
Abstract
Objective:
To investigate the influence of simultaneous administration of spironolactone (20 mg/kg per day, intraperitoneal (i.p.)) and aliskiren (50 mg/kg per day, i.p.) for a period of eight weeks on cardiac remodeling in TGR(mRen2)27 rats.
Methods:
Echocardiographic and electrophysiological and histological methods were used to determine the influence of spironolactone and aliskiren on cardiac remodeling.
Results:
1) the beneficial effect of aliskiren on SBP was enhanced by simultaneous administration of spironolactone; 2) echocardiographic studies showed that the left ventricle diameter (LVD), the left ventricle end diastolic volume (LVEDV) and the left ventricle posterior wall thickness (LVPW) were significantly reduced by the combination of both drugs when compared with aliskiren alone; 3) the ejection fraction was also increased; 4) histological studies indicated a greater decline in perivascular and interstitial fibrosis when both drugs were used; 5) the decrease of electrical remodeling of the left ventricle caused by aliskiren was further reduced by simultaneous administration of spironolactone; 6) the cardiac refractoriness increased by aliskiren was further incremented by spironolactone. Spironolactone (20 mg/kg per day) alone increased the ejection fraction and reduced LVD, LVEDV and LVPW but its effect was smaller than that achieved with the combination spironolactone plus aliskiren.
Conclusion:
The combination of an aldosterone inhibitor with a direct renin inhibitor proved to be of greater benefit for cardiac structural and electrical remodeling in this experimental model of hypertension than aliskiren alone.
Introduction
It is well known that aldosterone causes hypertension with consequent ventricular hypertrophy and fibrosis. In recent years evidence has been provided that aldosterone has a direct effect on the heart. Spironolactone, for instance, administered together with angiotensin-converting enzyme (ACE) inhibitors at doses that did not change the blood pressure, decreases the morbidity and mortality of patients with heart failure by 30% 1 – an effect in part due to a decrease in cardiac fibrosis. 2 It is known that Ang II is involved in the generation of fibrosis in part because aldosterone increases cardiac AT1 receptors’ density. 3 Moreover, Ang II plays a role on the generation of fibrosis in part because aldosterone increases the levels of AT1 receptors in the heart. 3 Indeed, in patients with primary aldosteronism the enhanced fibrosis is associated with higher incidence of atrial fibrillation. 4 The Randomized Aldactone Evaluation Study (RALES) 1 showed that spironolactone reduced the number of deaths of cardiac origin, while the EMPHASIS-HF Trial showed a decreased morbidity and mortality of patients with heart failure receiving eplerenone.5,6
The activation of mineralocorticoid receptors (MRs) is known to produced cardiac arrhythmias 7 and the blockade of MR with spironolactone proved to be useful during atrial fibrillation by preventing atrial remodeling including fibrosis and dilation. 8 In patients with systolic heart failure and mild symptoms, eplerenone reduced the incidence of new onset atrium fibrillation. 9
Evidence has been presented that cardiac expression of MR is increased in hypertension, 10 myocardial infarction 11 and diastolic heart failure 12 and that cardiomyocyte-specific MR over-expression does result in pronounced fibrosis. 7
The TGR(mRen2)27 rat is characterized by fulminant hypertension 13 and elevated serum aldosterone level. Moreover, the Ren2 transgene has been demonstrated to be expressed in different tissues including the heart,13,14–17 generating high levels of Ang II in the circulation and in the myocardium. 7 This finding is of particular interest because Ang II is considered to be an important cause of cardiac remodeling. Evidence is available that in this model the transgene is highly expressed in the adrenal gland and that the urinary excretion of aldosterone is 1.5–2.5-fold increased compared with Sprague Dawley rats. 18 Because the activation of the renin–angiotensin system is involved in the effect of aldosterone in cardiac muscle, particularly in the generation of fibrosis, 19 it is important to investigate whether renin inhibition potentiates the effect of spironolactone on cardiac remodeling. In the present work the influence of the combination of aliskiren plus spironolactone on structural and electrical remodeling of TGR(mRen2)27 rats was investigated.
