
Abstract
Objective:
Kidney development is key to the onset of hypertension and cardiovascular diseases in adults, and in the fetal stage will be impaired by a lack of nutrients in utero in animal models. However, few human studies have been performed.
Methods:
Kidney samples from fetuses in a fetal growth restriction (FGR) environment were collected and the morphological characteristics were observed. Potentially molecular mechanisms were explored by analyzing apoptosis and kidney-development related gene expression.
Results:
The results indicated that no malformations were observed in the kidney samples of the FGR group, but the mean kidney weight and volume were significantly decreased. Moreover, the ratio of apoptotic cells and Bax-positive cells was increased and the ratio of Bcl-2-positive cells was decreased in the FGR group, indicating potential apoptosis induction under an in utero FGR environment. Finally, aberrant expression of renin and angiotensinogen indicated potential kidney functional abnormalities in the FGR group.
Conclusions:
Our study suggested increased apoptosis and decreased renin and angiotensinogen expression during human kidney development in an FGR environment. The current results will be helpful to further explore the molecular mechanism of FGR and facilitate future studies of hypertension and cardiovascular diseases and the establishment of preventive methods.
Introduction
Ojeda et al. reported that growing fetuses display obvious plasticity to adapt to the dynamically changing in utero environment. Originally the so-called Baker Hypothesis described permanent responses to the impairment and stress in the developmental stages of a fetus, but since then, this hypothesis has been renamed the Fetal Origins of Adult Disease. 1 In this process, the fetus may survive, but exhibit permanent physiological, morphological and metabolic responses that increase susceptibilities to particular diseases. Recently, this concept has also been widely referred to as the Developmental Origins of Health and Disease. 2
Fetal growth restriction (FGR) can result from maternal dystrophia, preeclampsia and hyperuricemia. To protect key organs (heart and brain), the blood is redistributed to the key organs rather than the kidneys, liver and muscle tissues, which results in the non-optimal development of other organs under conditions of diminished oxygen and nutrition, which can enhance the prevalence of various diseases in adults. 3 Currently, about 30 million newborns worldwide are diagnosed with FGR, which is one of the most important potential risk factors of future health-related problems in humans.
Moreover, some studies reported that hypertension in adults aged 46–64 years was closely related to the incidence of lower birth weight.4,5 Other than higher blood pressure, low birth body weight may also induce the increasing incidence of diabetes and cardiovascular diseases (CVDs) in adults. In Sweden, an epidemiological study indicated that low birth weight (< 2.5 kg) and diminished weight gain by one year of age (< 8 kg) was strongly correlated to the incidence of diabetes and myocardial infarction later in life. 6 Therefore, FGR in the perinatal period may increase the risk of endocrinological abnormalities and CVD.
Although the mechanisms of FGR remain largely unknown, the importance of FGR has been accepted worldwide. Animal models have been used to mimic the compromised uterine environment of FGR to identify potential mechanisms. Typical methods to establish animal models of FGR include total thermal limitation, total protein limitation, maternal chronic oxygen deficit, dysfunctional placenta, and perinatal glucocorticoid treatment. More recently, models of FGR have been successfully established in mammals. In these models, significant correlations were identified between FGR and the onset of diseases in the mature animals. Offspring that matured in a compromised uterine environment exhibited changes in physiology and organ development. Moreover, kidney impairment was prevalent in all of the animal models, characterized by a decreased number of nephrons.
In humans, Keller et al. observed that the number of nephrons decreased by up to 50% and the glomerular volume doubled in hypertensive patients when compared with normotensive patients. These findings indicated that a decrease in nephron number resulted in hyperpiesis and the increased glomerular volume was attributable to compensatory hypertrophy and ultrafiltration. 7 Both research teams studied kidney development in a FGR model and suggested that the number of nephrons decreased by 35% compared with normal fetuses.8,9 Regarding the roles of the kidneys in the regulation of isohydria and blood pressure,1,10 a decrease in the nephron number likely contributes to onset of adult diseases; however, specific mechanisms remain largely unknown.
In the present study, we identified correlations between birth body weight and the number of nephrons by calculating the number of apoptotic renal cells in fetuses under FGR conditions compared with those of normal fetuses. Finally, important genes and proteins that promoted or inhibited apoptosis were identified and potential mechanisms explored.
Materials and methods
Ethics statement
All experimental protocols were approved by the institutional review board of Tianjin Central Hospital of Gynecology Obstetrics (Tianjin, China). All participants were informed of all procedural details, including the study duration, methods, publication of results and the disposal of the research samples, and submitted signed informed consent forms. No financial incentives were offered for sample collection. We guaranteed that all of the research samples were to be used for basic scientific research and not medical purposes.
