
Abstract
Background:
Angiotensin-converting enzyme inhibitors (ACEis) improve survival; however, their effect on erythropoiesis remains a matter of debate in this population. Since insertion/deletion (I/D) polymorphism of the angiotensin-converting enzyme (ACE) gene largely influences serum ACE activity, its effect on erythropoiesis is also anticipated.
Method:
In this multicentre, cross-sectional study of 660 patients on maintenance haemodialysis, we analysed the effect of ACEi use and ACE gene I/D polymorphism on haemoglobin levels and erythropoietin resistance. Patients were allocated in groups based on genotype and ACEi therapy. We identified 128 matched pairs with I/I and D/D genotypes.
Result:
There was no difference in haemoglobin levels between genotype groups. Haemoglobin levels were lower in patients on ACEi therapy in the entire cohort (95.5±12.1 g/l vs 97.4±13.4 g/l, p=0.02) and patients with I/D (95.2±11 g/l vs 98.2±11.9 g/l, p=0.04) and D/D (93.3±13.2 g/l vs 97.4±14.2 g/l, p=0.02) genotypes. In patient pairs treated with ACEi therapy, subjects with D/D genotype had lower Haemoglobin level (93.0±12.8 g/l vs 98.2±11.9 g/l, p=0.006) and higher erythropoietin resistance index (ERI) (199.1 vs 175.0, p=0.046) than individuals with I/I genotype.
Conclusion:
These results indicate that ACEi therapy may increase erythropoietin resistance and worsen erythropoiesis in haemodialysis patients with the D allele.
Keywords
Introduction
With the progression of chronic kidney disease, the prevalence of anaemia increases 1 mainly due to the impaired renal production of erythropoietin as well as the negative effects of the uraemic milieu on bone marrow function. Up to 10% of patients respond insufficiently to recombinant human erythropoietin (rHuEpo) due to high erythropoietin resistance in particular. Several well known factors, including vitamin and iron deficiencies, hyperparathyroidism and chronic inflammation contribute to the increased erythropoietin resistance, and the list has not been completed.2,3 Managing this resistance is one of paramount importance, because both anaemia and high delivered dose of rHuEpo have been associated with an increased mortality.4–7
The role of the renin-angiotensin system in erythropoiesis was gradually revealed over the past decades.8–10 Early in vitro studies proved that AT-II (angiotensin-II) could accelerate iron incorporation in erythrocytes accompanying an accelerated erythropoiesis. 11 Angiotensin-converting enzyme (ACE) may be implicated in the regulation of haematopoietic stem cell proliferation leading to accelerated stem cell mitosis and further differentiation to erythroid progenitors.12,13 Angiotensin–II type 1 receptor (AT1R) was found on the surface of erythroid progenitor cells, 14 and the AT-II stimulatory effect on erythropoiesis could be reversed by the AT1R-blocker, losartan. 15 Angiotensin increases erythropoietin production due to renal hypoxia in the preclinical model of 1967. 16 Later research proved this result in healthy human volunteers. What is more, the haemopoietic effect of AT-II could be blocked by AT1R blockers,17,18 ACE inhibitor (ACEi) therapy decreased the serum AT-II level resulting in decreased serum erythropoietin concentration in healthy volunteers which was reversible after withdrawal of ACEi drugs. 19 Increased AT1R expression on erythroid progenitor cells was also detected in kidney transplant patients with post-transplant erythrocytosis syndrome 20 and reducing the AT-II level by ACEi can induce apoptosis of erythroid precursors in post-transplant erythrocytosis syndrome. 21 Consequently, ACEi and also AT1R blockers have been become a standard therapy for this syndrome.22,23 There are also some common intracellular signals induced by AT-II and erythropoietin.24,25 In addition, inhibition of ACE was shown to reduce serum level of other erythropoiesis-stimulating factors such as insulin-like growth factor-1 and interleukin 12.26,27 Inhibition of the renin-angiotensin system has been reported to slow down the rate of erythropoiesis resulting in anaemia in a variety of clinical conditions28–32 or to increase rHuEpo requirements in dialysis patients.33,34 However, others could not confirm these results in chronic dialysed patients.35,36 The ACE gene insertion/deletion (I/D) polymorphism highly influences the serum concentration of ACE enzyme. This polymorphism is one of the factors most responsible for a wide interpersonal variability of serum ACE concentration. Individuals with the D allele have significantly higher serum ACE concentration than subjects with the I allele.37,38 Some studies found that the ACE gene I/D polymorphism was associated with erythropoietin resistance39–42 while others could not prove this relationship. 43
In our study, we hypothesised that the ACE gene I/D polymorphism has an impact on the effect of ACE inhibitor therapy on erythropoiesis. In a retrospective cohort of haemodialysis patients, we examined whether the D/D genotype was associated with higher haemoglobin and/or with lower erythropoietin requirements and if pharmacological inhibition of ACE can impair erythropoiesis. Furthermore, we examined the combined effect of ACE gene I/D polymorphism and ACEi therapy on erythropoiesis in haemodialysed patients.