Methods
Animals
Male TGR(mRen2)27 rats were received from Bowman Gray School of Medicine, Wake Forest University, Winston-Salem, NC, USA at six weeks of age. Animals were housed (three per cage) and maintained at 20–22°C and had free access to water and rat chow following the recommendations of NIH.
Experimental procedures
Animals were divided into four groups. Group 1 was the control TGR(mRen2)27 rats; Group 2 consisted of TGR(mRen2)27 rats treated with aliskiren (50 mg/kg per day, intraperitoneal (i.p.)) for eight weeks; Group 3 consisted of rats treated with aliskiren (50 mg/kg per day, i.p.) plus spironolactone (20 mg/kg per day, i.p.) for eight weeks; Group 4 consisted of rats treated with spironolactone (20 mg/kg per day) alone for a period of eight weeks.
Blood pressure
Systolic blood pressure (SBP) (mm Hg) was measured in triplicate via tail cuff method in conscious rats on a weekly basis using MC4000 blood pressure analysis system from Kent Scientific Corporation. Prior to the initial recorded blood pressures (about week 1), rats were allowed to acclimatize to the blood pressure system and measurements over several days. Tail cuff size was adjusted upward as needed for growth in tail diameter.
Echocardiography
Rats were anesthetized with an intraperitoneal administration of ketamine (50 mg/kg). Echocardiography evaluated left ventricular systolic and diastolic function. The hair was removed from the left hemithorax using a depilatory cream to facilitate imaging. The rats were positioned in a right lateral decubitus position. Echocardiograms were performed using a SonoSite ultrasound system using a 10-mHz transducer and electrocardiographic monitoring. The echosonographer was blinded to the treatment groups. M-mode echocardiography was performed using the parasternal short-axis view of the left ventricle (LV). The guidelines of the American Society of Echocardiography were used for measurement of the LV end-diastolic and end-systolic diameters, and posterior wall thickness. Images were captured digitally and a series of five consecutive cardiac cycles was measured and averaged for each individual measurement.
Measurements of transmembrane potentials and refractoriness
Intracellular potassium chloride (KCl) microelectrodes connected to a high impedance DCamplifier (WP Instruments, Model 750 Dual Probe with capacitance neutralization) were used to measure the transmembrane potentials. The right ventricular muscle was dissected and transferred to a bath through which oxygenated Krebs solution (36°C) flowed continuously. The composition of Krebs solution was as follows (mM): NaCl, 150; KCl, 5.4; CaCl2, 1.8; MgCl2, 1; HEPES, 5; glucose, 5; pH adjusted to 7.3. The solution was saturated with 100% O2. The muscle was stimulated with a fine pair of platinum electrodes (0.3 mm in diameter) by using rectangular current pulses generated by an electronic stimulator and isolation unit (Grass Instruments, Boston, USA). The intensity of the current pulses was twice threshold and the pulse duration was 3 ms. A bipolar stimulation was used and the rate of stimulation was 0.2 Hz. After 30 min of equilibration in Krebs solution, the membrane potential was recorded from superficial endocardial fibers. The determination of the stimulus strength was achieved by amplifying the voltage drop across a 10 MΩ resistor placed between the muscle and ground.
To measure cardiac refractoriness strength-current curves were obtained by applying a second current pulse of variable intensity but constant duration (2 ms) at different moments of the action potential and determining the minimal current strength required to elicit a clear propagated electrical response. The intervals were previously selected and kept constant during the experiments.
Measurements of macroscopic longitudinal and transverse conduction velocities
To investigate the influence of aliskiren on non-uniform anisotropic conduction, measurements of longitudinal and transverse conduction velocities were performed in fibers located at the middle of the papillary muscle. For this, the muscle was stimulated first in the longitudinal direction and then in the transverse direction and the activation time was recorded keeping the electrode inside the cell. The duration of the pulse (3 ms) and its intensity were kept constant. Values of latency were used to estimate the conduction velocity.