Kidney collection
A total of 11 FGR fetal kidney samples were collected from pregnant women with or without preeclampsia from November 2009 to December 2010 at Tianjin Central Hospital, Department of Gynecology and Obstetrics. Of these samples, eight were obtained from pregnant women with moderate to severe preeclampsia and three from women with normal pregnancies. During the same period, a total of 12 non-FGR samples were also collected from women with normal pregnancies. All kidney samples had normal morphologies with no obvious malformations.
The left kidneys were collected from late-term aborted fetuses, weighed and immediately fixed with 10% formalin before the nephron number was determined. The kidney volume was calculated using the water displacement method. Briefly, the kidney was submerged in a bottle full of water and the overflow was collected to determine the displaced volume.
Hematoxylin and eosin (H&E) staining
The kidney tissues were dehydrated with ethanol, embedded in paraffin, cut into 4–6-μm thick slices, dewaxed with xylene, subjected to gradient alcohol hydration and stained with H&E stain. The samples were cleared in xylene and mounted under a light microscope (80i; Nikon, Tokyo, Japan). Two experienced pathologists who were blinded to the experimental protocol scored the kidney tissues for the degree of apoptosis, and at least 20 H&E sections in each group were scored.
Apoptotic cell identification via the terminal deoxynucleotidyl transferase-mediated dUTP nick end-labeling (TUNEL) method
Apoptosis was indicated by DNA strand breaks in cell nuclei and detected using the TUNEL assay according to the manufacturer’s instructions. The H&E-stained sections were deparaffinized, digested with proteinase K (20 μg/ml; Roche Diagnostics, Basel, Switzerland) and then incubated with terminal deoxynucleotidyl transferase (TdT) buffer (0.3 U/μl) and biotinylated dUTP (0.2 mM; Roche) in 1× TdT buffer (Invitrogen, Carlsbad, CA, USA) for 1 h at 37°C. Next, the sections were incubated in 10% normal horse serum to block nonspecific binding and then incubated for 1 h at room temperature with an avidin–biotin complex (dilution, 1:100) included in the Vectastain Elite ABC Kit (Vector Laboratories, Inc., Burlingame, CA, USA). The sections were then counterstained with 4′,6-diamidino-2-phenylindole, dihydrochloride (DAPI; Life Technologies) to identify cell nuclei and examined by fluorescence microscopy (80i). TUNEL-positive cells were counted in five randomly chosen fields for each section and presented as a percentage of the total number of cells.
Reverse transcription polymerase chain reaction (RT-PCR) and quantitative RT-PCR (RT-qPCR) analysis
Total RNA was extracted from the kidney samples. cDNA was synthesized from 1 μg of DNase-treated RNA with random hexamers and an 80-ng equivalent was used in each PCR reaction. All cDNA synthesis and PCR reaction components were purchased from Invitrogen (Carlsbad, CA, USA). Expression levels of the selected target genes were further analyzed by real-time PCR. cDNA was prepared from 500 ng of total RNA following DNase treatment and 10 ng of RNA and gene-specific primers (Table 1) were used for PCR amplification. Melting curve analysis was performed at the end of each reaction. Data are presented as the mean ± standard error of the mean from three independent experiments. Expression levels were normalized to β-actin (internal control).
Polymerase chain reaction primers used to detect Bax, Bcl-2, renin, angiotensinogen and β-actin gene expression.

Western blot analysis
The kidney samples were lysed in 200 µl of radioimmunoprecipitation assay buffer containing fresh protease inhibitor cocktail tablets. Equivalent amounts of protein, as determined by the colorimetric Bradford protein assay, were resolved by sodium dodecyl sulfate-polyacrylamide gel electrophoresis with 12% agarose gels and then transferred to polyvinylidene fluoride membranes, which were then blocked with 5% non-fat dried milk before immunoassay using human monoclonal antibodies. Expression levels were normalized to glyceraldehyde 3-phosphate dehydrogenase (internal control).
Statistical analysis
Significant differences between the FGR and control groups were identified using the t-test. A probability (p) value < 0.05 was considered statistically significant.
Results
Clinical data
General clinical data for the patients and fetuses are summarized in Table 2. In the FGR group, the mean patient age was 25.3 ± 5.3 years (range, 21–32 years), which was not significantly different from that of the pregnant women in the control group. In the FGR group, the mean pregnancy duration was 33.4 weeks, which was comparable to that of the pregnant women in the control group (Table 2).
Summary of information on pregnant women.

