone alone in carotid atherosclerosis.
Introduction
Carotid atherosclerosis is highly associated with the severity of coronary artery disease (CAD) and is strongly associated with future myocardial infarction.1,2 A close association between carotid atherosclerosis and the extent of CAD has been well established.3,4 CAD is the leading cause of mortality following ischemic stroke. 5 Among several factors that lead to the formation of atherosclerosis, renin-angiotensin-aldosterone system (RAAS) has well-established roles in atherogenesis. 6 Activated RAAS is associated with an increased risk of coronary and cerebrovascular events independent of blood pressure levels.7,8 The most well-known enzymes participating in the RAAS are renin and angiotensinogen-converting enzyme. Plasma renin concentration is associated with long-term cardiovascular mortality in patients referred to coronary angiography. 9 Aldosterone can exert proinflammatory effects via mineralocorticoid receptor-dependent and -independent pathways. There is an important role for aldosterone and mineralocorticoid receptor activation in the induction of oxidative stress and inflammation leading to endothelial dysfunction and vascular remodeling during activation of RAAS. 10 Aldosterone is considered a key player in cellular processes underlying vascular hypertrophy and fibrosis. 11 Plasma aldosterone was an independent predictor of carotid plaque progression in patients with cardiovascular risks. 12 In patients with stable CAD, plasma aldosterone levels are independently associated with the risk of major vascular events and vascular mortality and with atherosclerotic burden. 13 There was an inverse relationship between plasma renin activity and carotid intima-media thickness (IMT) and severity of carotid artery lesions in patients with mild-to-moderate hypertension. 14 However, high plasma aldosterone or aldosterone-to-renin ratio (ARR) were found to be associated with impaired flow-mediated dilation and progression of subclinical atherosclerosis in young to middle-aged individuals. 15
Hence, the association between RAAS and carotid atherosclerosis and the evidence linking the RAAS with central and cerebral vascular atherosclerosis remains controversial. Therefore, we investigated the relationships of plasma aldosterone and renin levels and ARR with carotid IMT and plaque score in patients with angiographically proven CAD.
Materials and methods
Study population
A total of 111 patients with stable angina pectoris undergoing coronary angiography were enrolled in this study. The medical ethics committee of Kaohsiung Municipal Min-Sheng Hospital approved the study, and written informed consent was obtained from all participants. Smoking status was classified as non-smoking, ex-smoker (ceased smoking for at least one year) or current smoker. Patients with Conn’s disease, Addison’s disease, cirrhosis of the liver or undergoing hormone replacement therapy were excluded from the study. Clinical blood pressure was measured before duplex ultrasound examination with a standard mercury sphygmomanometer. The measurement of blood pressure followed the guidelines outlined by the American Heart Association Council on High Blood Pressure Research. 16 The diagnosis of hypertension was based on multiple measurements on separate occasions over a period of time. The patients were seated with their back supported and both feet lying flat on the floor for at least five minutes in a quiet room, with an empty bladder. At least two measurements of blood pressure were taken each time, separated by at least one minute. Blood pressure was measured by a mercury sphygmomanometer. Body mass index (BMI) was calculated as weight (in kilograms) divided by height (in meters) squared. We also measured serum levels of urea nitrogen, sodium, potassium, creatinine, glucose, total cholesterol, triglycerides, high-sensitivity C-reactive protein (hs-CRP), supine plasma renin and aldosterone levels.
Measurements of carotid IMT and plaque score
Duplex ultrasonography of the left and right common carotid arteries (CCAs) was performed with a 7.5-MHz linear array transducer on a SONOS 5500 ultrasound system (Hewlett-Packard, Andover, MA, USA). All ultrasound measurements were made by two experienced vascular technologists and images were recorded on digital video discs for further analyses using previously described methods.17,18 The distance between the lumen-intima interface and the media-adventitia interface of the near and far walls of distal CCAs and bifurcations were measured. Carotid IMT was measured at eight points of each CCA and bifurcation and the mean value of all measurements of both left and right carotid arteries was calculated. Thickened carotid IMT was defined as the mean value > 0.9 mm. Carotid plaque is defined as the presence of focal wall thickening that is at least 50% greater than that of the surrounding vessel wall or as a focal region with carotid IMT greater than 1.5 mm that protrudes into the lumen that is distinct from the adjacent boundary. 19 Total carotid plaque score was defined as the sum of the presence of plaques at the near and far walls of bilateral sides at three locations (CCA, carotid bifurcation and internal carotid artery).