Histological studies
To determine the presence of interstitial fibrosis, coronal sections taken from the equator of the heart were obtained and immediately fixed in formalin (10%). Some sections were stained with hematoxylin-eosin and others with Masson trichrome for the study of interstitial and perivascular fibrosis. Connective tissues and muscle areas were manually traced using a digitized pad connected to a computer. The volume fraction of interstitial fibrosis was calculated as the sum of all connective tissue areas divided by the sum of all connective and muscle areas in the field. Tissues were analyzed using a LSM 5 Pascal Confocal System, Carl Zeiss (Microimaging, Inc.). Measurements of percent of fibrosis as well as ventricular wall width were performed using a MCID (Micro Computer Imaging Device, Amersham Biosciences, and Canada, United Kigdom). Perivascular fibrosis represented by percent adventitial area per vessel was also investigated. For this, coronary arteries of approximately equal cross-sectional area were traced and used for estimation of percent area of fibrosis.
Drugs
Spironolactone was from Sigma Chemical (Saint Louis, MO, USA) and aliskiren was kindly provided by Novartis Pharmaceuticals.
Statistical analysis
Data are mean ± SEM. Comparison between groups was done by the analysis of variance (ANOVA) and Tukey’s post hoc, and differences were considered significant when p < 0.05.
Results
Influence of spironolactone plus aliskiren on SBP
Measurements of SBP performed on TGR(mRen2)27 rats treated with aliskiren (50mg/kg per day) plus spironolactone (20mg/kg per day) for a period of eight weeks indicated a greater decline of blood pressure than that achieved with the combination of these drugs when compared with the administration of aliskiren alone (see Figure 1). The SBP in TGR(mRen2)27 rats not exposed to the drugs remained high during the eight week period of the study, as shown in Figure 1.
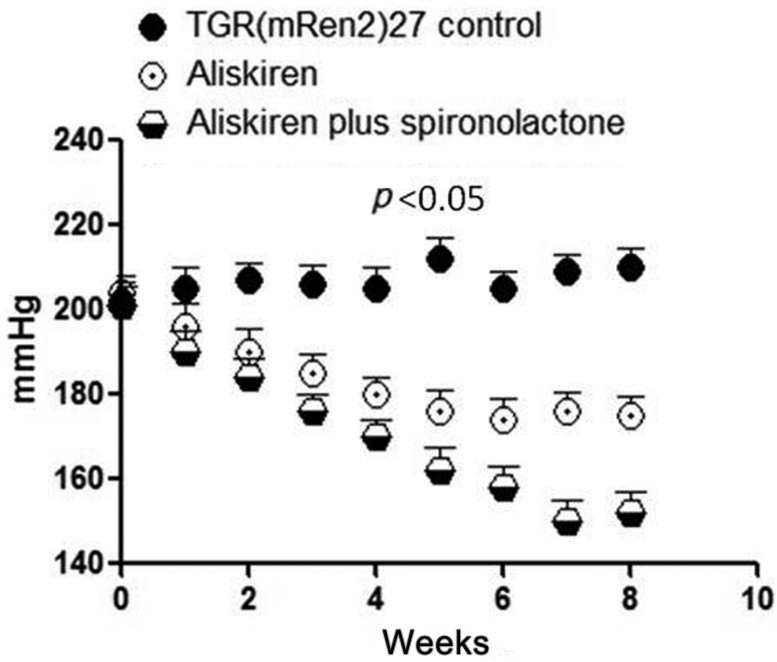
Influence of aliskiren (50mg/kg per day, intraperitoneal (i.p.)) plus spironolactone (20 mg/kg per day, i.p.) administration for a period of eight weeks on the systolic blood pressure of TGR(mRen2)27 rats. Results found with administration of aliskiren (50 mg/kg per day) alone as well values of systolic blood pressure in the animals not exposed to the drugs were also shown. Each point is the average from eight rats. Vertical line at each point, SEM (p<0.05).