Subjects and methods
Eleven dialysis centres of B. Braun Avitum Hungary CPLC participated in this Hungarian cross-sectional multicentre observational Angiotensin-converting enzyme gene B. Braun Avitum Hungary CPLC Dialysis Network (ACEGENE-BB_HU) study in 1997. Patients of Caucasian origin who were on maintenance haemodialysis for more than three months and consented for genotyping were enrolled in the study. Samples from 716 patients were genotyped. We further excluded 56 patients with severe liver disease, active malignancies and haemorrhagic or haematologic diseases from statistical analysis because these disorders may influence the haematological status. The remaining primary cohort included 660 patients, who were allocated into three subgroups based on their genotype (I/I, I/D and D/D). For secondary analysis, we identified matching pairs of patients with I/I and D/D genotype and I/D heterozygotes were not included in the secondary analysis. Matching variables were gender, age, time on dialysis (the following groups were created: less than 12 months, 12–35 months, 36–59 months, more than 60 months), diabetes and the actual use of any ACEi therapy. 127 pairs were identified. Age was not a strict matching variable because it had no significant impact on haemoglobin level. However, we strove to match patients with similar age. As a result, 90% of the pairs had similar age (±15 years) and in the case of 10 pairs there were higher range (16–39 years).
Demographic data including age, gender, dialysis vintage, cause of end-stage kidney disease, diabetes status, use of ACEi as well as laboratory data and rHuEpo dose were extracted from local database.
Ethylenediaminetetraacetic acid (EDTA) samples were collected before dialysis and DNA was isolated from peripheral blood leukocytes by standard non-enzymatic method. Genotyping of the I/D single nucleotide polymorphism in intron 16 of the ACE gene was carried out using the conventional technique. 38 Epoetin alfa was used exclusively as rHuEpo. Erythropoietin resistance index (ERI) was calculated from the monthly rHuEpo dose (prescribed in the months of blood sampling), divided by the haemoglobin (g/l) level.
Parameters following normal distribution were reported using mean and standard deviation (SD). Parameters with non-normal distribution, such as rHuEpo dose, time on dialysis and ERI were reported using median and lower–upper quartiles (Q1–Q3). Differences between two independent groups were compared using Student’s t-test and Mann-Whitney test. Genotype groups (I/I, I/D and D/D) were compared using one-way analysis of variance (ANOVA) (Tukey’s test used for post-hoc analysis) or Kruskal-Wallis tests for continuous variables and z-test for categorical variables. Haemoglobin as a dependent variable was tested in univariate, multivariate linear regression and GLM-analysis (General Linear Model) of covariance model. For the comparison of patient’s pairs (I/I versus D/D genotype), the dependent samples t-test, the Wilcoxon matched pairs test were used, as appropriate. The statistical analysis was performed by STATISTICA software package (version 10, Tulsa, Oklahoma, USA).
All patients gave written consent to the genetic testing and data collection. The study was approved by the local and central ethical committees and it was financially supported by the Hungarian Scientific Research Fund (OTKA, TO23927). This research adhered to the principles of the Declaration of Helsinki.
Results
Characteristics of patients are summarised in Table 1. The proportions of patients with I/I, I/D and D/D genotypes were 20%, 41.5%, and 38.5%, respectively. In the whole cohort, male gender was more prevalent (51.7% vs 48.3%), mean age was 54.5±16.5 years and patients were on dialysis therapy for two years (23.8 months (11.2–46.6)). ACE inhibitor therapy was prescribed for 48.3% and rHuEpo therapy for 80.6% of all patients. The most frequent cause of end-stage renal disease was coded as glomerulonephritis in the patient registry, followed by tubulointerstitial nephritis, diabetes, polycystic kidney disease and hypertension. There were no differences in demographic or laboratory parameters and rHuEpo doses between the three genotype groups. Haemoglobin levels were comparable in the genotype groups, and also the proportion of patients receiving rHuEpo therapy and rHuEpo doses was similar. The proportion of patients receiving ACEi therapy was also similar in the genotype groups. The only significant differences were detected in haemoglobin levels (95.5±12.1 g/l vs 97.4±13.4 g/l, p=0.02) and frequency of rHuEpo therapy (86.2% vs 75.4%, p=0.01) between patients with ACEi therapy and without ACEi therapy (Table 1). When we further analysed this association in different genotype groups, we found that haemoglobin levels in patients not receiving ACEi therapy were higher in patients with I/D genotype (95.2±11 g/l vs 98.2±11.9 g/l, p=0.04) and D/D genotype (93.3±13.2 g/l vs 97.4±14.2 g/l, p=0.02), but this difference was not found in patients with I/I genotype (97.9±11.6 g/l vs 95.9±14.9 g/l, p=0.39). We observed a trend towards decreasing haemoglobin levels in I/D and D/D genotype groups among patients receiving ACEi therapy (Figure 1).
