
Abstract
Aim:
To our knowledge, the relationship between simple renal cysts, hypertension and three significant genes of the renin-angiotensin system (AGT, AT1R and ACE1) has not been studied. The present study was designed to search for possible relationships between these significant polymorphic components, hypertension and simple renal cysts in Shiraz province (Iran).
Methods:
A total of 160 participants were recruited from the Motahari Clinic at Shiraz University of Medical Sciences. The subjects were divided into four main groups. Detection of the ACE1 genotype was performed with a nested-polymerase chain reaction (PCR) protocol. Two separate restriction fragment length polymorphism-PCR assays were used to identify AGT and AT1R genotypes.
Results:
The allele frequency of AGT M235T differed significantly between group 1 (patients with simple renal cysts and hypertension) and normal individuals (p <0.05). There were no significant differences in frequency for the other genes (ACE1 and AT1R).
Conclusions:
Our findings show a relationship between the AGT-TT genotype and hypertension in patients with both hypertension and simple renal cysts. This finding suggests an additive role for the AGT gene of the renin-angiotensin system in the process of hypertension and simple renal cysts formation. Future studies are needed to elucidate the mechanisms through which this association is mediated.
Introduction
Renal cysts are the most common space-occupying lesions of the kidney. 1 A classification of renal cysts on the basis of their appearance on computed tomography was introduced by Bosniak in 1986 and refined in 2003. 2 Whether labeled simple or complex, regardless of their radiologic characteristics, the terms used are all descriptive. Simple cysts are distinct lesions within the kidney that are typically cortical, extending outside the parenchyma. They are commonly considered as a harmless anomaly, while cases of complicated renal cysts have been reported. The majority of complications are spontaneous rupture, hemorrhage and infections. The reported overall prevalence of simple cysts is variable. Depending on the population and method of study, the prevalence ranges from 2.38% in the second to 35.29% in the seventh decade of life. 3 Some potential risk factors for the appearance of simple cysts are age, sex, renal stone, serum creatinine, smoking and hypertension. Sporadically, they become symptomatic and may present with flank pain, abdominal discomfort, a palpable mass or hematuria as a result of complications, or subsequent to an enlarging cyst.3–7
Previous studies have noted the association between simple renal cysts and hypertension, but the relationship between these cysts and hypertension has not been studied yet.8–10 Some case reports have described patients with simple renal cysts and hypertension in whom renin released from the affected kidney was increased and blood pressure normalized after surgical removal of the cysts. 11
The renin-angiotensin system as a circulating or hormonal system regulates blood pressure, electrolyte and fluid homeostasis and is mainly related to the short- and long-term regulation of arterial blood pressure.12, 13 Studies of the renin-angiotensin system in experimental animal models have detected remarkable genetic polymorphisms chiefly involving the angiotensinogen gene (AGT), AT1 receptor gene (AT1R) and angiotensin-converting enzyme gene (ACE1). Studies that investigated hypertension in relation with the renin-angiotensin system have indicated that there are naturally occurring genetic variations within the renin-angiotensin system in animals as well as humans. 13
In diverse genetic or environmental backgrounds, a specific gene variant might be a sign of different pathophysiological implications.14, 15 As a result, the present case-control study was designed as (to our knowledge) the first attempt to identify possible associations between polymorphisms of three significant genes of the renin-angiotensin system (AGT, ACE1 and AT1R) and hypertension in patients with simple renal cysts in a southern population of Iran (Shiraz).
Methods
Study subjects
A total of 160 participants were recruited from Motahari Clinic, affiliated with Shiraz University of Medical Sciences. The subjects were divided into four groups: patients with simple renal cysts and hypertension (group 1, n = 40), simple renal cysts without hypertension (group 2, n = 40) healthy individuals without any renal complications (group 3, control, n = 40) and hypertension without simple renal cysts (group 4, n = 40).
Informed consent was obtained from all participants. The protocol for this project was approved by the ethics committee of Shiraz University of Medical Sciences, Iran. In this study hypertension was defined as 140 mmHg systolic blood pressure and 90 mmHg diastolic blood pressures or the use of antihypertensive therapy. Blood pressure was measured on the right arm with an automated blood pressure monitor while the subject was seated and resting for at least 10 minutes.
DNA preparation
Blood samples (5.0 ml) were drawn from a peripheral vein into an ethylenediaminetetraacetic acid (EDTA) tube by a qualified lab technician. Genomic DNA extraction was performed with the standard salting-out protocol. The quality and quantity of extracted DNA were evaluated with a NanoDrop spectrophotometer at 260/280 nm.
Determination of ACE1, AGT and AT1R genotypes
The ACE1 genotypes (insertions and deletions) were determined with a nested polymerase chain reaction (PCR) protocol. In this method the polymorphism status was first assessed, and then to increase accuracy, another reaction was performed. The second independent reaction was run under the same PCR conditions except for annealing temperature and primer sequence (Table 1).
PCR cycling conditions of ACE1 are represented as temperature and time [minute (m), seconds (s) of denaturation, annealing and extension, × number of cycles].