Echocardiographic studies
Echocardiographic studies showed an improvement of heart function and a decrease of cardiac remodeling. As shown in Table 1, aliskiren (50mg/kg per day) plus spironolactone (20 mg/kg per day) increased the ejection fraction and reduced the left ventricle diameter (LVD), the left ventricle end diastolic volume (LVEDV) and the left ventricle posterior wall thickness (LVPW). The decline in cardiac remodeling was greater than that achieved with aliskiren (50mg/kg per day) alone (see Table 1). Spironolactone (20 mg/kg per day), by itself, increased the ejection fraction and reduced the cardiac remodeling, as shown in Table 2. As it can be seen, the effect of spironolactone, was smaller than that achieved with the combination of spironolactone plus aliskiren.
Echocardiographic studies performed on TGR(mRen2)27 rats treated with aliskiren (50mg/kg per day) or aliskiren plus spironolactone (20 mg/kg per day) for a period of eight weeks.
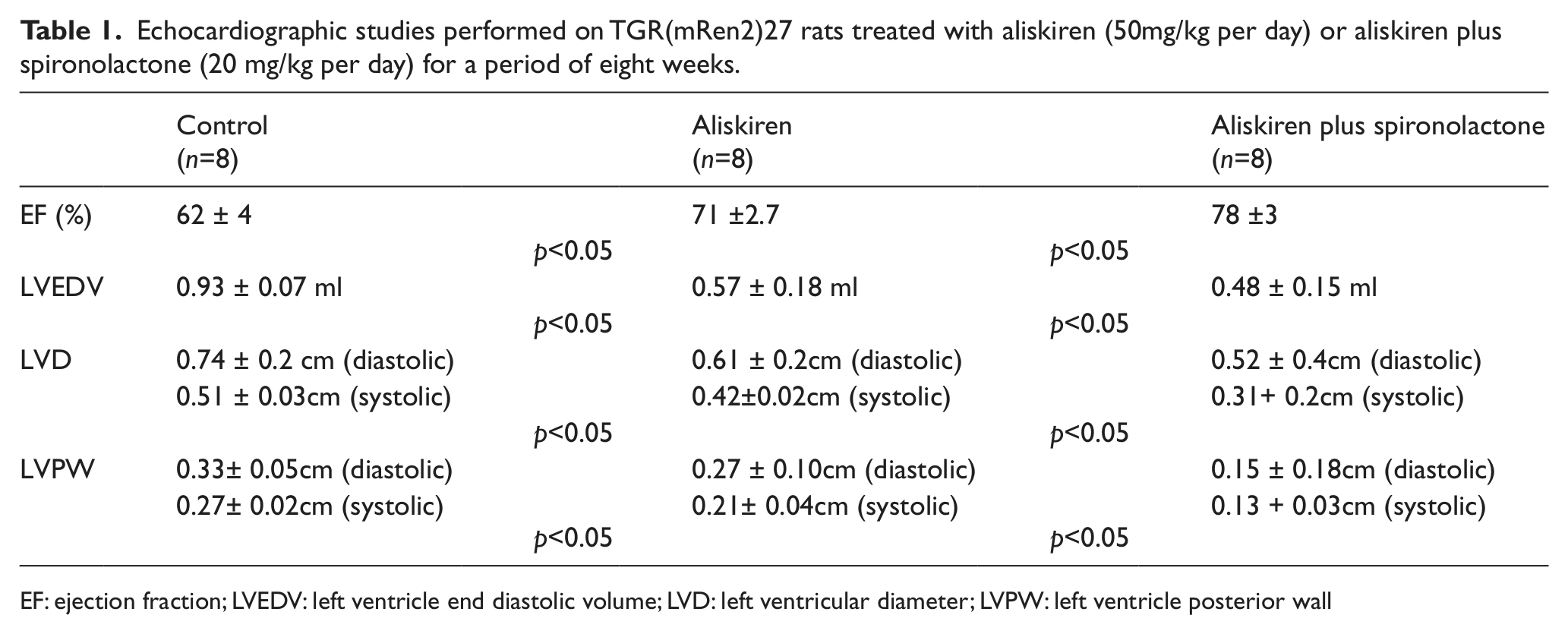
EF: ejection fraction; LVEDV: left ventricle end diastolic volume; LVD: left ventricular diameter; LVPW: left ventricle posterior wall
Resting echocardiographic studies performed on TGR(mRen2)27 rats treated with spironolactone (20 mg/kg per day) for a period of eight weeks.