Coronary angiographic evaluation
Coronary angiography was performed by the Judkin’s method. Two different scores were used to evaluate the angiographic severity and extension of CAD: the number of stenosed (>50% reduction of luminal diameter) or occluded vessels (one- to three-vessel disease), and the complexity and severity scoring method according to the SYNTAX score. 20 Scoring of all coronary angiograms was performed visually by a single experienced observer who was blinded to clinical and laboratory data. The intraclass correlation coefficient for intra-rater reliability was 1.0 (one- to three-vessel disease score), and 0.93 (tertiles of the SYNTAX score).
Measurements of plasma renin and aldosterone levels
Venous blood was drawn (typically between 8 a.m. and 9 a.m.) from each participant after he or she had been in a supine position for five to 10 minutes. Plasma renin and aldosterone concentrations were measured using radioimmunoassay according to current guidelines in plasma samples obtained with patients in the supine position, as previously described. 21 The coated tube radioimmunoassay kits for in vitro diagnostic use were manufactured by Diagnostic System Laboratories Inc (Webster, TX, USA) and OBI-DSL (Cherwell Innovation Centre, Upper Heyford, Oxfordshire, UK) and used a highly specific rabbit antialdosterone and antirenin polyclonal antibody. Cross-reactivity to closely related naturally occurring steroids is negligible. For aldosterone, the normal range was 35–300 pg/ml supine. For renin, the normal range was 3.6–20 pg/ml supine. Plasma ARR was calculated as aldosterone in pg/ml divided by renin in pg/ml.
Statistical analysis
Results are expressed as mean±SD, or as a percentage, when appropriate. We used the Kolmogorov-Smirnov test to evaluate normal distribution. Differences between groups were assessed either by the two-tailed Mann-Whitney test or by the Kruskal-Wallis test. In the univariate analysis, unadjusted means were compared by one-way analysis of variance (ANOVA). To analyze the relationship between variables and carotid IMT and plaque score, univariate linear regression analysis was used. Correlations between variables were analyzed by Spearman’s correlation coefficient by rank. To predict the presence of CAD patients with carotid plaque or thickened IMT, logistic regression analysis (forced entry methods) was used. Receiver-operating characteristic (ROC) curves were constructed to assess the best values of aldosterone, renin and ARR, optimizing sensitivity for the identification of the presence of CAD patients with or without carotid plaque or thickened IMT. The area under the ROC curve and 95% confidence intervals (CI) were used to assess the predictive power for the presence or absence of CAD patients with carotid plaque or thickened IMT. A two-sided probability value of p < 0.05 was considered to be statistically significant. Statistical analysis was performed with SPSS software (version Windows 18.0, SPSS Inc, Chicago, IL, USA).
Results
Patient characteristics
Among all enrolled patients, 30 patients (27%, Group 1) had normal coronary angiography, 32 (29%, Group 2) had CAD but without carotid plaque and 49 (44%, Group 3) had CAD and at least one carotid plaque (Table 1). The prevalence of diabetes mellitus, hypertension and smoking status was not different among these three groups. The mean age of Group 3 was older than Group 1 and 2 (p = 0.013). Serum creatinine was significantly higher in Group 3 than in Group 1 and 2 (p = 0.001). Group 3 also had a thicker carotid IMT than that of Group 1 and 2 (p = 0.001). The mean SYNTAX score in Group 3 was significantly higher than in Group 1 and 2 (p < 0.001). Medications were not significantly different except the usage of clopidogrel was more prevalent in Group 3 patients. All subjects had plasma aldosterone levels within the normal range, except for one patient with aldosterone slightly above the upper limit of the normal range. Nevertheless, plasma aldosterone levels were higher in Group 3 (Group 3 vs. Group 1, 100.5±57.4 vs. 81.0±21.2 pg/ml, p = 0.154 and Group 3 vs. Group 2, 100.5±57.4 vs. 87.7±32.8 pg/ml, p = 0.288) but without statistical significance (Figure 1). However, plasma renin levels were significantly different among the three groups and were highest in Group 3 (Group 3 vs. Group 1, 24.5±27.7 vs. 9.2±6.9 pg/ml, p = 0.020 and Group 3 vs. Group 2, 24.5±27.7 pg/ml vs. 10.1±10.3 pg/ml, p = 0.011). In addition, the mean value of ARR was significantly lower in Group 3 than those in Groups 1 and 2 (Group 3 vs. Group 1, 8.4±7.5 vs. 13.7±10.0 pg/ml, p = 0.019 and Group 3 vs. Group 2, 8.4±7.5 pg/ml vs. 18.0±17.1 pg/ml, p = 0.001). Serum potassium and sodium levels were not significantly different among the three groups (Table 1).