PCR: polymerase chain reaction; ACE1: angiotensin-converting enzyme gene; RP: reverse primer.
PCR amplification of deletions (D) and insertions (I) of ACE1 were evaluated in a 25 μl reaction mixture containing 200 ng of the template DNA, 7.5 pmol/l of each primer, 0.2 mM of each dNTP, 1.5 mM MgCl2, 2.5 µL10× buffer and 1 U Taq DNA polymerase.
The PCR amplification included 30 cycles of denaturation at 94°C (one minute), annealing at 58°C (one minute) and extension at 72°C (two minutes). The amplification reaction yielded a 335-bp product only in the presence of the I allele (ID heterozygous) whereas no product was found in DD-homozygous individuals.12, 13
The PCR conditions for determining the genotype of AGT were amplification of 200–300 ng of genomic DNA in a 25 μl reaction mixture consisting of 7.5 pmol of each primer, 0.5 mM of each dNTP, 2 mM MgCl2, 2.5 µL10× buffer and 1.25 U Taq DNA polymerase.
The PCR amplification for AGT included 30 cycles at 94°C (30 seconds), 60°C (45 seconds) and 68°C (one minute). The amplified products were analyzed by electrophoresis in 1.5% agarose gel. To identify the AGT M235T genotype, 104-bp PCR products were digested with an MspI restriction enzyme. The 73-bp and 31-bp digestion products were then analyzed by electrophoresis in 3% agarose gel. AGT M235T heterozygotes showed three bands, whereas the T-type variant was not digested and showed only the 104-bp band.
The AT1R A1166C genotype was identified by restriction fragment length polymorphism-PCR amplification that was performed in a 25 μl reaction mixture containing 7.5 pmol forward primer, 7.5 pmol reverse primer, 0.2 mM of each dNTP, 2 mM MgCl2, 2.5 µL10× buffer, 1 U Taq DNA polymerase and 200 ng of the template DNA. The initial denaturation was set up for five minutes at 94°C followed by 35 cycles of denaturation for 30 seconds at 94°C, annealing for 30 seconds at 55°C, and extension for 60 seconds at 72°C. The size of the PCR products was 540 bp for the A allele and 110 bp for the C allele. A negative control containing no genomic DNA and a positive control of known genotype were always used in the set of reactions. The PCR cycling conditions for AT1R and AGT are shown in Table 2.
PCR cycling conditions of AGT and AT1R are represented as temperature and time [minute (m), seconds (s) of denaturation, annealing and extension, × number of cycles].
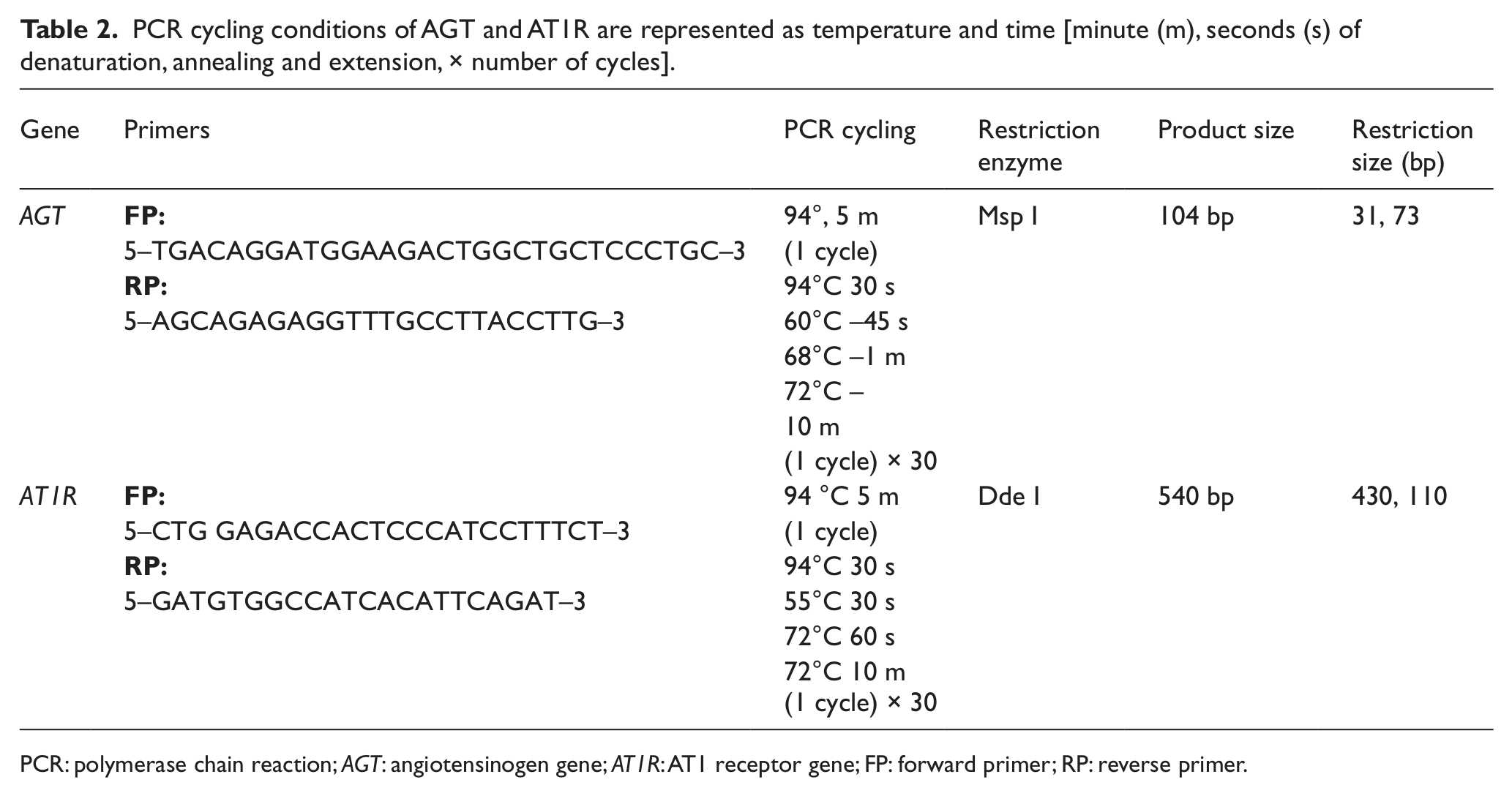
PCR: polymerase chain reaction; AGT: angiotensinogen gene; AT1R: AT1 receptor gene; FP: forward primer; RP: reverse primer.
Statistical analyses
All statistical analyses were performed with SPSS software version 14.0 for Microsoft Windows. Group findings were compared with the chi squared test. P < 0.05 was considered statistically significant.
Results
AGT genotyping
We studied 160 individuals with a mean age of 55 ± 10 years. The participants were divided into four groups. Figure 1 shows the prevalence of the different genetic polymorphisms of AGT in the four groups. None of the genotype distributions followed the Hardy-Weinberg equilibrium. The overall frequency of the M and T alleles was 52.5% and 47.5%, respectively. Table 3 compares allele frequencies for AGT, which was statistically significant between groups 1 and 2 (p value = 0.035)