Demographic and laboratory characteristics of patients based on genotype and angiotensin-converting enzyme inhibitor (ACEi) therapy.

ACE: angiotensin-converting enzyme; D: deletion; ERI: erythropoietin resistance index; I: insertion; IQR: interquartile range; rHuEpo: recombinant human erythropoietin; SD: standard deviation.

Effect of angiotensin-converting enzyme inhibitor (ACEi) therapy on haemoglobin levels in patients with different angiotensin-converting enzyme (ACE) gene insertion/deletion (I/D) genotype. Analysis of variance (ANOVA) using Tukey’s test for statistical comparisons of groups.
In univariate linear regression models, higher haemoglobin levels were associated with male gender, longer dialysis vintage and ACEi therapy. In addition to these parameters, diabetes emerged as an additional predictor in our multivariate model. The ACE gene I/D polymorphism (I/I and I/D-D/D) and age were not associated with haemoglobin levels (Table 2).
Uni- and multivariate linear regression models with haemoglobin as dependent variable.
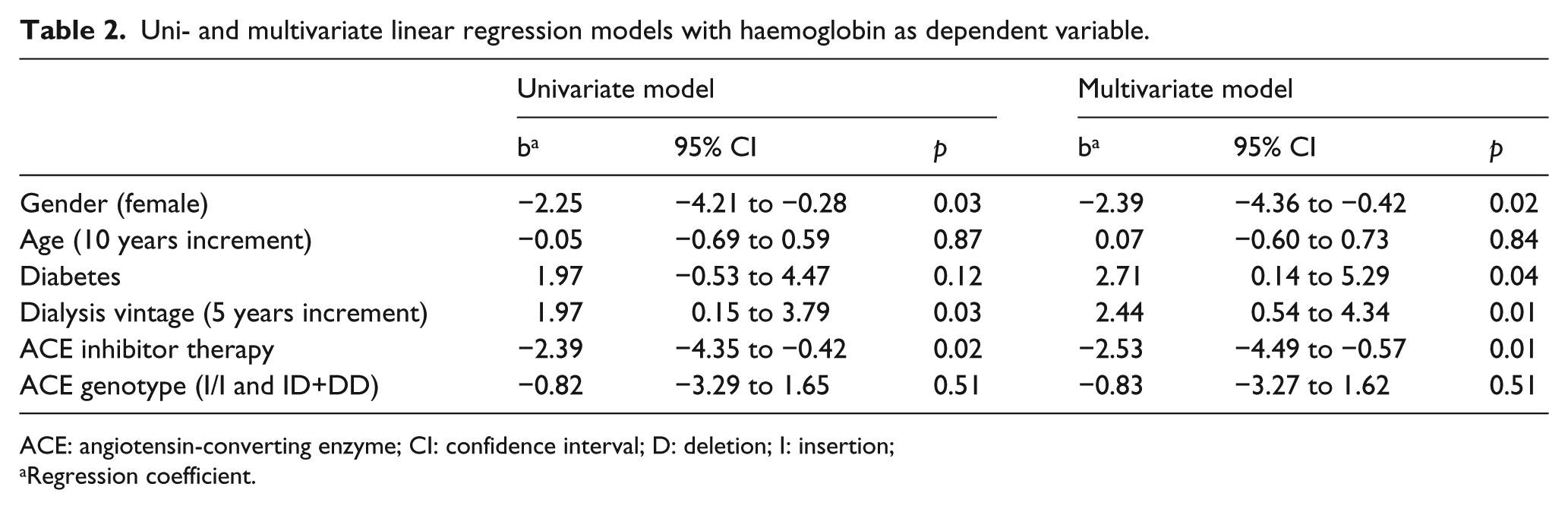
ACE: angiotensin-converting enzyme; CI: confidence interval; D: deletion; I: insertion;
Regression coefficient.
