
Abstract
Introduction:
The Keriyans live in the hot, arid areas of Taklimakan Desert and maintain a primitive way of life. They have a low incidence of hypertension. However, little is known about the adaptive compensation in the organism. In the present study, we explored the the traditional risk factors of hypertension in the Keriyans.
Materials and methods:
We performed an epidemiological survey of Keriyans in a randomly selected natural population including 508 individuals aged 16 years or more, using the WHO MONICA scheme and 151 randomly selected age/gender-matched controls, Uighurs, from the nearest villagers to the Keriyans.
Results:
The incidence of hypertension in the Keriyans was significantly lower than that in the controls(p<0.001). Multivariate logistic regression analysis indicated that age, hyperglycemia and salt consumption as well as sodium intake in diet were associated with traditional hypertension risk factors. Correlation between water quality and hypertension showed that calcium was positively associated with the detection rate of hypertension.
Conclusions:
Age, hyperglycemia and salt consumption as well as sodium intake in diet were correlated with hypertension risk factors, which leads to the speculation that the water of the desert draught area which is characterized by low calcium and high magnesium levels might account for the low incidence of hypertension in Keriyans.
Introduction
The Taklimakan Desert, the largest desert in China and the second largest in the world, is called the “Dead Sea”. A nomadic tribe, the Keriyans, live in the center of the Taklamakan Desert along the seasonal Keriya River. This is one of the most harsh, hot and arid areas in the world with an annual rainfall of less than 20 mm and temperature highs of between 50−60°C. In a sense, the Keriyans offer some important advantages for scientific research since they are almost entirely secluded from the world due to undeveloped traffic, the monotone nature of genetic background due to less communication with others and low education, and the economic blockade due to their nomadic lifestyle. They survive on meat products and desert sap seepage, and live in tribe-dominated familial clusters, which yield close marital relationships. Therefore, the Keriyans are a clannish tribe with their own characteristics, for example in terms of lifestyle, marriage, diet and drinking-water. In the present study, we aimed to explore the traditional risk factors of hypertension in the Taklimakan Desert of Xinjiang Province as well as the association of hypertension with their diet and water quality.
Methods
The protocol of the study was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University and Hetian Region Government. Informed written consent for participation in the study was obtained from each participant.
Study population
We conducted medical surveys in the Keriyan Village twice in September 2005 and October 2008. The first medical surveys were conducted in the Keriyan Village in September 2005, i.e., Phase I. The total population included 985 individuals according to local registration in Phase I. The total population included 1171 individuals according to local registration in October 2008, i.e. Phase II. A total of 790 individuals were randomly sampled. Of these, 508 (61%) (290 males and 218 females) were between 16–29 years of age, and 282 (173 males and 109 females) were older ≥30 years of age. As a reference we also randomly selected 151 Uighur adults (age≥30 years, mean 48.99±13.84) including 77 males and 74 females in the Yutian county (they are the nearest villagers to the Keriyans. At present, most people think Keriyans are related to the Uighurs, but this remains to be confirmed.
Questionnaire survey
The standardized methods of the World Health Organization (WHO) MONICA project were used to collect information on anthropometry (body height, weight, waist and hip circumference abdominal perimeter) and lifestyle habits (including 24 h diet recall). Other measurements included blood pressure, an electrocardiograph and an echocardiogram. Cigarette smoking was defined as smoking at least one cigarette per day for one year or more. According the National Institute on Alcohol Abuse and Alcoholism (NIAAA) criteria, alcohol drinking was defined as drinking at least 8 g alcohol per week.
Physical examination and sample collection
Body height, weight, waist circumference, blood pressure were checked. Body mass index (BMI) was calculated as mass in kilograms divided by the square of height in meters. Ethylene Diamine Tetraacetic Acid (EDTA)-blood samples were obtained after a fasting period. Blood electrolyte, glucose, cholesterol, renal and liver functions and a serum iron assay were determined by use of an automatic biochemical analyzer in the central laboratory of the First Affiliated Hospital of Xinjiang Medical University. Fasting plasma glucose was detected by a Glucorder Analyzer (Roche).
