
Abstract
Introduction:
Brachial blood pressure increases with exercise and an excessive rise predicts increased cardiovascular risk. Measurement of brachial blood pressure alone may exaggerate the true blood pressure elevation due to exercise-induced change to pressure amplification. Whether blood pressure-lowering treatment modulates pressure amplification during exercise is unknown.
Methods:
Thirty-two participants with stage 1–2 hypertension (mean age 59.2 years) received eight weeks’ blood pressure lowering with either aliskiren (300mg, n=16) or valsartan (320mg, n=16). Brachial and central aortic pressure (CASP) were measured non-invasively during treadmill exercise (Bruce protocol) at baseline, after eight weeks’ treatment and 48 hours following treatment withdrawal.
Results:
The rise in brachial blood pressure with exercise exceeded the rise in CASP, indicative of enhanced pressure amplification. Eight weeks’ treatment elicited similar reductions in brachial blood pressure and CASP which did not differ between rest and peak exercise (p>0.05). The exercise-induced increase in systolic pressure amplification did not differ between baseline and following eight weeks’ treatment (p>0.05). These effects remained unchanged following treatment withdrawal.
Conclusion:
Blood pressure lowering does not directly influence the relationship between aortic and brachial pressure either at rest or during exercise in patients with hypertension, other than through proportionate lowering of both pressures. These effects remained unchanged 48 hours after a simulated missed medication dose.
Keywords
Introduction
Brachial blood pressure (BP) increases with exercise and an exaggerated rise in BP during exercise has been shown to be an independent predictor of myocardial infarction, left ventricular hypertrophy, stroke and cardiovascular death.1–4 It is, however, well recognized that brachial BP can be an imperfect surrogate for the corresponding central aortic pressure at the aortic root, due to variation in the degree of aortic–brachial pressure amplification. To date, the effect of exercise on central aortic pressure has received little attention, in part due to the complexity of undertaking such measurements during active exercise. Early invasive studies with direct measurement of aortic pressure demonstrated an exaggeration of pressure amplification from the aortic root to the periphery with vigorous exercise, such that the exercise-induced rise in peripheral pressure was found to exceed the rise in central pressure.5,6 More recently these differential effects of exercise on peripheral and central pressure have been confirmed using non-invasive methods based on peripheral pulse wave analysis, suggesting that the magnitude of pressure amplification may depend upon the type and extent of exercise undertaken, as well as age and other factors.7–11
Remarkably, to date no previous study has reported the effects of BP-lowering treatment on the response of central pressure to exercise. We recently reported in this journal data from a study evaluating the effects of two different strategies for therapeutic inhibition of the renin–angiotensin system (RAS) on brachial BP during exercise. This study compared the direct renin-inhibitor aliskiren with the angiotensin receptor blocker valsartan and showed that both treatments similarly attenuated an exercise-induced rise in brachial pressure. 12 In that study, central aortic pressure was also recorded non-invasively via pulse wave analysis, using tonometry (BPro™, HealthSTATS International, Singapore) and mathematical computation of the radial pressure wave. 13 These data are presented in the current report and describes for the first time the effects of BP-lowering therapy on the relationship between central aortic and brachial pressures during exercise.
Patients and methods
The results presented in this paper derive from both pre-specified and exploratory analysis of data from patients recruited into a multicentre randomized controlled trial (RCT) evaluating the effects of RAS blockade on brachial and central aortic pressures (ClinicalTrials.gov NCT00819767) and EUDRA CT (2008-005500-10). 12
Patients
Men and women aged ≥ 50 years with stage 1–2 hypertension (mean sitting systolic BP (msSBP) ≥ 140 mmHg and < 180 mmHg, and mean sitting diastolic BP (msDBP) < 110 mmHg, measured at rest) were eligible for inclusion. In addition, patients had to be anticipated to be able to reach peak exercise capacity (85% of their predicted maximum heart rate) during a treadmill exercise test conducted according to the standard Bruce protocol.
The main exclusion criteria included: secondary hypertension, therapy with more than two antihypertensive drugs, a history of severe cardiovascular or cerebrovascular disease, known Keith–Wagener grade III or IV hypertensive retinopathy, and type I diabetes. Pregnant or nursing women were also excluded. All patients provided written informed consent before participating in any study procedures and all study centres received approval from the relevant local and central ethical review boards.
