
Abstract
Introduction:
Angiotensin I converting enzyme (ACE) insertion and deletion (I/D) polymorphism has been implicated in the pathogenesis of osteoarthritis (OA). In recent years, numerous genetic factors have been identified and implicated in OA. In this Asian Indian population-based study, we aimed to evaluate the relationship between ACE (I28005D) gene polymorphism and primary OA. We performed a case-control association study to identify and explore the correlation between clinically, radiologically diagnosed individuals with primary knee OA and the ACE I/D polymorphism.
Methods:
Genomic DNA was isolated from 200 samples, including 100 OA cases and 100 healthy volunteers. DNA was amplified by polymerase chain reaction (PCR) using I and D allele-specific primers. PCR products were assessed via UV visualization of products electrophoresed on 2% agarose gels.
Results:
The groups differed significantly in genotype distributions (p < 0.05). The primary knee OA group showed a considerably higher incidence of the DD genotype and the D allele compared to the control group (OR = 2.14, 95% CI: 1.10–4.15, p = 0.02 and OR = 2.08, 95% CI: 1.39–3.10, p = 0.0003).
Conclusion:
The ACE gene polymorphism I28005D was found to be associated with primary knee OA in Asian Indian populations. This is the first study in India to report that the ACE gene polymorphism is a risk factor for early onset primary knee OA.
Keywords
Introduction
The insertion and deletion (I/D) polymorphism of the angiotensin-converting enzyme (ACE: NM 000789.2) gene is the first genetic variant associated with human physical performance and is in strong linkage disequilibrium with genetic factors that influence serum ACE concentrations. The I allele has been associated with certain aspects of endurance performance and functionally associated with reduced ACE serum levels and activity.1,2 The ACE gene, which consists of 26 exons, is 44,770 bp in size and is located on chromosome 17q23.3. The I allele of the ACE polymorphism (rs4646994) contains an Alu repeat sequence that is absent from the D allele, resulting in II, ID, and DD genotypes. 3 The D allele has been shown to be associated with higher levels of circulatory ACE enzyme in a dose-dependent manner. Despite being an intronic variation, it accounts for approximately half of the observed variance in plasma levels of the ACE protein. 4 The role of ACE polymorphism has been investigated as a risk factor for several diseases. Worldwide estimates indicate that 9.6% of men and 18% of women of 60 years of age have symptomatic osteoarthritis (OA).
OA is a multifactorial disease and is the most common form of arthritis with a clear genetic component, affecting 40% of individuals across age groups; it is also one of the most common disabling diseases worldwide. 5 It is characterized by the progressive loss of articular cartilage in the synovial joints and changes in the adjacent bone. 6 OA is a polygenic disease and its pathogenesis is influenced by several environmental factors such as ageing, hormones, mechanical factors, and lifestyle. Results of family-based and candidate gene studies have demonstrated that a genetic component is implicated in its pathophysiology. 7 ACE is a candidate gene for the development of OA, and it is known to play an important role in several inflammatory and immune-related disorders. ACE polymorphisms have been shown to be related to rheumatic and autoimmune diseases in particular.8,9 Based on these prior studies, we hypothesized that studies of ACE in OA patients could be used for determining the risk factors involved in the pathogenesis of this disease. To improve our understanding of the importance of ACE in the pathology of OA, we directly investigated the I28005D polymorphism of the ACE gene in OA patients from an Asian Indian population.
Materials and methods
Ethics
Ethical approval (KHL No. e374/07) for this research was obtained from the Institutional Ethics Committee, Hyderabad, India.
Assortment of subjects
Our study included 100 cases aged 25–65 years from the Department of Orthopedics, Kamineni Hospitals, Hyderabad, India who were clinically and radiologically diagnosed with primary knee OA based on the criteria that they should have KL grade 0–4, 10 and 100 age- and gender-matched healthy controls with no history of OA or any complications of metabolic disorders.
Collection of blood
Two milliliters of venous blood was collected in EDTA vacutainers from each subject (n = 200). Personal and family histories were taken simultaneously using a well-designed proforma.
Genotyping of polymorphism
Genomic DNA was isolated from blood samples using a salting-out technique. For DNA extraction, EDTA (300 µL) was added to the blood, and further dissolved in 50 µL of tris-EDTA buffer. 11 The quality of the isolated genomic DNA was quantified using a NanoDrop 2000 (Thermo Fisher Scientific, MA, and USA). The oligonucleotide sequences of the PCR primers for the I28005D alleles were selected from our previous studies, which had been performed in the same population.11,12 Genotyping for the ACE (rs4646994; I28005D) gene was accomplished by direct PCR, and successful amplification was confirmed by electrophoresis on 2% agarose gels. PCR reactions were performed in a thermal cycler, with initial denaturation at 95°C for 5 min, followed by 35 amplification cycles, each of which consisted of denaturation at 95°C for 30 s, 59°C for 30 s, 72°C for 45 s, and a final extension at 72°C for 5 min. Detection of a large band (490 bp) indicated that the allele contained the 287-bp Alu sequence; detection of a 190-bp band indicated the short allele, which does not contain the Alu sequence. Individuals with both the large and the short fragments, i.e. 490/190 bp, were identified as heterozygotes (Figure 1). Genotype fragments were imaged using a gel documentation system (Kamineni Life Sciences, Moula Ali, Hyderabad, India).

