
Abstract
Objective:
The M235T polymorphism in the angiotensinogen gene has been reported to be associated with the development of atrial fibrillation (AF).However, results from observational studies are conflicting.
Methods:
PubMed, google scholar and China National Knowledge Infrastructure database(2000.1–2013.4) were searched for eligible articles; four separate studies with 2580 subjects on the relationship between M235T polymorphism and AF were analyzed by meta-analysis. The associations between M235T polymorphism and AF risk were estimated by pooled odds ratio (OR) and 95% confidence interval (CI) using a fixed or random-effects model.
Results:
There was a significant association between M235T polymorphism and AF. The pooled OR for the recessive model in the total population was 2.17 (95% CI: 1.39–3.38, I2=0%). In a subgroup analysis by nationality, the pooled OR for TT vs. MM genotype was 0.55 (95% CI: 0.32–0.95, I2=0%) and the pooled OR for the recessive model was 1.86 (95% CI: 1.08–3.20, I2=0%) in Asians.
Conclusions:
The current meta-analysis suggested that the M235T polymorphism in the angiotensinogen gene might be related to the increased risk of AF in Asians. Conclusive evidence on the effects of the variants in AF should be addressed in further studies.
Introduction
Atrial fibrillation (AF) is a common and serious disorder in clinical practice and is associated with increased cardiovascular morbidity and mortality.1,2 The incidence of AF is increasing. It now affects more than 5% of individuals over 65 years of age in Western countries. AF is most likely a result of a combination of lifestyle and environmental factors. The major risk factors for development and persistence of AF are age, heart disease, high blood pressure, lung disease, hyperthyroidism, family history, caffeine intake, psychological stress, fatigue and high-dose steroid therapy. Epidemiological observations and genome-wide association studies (GWAS) have revealed a number of genetic variants that predispose to AF, most of which have been observed or are presumed to affect the atrial action potential duration. 3
The renin–angiotensin system (RAS) has been shown to be involved in many cardiovascular diseases, including myocardial fibrosis and hypertrophy in hypertensive heart disease, 4 myocardial infarction, 5 cardiomyopathy 6 and congestive heart failure. 7 Experimental investigation shows that AF is associated with RAS activation in the atria in a human and dog model.8,9 A recent study suggested that inhibitors of the RAS may reduce the risk of new-onset AF,10,11 indicating that the RAS may be involved in the pathogenesis of atrial structural and electrical remodeling. The RAS seems to be involved in the genesis of arrhythmia by the following two mechanisms: the induction of AF and structural remodeling by mitogen-activated protein kinase (MAPK) expression, and reduction of collagenase activity and the induction of electrical remodeling by shortening of the atrial effective refractory period (AERP) and of the action potential duration. 12
Angiotensinogen (AGT) is an important component of the RAS. The AGT gene M235T polymorphism (a methionine to threonine amino acid substitution at codon 235, designated the M and T alleles) has been reported to elevate the serum level of AGT. 13 To date, while several studies have found an association between M235T and AF, other have not, suggesting that it may serve as a possible risk factor for AF. However, this specific association remains controversial. The present meta-analysis was performed in order to determine a more precise estimation of the associations between the M235T polymorphism in the angiotensinogen gene and AF.
Materials and methods
Literature search strategy
All case-control studies of M235T polymorphism and AF risk published up to 1 April 2013 were identified through systematic searches in PubMed, google scholar and China National Knowledge Infrastructure (CNKI) databases. No limits were applied for language, and foreign literature was translated. The search terms used were: ‘M235T’, ‘atrial fibrillation/AF’, ‘angiotensinogen/AGT’ and ‘gene polymorphism’. For each article identified, a manual search of the relevant references was also performed within a range of published years from 2000–2013. The reference lists of major textbooks, review articles, and of all the included articles identified by the search were then individually searched to find other potentially eligible studies.
Inclusion and exclusion criteria
A study was included in the meta-analysis if it satisfied the following criteria: 1) evaluation of the association of M235T polymorphism and AF; 2) AF was defined as irregular and uncoordinated atrial electrical activity on surface electrocardiogram and(or) holter monitoring; 3) studies that included sufficient genotype data for extraction. Studies were excluded when: 1) they were not case-control studies that evaluated the association between M235T polymorphism and AF risk; 2) they were based on incomplete raw data and no usable data were reported; 3) they were case reports, letters, reviews, and editorial articles; 4) the studies contained duplicated data.