Clinical characteristics and biochemical parameters of all enrolled patients.

Results are expressed as mean ± SD. CAD: coronary artery disease; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; LDL: low density lipoprotein; HDL: high density lipoprotein; hs-CRP: high-sensitivity C-reactive protein; ARR: aldosterone to renin ratio; IMT: intima-media thickness; LVEF: left ventricular ejection fraction.
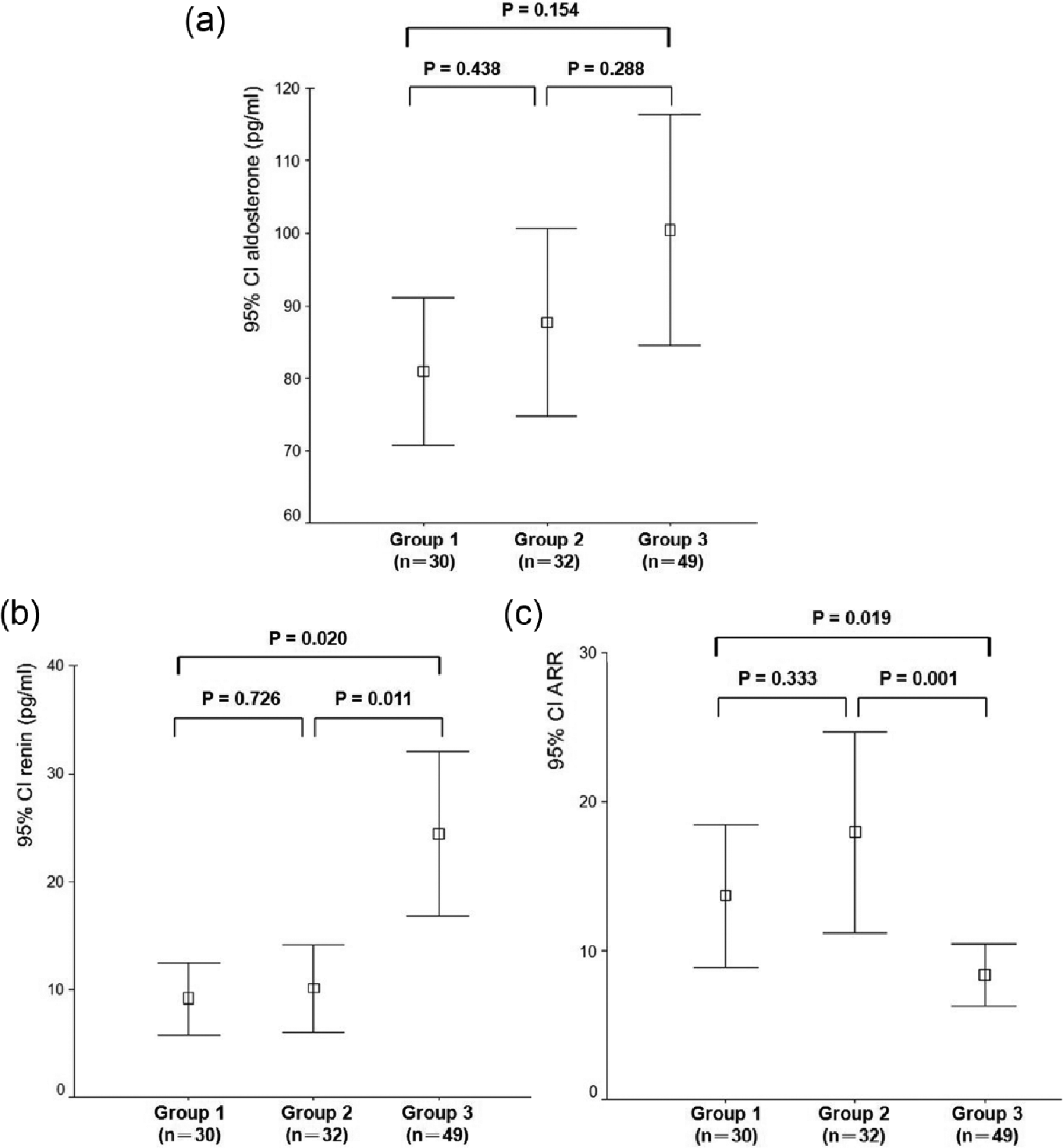
The differences of plasma aldosterone (a) and renin (b) levels and aldosterone to renin ratio (ARR) (c) between patients with normal coronary angiography (Group 1), with coronary artery disease (CAD) but without carotid plaque (Group 2) and with CAD and carotid plaques (Group 3) are illustrated. CI: confidence interval.