Collection and analysis of water samples
Local drinking water samples in the Taklimakan Desert and Yutian country were collected according to the standard criteria for drinking water, as stipulated by the People’s Republic of China in July 2007. The water was assayed for hardness, chloride, sulfide, fluoride, iron, magnesium and calcium using the graphite furnace atomic absorption spectrophotometry method according to the criteria of GB/T 5750.12-2006.
Diet evaluation
A 24 h dietary recall as well as a food frequency questionnaire was obtained. The nutrient intake was calculated using the nutrition calculator version 1.6 (Chinese Disease Control Center (CDC), China).
Diagnostic criteria
Hypertension was diagnosed as a blood pressure mean of three independent measurements of systolic/diastolic blood pressure greater than or equal to 140/90 mm Hg (1 mm Hg=0.133 kpa) or the use of antihypertensive medication according to the Guidelines for Prevention and Treatment of Hypertension in China (2004) 1 .
Criteria for overweight and obesity
BMI was calculated as weight/height2 (kg/m2). The Working Group on Obesity 2 in Chinese recommended a cut-off level for defining normal weight as a BMI of 18.5−23.9 kg/m2, overweight as BMI of 24.0−27.9 kg/m2, and obesity as BMI of 28.0 kg/m2 or more.
Statistical analysis
SPSS 15.0 was used to perform the statistical analysis. Continuous data was expressed as a mean±standard deviation (SD). Student’s t-test with two-tailed values was used to compare groups when continuous variables were normally distributed and the homogeneity of variance. Groups were compared using the Chi-squared test for the categorical variables. Statistical significance was accepted at p<0.05.
Results
Baseline characteristics
The mean age of 508 Keriyans aged 16 years or more was 36.14±15.96 years, and the mean systolic and diastolic blood pressures were 109.81±18.36 mm Hg and 72.58±11.39 mm Hg with a hypertension detection rate of 10.89%. In adults with age≥30 years (mean 47.09±14.52), the hypertension detection rate was 14.55% for the Keriyans and 42.95% for the Yutian population which was significantly different (p<0.05).
When comparing the two populations with ages≥30 years, statistically significant differences were observed for BMI, Serum triglycerides (TG), the total cholesterol (TC), the high-density lipoprotein cholesterol (HDLC), the low -density lipoprotein cholesterol (LDLC), fasting glucose, fat and salt intake (p<0.05), whereas no difference was noted for waist circumference (Table 1). Univariate analysis indicated that age, gender, alcohol drinking, overweight and obesity, waist circumference, low LDLC, high plasma glucose levels, high salt intake and high fat intake served as the hypertension risk factors of Keriyans population in this study. Multivariate unconditional logistic regression analysis showed that age, gender, waist circumference, high plasma glucose levels and a high salt intake were significantly associated with hypertension for Keriyans population (Table 2),but also were significantly associated with hypertension for Yutian population except waist (Table 3).
Comparisons of the baseline risk factors between “Keriyan” and Yutian populations.

BMI: body mass index; SD: standard deviation. ap<0.05, bp<0.001.
Regression analysis of hypertension with its related risk factors in “Keriyan” (age≥30 years).

CI: confidence interval; OR: odds ratio. ap<0.05, bp<0.001.
Regression analysis of hypertension with its related risk factors in Yutian populations (age≥30 years).