EF: ejection fraction; LVEDV: left ventricle end diastolic volume; LVD: left ventricular diameter; LVPW: left ventricle posterior wall
Histologic studies
Histological studies indicated that the interstitial and perivascular fibrosis, for instance, were both significantly reduced in rats treated with spironolactone (20mg/kg per day) plus aliskiren (50 mg/kg per day) for a period of eight weeks. As shown in Figures 2, 3 and 4, the percent area of interstitial and perivascular fibrosis was smaller in TGR rats treated with aliskiren (50mg/kg per day) plus spironolactone (20 mg/kg per day) for eight weeks than that achieved with aliskiren (50 mg/kg per day for eight weeks) alone. Spironolactone, by itself, reduced the fibrotic are of the left ventricle by 13.3 ± 2.6% (n=25) (p<0.05).
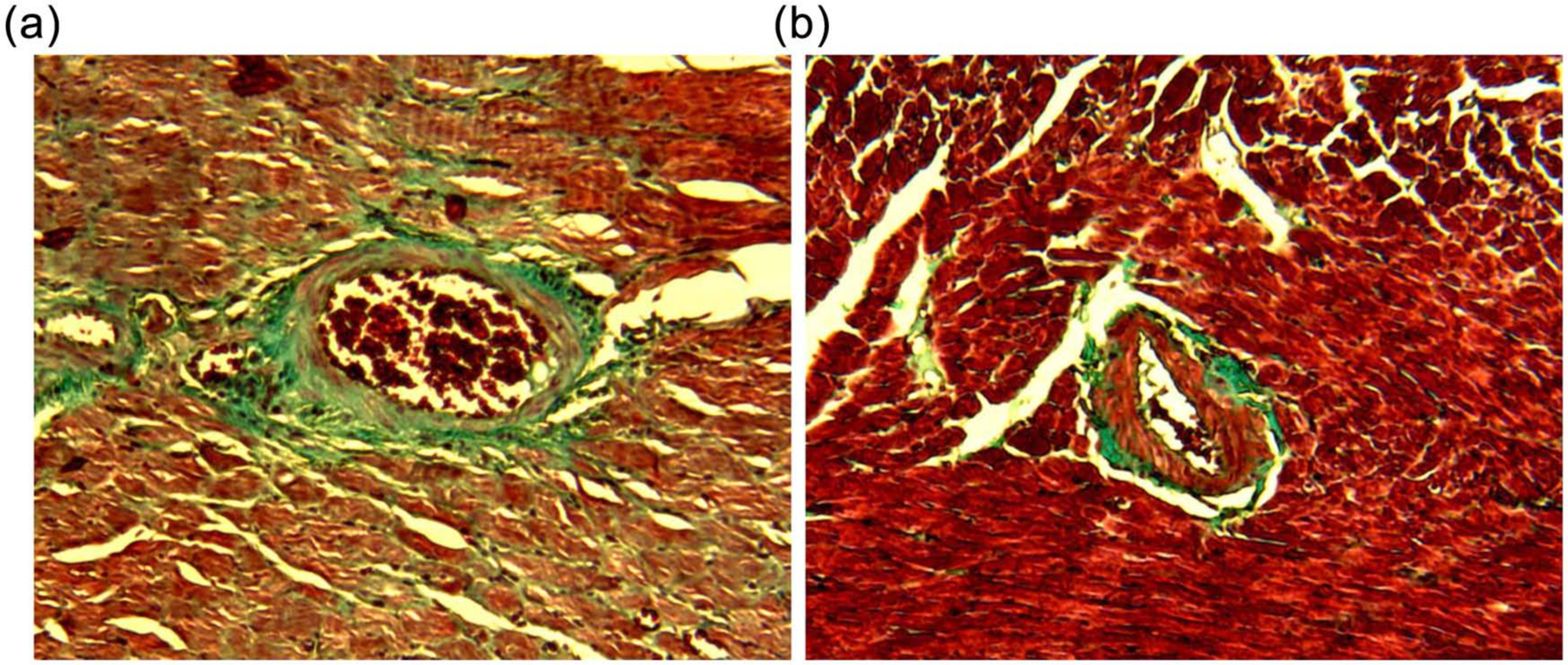
(a) Perivascular fibrosis of rat coronary artery as well as interstitial fibrosis from control TGR(mRen2)27 rat. (b) After treatment with aliskiren (50mg/kg per day) plus spironolactone (20 mg/kg per day) for a period of eight weeks.

