
Abstract
Introduction:
ABO rs495828 polymorphism has recently been associated with risk of hypertension and cough induced by angiotensin-converting enzyme (ACE) inhibitors, which could be due to low ACE plasma activity. To study whether ABO rs495828 is associated with ACE activity. The association between ABO genotype and phenotype, and differences in ACE activity between the ABO phenotype groups were also studied.
Subjects and methods:
We genotyped 168 subjects for rs495828. ACE plasma activity and ABO histo-blood group were measured in all minor allele homozygous subjects (TT) that agreed to participate in the study (n=8) and in age- and gender-matched heterozygous subjects (GT; n=8) and major allele homozygous subjects (GG; n=8).
Results:
A non-significant trend was found in ACE activity among rs495828 genotype groups; however the polymorphism was significantly associated with ABO phenotype (p=0.007), which in turn was associated with ACE activity (p=0.029).
Conclusion:
These results provide new evidence for the ABO-ACE relationship. Although the genetic marker studied here may be involved somehow, ABO phenotype is shown to be a better predictor of ACE plasma activity.
Introduction
Hypertension is a serious public-health issue worldwide because of its high prevalence (it affects more than a quarter of the world’s adult population) and because it is an important risk factor in cardiovascular and kidney diseases. 1 Hypertension is considered a complex highly heritable trait so that, besides potential environmental risks, multiple genetic factors play a role in its occurrence. 2 Angiotensin-converting enzyme (ACE) is a key protein in the renin-angiotensin system that catalyses the conversion of angiotensin I to angiotensin II, a protein involved in raising systemic blood pressure. Consequently, ACE has become one of the most important targets in hypertension treatment. It is well known that ACE inhibitors (ACEIs) produce more beneficial effects than a simple reduction of blood pressure, which explains their wide use in diverse populations; not only those with hypertension but also those with heart failure, myocardial infarction or stable coronary disease. However, significant heterogeneity exists with regard to the effectiveness and tolerability of ACEIs, which makes pharmacogenetic studies crucial to ensure a safer and more efficacious treatment for patients. ACE and other genes related to the renin-angiotensin system have been frequently considered as candidate genes in both pharmacogenetic and cardiovascular disease risk studies.3,4 Particularly, the insertion/deletion polymorphism in intron 16 of the ACE gene represents the most studied genetic variant, which is strongly associated with ACE plasma activity. 5 This polymorphism has been associated with a wide range of clinical outcomes including cardiovascular diseases, diabetic nephropathy, response to ACEI therapy or excess mortality in patients with type I diabetes.6–8 However, polymorphisms located in other genes indirectly related to ACE have to be taken into account because they can become important prediction markers.
In previous research performed by our group, the rs495828 polymorphism located in the promoter region of the ABO gene was found to be strongly associated with both risk of hypertension and ACE inhibitor-induced cough.9,10 While the T allele was found to be a protection factor for hypertension, the same allele was a risk factor for the cough in patients treated with ACEI. If the T allele gives rise to lower ACE activity, it could lead to lower risk of hypertension and higher bradykinin levels thus triggering the cough in patients treated with ACEI, which would fit with our previous results perfectly (Figure 1). There are very few references to this polymorphism, but it seems to be highly relevant as it has been associated with other features including certain haematological traits 11 and with venous thromboembolism. 12 With the objective of testing the hypothesis that the T allele leads to lower ACE activity, which emerged from our previous studies and has been previously reported in Asian subjects, 13 we examined whether there is an association between the rs495828 polymorphism and ACE plasma activity in a Caucasian population. Moreover, we studied the association between ABO genotype and phenotype (considered as the presence of antigen A or absence of any antigen), and we also compared the ACE plasma activity of the different ABO phenotype groups.