Factors affecting carotid IMT and plaque score
Univariate analysis of clinical and biochemical factors affecting carotid IMT and carotid plaque score is shown in Table 2. Age, serum creatinine, plasma renin level, SYNTAX score and plaque score were found to be positively correlated with carotid IMT. Age, serum creatinine, hs-CRP, plasma renin level and SYNTAX score were also found to be positively correlated with carotid plaque score. However, ARR was inversely associated with carotid IMT and plaque score (Table 2).
Univariate analysis of clinical and biochemical factors affecting carotid intima-media thickness and plaque score in all CAD patients.
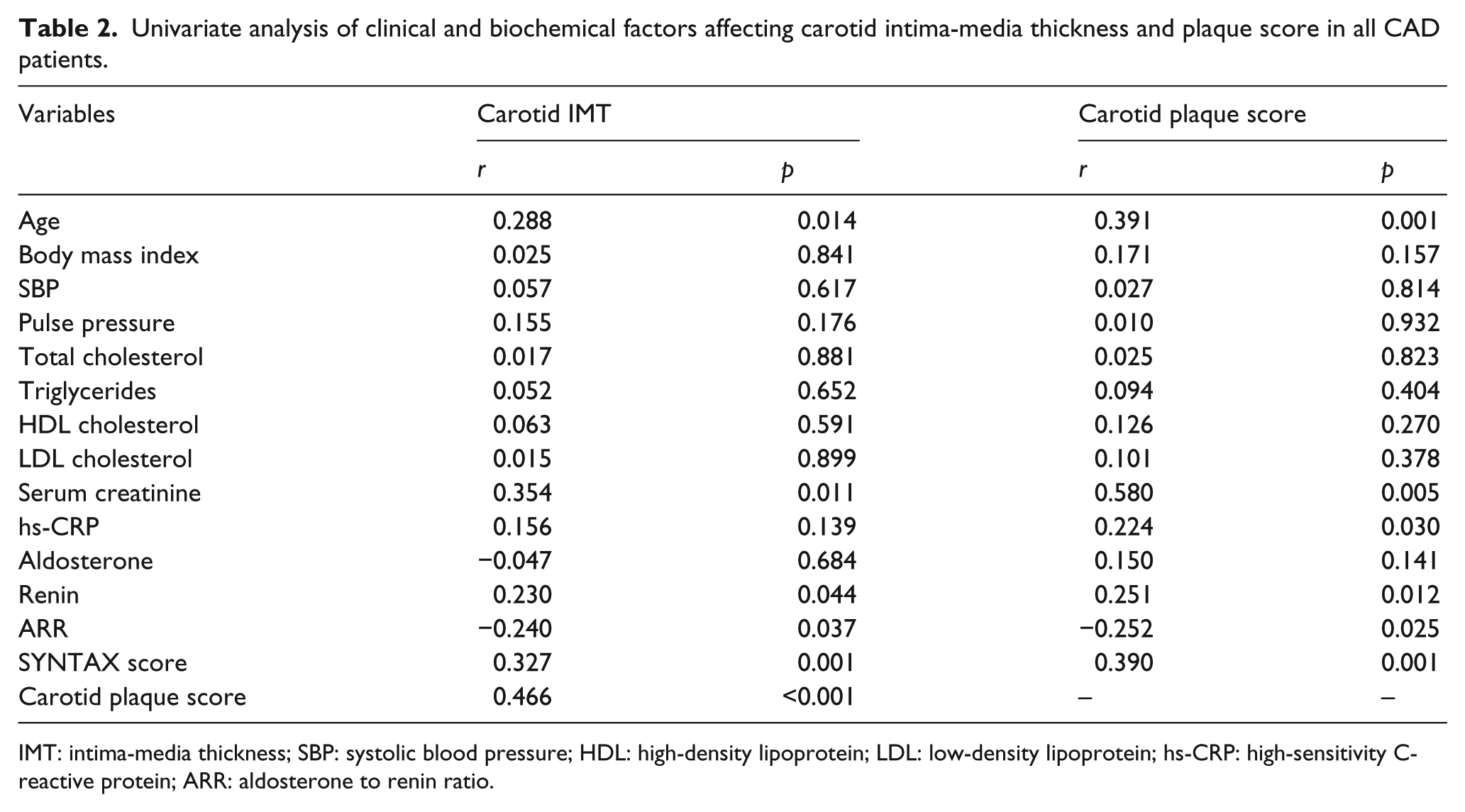
IMT: intima-media thickness; SBP: systolic blood pressure; HDL: high-density lipoprotein; LDL: low-density lipoprotein; hs-CRP: high-sensitivity C-reactive protein; ARR: aldosterone to renin ratio.
Predictors of CAD patients with carotid plaques and thickened carotid IMT
As shown in Table 3, the unadjusted and adjusted odds ratios associated with the plasma renin levels for prediction of CAD patients with carotid plaques were 1.132 and 1.124 (p = 0.015 and 0.017, respectively). The unadjusted and adjusted odds ratios associated with the ARR for prediction of CAD patients with carotid plaques were 0.906 and 0.906 (p = 0.010 and 0.011, respectively). As shown in Table 4, the odds ratios associated