Average decrease of percent area of perivascular fibrosis elicited by aliskiren (50mg/kg per day) plus spironolactone (spiron; 20 mg/kg per day) administration for a period of eight weeks. The influence of aliskiren (50mg/kg per day) alone is also shown. Each bar is the average from eight rats. Vertical line at each bar, SEM (p<0.05).

Average decrease of interstitial fibrosis elicited by aliskiren (50 mg/kg per day) plus spironolactone (spiron; 20 mg/kg per day) administration for a period of eight weeks. The influence of aliskiren (50mg/kg per day) alone is also shown. Each bar is the average from eight rats. Vertical line at each bar, SEM (p<0.05).
Influence of aliskiren plus spironolactone on electrical remodeling
Measurements of resting membrane potential performed on the left ventricle of TGR rats treated with aliskiren (50 mg/kg per day) plus spironolactone (20 mg/kg per day) for eight weeks showed an increase of membrane potential from –64 ± 4.4 mV (n= 25) (eight animals) to –78 ± 4.5 mV (n= 23 ) (eight animals (p<0.05). The cardiac refractoriness was significantly increased in rats treated with both drugs, as shown in Figure 5 – an effect even greater than that achieved with aliskiren alone. This finding indicates that a greater intensity of the electrical stimulus was necessary to elicit a propagated response in rats treated with spironolactone plus aliskiren compared with controls or aliskiren alone (see Figure 5).

Increase of cardiac refractoriness caused by the administration of aliskiren (50mg/kg per day) plus spironolactone (20 mg/kg per day) for a period of eight weeks. The effect of aliskiren (50 mg/kg per day) alone is also shown. Each point is the average from 20 experiments (eight rats).Vertical line at each point, SEM (p<0.05).
Measurements of conduction velocity for the longitudinal (θl) and transversal direction (θt) showed a significant improvement in rats treated with spironolactone plus aliskiren. As shown in Table 3, the average value of θl for control animals was 30 ± 4.3 cm/s while the conduction velocity measured in the transverse direction (θt) was 12 ± 4.1 cm/s, which indicates an anisotropic ratio (θl / θt ) of 2.5. For animals treated with aliskiren (50 mg/kg per day) for eight weeks the values of θl and θt were 50 ± 2.8 cm/s and 36 ± 2.6 cm/s, respectively, which represents an anisotropic ratio of 1.4. For the animals treated with aliskiren (50 mg/kg per day) plus spironolactone (20 mg/kg per day) for eight weeks the values for θl and θt were 59 ±2.7 cm/s and 42 ± 2.8cm/s, respectively. In this case the anisotropic ratio was 1.3. The appreciable improvement of impulse conduction, particularly in the transverse direction, caused the combination of both drugs to result in a smaller generation of slow conduction and development of reentrant rhythms. Spironolactone (20 mg/kg per day) alone increased the resting potential of ventricular fibers from –64 ± 4.4 mV (n= 25) (eight animals) to 71 ± 3.5 mV (n=23) (seven animals) (p<0.05) and incremented the conduction velocity by 15.8+/–3.2% (n=12)(four animals) (not shown).