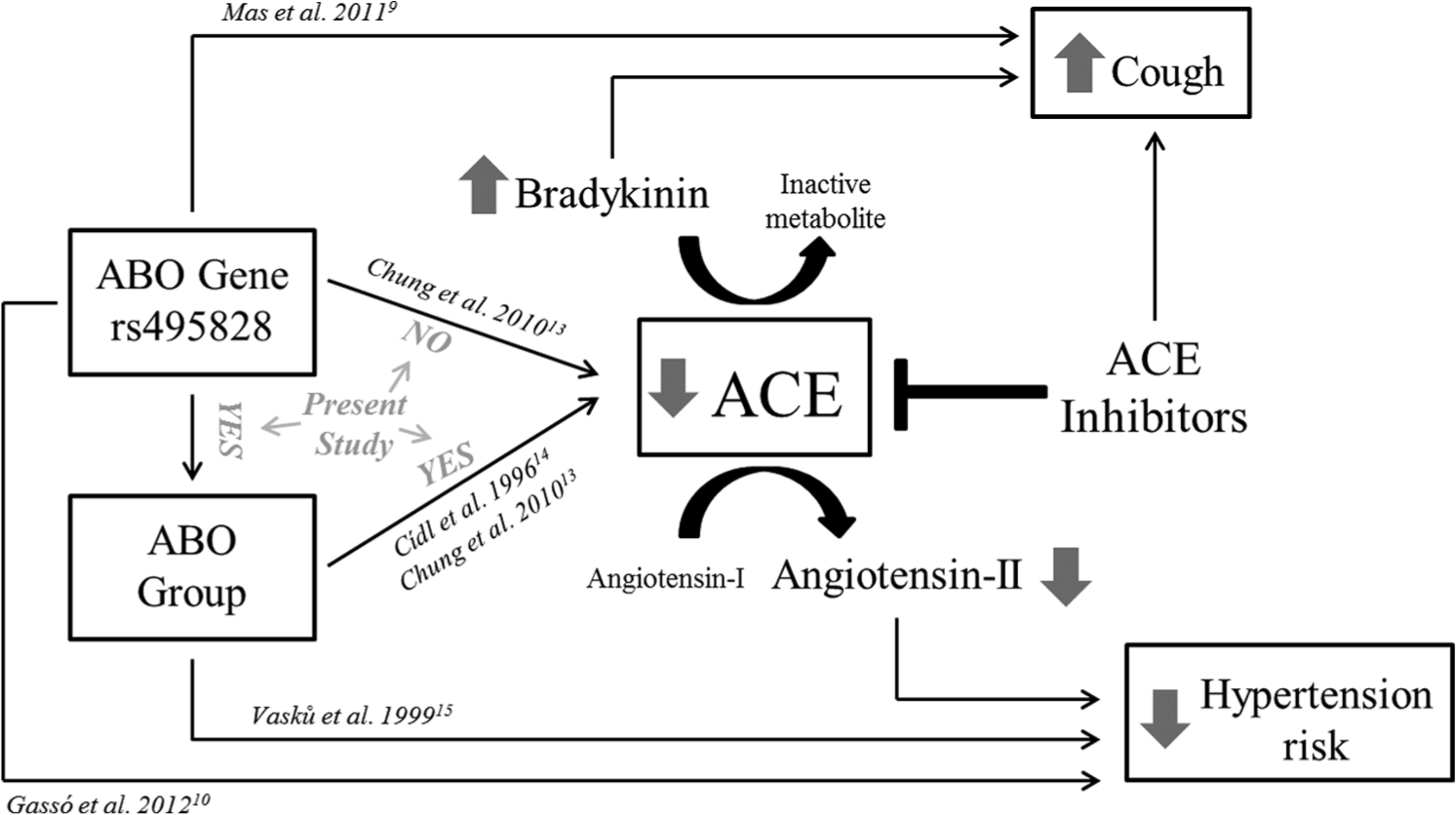
Schematic relationship between ABO, angiotensin-converting enzyme (ACE), risk of hypertension and ACE inhibitor-induced cough.