Data extraction
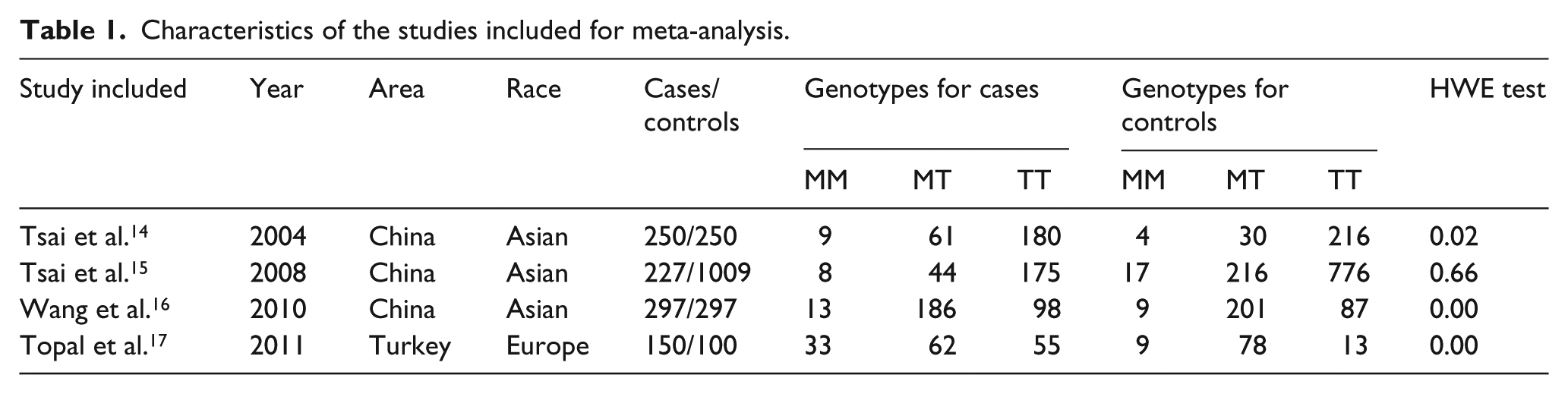
According to a standard protocol, the data were independently collected in duplicate by two doctors (HuiXuan Wang and Yi Teng), and disagreements were discussed to reach a consensus. The information extracted from each study included the first author, year of publication, region, race, number of genotypes, total number of cases and controls, and evidence of Hardy–Weinberg equilibrium (HWE) in controls (see Table 1).
Characteristics of the studies included for meta-analysis.
Statistical analysis
We assessed HWE in the controls for each study using χ2 test, and a p<0.05 was considered as significant disequilibrium. The strength of the association between AF and the M235T polymorphism was estimated using odds ratios (Ors) and the corresponding 95% confidence intervals (CIs). The pooled ORs were performed for a co-dominant model (TT vs. MM, TT vs. MT), a dominant model (MM+MT vs. TT), and a recessive model (TT+MT vs. MM). Q test and I2 test was performed to quantify the proportion of the total variation due to heterogeneity. I2 ranges from 0–100%. A value of 0% indicates no observed heterogeneity, and larger values reflect increasing heterogeneity, with 25% regarded as low, 50% as moderate, and 75% as severe heterogeneity. When the effects were assumed to be homogeneous (p>0.1, I2<50%), the fixed-effects model was used. Otherwise, the random-effects model was more appropriate. To evaluate ethnicity-specific effects, subgroup analyses were performed to explore and explain the diversity among the results of different studies. Since only one study was performed in Europe, the result of subgroup analysis by ethnicity may not be reliable for Europeans. Sensitivity analysis was performed through random-effect model values compared with the fixed effect. The funnel plot asymmetry was assessed by Begg’s test to estimate potential publication bias (p<0.05 was the representative of statistical significance). The statistical analyses were performed using the STATA 10.0 software (StataCorp, College Station, TX). To ensure the reliability and the accuracy of the results, two reviewers (Ke Wang, ZhengWu Xia) populated the data in the statistic software programs independently and got the same results.