Study design
The study design has been reported previously 12 and is outlined below.
The study from which data were analysed was a randomized, double blind, parallel-group study. After a two-week washout and a one- to two-week placebo run-in period, eligible patients were randomized to once-daily aliskiren 150 mg or valsartan 160 mg for one week, with forced titration to double the initial dose for a further seven weeks (Figure 1). Three treadmill exercise tests were conducted using the standard Bruce protocol at: (i) baseline (immediately prior to randomization), (ii) at the end of the active treatment period (week 8) and (iii) 48 hours after treatment withdrawal, to evaluate the persistence of the treatment effect two days after treatment withdrawal (missed dose, week 8 + 2 days).
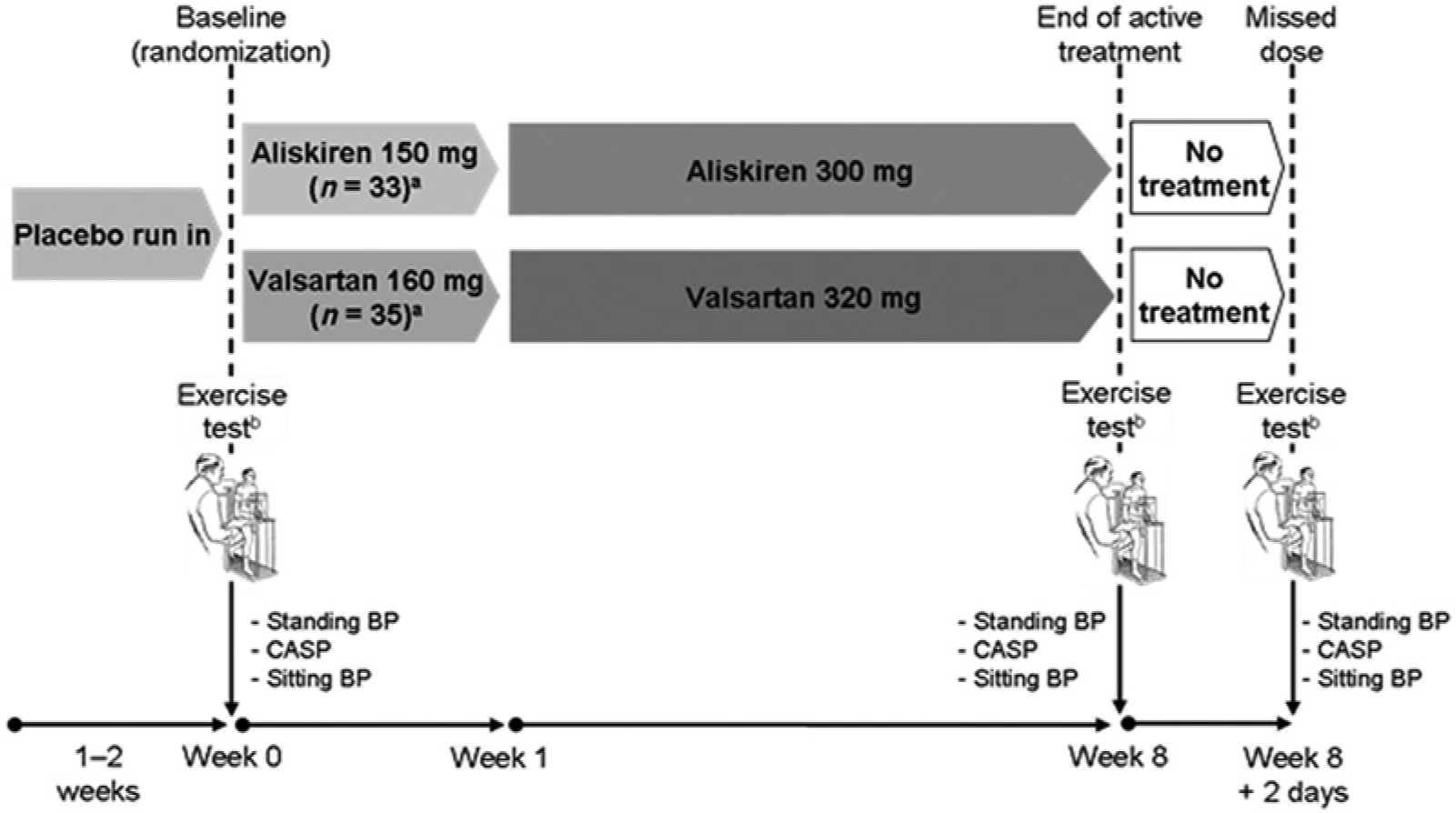
Overall study design. All doses were administered once daily.