In the FGR group, a total of 11 fetuses (six males and five females) were collected, including three that died intrauterine because of placental abruption induced by severe preeclampsia, two from late-term abortions because of malformations (one cheilopalatognathus and one diaphragmatocele) merged with severe preeclampsia, and six because of FGR. In the control group, a total of 12 fetuses (five males and seven females) were collected, including four due to cheilopalatognathus, one with abnormal brain development, two with diaphragmatocele, one with achondroplasia, two with esophageal atresia and two that were aborted by parental consent. Of the 23 fetuses, all kidneys had normal morphologies with no obvious malformations (Table 3).
Summary of fetal information.

The morphology was no malformation and looks normal.
SN: serial number; M: male; F: female; PASP: placental abruption induced by severe preeclampsia; ABD: abnormal brain development
Characteristics of the kidney samples
To confirm the effects of FGR on kidney development, characteristics of the kidney samples were analyzed. In the FGR group, the average fetal birth weight was 1094 ± 383 g, which was significantly lower than that in the control group (1964 ± 439 g). Moreover, the kidney weight and volume collected from the FGR fetuses were also significantly decreased compared with those in the control group. The nephrons were counted, which showed a lower number in the FGR group (Table 4).
Comparison of birth weights and kidney characteristics between FGR and control groups.
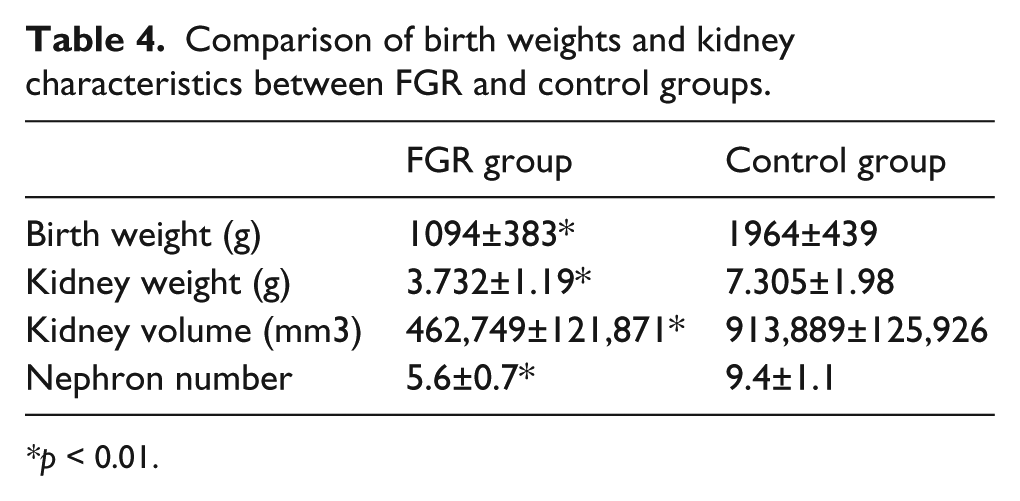
p < 0.01.
Next, fetal weight and the number of nephrons were analyzed, which identified a significant positive correlation (Spearman’s rank correlation coefficient, 0.86584; p < 0.001) (Figure 1), indicating that the decreased number of nephrons contributed to decreased body weight. There were no correlations between fetal gender and the number of nephrons.

Correlations of fetal body weight and the number of nephrons.
Apoptotic cell analysis
The TUNEL assay was performed to analyze the mechanisms of impaired kidney weight and volume in the FGR group. The positively stained cells, in which the nuclei were stained yellow, were regarded as apoptotic (Figure 2(a) and (b)). A total of 1000 cells were analyzed in five random views and the number of apoptotic cells was recorded. The results showed that about 10% of cells in the samples from the FGR group were apoptotic, whereas only 5.7% were apoptotic in the control group, which was significantly lower (Figure 2(c)). Moreover, two apoptosis-related genes were expressed in the FGR and control groups. Immunohistochemical analysis revealed a much higher ratio of Bax-positive cells and much lower ratio of Bcl-2-positive cells in the FGR group compared with the control group (Figure 3).