In order to further clarify the effects of ACEi therapy on haemoglobin levels of patients with different genotypes we analysed the combined effect of ACEi therapy and ACE I/D polymorphism on haemoglobin in an analysis of covariance (ANCOVA) model including dialysis vintage as additional covariant factor as well. In this model, neither ACEi therapy nor ACE gene I/D polymorphism had significant impact on the haemoglobin level (p=0.53 for both variables). However, the ANCOVA model and also the multivariate regression model revealed significant interaction (p=0.02) between ACEi therapy and ACE I/D polymorphism.
Since we detected several additional interactions between predictor variables, namely gender, dialysis vintage, diabetes, ACE I/D polymorphism and ACEi therapy, we decided to use matched-pair analysis in order to control for those potential confounders. We identified 127 matched pairs from I/I and D/D genotype groups based on gender, age, dialysis vintage, diabetes status, ACEi therapy. Compared to the entire cohort, mean age (54.7±14.5 vs 54.5±16.5 years), dialysis vintage (28.1 (13.4–47.9) vs 23.8 (11.2–46.6)), proportion of male subjects (54.3% vs 51.7%), the prevalence of diabetes (17.3% vs 19.5%) and ACE inhibitor use was similar (51.2% vs 48.3%) in the paired subcohort. Also, haemoglobin levels (96.4±13.0 g/l vs 96.3±12.8 g/l), monthly rHuEpo doses (18,000 (13,000–24,000) vs 16,000 (13,000–22,000)) and ERI values (190.9 (130.8–242.4) vs 181.0 (133.3–241.0)) were similar (Table 1).
In the subgroup of 127 pairs, patients were further grouped based on ACEi treatment status. In pairs not receiving ACEi therapy (62 pairs), monthly rHuEpo doses (18,500 (14,500–20,000) IU/month vs 18,000 (12,000–20,000) IU/month, p=0.73) and haemoglobin levels were comparable (95.6±14.1 g/l vs 99.0±12.8 g/l, p=0.14). ERI was not different in the two genotype groups (202.0 (137.2–243.2) vs 177.8 (122.4–225.0), p=0.59). In contrast, among patients receiving ACEi therapy (65 pairs), D/D genotype was associated with lower haemoglobin levels (98.2±11.9 g/l vs 93.0±12.8 g/l, p=0.006) and higher ERI (175.0 (116.5–233.0) vs 199.1 (147.9–250.0), p=0.05) compared to those with I/I genotype, while rHuEpo doses were similar in both groups (16,000 (12,000–24,000) vs 17,000 (14,000–24,000), p=0.16). (Table 3).
Comparison of haemoglobin, recombinant human erythropoietin (rHuEpo) dose and erythropoietin resistance index (ERI) between genotype pairs in patients with respect to angiotensin-converting enzyme inhibitor (ACEi) therapy.

ACE: angiotensin-converting enzyme; D: deletion; I: insertion; SD: standard deviation.
Discussion
In this cross-sectional study among Caucasian patients on maintenance haemodialysis, we found that ACEi therapy modifies the effect of ACE gene I/D polymorphism on erythropoiesis. Our results suggest that in patients with D/D genotype or with D allele, the pharmacological inhibition of ACE enzyme can increase erythropoietin resistance and worsen erythropoiesis. We did not find any direct association between erythropoietin resistance and ACE gene I/D polymorphism alone. To our knowledge, this is the first study examining the combined effect of ACE gene I/D polymorphism and ACEi therapy on erythropoiesis in Caucasian dialysis patients.
These results might provide possible explanations for the conflicting findings in earlier studies regarding ACEi therapy and erythropoietin resistance in dialysis patients. While some studies reported negative effect of ACEis on erythropoietin resistance and anaemia in haemodialysis43–46 others could not demonstrate this relationship.35–50 In our entire cohort, ACEi use was associated with lower haemoglobin levels; however, we did not observe this relationship in the subcohort of patients with II genotype of the ACE gene. ACE inhibition was associated with increased erythropoietin resistance in patients with D/D or I/D genotypes only (Figure 1).
The detected effect of ACE inhibition on haemoglobin levels in patients with D/D genotype in our study was also clinically relevant. While 42.1% of patients on ACE inhibitor therapy reached treatment target of haemoglobin>100 g/l in the I/I group, only 27% of patients with D/D genotype achieved this goal (p=0.05) (data not shown).