with the plasma renin levels and ARR for prediction of CAD patients with thickened carotid IMT were insignificant. However, hs-CRP was a significant predictor of thickened carotid IMT after adjustment for age (odds ratio 5.441, 95% CI 1.052–28.131, p = 0.043). The areas under the ROC curves for the plasma aldosterone and renin to predict the CAD patients with carotid plaques were 0.636 and 0.738, respectively (Figure 2(a)). The area under the ROC curve for the plasma ARR to predict CAD patients without carotid plaque was 0.679 (Figure 2(b)). These results indicated that decrease in ARR was associated with higher carotid plaque score in patients with CAD. When we set the cutoff value to predict the presence of CAD patients with carotid plaques to a plasma renin level of 8.5 pg/ml, the sensitivity and specificity were 68.8% and 62.5%, respectively. In contrast, when we set the cutoff value to predict the presence of CAD patients without carotid plaque to a plasma ARR of 8.0, the sensitivity and specificity were 68.8% and 61.7%, respectively.
Predictors of CAD patients with carotid plaques.

Adjusted for age. CAD: coronary artery disease; IMT: intima-media thickness; HDL: high-density lipoprotein; LDL: low-density lipoprotein; hs-CRP: high-sensitivity C-reactive protein; ARR: aldosterone to renin ratio; CI: confidence interval.
Predictors of CAD patients with thickened carotid IMT.