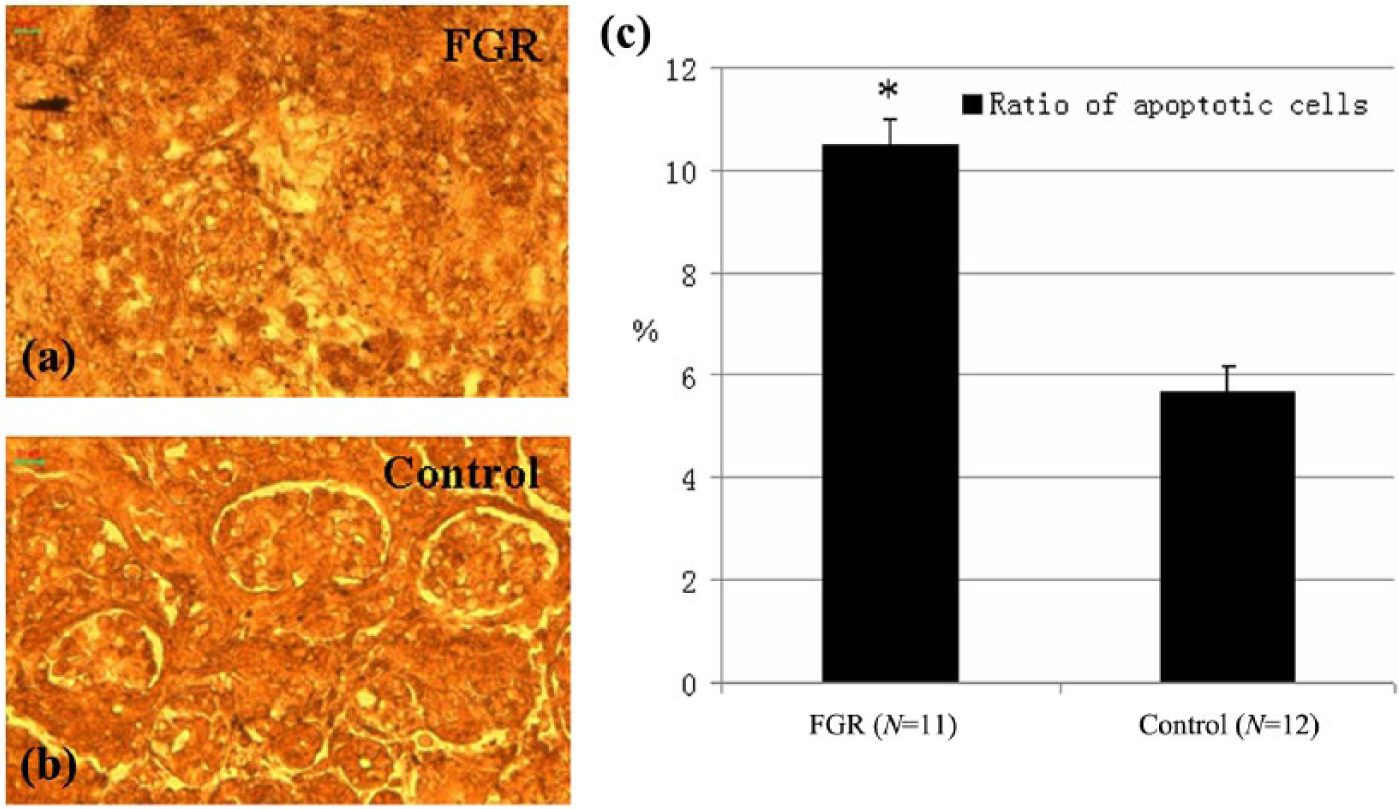
Effects of fetal growth restriction (FGR) on apoptosis of kidney cells. (a) Apoptotic cells in an FGR kidney section; (b) apoptotic cells in a control kidney section; (c) comparison of the ratio of the apoptotic cells between the FGR and the control kidney samples. Scale bar =50μm.

Expression of apoptosis-related genes in kidney samples. (a) Bax expression in a fetal growth restriction (FGR) kidney section. (b) Bax expression in a control kidney section. (c) Bcl-2 expression in a FGR kidney section. (d) Bcl-2 expression in a control kidney section. (e) Comparison of the ratio of Bax- and Bcl-2-positive cells between the FGR and control kidney samples. Scale bar =50μm. *p < 0.05. (f) Comparison of relative Bax and Bcl-2 mRNA expression. *p < 0.05.
Identification of renin and angiotensinogen in kidney samples
To further identify differences between the FGR and control groups, two important genes closely related to kidney development, renin and angiotensinogen, were analyzed by RT-PCR and western blot analyses. The results showed that the gene expression profiles of renin and angiotensinogen were significantly down-regulated in the FGR group compared with those of the control group, and the protein expression profiles showed similar tendencies (Figure 4).

Effects of fetal growth restriction (FGR) on the expression profiles of renin and angiotensinogen. (a) Comparison of relative renin and angiotensinogen mRNA expression. *p < 0.05. (b) Western blotting results of the FGR and control samples. (c) Comparison of relative protein expression of renin and angiotensinogen proteins. *p < 0.05.