Exercise tests were conducted according to American College of Cardiology/American Heart Association (ACC/AHA) 14 and European Society of Cardiology (ESC) guidelines for exercise testing 15 and patients were closely monitored before, during and after the tests. Electrocardiogram (ECG) monitoring was continuously performed during the test to ensure patient safety and tests could be stopped if any of several ECG criteria were met (such as severe ST-segment depression; ST-segment elevation; frequent ventricular extra-systoles; onset of ventricular tachycardia).
Study assessments
The main objective of this analysis was to assess the exercise-induced changes in central aortic systolic pressure (CASP) relative to the corresponding changes in standing brachial BP after eight weeks of aliskiren or valsartan therapy and following treatment withdrawal. Our primary focus was on CASP because the measurement of pulse pressure (brachial and central) is dependent upon accurately determining true diastolic pressure, which we found to be less reliable with manual sphygmomanometry during exercise. The primary endpoint for this analysis was the change in systolic pressure amplification from rest to peak exercise, comparing baseline with end of treatment (eight weeks). Changes in other central haemodynamic variables during exercise were also investigated. In order to standardize exercise effort according to the Bruce protocol, incremental treadmill exercise was maintained by each participant until 85% predicted maximal heart rate (HR) had been achieved (100% of predicted HR: female 200 – age; male 220 – age).
For the primary analysis, due to the limited size of the study, baseline and treatment data for the study population were pooled to assess the physiological effects of exercise on brachial and central pressure parameters. This was a reasonable approach as we had shown that both valsartan and aliskiren had had similar effects on brachial pressure at rest and during exercise. 12 Brachial BP and CASP were measured whilst standing at rest, at peak exercise and during the recovery phase, prior to administering study medication. Other central haemodynamic variables, including systolic pressure amplification ratio (calculated as brachial/central BP), were also recorded.
Standing BP provided the baseline (at rest) value for the exercise test, and was the mean of three measurements taken at 1–2-min intervals prior to the test. Standing BP was also measured during exercise at the end of each 3-min period, immediately after reaching peak exercise capacity and during the recovery period (10, 20 and 30 min after peak exercise; Figure 1 and Supplementary Digital Content Figure 1 online). A mercury sphygmomanometer was used for brachial BP measurement due to the recognized unreliability of automated BP measurement during exercise. Systolic BP was defined according to the onset of Korotkoff phase I sounds, whilst diastolic pressure was defined using Korotkoff phase IV sounds.
Measurement of central aortic pressure
Central aortic pressures were measured using the BPro™ device (HealthSTATS International, Singapore) during each exercise test at rest, at peak exercise and during recovery (at 10, 20 and 30 min after peak exercise). The device, designed like a wrist watch, uses applanation tonometry to capture radial artery waveforms, which are calibrated to brachial BP and processed using a validated algorithm to derive central aortic pressures.13,16 The device was worn clamped to the wrist using a ‘square lock’ restraint, which allowed reliable and consistent recording of high-fidelity radial artery waveforms during exercise testing. At rest, waveforms were captured immediately following the final of three brachial blood pressure measurements (within 15 s) and calibrated to the averaged brachial blood pressure. At peak exercise and during the recovery period, waveforms were captured immediately following the first brachial blood pressure measurement with the participant temporarily stationary and with their wrist held still at heart level. Captured waveforms were back-calibrated to the appropriate brachial blood pressure value. For all measurements using the BPro™ device, arterial pressure waveforms were sampled in 10-s blocks over the course of 20–30 s and the first stable waveform block used for data analysis. In selecting the first stable waveform block, waveforms were visually inspected for anomalies by an experienced operator and quality control criteria applied to ensure adequate pulse height (100 mV) and pulse length variability (<20%).