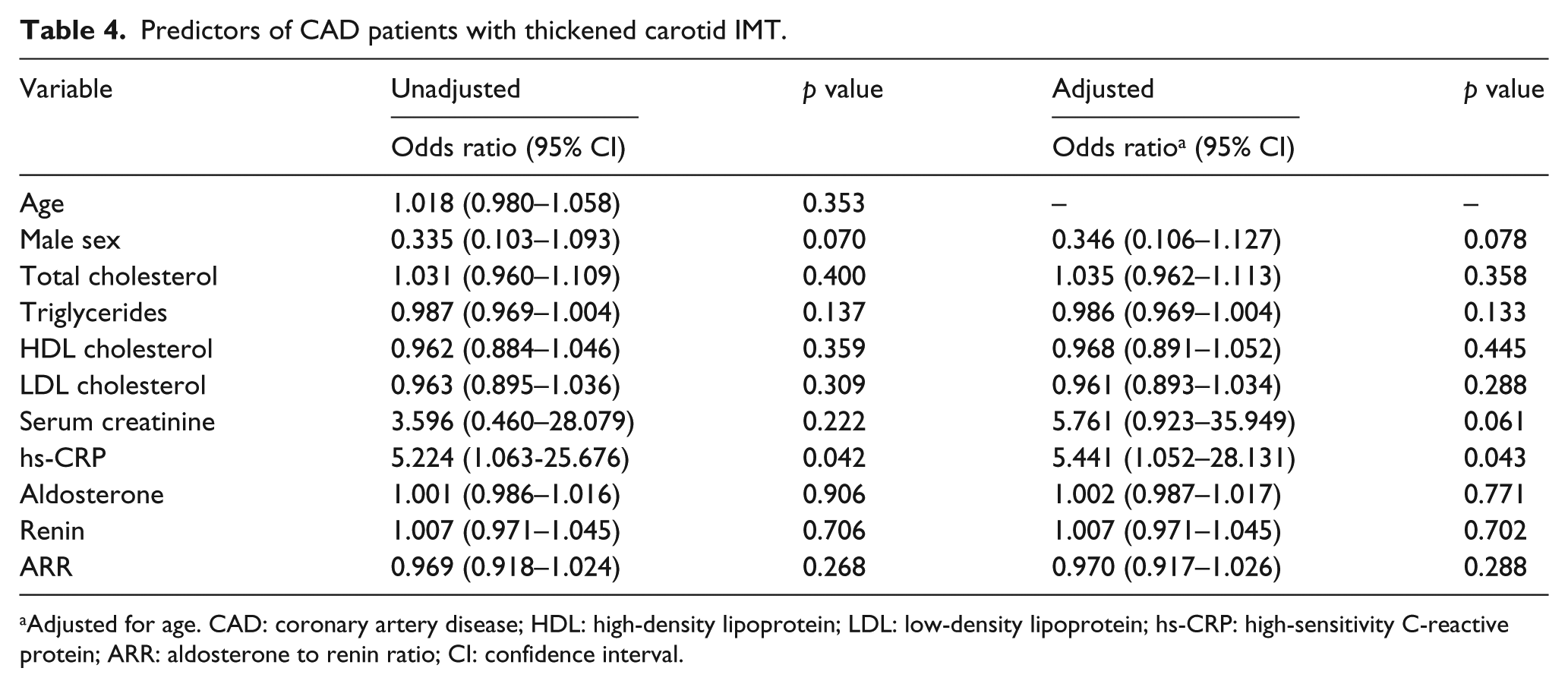
Adjusted for age. CAD: coronary artery disease; HDL: high-density lipoprotein; LDL: low-density lipoprotein; hs-CRP: high-sensitivity C-reactive protein; ARR: aldosterone to renin ratio; CI: confidence interval.

The receiver-operating characteristic (ROC) curve for the plasma aldosterone and renin levels to identify patients with coronary artery disease and carotid plaques (a) and the ROC curve for the plasma aldosterone to renin ratio (ARR) to identify patients with coronary artery disease but without carotid plaque (b). AUC: area under the ROC curve; CI: confidence interval.
Discussion
In this cross-sectional study, we examined the relationship between RAAS and carotid atherosclerosis in stable CAD patients. Our results demonstrated that plasma renin levels and ARR are independently associated with presence of carotid plaques. In addition, hs-CRP is independently associated with carotid IMT in CAD patients. These results indicated that plasma renin may have important effects on the formation of carotid atherosclerosis in CAD patients, and plasma renin suppressed by aldosterone (higher ARR) might be a relevant anti-atherogenic indicator in these patients. This study also disclosed that detection of carotid plaques is not infrequent in aged patients with stable CAD. Carotid plaques were present in 60% of CAD patients. These patients had significantly higher hs-CRP and thicker carotid IMT than the remaining patients with CAD. In these patients with carotid plaques, plasma renin levels were in a normal/high-normal range and aldosterone levels were in a high-normal range, suggesting that inflammation and renin escape from suppression by aldosterone excess caused carotid vascular damage and plaque formation in CAD patients.