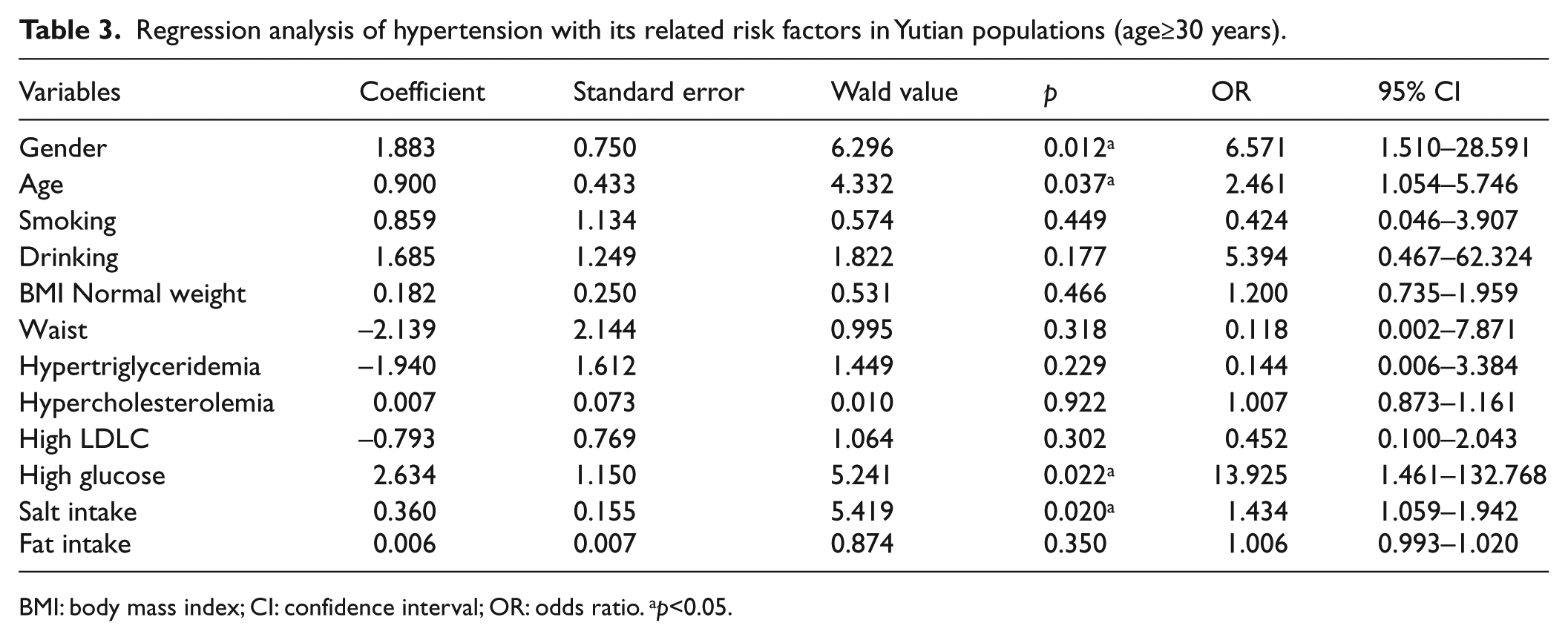
BMI: body mass index; CI: confidence interval; OR: odds ratio. ap<0.05.
Nutrition intake in diet and hypertension
The association of the nutrition intake for the Keriyans (age≥30 years) with hypertension was, in general, weak. In the univariate analysis, no significant associations were noted for energy, fat, carbohydrate, prandial fiber, protein, cholesterol, vitamin A, aneurin, riboflavin, nicotinic acid, vitamin C and E, phosphorus, magnesium, potassium, iron, zinc, selenium, manganese and copper. Calcium, sodium, salt intake were risk factors with hypertension. In the multivariate unconditional regression analysis salt intake, riboflavin, calcium and sodium were positive associated with hypertension, whereas nicotinic acid showed negative associations. Stepwise logistic stepwise regression analysis incorporating the nutriment of significance showed that salt intake (odds ratio (OR)=1.724) and sodium intake (OR=1.002) as the risk factors showed significant and positive associations with hypertension. And for Yutian population, this analysis showed that sodium intake (OR=1.001) as the risk factors with hypertension (Table 4).
Multivariate regression analysis of hypertension with age, high glucose and salt intake in “desert men” and Yutian populations.

CI: confidence interval; OR: odds ratio. ap<0.05, bp<0.001.
Correlation analysis of the water samples indicated that the coefficients were significant at 0.05 level with hypertension and showed a positive correlation for water calcium(r=0.642), Negative associations were found for solids (r=0.813), sulfate (r=0.748), chloride (r=0.855), potassium (r=0.954), sodium (r=0.829) and magnesium (r=0.710). No statistically significant difference was observed for water hardness, manganese, copper and iron.
Discussion
The Keriyans have adapted to the extreme hot and arid environment in the Taklimakan Desert. They hardly sweat or feel thirsty even when they graze their livestock in the desert at about 50–60°C during the day. It is speculated that they have a special fitness index, acid-base and electrolyte balance regulation system or genetic basis for this. The Keriyans are isolated from the rest of the world because their environment is inaccessible for the others. Moreover, they are generally married within their community and rarely marry anyone else from the outside world. Thus, the characteristics of the Keriyans result from gene-environment interaction. The Keriyans live in a different way from the control group. They have two meals a day with low calorie intake but they consume much energy when they graze livestock among the sparse Populus euphratica trees and sand dunes. The Keriyans are seldom fat and the incidence rate of hypertension, diabetes is very low according to our survey.