Subjects and methods
A total of 168 college students (aged between 18–31 years) were recruited at the School of Medicine, University of Barcelona. Each participant answered a questionnaire via an interview, which elicited demographic information including personal medical history. All the study participants were Caucasians. Ethnicity was determined by self-reported ancestries. Written informed consent was obtained from each subject. The study was approved by the hospital’s ethics committee.
Blood samples were collected from the participating individuals in EDTA (K2EDTA BD Vacutainer EDTA tubes; Becton Dickinson, Franklin Lakes, New Jersey, USA) and genomic DNA was isolated using a DNA purification kit (Puregene; Gentra Systems, Indianapolis, Indiana, USA). The DNA concentration was determined by absorbance (ND1000; NanoDrop, Wilmington, Delaware, USA). The rs495828 was genotyped using TaqMan genotyping assay (C__26744830_10; Applied Biosystems, Foster City, California, USA) to detect the genetic variant (G/T, forward strand) in chromosome position 9: 136154867 (NCBI Build 37). A total of 11 minor allele homozygous subjects (TT) were found in our population but it was only possible to engage eight of them in further study. We selected eight major allele homozygous (GG) and eight heterozygous (GT) who were age- and gender-matched with the minor allele homozygous subjects. All 24 participants provided baseline 12-hour fasting blood samples. None of our volunteers were being treated with ACE inhibitors or any other antihypertensive treatment at the time of the study. One subject declined to participate in the final analysis leaving a total of 23 participants with blood samples and genotype information.
The activity of the angiotensin-converting enzyme was assessed by quantifying hydrolysis of the substratum N-[3-(furyl)acryloyl]-L-phenylalanyglycylglycyne to N-[3-(furyl)acryloyl]-L-phenylalanyne and glycylglycine. Hydrolysis was associated with a reduction in absorption which was quantified at 340 nm (ACE test; LTA s.r.l, Milano, Italy). ABO histo-blood group was determined by measuring the presence or absence of antigens A and B in the erythrocytes, as well as the presence or absence of anti-A and anti-B antibodies in serum or plasma. The procedure was performed in gel-columns (Ortho Diagnostic Systems, Inc., Raritan, New Jersey, USA) using the haemagglutination method.
Data were analysed using IBM SPSS statistics 20. Fisher’s exact test was used for categorical variables and the non-parametric Kruskal-Wallis or Mann-Whitney U tests were used for continuous variables. Fisher’s exact test for the 2×3 contingency table was performed using R statistical software. Results are expressed as mean±standard deviation (SD). Two samples were excluded from the analysis as the corresponding subjects had abnormal body mass index (BMI) values, and another was excluded due to a hypertensive clinical history. Statistical significance was set at p<0.05.
Results
In our population of 168 subjects, T allele frequency was 22.6%, similar to that reported in European HapMap samples (18.6–21.7%). The genotype frequencies were 61.3% (major allele homozygous GG), 32.1% (heterozygous GT) and 6.5% (minor allele homozygous TT); which do not deviate from Hardy-Weinberg expectation. From a total of 11 minor allele homozygous subjects, it was only possible to engage eight of them in further study. Blood samples were collected from the eight minor allele homozygous and from age- and gender-matched heterozygous (n=8) and major allele homozygous subjects (n=8) to measure ACE plasma activity and ABO histo-blood group. Four subjects were excluded from the analyses due to voluntary withdrawal, hypertensive clinical history or abnormal BMI. A total of six participants were smokers at the time of the recruitment. None of the subjects were heavy alcohol users but the majority of them stated a sporadic alcohol use.