Results
Study characteristics
As a result of the literature search and screening 257 papers were retrieved, of which four eligible studies concerning the association between AGT M235T polymorphism and risk of AF were identified for this meta-analysis.14–17 The data of the four studies were gathered from 924 AF patients and 1656 controls (Figure1 and Table1), containing the case-control studies of three Asian and one European population. The genotype distributions among the controls of all studies were not consistent with HWE except for one study. 15 Of the four included studies, one paper used population-based controls 17 and three papers used hospital-based controls.14–16

Flow diagram of study searching and selection process.
Quantitative synthesis
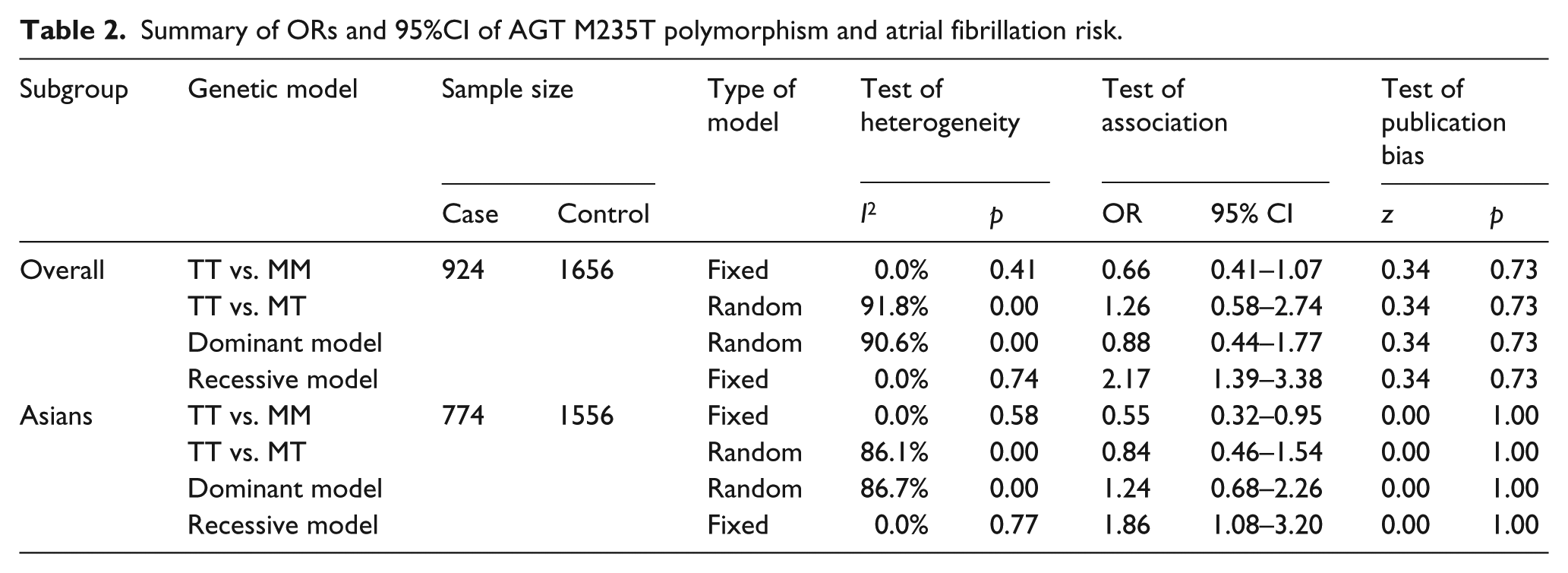
A summary of the meta-analysis findings of the association between M235T polymorphism and AF risk is shown in Table 2. The meta-analysis results showed significant associations between M235T polymorphism and AF risk (the recessive model: OR=2.17, 95% CI=1.39–3.38, I2=0%). In the subgroup analysis by nationality (Figure 2), studies were divided into Caucasian and Asian populations. Since only one study was performed in Caucasian patients, the result of subgroup analysis by ethnicity may not be reliable for Caucasians. Other results confirmed that there were significant associations between M235T polymorphism and AF risk in Asians (TT vs. MM: OR=0.55, 95% CI 0.32–0.95, I2=0%; the recessive model: OR=1.86, 95% CI=1.08–3.20, I2=0%). Sensitivity analysis was performed through random-effect model values compared with the fixed effect, and the analysis did not alter the significance of the final results, which indicated that the previous data were robust and authentic.