Influence of aliskiren (50mg/kg per day) plus spironolactone (20 mg/kg per day) on longitudinal (θl) and transverse (θt) conduction velocity (cm/s) in ventricular muscle of TGR(mRen2)27 rat.

Discussion
The present results indicate that spironolactone potentiates the beneficial effect of direct renin inhibition on cardiac structural and electrical remodeling in hypertensive TGR(mRen2)27 rats. This conclusion is supported by echocardiographic studies which demonstrated a greater improvement of cardiac function when spironolactone is administered together with aliskiren.
Of particular interest was the decline of perivascular and interstitial fibrosis seen with both drugs. Evidence is available that structural discontinuities in cardiac muscle represented by an increase in gap junctional resistance as well as by membrane factors alter the conduction properties of a continuous cardiac fiber. 20 In addition, the changes in the structural organization of the cardiac muscle, and particularly the generation of interstitial fibrosis, lead to serious impairment of impulse propagation and enhance the probability of reentrant rhythms.21-24 Interstitial fibrosis, for instance, not only generates cellular sequestration in the ventricular muscle, preventing the impulse propagation reaching the isolated cells, 24 but decreases the transverse conduction velocity, as shown above, facilitating the generation of reentrant rhythms.
Although the decline in SBP is probably involved in the beneficial effect of spironolactone on cardiac remodeling, there is evidence that the drug reduced mortality and morbidity independently of blood pressure. 2 Therefore, one cannot rule out the possibility that a direct cardiac effect of spironolactone reducing fibrosis is involved in the beneficial effect of the drug on cardiac remodeling as described above. As shown above, experiments performed with spironolactone alone showed a significant decline of the fibrotic area of the left ventricle (see also De Mello 21 ).
Evidence is available that chronic administration of eplerenone reduces the cardiac effect of Ang II through a decline in AT1 receptor level at the surface cell membrane. 25 Because AT1 receptor is a mechanosensor involved in cardiac remodeling26,27 it is reasonable to think that part of the beneficial effect of spironolactone described above is related to a smaller sensitivity of cardiac muscle to mechanical stress. 28 Indeed, previous studies indicated that aliskiren, at low doses, reduces the structural and electrical remodeling independently of blood pressure. 28 The probable mechanism involved in the beneficial effect of aliskiren is a decreased sensitivity to mechanical stress. 28 Because evidence is available that eplerenone has beneficial effects in the failing heart by stimulating endothelial NO synthase with consequent decrease of oxidative stress, 29 it is conceivable that at least part of the beneficial effect of spironolactone on cardiac remodeling is related to the decline of oxidative stress.
Spironolactone or eplerenone are now recommended for patients with New York Heart Association class III or IV symptoms or previous acute myocardial infarction, and more recently evidence has been presented that eplerenone is useful in patients with atrial fibrillation and mild systolic heart failure.5,9 The mechanism involved seems to be a reduction of atrial remodeling including interstitial fibrosis. Our novel findings substantiate the view that the reduction of structural remodeling with consequent improvement of impulse propagation and increase of refractoriness caused by spironolactone associated with renin inhibition decreases the incidence of cardiac arrhythmias in the hypertensive heart. The decline in Ang II plasma level elicited by aliskiren associated with the mineralocorticoid inhibitor proved to be the major explanation for the improvement of heart function and the reduction of cardiac fibrosis.
In conclusion, the present results indicate that the combination of direct renin inhibition with aldosterone blockade is of benefit by reducing the structural and electrical cardiac remodeling in the hypertensive TGR(mRen2)27 rat. These results have important implications for patients with heart failure and essential hypertension.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was supported by a grant from Novartis (Study Number CSP-100A-USNC07) to WDM.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Novartis (Study Number CSP-100A-USNC07) to WDM.