Serum and tissue ACE activity and AT-II levels are greatly influenced by ACE gene I/D polymorphism: individuals with the D/D allele have the highest activity of ACE. 37 In our model, the presumably relative greater fall in AT-II levels and endogenous EPO production as a response to ACEi therapy in patients with D/D genotype resulted in lower haemoglobin levels and higher exogenous rHuEpo requirement (also perceived as higher erythropoietin resistance) compared to patients with I/I genotype.
Lower rHuEpo dose requirement was associated with the D/D genotype in patients on peritoneal dialysis in the United Kingdom in two studies by Varagunam et al. and Sharples et al.39,41 These findings are in agreement with our model in the sense that D/D genotype is associated with higher AT-II levels, an important stimulus of erythropoiesis and also higher endogenous erythropoietin levels. 43 Therefore, lower exogenous rHuEpo doses were required to achieve treatment targets in patients with D/D genotype. However, those patient populations might be very unlike our cohort because of the different dialysis modality, likely significant residual renal function and lower level of chronic inflammation. In addition, a greater proportion of our patients received ACEi therapy compared to those studies.
Among haemodialysis patients in Korea, Jeong et al. 42 demonstrated lower erythropoietin resistance in patients with D/D genotype compared to I/D or I/I genotypes. Although we also observed a trend towards higher haemoglobin levels and lower erythropoietin resistance in our matched patients with D/D genotype compared to I/I genotype not receiving ACEis, this was statistically not significant. Differences in allele frequencies between races and the – not documented – distribution of patients with ACEi therapy among genotype groups in the referred study could be potential explanations for this discrepancy.
There are a number of limitations to this study: (a) because of the cross-sectional nature of our study, we could not detect temporal changes of haemoglobin levels, rHuEpo doses and prescription of ACE inhibitors; (b) in addition, we did not capture several potential confounders, such as chronic inflammation, iron status and iron therapy, parathyroid hormone levels, residual kidney function, dialysis dose, previous kidney transplant and use of immunosuppressive medication, smoking habits or alcohol consumption that all are likely to affect erythropoiesis in haemodialysis patients; (c) furthermore, we did not measure serum erythropoietin and AT-II levels or ACE activity: these might have helped in understanding the pathophysiological background of our results, but are unlikely to affect the explored associations; (d) patients were on a wide variety of ACEis and we did not capture its type, dosage or length of treatment: however, very few studies included those data in the analysis, and we are confident that including ACEi treatment pattern in the analysis would not impact our main findings; (e) many patients fell out when using our paired model in the secondary analysis and this might have distorted results; however, we think that this sub-cohort was representative for the entire study population; (f) more importantly, since we included only patients of Caucasian origin into our database, our results might not be generalisable to patients of other races.
Despite those limitations, our results might have clinical implications concerning the management of renal anaemia. About 5–10% of patients on haemodialysis receiving rHuEpo have high erythropoietin resistance. If ACEi treatment can be a contributing factor to the resistance, a trial of holding ACEi therapy could potentially result in increased erythropoiein response in some patients, likely those with D allele in their ACE gene.
Conclusions
We confirmed that the variable effect of ACE inhibition on erythropoiesis is linked to the polymorphism of the ACE gene. ACEi therapy in patients with the D/D genotype or D allele resulted in lower haemoglobin levels and higher erythropoietin resistance compared to patients with the I/I genotype. Our study might provide an additional argument for individualised therapies in the future, when detecting genetic polymorphisms might be part of personalised management of end-stage renal disease patients.
Footnotes
Acknowledgements
The authors thank András Paksy for his invaluable help in the statistical analysis.
ACEGENE-BB_HU Workgroup’s collaborators from B. Braun Avitum Hungary CPLC Dialysis Network: Attila Benke (Veszprém), Béla Borbás (Debrecen), Sándor Ferenczi (Győr), Mária Hengsperger (Mátészalka), Szilvia Kazup (Siófok), Lajos Nagy (Tatabánya), József Németh (Dunaújváros), Antal Rozinka (Kisvárda), Tamás Szabó (Kistarcsa), Tamás Szelestei (Kaposvár), Eszter Tóth (Békéscsaba, Gyula), Gábor Varga (Ajka), Gyula Wágner (Szekszárd), Gábor Zakar (Székesfehérvár).
Conflict of interest
None declared.
Funding
The authors wish to thank Csaba Szalay for the determination of the ACE gene polymorphism, which was funded by the Hungarian Scientific Research Fund (OTKA, TO23927/1997). This work was also supported by B.Braun Avitum Hungary CPLC Dialysis Network.