Statistical analyses
The study population was defined as those participants completing central and brachial blood pressure measurements both at rest and at peak exercise. Normally distributed variables are presented as mean ± SD, non-normally distributed data are presented as median ± interquartile range. Comparison between continuous variables used paired Student’s t-test or repeated measures analysis of variance. In all tests a two-tailed p-value of ≤0.05 was considered statistically significant. Database management and statistical analysis were performed using IBM SPSS for Windows version 20 (IBM corporation, Armonk, NY, USA).
Results
We have previously reported in this journal the influence of BP lowering during exercise testing on brachial blood pressure in 68 participants. 12 Of these, 32 participants (16 aliskiren, 16 valsartan) completed central pressure recordings both at rest and at peak exercise across the eight week treatment period. The present report describes the influence of BP lowering on brachial and central pressure during exercise testing in these 32 participants.
Patient disposition and baseline characteristics
More than two-thirds of patients in the study were male (68.8%) and almost all were Caucasian (96.9%). Mean age was 59.2 years, and 34.4% of patients were obese (body mass index (BMI) ≥ 30 kg/m2) with a mean BMI of 28.8 kg/m2 (Table 1). The baseline characteristics of the study population were similar to those previously reported for the entire patient population 12 (n=68).
Patient demographics and baseline characteristics.

Data are for the randomized set. Values are presented as mean ± standard deviation unless otherwise stated.
BMI ≥ 30 kg/m2.
BMI: body mass index; BP: blood pressure; DBP: diastolic blood pressure; SBP: systolic blood pressure
Effects of exercise on CASP and brachial BP at baseline in the pooled population
At baseline, as expected, standing CASP was lower than standing brachial SBP at rest (137.0±10.3 vs. 150.9±10.9 mmHg) in the pooled patient population (n=32). CASP increased from rest to peak exercise by a mean of 30±25.5 mmHg, and then fell to below the resting level during the recovery period (Figure 2). The changes in standing brachial SBP showed a similar profile during exercise (Figure 2), although the mean increase from rest to peak exercise (50.6±28.4 mmHg) was much greater than that for CASP (p<0.01). Systolic pressure amplification, that is, the ratio between CASP and brachial SBP, together with the difference between brachial and central pressures, showed a marked elevation with peak exercise before declining to resting values during recovery (Figure 3).

Influence of blood pressure-lowering treatment on brachial and central blood pressure during exercise in the pooled population. Data were analysed at baseline, after eight weeks of treatment and 48 hours after a missed dose. Data show mean ± SEM.

Influence of BP-lowering treatment on systolic pressure amplification and the difference between brachial and central pressure during exercise in the pooled population. Data show mean ± SEM.
Effects of BP lowering at rest and during exercise in the pooled population
Eight weeks’ BP-lowering treatment was associated with reductions in both brachial SBP and CASP from baseline at rest (Figure 2). Eight weeks’ treatment was also associated with reductions in brachial SBP and CASP at peak exercise. The extent of the treatment-induced reductions at rest and peak exercise did not differ when compared (reduction in brachial SBP: rest −15.9±13.0 mmHg, peak exercise −12.7±25.9; difference 3.2±26.5 mmHg, p=0.5; reduction in CASP: rest −16.1±13.5 mmHg, peak exercise −8.9±23.3 mmHg; difference 7.1±24.6 mmHg, p=0.11). Similarly, the extent of the increase in brachial SBP and CASP from rest to peak exercise did not differ between baseline and after eight weeks’ treatment (brachial SBP change (rest–peak exercise): baseline 50.6±28.4 mmHg; eight weeks’ treatment 53.8±21.7 mmHg, p=0.5; CASP change (rest–peak exercise): baseline 30±25.5 mmHg; eight weeks’ treatment 37.1±19.2 mmHg, p=0.11). Whilst statistical analysis revealed no difference between the effects of treatment at rest and peak exercise, a trend towards a lesser reduction in CASP, however, was apparent at peak exercise relative to rest. Similarly, a trend toward a greater increase in CASP with achievement of peak exercise was seen following eight weeks’ treatment relative to baseline. Importantly, as reported at baseline, the rise in brachial SBP exceeded the rise in CASP following eight weeks’ treatment.