Summary of ORs and 95%CI of AGT M235T polymorphism and atrial fibrillation risk.
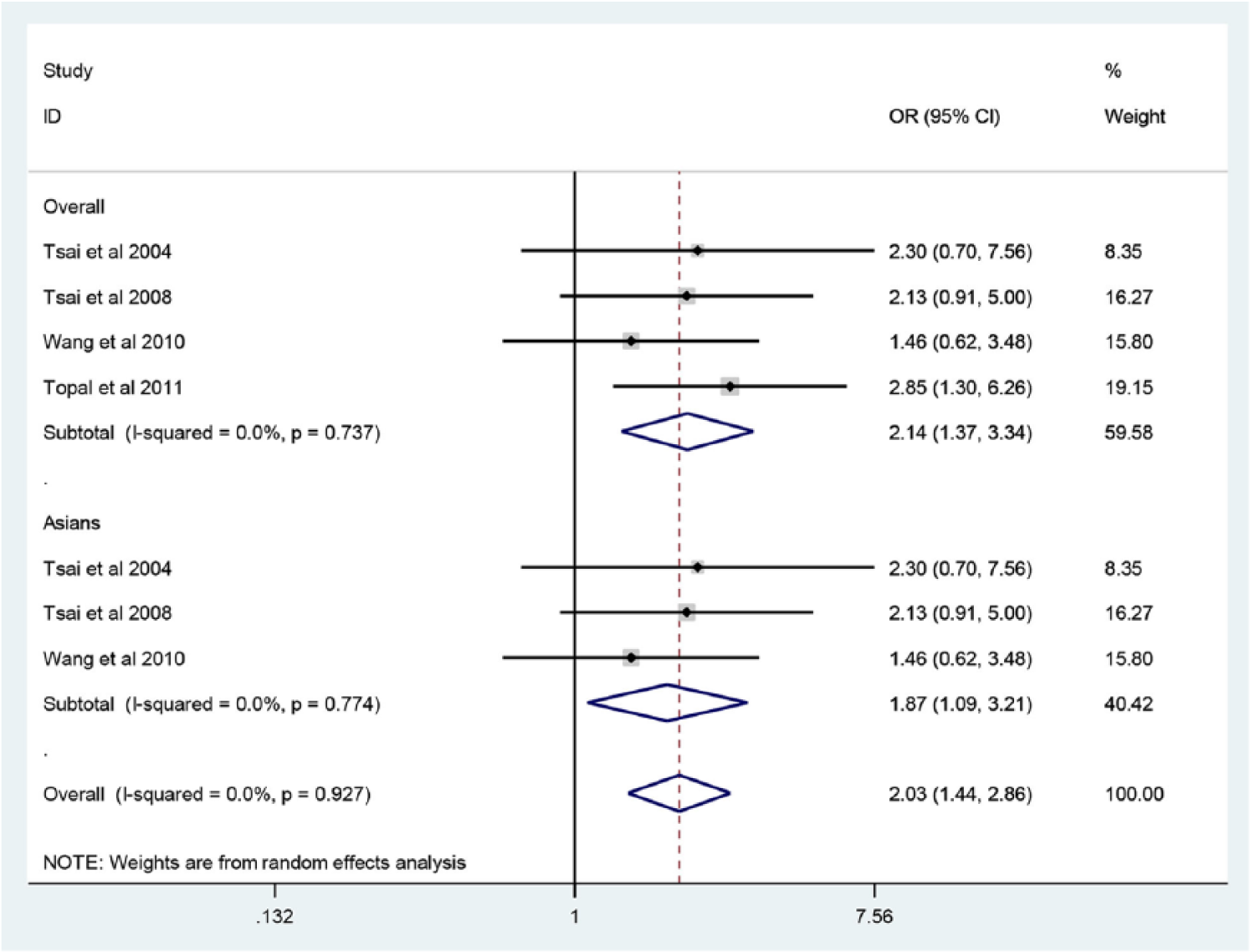
Meta-analysis of the relationship between the M235T polymorphism and atrial fibrillation risk using a recessive model.
Heterogeneity analysis and publication bias
The funnel plot and Begg’s test was used to assess the publication bias. There was no evidence of publication bias visually from the funnel plot (p>0.05, Table 2), which implied that the publication bias was low in the present meta-analysis (Figure 3).