Gel picture showing the ethedium bromide stained PCR products.
Statistical analysis
Associations between genotype and OA were examined by odds ratio analysis, with 95% confidence intervals (CIs) and chi-square analysis, using the software OpenEpi. The allele frequencies of the ACE gene were tested to determine whether they were in Hardy–Weinberg equilibrium (HWE). Allelic frequencies were calculated according to the number of different alleles observed and the total number of alleles examined. Clinical data are expressed as mean ± standard deviation (M ± SD). Data were also analyzed by analysis of variance (ANOVA). An independent sample t-test was used to test the cases and controls. Statistical significance was defined as p < 0.05.
Results
Baseline characteristics
Table 1 shows the demographic characteristics of the subjects included in this case-control study, with (n = 100) and without (n = 100) OA. The groups did not differ significantly in gene or age composition (p = 0.88 and p = 0.87, respectively); however, they did differ significantly in weight (p = 0.001) and body mass index (BMI) (p = 0.01). Twenty-eight percent of patients had a positive family history.
Clinical characteristics of OA cases and controls.

NA= Not applicable/ not analyzed.
Association study
Single nucleotide polymorphism (SNP) I28005D, located in the intron 16 region of the ACE gene, showed a significant association with OA. In both the control and OA groups, the ACE alleles were found to be in HWE. Table 2 shows the distribution of the ACE gene I28005D genotypes in OA cases and controls. In controls, the genotype distribution was 32% (I/I), 46% (I/D), and 22% (D/D), whereas in OA patients, the distribution was 18% (I/I), 38% (I/D), and 44% (D/D). Significant variation was observed in the distribution of the D allele (OR = 2.08, 95% CI: 1.39–3.10, p = 0.0003) and the DD genotype (OR = 2.14, 95% CI: 1.10–4.15, p = 0.02) in the patient group compared to the control subjects. The D allele was significantly associated with the disease according to the dominant (OR = 2.14, 95% CI: 1.10–4.15, p = 0.02) and recessive models of inheritance (OR = 2.78, 95% CI: 1.50–5.15, p = 0.001). BMI is one of the co-variants for OA, and the obese population is more prone to the disease (Figure 2(a)). Hence, the study group was categorized as normal (18.5–24.9 BMI), overweight (25–29.9 BMI), or obese (>30 BMI) based on BMI. The prevalence of the D allele was higher in OA cases compared to controls, as shown in Table 3 (Figure 2(b)).
Genotype and allele distribution of ACE (I28005D) gene polymorphism.


(a) Correlation of BMI of OA cases vs. controls. (b) Correlation of genotype of OA cases vs. controls.
Calculation of weight and genotypes of ACE gene.

Yates correction and p value <0.0001.
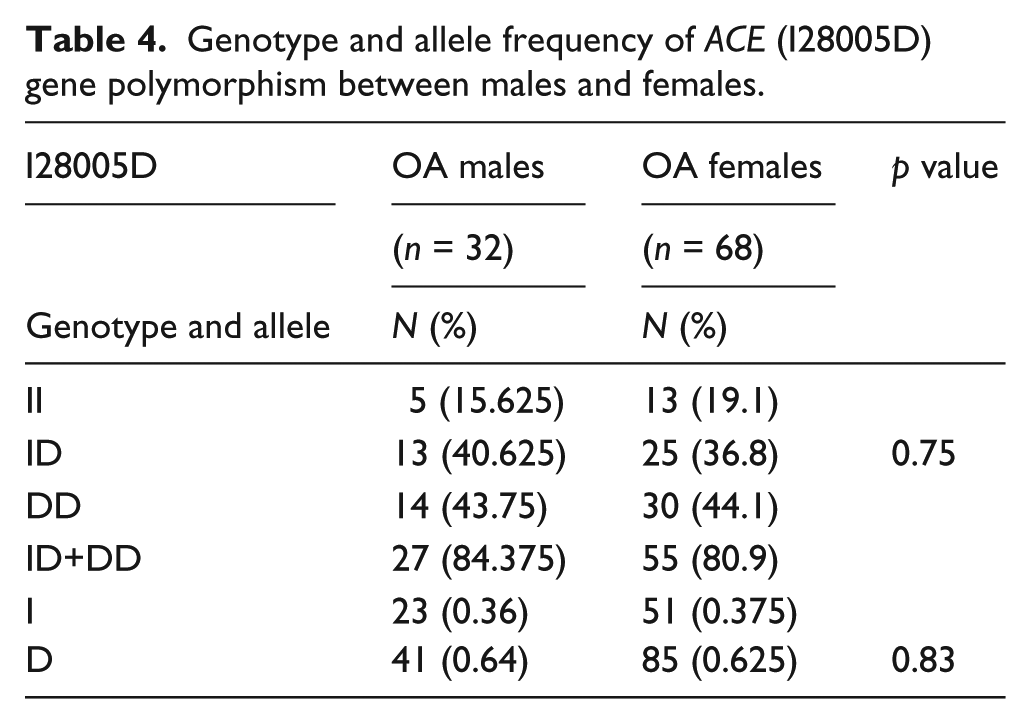
Both overweight and obese individuals with the D allele were more prone to OA. The controls did not show any association between BMI and genotype (Figure 3(a) and (b)). Neither allele nor genotype showed an association between the ACE I28005D polymorphism and OA, as shown in Table 4 (see also Figure 3(c)).