Discussion
In the present study, we systematically investigated the effects of FGR on kidney development and identified important gene expression profiles. The results indicated no malformations in the kidney samples from the FGR group, but the mean kidney weight and volume were significantly decreased compared with the controls. Moreover, the ratio of apoptotic and Bax-positive cells was increased and the ratio of Bcl-2-positive cells was decreased, which indicated potential apoptosis induction under the in utero FGR environment. Finally, the aberrant expression of two important kidney development genes indicated potential functional abnormalities in the FGR group.
Hypertension threatens the health of 25% of the population worldwide and contributes to the onset of CVD and chronic renal diseases; 11 however, the pathology remains unclear, resulting in the scarcity of preventive methods. 2 Baker et al. suggested that CVD was actually the result of the fetus adapting to the lack of nutrients in the uterine environment, resulting in morphological and functional changes of important fetal organs and an increased risk of hypertension and CVD later in life. These results were in accordance with previous epidemiological investigations. 12
Results from a previous animal model study suggested that limited protein intake during pregnancy may result in FGR with offspring with a decreased number of nephrons,13-15 in accordance with results from a human study. 16 However, the molecular mechanisms remain unknown. In the present study, we observed decreased fetal body weight, kidney volume and weight, and number of nephrons in the FGR group.
During development of organs and tissues, programmed cell death is an important process; however, aberrant apoptosis will result in altered organ morphology and function. 17 During kidney development, nephron formation will be impaired in response to excessive cell death, resulting in the presence of atrophic nephrons. In the present study, the number of apoptotic cells was increased in kidney samples from the FGR group, which may have resulted in the decreased kidney volume and weight, as well as the lower number of nephrons. Welham et al. fed pregnant rats with a low protein diet and observed that the offspring became hypertensive because of the decreased number of nephrons, the increased number of apoptotic cells, and the changes in renin and angiotensinogen expression. Therefore, they concluded that a lack of nutrients in the uterine environment will result in hypertension when the offspring mature into adults. 18
In the present study, Bax and Bcl-2 expression were analyzed. Bcl-2 is a key regulator of apoptosis inhibition, which can prolong cell proliferation and increase cell number. Bax belongs to the Bcl-2 family, but functions in opposition to Bcl-2. Bax can induce cell apoptosis and inactive Bcl-2 by forming heterogenous dimers that coalesce with Bcl-2.19-21 Pham et al. suggested that Bcl-2 expression was significantly down-regulated and Bax expression was significantly up-regulated in FGR models,22,23 which was similar to our results in humans.
Results from a previous animal study suggested that the decreased number of nephrons in FGR was not only related to cell apoptosis, but also to the changes in the renin–angiotensinogen system (RAS). 24 RAS plays a key role in the regulation of body fluids and salt metabolism, and was higher expressed in the developing kidney. Thus, aberrant expression of genes in the RAS will result in abnormal kidney development. Goyal et al. observed a decreased number of nephrons and onset of hypertension in a mouse model treated with an angiotensin receptor blocker and suggested that RAS plays a key role in kidney growth and maturation. 25 Grigore et al. feed neonatal mice with a high dose of the angiotensin receptor inhibitor losartan and found that all mice became hypertensive by the age of 22 weeks and the number of nephrons was decreased by at least 42%, which indicated that insufficient angiotensin activity will disrupt normal kidney development and result in a decreased number of nephrons. 26
In humans, Moritz et al. observed that cells containing renin were located in the deep cortex and suggested that both the lack of nutrients in the uterine environment and inhibition of RAS activity resulted from kidney impairment, and the limited supply of nutrients and oxygen inhibited RAS expression. 27 In the present study, we showed that renin and angiotensinogen were two key genes that were down-regulated in the RAS, which provided further proof of Moritz’s hypothesis. Zhang et al. suggested the mRNA expression of these two genes was dysregulated in FGR offspring of sheep. 28 However, in a previous mouse study, Vehaskari et al. suggested the opposite: an up-regulation of mRNA expression of the renal renin protein, 29 which may reflect a potential compensatory mechanism when the fetus is subjected to a lack of nutrients in the uterine environment.
In conclusion, the results of the present study suggested the roles of apoptosis in kidney development of human FGR fetuses and also indicated changes in RAS gene expression profiles in these samples. The current results will be helpful for further explorations of FGR molecular mechanisms and also facilitate future studies of hypertension and CVD, and the establishment of preventive methods.
Footnotes
Conflict of interest
The authors declare no conflicts of interest.
Funding
This work was supported by key program of Tianjin health care (grant number 12KG128).