Although animal studies indicated that aldosterone might cause important vascular inflammation and damage,22,23 the clinical evidence supporting a direct role of aldosterone as a potential contributor to vascular dysfunction or cardiovascular events is still limited. A simple model to assess possible detrimental effects of aldosterone on the vasculature is primary aldosteronism in which patients experienced more cardiovascular events than did patients with essential hypertension. 24 Patients with primary aldosteronism also have increased common carotid IMT compared to the patients with essential hypertension. 25 It is well known that aldosterone has direct effects on the vasculature and has been associated with vascular smooth muscle cell hypertrophy, endothelial dysfunction, cardiac fibrosis, proteinuria, and renal vascular injury. 26 Clinical trials have proven the benefit of aldosterone receptor antagonism. Treatments that block the pathologic effects of the RAAS at several points have been shown to limit target-organ damage in hypertension and to decrease cardiovascular morbidity and mortality. 27 These study results proved the important role of aldosterone in the pathogenesis of atherosclerosis. However, an observation study had showed that the overall prevalence of carotid artery lesions was not significantly different between patients with primary aldosteronism and primary hypertension. 28 Although the studied population differed from our cohort, we have also showed that plasma aldosterone levels are not significantly associated with carotid atherosclerosis in this high-risk population.
The prognostic value of plasma renin for cardiovascular events is also controversial. In a community-based cohort, renin, aldosterone and ARR were not associated with all-cause mortality in hypertensive individuals. 29 However, plasma renin concentration is associated with an increased risk for cardiovascular events regardless of blood pressure according to a community-based cohort study. 30 To date, studies focusing on the relationship between carotid atherosclerotic plaques and ARR are scarce. Only one study evaluating the association of vascular damage and ARR in hypertensive children was reported. 31 The results showed that there was a positive association between carotid IMT and ARR but not serum aldosterone concentration or plasma renin activity in hypertensive children. However, our results showed that ARR was inversely associated with carotid IMT and plaque score, and plasma renin was positively associated with carotid IMT and plaque score in CAD patients. Carotid IMT and plaque score are not related to plasma aldosterone concentration. The associations between plasma renin and ARR and carotid IMT disappeared after adjustment of confounding factors (Table 4). The discrepancy in these two studies can be explained by the extremely different selected populations. Moreover, several studies have showed that the ultrasound assessment of carotid plaque, compared with that of carotid IMT, had a higher diagnostic accuracy for the prediction of future ischemic stroke and CAD events.32–35 Hence, plasma renin level and ARR might have significant prognostic values in stable CAD patients. Carotid plaque was a stronger predictor of coronary events than IMT and is more strongly associated with coronary stenosis than IMT.32,36 Carotid IMT is biologically distinct from carotid plaque, and from a pathological point of view, IMT is not really atherosclerosis, but another phenotype.33,34
There were several limitations in the present study. First, we studied a relatively small group of consecutive patients who were referred for coronary angiography because of stable angina pectoris and suspected CAD. Hence, the findings of our analyses in these CAD patients may not be extrapolated to a broader population such as patients with acute coronary syndrome. Second, the mean age of our patients was relatively high. The prevalence of multi-vessel CAD was much higher in advanced age, and the extent of CAD was affected by the integration of coronary risk factors including age and other risk factors. These selection biases could mean that our findings regarding the relationship between ARR and carotid plaque score are relevant only to this specific group and may not be applicable to the general population.
In conclusion, escape of plasma renin from suppression by relatively high plasma aldosterone levels represented by high plasma renin and low ARR might be a marker of structural vascular damage. This phenomenon occurs as a consequence of RAAS-mediated vascular injury and pinpoints marked atherosclerosis in coronary and carotid arteries. Identification of high renin and low ARR is important to identify patients with concomitant severe CAD and carotid atherosclerosis. More research is needed to identify the determinants of carotid atherosclerotic risk and to assess the best treatment strategy to decrease cardiovascular morbidity and mortality in CAD patients.
Footnotes
Acknowledgements
The authors thank the staff at the Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University for their role in data management and statistical analysis.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.