Systolic pressure amplification and the difference between brachial and central pressure both showed an increase from rest to peak exercise (Figure 3). The extent of these increases with exercise did not differ between baseline and after eight weeks’ treatment (increase in systolic amplification (rest to peak exercise) at baseline 0.11±0.09; increase in systolic amplification (rest to peak exercise) after eight weeks’ treatment 0.08±0.1; difference 0.03±0.1, p=0.08; increase in brachial minus central pressure (rest to peak exercise) at baseline 20.6±13 mmHg; increase in brachial minus central pressure (rest to peak exercise) after eight weeks’ treatment 16.7±13.2 mmHg; difference 3.9±14.8 mmHg, p=0.15). However, consistent with the effects of treatment on CASP relative to brachial SBP, trends towards lesser increases in systolic amplification and the difference between brachial and central pressure were seen with exercise, following eight weeks’ treatment (Supplementary Digital Content Figure 2).
These data indicate that whilst eight weeks’ treatment reduced brachial and central BP both at rest and at peak exercise, the pattern of change in these parameters with exercise remained essentially unaltered. This was seen in spite of some residual variability in the effects of treatment on central pressure at peak exercise.
Effects of a missed medication dose on BP lowering at rest and during exercise in the pooled population
Forty-eight hours after a missed medication dose, brachial and central pressures remained unaltered both at rest and at peak exercise relative to values seen after eight weeks’ treatment (Figure 2). Similarly, the increase with exercise in systolic pressure amplification and the difference between brachial and central pressure remained unchanged relative to that seen at eight weeks or baseline following a missed medication dose (Figure 3).
Analysis of data by BP-lowering treatment type
Whilst this study was not powered to demonstrate differences in exercise haemodynamics between treatments, the changes in brachial and central pressure during exercise were broadly similar when the two different treatments (aliskiren versus valsartan) were compared (Figure 4).

Influence of treatment type on brachial SBP and CASP during exercise. Data are shown at baseline, after eight weeks of treatment and 48 hours after a missed dose. Upper panel: aliskiren; lower panel: valsartan. Data show mean ± SEM.
Discussion
To our knowledge, this is the first report of the influence of BP lowering on exercise-induced change in brachial and central blood pressure in people with hypertension. The main findings are that the rise in central pressure from rest to peak exercise was markedly lower than the corresponding rise in brachial pressure, consistent with increased aortic–brachial systolic pressure amplification during exercise. Blood pressure lowering treatment for eight weeks reduced both brachial and central pressures at rest and during exercise. However, the reductions in aortic and brachial pressures following treatment were proportionate to the pre-treatment relationship between aortic and brachial pressures, at all time points. These findings demonstrate for the first time that BP-lowering treatment, at least with the drugs tested here, does not exert a major influence on the relationship between aortic and brachial pressure at rest and during exercise, other than through proportionate lowering of both pressures. Consistent with the latter, the increased systolic pressure amplification associated with peak exercise was not significantly modulated by BP-lowering treatment, nor was there any significant treatment-induced change in the difference between aortic and brachial pressure at corresponding time points. If anything, there was a trend toward a lesser reduction in central relative to brachial pressure at peak exercise, together with a trend to a smaller exercise-induced increase in systolic amplification following eight weeks’ treatment, which did not achieve statistical significance. Finally, the beneficial influence of treatment on brachial and central pressure during exercise was not diminished 48 h after medication withdrawal, simulating a missed medication dose.
The exaggeration of systolic and pulse pressure amplification with exercise has been demonstrated in previous studies using both direct5,6 and indirect7–11 measurement of aortic pressure waveforms, together with contemporaneous measurement of peripheral BP. This indicates that the true pressure excursion (i.e. central pressure) during exercise is much less dramatic than the typical rise in brachial pressure. This may be a direct consequence of functional changes in the systemic circulation in response to the demands of the working musculature for increased perfusion, but may also serve to protect the major organs against excessive pressure elevations during the exercise period.