As shown in Table 1, there were no significant differences across ABO genotype groups with respect to gender, age, BMI or smoking habit. Although the highest and the lowest mean ACE activity values were observed in major and minor allele homozygous subjects, respectively, no significant differences were found. Similarly, lower ACE plasma levels were observed in T allele carriers (68.5±18.2 U/l) compared with those subjects without the minor allele (80.4±19.5 U/l) but these differences also did not reach statistical significance. However, ABO phenotype was significantly different across the three ABO genotype groups (p=0.01). Although no B histo-blood group was detected, subjects from the other ABO groups were present in our population. While only two individuals corresponded to the AB histo-blood group, the majority of participants corresponded to the A or O group (11 and 7, respectively). All the minor allele homozygous subjects corresponded to the A histo-blood group, and 12 of the 13 participants who expressed the A antigen (A or AB histo-blood group) were carriers of the minor allele T (p=0.007) (Table 1). Moreover, significantly lower ACE activity (64.9 ± 16.1 U/l) was found in subjects expressing glycosyltransferase (A and AB histo-blood groups) compared to those not expressing the enzyme (O histo-blood group) (85.3 ± 17.2 U/l) (p=0.029).
Characteristics of subjects according to ABO rs495828 genotypes and ABO phenotypes.
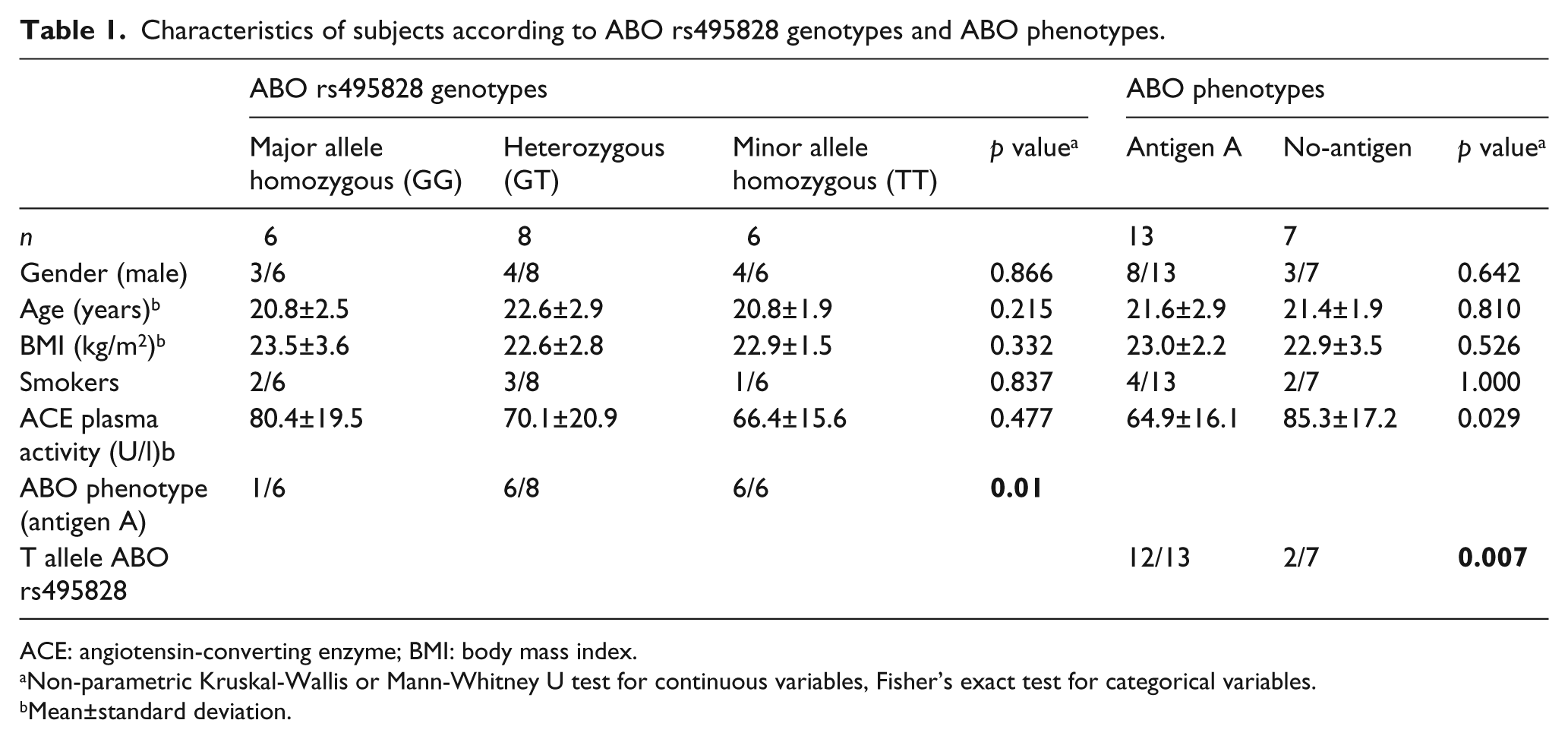
ACE: angiotensin-converting enzyme; BMI: body mass index.