(a) Correlation of obese and overweight cases. (b) Correlation of controls. (c) Correlation between genotype and BMI of male and female cases.
Genotype and allele frequency of ACE (I28005D) gene polymorphism between males and females.
Other confounding factors, such as hypertension, type 2 diabetes mellitus (T2DM), and thyroid dysregulation were also investigated, and it was found that hypertensive individuals are more prone to OA.
Discussion
Severe OA is a cause of social, economic, and personal burden, and is the main cause of an increasing need for knee joint replacement. Susceptibility to complex diseases, such as OA, is often associated with genetic polymorphisms. A comprehensive study of CUMAGAS-OSTEO identified 66 variants, two of which, GDF5 (rs143383) and LRCH1 (rs912428), were associated with OA. 13 Recently it has been shown that the renin–angiotensin system (RAS) is directly involved in bone metabolism, and ACE inhibitors have been shown to have beneficial effects, attributed to a reduced level of angiotensin II and suppressed stimulation of the angiotensin II signaling pathway. 14 The RAS is primarily involved in the regulation of blood pressure and serum electrolytes. The biological mechanism of ACE has been shown to involve a metalloenzyme that converts angiotensin I to a potent vasoconstrictor, angiotensin II, and inactivates bradykinin, which is a vasodilator of the kallikrein–kinin system and has major implications in inflammatory processes including OA. 8 The RAS has been shown to be involved in the pathogenesis of several diseases, including fibrosis in the heart, kidney, lung, and liver during chronic inflammation, through regulation of cell growth, inflammation, oxidative stress, and fibrosis.
To the best of our knowledge, this is the first study to assess the association of polymorphisms of the ACE gene I28005D with OA in an Asian Indian population. In the present study, primary knee OA was found to be significantly associated with the DD genotypic and D allelic distributions compared to controls (2.78, 95% CI: 1.50–5.15, p = 0.001 and 2.08, 95% CI: 1.39–3.10, p = 0.0003). Our study shows that individuals with the D allele or the DD genotype have a more than twofold increased risk of developing OA. Thus, the I28005D polymorphism was found to be a biomarker for increased risk of OA and a risk allele among Asian Indians.
Several earlier studies conducted in Asian Indian populations found an association between ACE polymorphisms and certain diseases. We have previously reported an association of ACE polymorphism with T2DM with neuropathy and gestational diabetes.11,12 Narne et al. showed that it is associated with coronary artery disease (CAD) and myocardial infarction (MI), 15 Ganesan et al. showed an association with CAD and T2DM, 16 and Reddy et al. showed a significant association between MI and the DD genotype in our population. 17
Because weight and BMI primarily affect the knee joint, we categorized the OA cases into normal, overweight, and obese groups, based on BMI. It was observed that 68% of OA cases were obese and 26% were overweight. Obese individuals showed a 26-fold increased risk for development of OA compared to controls with normal body weight (26.44, 95% CI: 10.10–69.20, p < 0.0001), and overweight individuals showed a 12-fold increased risk for developing OA (12.13, 95% CI: 4.35–33.78, p < 0.0001). It is well established that weight gain is a risk factor for knee OA; however, a recent study by Apold et al. using a large sample size has indicated that the impact of weight gain is strongest in the younger age group and that this association weakens in the older age group. 18 Because 53% of the age-matched controls were also obese, it is evident that factors other than weight are also important in primary OA.
We attempted to determine the combined association of BMI and ACE ID polymorphism in OA. Our data indicated that the D allele potentiates the effect of BMI in both overweight and obese patients. We observed that >80% of overweight and obese patients possessed the D allele, whereas all patients with a normal BMI possessed the deleterious allele. An ANOVA showed a significant association (p < 0.0001) between BMI and genotype.
Our results are consistent with results reported by Hong et al., 9 Inanir et al., 8 and Bayram et al., 19 who showed that the DD genotype and the D allele are risk factors for OA in Korean and Turkish populations. However, a study on the same Turkish population by Bayram et al. did not find a significant association between OA and ACE polymorphism in patients with synovial fluid. 20 A study by Shehab et al. also failed to show an association between the ACE gene and OA in a Kuwaiti population. 21 Our present study was limited by our small sample size, and we were not able to measure the ACE levels; however, this study reports a significant association between polymorphism of the ACE gene I28005D and OA. In conclusion, angiotensin I converting enzyme (ACE) gene polymorphism is associated with primary knee OA in Asian Indian populations.
Footnotes
Acknowledgements
Gratitude is expressed to all the volunteers who participated in this study.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by Kamineni Hospitals, Hyderabad, India.