The mechanism for the increase in systolic pressure amplification during exercise has not been fully elucidated. Dynamic exercise is associated with increases in cardiac output, heart rate and sympathetic mediated vasoconstriction and venoconstriction. In addition to the consequent elevation in systemic BP in response to exercise, stimuli within the exercising musculature mediate localized vasodilatation in response to the increased metabolic activity to maintain adequate muscle perfusion. Thus assessment of central BP together with peripheral blood pressure as measured over a non-working musculature, for example, over the brachial artery in the case of treadmill exercise, demonstrates enhanced pressure amplification relative to the resting state.5–11 By contrast, the degree of central to peripheral amplification has been reported to be attenuated when peripheral pressure is measured over the working muscle 5 as a consequence of local vasodilatation in the working limb.17,18 Similarly, the exercise-induced enhancement in central to peripheral amplification measured over the non-working muscle has been reported to be attenuated following initiation of local vasodilator stimuli such as induction of reactive hyperaemia 6 or application of heat locally. 19 These observations indicate that the increased pressure amplification induced by exercise may be modulated by local conditions and may involve changes to pressure wave reflections in the face of an unchanged or diminished aortic impedance. Alternatively the enhanced amplification may result as a consequence of increased blood flow into a vasoconstricted vasculature and may also result in part from enhanced sensitivity of central BP to increasing HR. 20
Our observation that the enhancement in pressure amplification with exercise remained relatively unchanged despite BP lowering is intriguing. It suggests either that in spite of effective BP lowering, RAS blockade does not directly affect the physiological performance of the arterial system during exercise, or that global changes to the physical characteristics of the arterial system do not modulate the pressure amplification response to exercise. The latter is consistent with other studies investigating the influence of factors such as diabetes or ageing on pressure amplification. Thus, whilst type 2 diabetes has been associated with exaggerated brachial and central BP responses to exercise relative to age- and gender-matched people without diabetes, no difference in systolic or pulse pressure amplification between groups was reported either at baseline or following exercise. 21 In a study comparing the effects of exercise on brachial and central pressure in groups of young and older men, Casey and colleagues 11 reported that whilst ageing was associated with changes to brachial and central pressure at both rest and peak exercise, there was little difference in the magnitude of the pressure amplification change to exercise in relation to age. Similar data were reported by Sharman and colleagues 10 with regard to the influence of age on the exercise-mediated change from baseline values in pressure amplification. However, these workers also reported a reduction in the extent of exercise-induced amplification in the presence of hypercholesterolaemia. This was interpreted to indicate that exercise-induced elevations in pressure amplification were attenuated by enhanced peripheral pressure wave reflections resulting from impaired endothelial function with hypercholesterolaemia.
Our findings would not necessarily support a major role for wave reflection. Treatment-induced reduction in wave reflections might have been expected to minimize the exercise-induced increase in central relative to brachial pressure, thereby enhancing the amplification response. Instead, we found a trend towards an attenuated exercise-induced increase in amplification following treatment, which is difficult to reconcile with the concept of beneficial effects of treatment on wave reflections.
Our suggestion that wave reflections are unlikely to play a major role in modulating exercise-mediated pressure amplification is supported by recent work using wave separation analysis during moderate exercise22,23 which indicates that changes in pressure amplification with exercise are independent of changes to arterial pressure wave reflections. Similarly, other studies investigating the influence of short-term infusion with noradrenaline or inhibitors of nitric oxide synthase (LNMMA) on the change in pressure amplification during exercise 8 report no change to the exercise-induced increase in pressure amplification with drug infusion. These data are also consistent with the notion that exercise-induced changes to pressure amplification are independent of global change in arterial physical characteristics.
A key issue for the interpretation of exercise studies using non-invasive measurements of central pressure is whether exercise itself has any influence on the method for deriving central pressure. Previous studies have produced equivocal findings. Sharman and colleagues, using a commercially available generalized transfer function for deriving central pressure, reported no influence of exercise on non-invasively-derived central pressure in a small group of patients referred for diagnostic cardiac catheterization. 7 Similarly Holland and colleagues 24 reported non-invasively-derived central pressure to be a reproducible and reliable technique during haemodynamic perturbations induced by exercise. However, using a radial to carotid transfer function, Payne and colleagues reported that exercise was associated with an underestimation of transfer function-derived carotid pressure compared with directly measured carotid pressure, in a group of healthy men undergoing moderate exercise. 25 Other workers using a digital to aortic transfer function generated in cardiac patients reported that exercise modulates the characteristics of the transfer function such that derivation of aortic pressure became unreliable, especially at higher heart rates. 26 Importantly, however, the extent of any possible underestimation in central systolic pressure defined in these studies was small, that is, no more than 5mmHg, when compared with the rise in central pressure with exercise (circa 30mmHg in our study) and is comparable to the variability typically seen in comparisons between invasively-measured and non-invasively-derived central pressure.