Non-parametric Kruskal-Wallis or Mann-Whitney U test for continuous variables, Fisher’s exact test for categorical variables.
Mean±standard deviation.
Discussion
After having found significant associations between the minor allele T of ABO rs495828 polymorphism and both risk of hypertension and ACE inhibitor-induced cough,9,10 we hypothesised that these associations could be due to this allele giving rise to low ACE activity, as previously reported in an Asian population. 13
To test our hypothesis, we genotyped a total of 168 healthy subjects to classify them into the three possible genotype groups. For subsequent quantification of ACE activity, and bearing in mind the high interindividual variability in the activity of this enzyme, we focused on reducing the effect of factors other than the studied polymorphism. Therefore, we firstly recruited the identified minor allele homozygous subjects to then recruit age- and gender-matched heterozygous and major allele homozygous subjects. All of them were Caucasian and were not being treated with ACEIs or any other antihypertensive treatment. Moreover, we ensured that BMI, smoking and alcohol use were similar between the three genotype groups.
Contrary to expectations, the results of this study do not support the initial hypothesis. Although a slight trend was detected, it was not significant. However, the minor allele T was strongly associated with ABO phenotype; specifically with the expression of glycosyltransferase isoform A, which in turn was associated with low ACE activity. The ABO gene encodes the glycosyltransferase that transfers monosaccharides to cell-surface H antigens. The three major isoforms A, B and O, have their own specificity and activity. Glycosylation of the H antigens of ABO groups A and B is catalysed by glycosyltransferases A (for N-acetyl galactosamine) and B (for D-galactose), respectively. The O allele does not produce an active enzyme. Differences in ACE glycosylation depending on ABO group would lead to differences in ACE activity and consequently to differences in blood pressure and hypertension risk.13–15 The evidence of ABO rs495828 functionality found here further supports associations previous published between this polymorphism and different traits.9–12
The main limitation of this study is the small sample size. Taking this into account we cannot rule out that rs495828 may be involved, at least in part, in determining ACE activity. However, the results obtained here indicate that ABO phenotype would be a better predictor than a single polymorphism. So, it would probably be necessary to genotype other informative ABO variants associated with other histo-blood groups, such as rs817619 or rs8176746 (O and B histo-blood groups, respectively), to better predict ACE activity using ABO genetic markers.
Conclusion
This study clearly represents new evidence in favour of a relationship between ABO and ACE plasma activity. Although the results make the influence of the ABO rs495828 polymorphism on ABO phenotype clear, they also show the ABO phenotype to be a better predictor of ACE plasma activity than the rs495828 ABO genotype. Pharmacogenetic and disease risk studies have identified many relevant genetic markers, but phenotypic traits cannot be ignored as they sometimes prove to be highly valuable. Therefore, both genetic and phenotypic markers should be included in future predictor models for earlier diagnosis of hypertension risk and for safer and more efficacious ACE-inhibitor treatment.
Footnotes
Acknowledgements
The authors wish to thank the Language Advisory Service at the University of Barcelona for manuscript revision.
Conflicts of interest
None declared.
Funding
This study was supported by the Catalonia Ministry of Innovation, Universities and Enterprise (DIUE, 2009SGR1501). PG was supported by a ‘Sara Borrell’ contract (CD09/00296) from the Spanish Ministry of Health, Instituto de Salud Carlos III (Fondo de Investigacion Sanitaria (FIS)).