First, soil salt is the main seasoning for Keriyans, who consume low levels of sodium in diet. It is estimated that the average salt intake (±SD) among adult Keriyans is 5.02±1.43 g, and the average sodium intake is 98.44±29.72 mmol; thereof intake of less than 100 mmol accounts for 58.5%. In contrast, among Yutian adults the average salt intake is estimated at a significant high level of 10.85±2.44 g (p<0.001), as well as the average sodium intake at 199.93±51.42 mmol p<0.001) with the intake of less than 100 mmol accounting for 1.0%.
Evidence is mounting to suggest that the dietary intake of potassium, sodium, calcium and magnesium are closely associated with blood pressure variation. The aborigines on the Pacific Islands have been accustomed to a virtually no-salt diet, and there are almost no hypertension cases reported. 3 In contrast, the average salt intake among residents in Hokkaido reaches as high as 15−20 g per day, even 26−55 g per day, which results in a high incidence of hypertension (84%). 4 Experimental animal studies also support the notion that high sodium intake can accelerate the development of hypertension and vascular damage.5,6 Secondly, the drinking water of the Keriyans is from the sap seepage, which contains high levels of magnesium (119.23 mg/l) when compared with the standard threshold (20−30 mg/l), while the calcium content is relatively lower than the standard baseline (40−80 mg/l).
Our correlation analysis indicated that the calcium content of the water was associated with the hypertension detection rate in a positive manner, while for magnesium in a negative manner, which could lend some support for the antagonistic action of calcium and magnesium in blood pressure regulation. However, in general, the drinking water in the Taklimakan Desert is characterized by high magnesium content, in line with the low detection rate of hypertension in this study. We thus speculate that the low incidence of hypertension among Keriyans might be attributed to their drinking water. Since the establishment of the Tongguzbasti village in 1990 in Hetian City, modern ways are gradually infiltrating this previously closed region and, accordingly, the incidence of hypertension might increase and so need periodic follow-ups. It is reported that calcium content in drinking water is positively related to systolic blood pressure and has also served as a risk factor for cardiovascular diseases. 7 In 1999, Yang and Chiu documented that there is a significant protective effect of magnesium intake from drinking water on the risk of hypertension, 8 which leads to the speculation that magnesium plays an important role in blood pressure regulation. The potential mechanisms for magnesium to lower blood pressure might be (a) the dilatation of renal vessels; (b) the acceleration of prostaglandin release; (c) the stimulation of sodium pumping and adenosine kinase, which is increased in case of magnesium loss; (d) the regulation by renin of magnesium can make the blood vessels constricted. On the other hand, magnesium excess can dilate the vascular smooth muscular or block ganglions, which can dilate the peripheral vessels, and hence lower blood pressure. 8 Magnesium is involved in in a variety of physiological processes of the vascular tissues, and is related closely to blood pressure regulation. In the peripheral vasculature, magnesium and calcium are involved in regulation via neurohumoral effects, the kidneys and adrenal glands.9,10
Conclusion
Correlation analysis indicated that age, hyperglycemia and salt consumption were correlated with Keriyans’ hypertension risk factors, which leads to the speculation that the water of the desert area which is characterized by low calcium and high magnesium might account for the low incidence of hypertension in Keriyans. The Keriyans live a different lifestyle from the controls. They have a low calorie intake but they expend much energy. They consume significantly lower levels of sodium than other groups. We speculate that low salt intake is the most important factor of the low incidence of hypertension and low calcium and high magnesium levels in water might be another reasons for the low incidence of hypertension in Keriyans.
To our knowledge, this is the first epidemiologic study of hypertension risk factors in the Keriyans in Taklimakan Desert. Our results may be helpful to study mechanisms of how people adapt to the extreme hot and arid environment.
Footnotes
Conflict of interest
The authors declare that there are no conflicts of interest.
Funding
This work was financially supported by the National Science Foundation of China (Grant No. 30760070)