By contrast, studies using direct invasive measurement of aortic pressure suggest little influence of exercise on aortic waveform shape, 27 or on the impedance spectrum, 22 indicating that underestimation of central pressure in non-invasive studies may be specific to use of a generalized transfer function derived at rest. The present study used low-pass filtering via a N-point moving average to derive central pressure non-invasively rather than using a generalized transfer function. Whilst exercise was associated with modulation to the shape of the radial pressure wave, whether exercise potentially modulates the degree of filtering required accurately to derive central pressure is unknown.
The persistence of BP-lowering effects following a missed dose of BP-lowering medication, which mimics lack of compliance to treatment, is another important treatment consideration. 28 For sportsmen and very active individuals, the effects of a missed dose on the changes in BP during exercise are of particular clinical importance, given the relationship between exercise-induced rises in SBP and adverse clinical outcomes.1–4 The current study suggests that the beneficial effects of BP lowering with valsartan or aliskiren were maintained following a missed dose, even during the stress induced by vigorous exercise. This finding is consistent with data from the ASSERTIVE study, which compared the effect of aliskiren and telmisartan on BP after a one-week treatment withdrawal.29,30
The present study has a number of limitations, which should be addressed. This was a small study with an exploratory objective to investigate the influence of RAS-blocking treatment on the exercise-induced rise in central pressure. As such it was not powered to demonstrate differences in central pressures or related haemodynamic parameters between the two different treatments used in the study. Similarly, the study was not powered to investigate the response of central pressure elevation to exercise by age, gender or height. Nevertheless, our study was well powered to show changes in both brachial and central blood pressure and amplification in response to exercise and the data are consistent with previously published reports. However, this is the first study to report the effects of BP-lowering treatment on exercise-induced pressure amplification change. As such it was not possible, a priori, to calculate the necessary sample size required should a change in the amplification response to exercise become apparent – especially one that trended in the opposite direction to what many might have predicted. An indicative, retrospective power calculation indicates that the study would have required 77 participants to demonstrate a significant decrease in systolic pressure amplification and a sample size of 115 to show a significant change for the difference between brachial and central pressure with exercise between baseline and end of treatment. This information will be useful for calculating statistical power for future studies of this kind. We focused on systolic pressure amplification rather than pulse pressure. Although diastolic pressures were measured at rest and during exercise, the investigators noted that the measurement of DBP by auscultation (Korotkoff phase IV) during exercise was problematic due to noise and movement, and less reliable than systolic pressure recordings. Moreover, other workers have reported rhythmic variations in pulse pressure associated with exercise, particularly upright dynamic exercise.31,32 We therefore elected to focus our data analysis on systolic pressure. Undertaking detailed physiological studies during exercise is complex. Despite the small numbers, our findings clearly demonstrate that BP lowering does not enhance exercise-mediated pressure amplification. If anything there was a trend to the opposite direction, that is, towards an attenuation in exercise-mediated amplification. Importantly, these data were recorded within the rigorous context of a randomized clinical trial of BP lowering.
In conclusion, this study reports for the first time that BP lowering treatment, at least with the RAS-blocking drugs tested here, did not directly influence the relationship between aortic and brachial pressure at rest and during exercise, other than through proportionate lowering of both pressures. Further work is needed to better understand the mechanisms underpinning aortic–brachial pressure amplification during exercise.
Footnotes
Acknowledgements
The authors thank Michael Ulrich (Novartis Pharma AG, Basel, Switzerland) for providing project management support.
Conflict of interest
BW is a National Institute for Health Research (NIHR) Senior Investigator and is supported by the NIHR UCL Hospitals Biomedical Research Centre. BW has received research funding from Novartis Pharma AG. FB, JB and PB are employees of Novartis Pharma AG and are thus eligible for Novartis stock and stock options. PSL has no conflicts of interest to declare.
Funding
This work was supported by Novartis Pharma AG, Basel, Switzerland as part of the Aliskiren Global Clinical Development programme.
Study investigators
Dr R Cifkova, Dr J Belohlavek and Dr P Vodnansky (Czech Republic); Dr A Kalina, Dr G Balogh and Dr Z Zilahi (Hungary); Dr KK Poh and Dr RS Tan (Singapore).