Begg’s funnel plot test of publication bias for the association of the M235T polymorphism with AF risk using a recessive model.
Discussion
To the best of our knowledge, this is the first meta-analysis of the comprehensive assessment of the relationship between the AGT gene M235T polymorphism and the risk of AF. To date, although several studies have evaluated the association between the AGT gene M235T polymorphism and AF, the association remains poorly understood. Tsai et al. were first to report reported the association between M235T polymorphisms and AF; a total of 250 patients with AF and 250 controls were selected in the study, and they found that patients who have M235T polymorphism may be more liable to develop AF. 14 However, this study was in a Chinese population, and it may be not applicable to other ethnic groups. Later, several studies, but not all, have found the association of M235T polymorphism with increased risk for AF. Furthermore, as these results above were based on a small number of samples, it is possible that the observed associations reflect chance observations rather than true associations.
To help clarify these controversial findings, we performed a meta-analysis to obtain a more comprehensive result by combining comparable studies, so increasing the sample size and statistical power. In the present meta-analysis, we quantitatively assessed the association between M235T polymorphism and AF risk. All relevant studies published in any language were included in the meta-analysis, which would reduce language bias. Four studies were finally included, with a total of 924 AF patients and 1656 controls. The pooled OR for the recessive model was 2.17 (95% CI: 1.39–3.38, I2=0%). Because of the difference in genetic backgrounds and the environment in which the subjects lived, we performed an ethnicity-specific subgroup analysis; the pooled OR for TT vs. MM genotype was 0.55 (95% CI: 0.32–0.95, I2=0%) and the pooled OR for the recessive model was 1.86 (95% CI: 1.08–3.20, I2=0%) in Asians, suggesting a significant association between M235T polymorphism and AF in Asians. Since only one study published in Europe was found, we could not perform a stratified analysis in Caucasians. However, it is worth mentioning that Ravn et al. found no relationship between AF and M235T polymorphisms in the Danish general population in a cohort study. 18 The differences in the results might be caused by the difference in the genetic composition of the populations. In addition, gene–gene and gene–environment interactions might explain the differences. Thus the relationship between AF and M235T polymorphisms in Caucasians needs further research.
The meta-analysis suggested that the M235T polymorphism might be related to an increased risk of AF in Asians. The mechanism of how AGT gene M235T polymorphism relates to AF risk is still unclear. Serum AGT levels were shown to be increased within the heart and kidney in subjects carrying the 235T allele, 13 and AGT interacts with renin to produce angiotensin II. Angiotensin II has been shown to trigger the MAPK pathway, 9 which is responsible for the proliferation of fibroblasts and hypertrophy of cardiomyocytes, and is involved in the mechanism of atrial structural and electrical remodeling caused by the occurrence of AF. 19 These results indicate that subjects taking ACE inhibitors and angiotensin receptor blockers may have a better therapeutic effect when carrying the 235M allele, but this is to be confirmed by further experiments. In addition, multiple gene polymorphism (M235T, G-6A, and G-217A) may synergize to increase the overall risk of AF in single-locus analysis. 14
Some limitations of this meta-analysis should be considered when interpreting the results. First, although all cases and controls of each study were well defined with similar inclusion criteria, there may be potential factors that were not taken into account that may have influenced our results. Second, our analysis did not consider the possibility of gene–gene or SNP–SNP interactions, or the possibility of linkage disequilibrium between polymorphisms. Further investigations of the haplotypic effect of a gene and the study of multiple polymorphisms in different genes are needed. In addition, the results of the meta-analysis may be affected by confounding factors, such as gender and age; however, gender-related and age-related subgroup analysis could not be performed because of incomplete data. Finally, three included studies were not in HWE equilibrium; departure from HWE can be explained by natural selection, population admixture, inbreeding, experimental errors and duplication. 20 Unfortunately, the included studies report very limited information to provide any detailed insight into these potential problems. Thus, there is no way to determine for which of the above reasons the violation has occurred.
In conclusion, our study indicates that the M235T polymorphism in the angiotensinogen gene might be related to increased risk of AF in Asians. Due to limitations shown above in this analysis, well-designed studies with large sample sizes are needed to confirm our results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research supported by National High Technology Research and Development program of China (grant # 2011AA02A111).