Genotype and allele distribution of AGT gene polymorphisms in four groups.
Comparison of groups 1 and 3.

OR: odds ratio; CI: confidence interval.
Significant difference*
Figure 2 shows the PCR products of the AGT gene detected with gel electrophoresis.

Gel electrophoresis of AGT gene (73 and 31 bp MM genotype 104, 73 and 31 bp MT genotype and 104 bp TT genotype).
AT1R genotyping
Figure 3 shows the prevalence of the different genetic polymorphisms of AT1R in the four groups. None of the genotype distributions followed the Hardy-Weinberg equilibrium. The overall frequency of the A and C alleles were 76.25% and 23.75%, respectively.

Genotype and allele distribution of AT1R gene polymorphisms in four groups. There were no statistically significant differences.
ACE1 genotyping
Figure 4 shows the prevalence of the different genetic polymorphisms of ACE1 in the four groups. None of the genotype distributions followed the Hardy-Weinberg equilibrium. The overall frequency of the A and C alleles was 36.6% and 63.3%, respectively. Table 4 compares the different allele frequencies for AT1R and ACE1; none of the differences was statistically significant.

Genotype and allele distribution of ACE1 gene polymorphisms in four groups. No statistically significant differences in genotype versus genotype distribution.
Statistical analysis of AT1R and ACE1.

AT1R: AT1 receptor gene; ACE1: angiotensin-converting enzyme gene; OR: odds ratio.
Discussion
Recent advances in molecular biology have provided the genes that are responsible for a number of renal cystic diseases in adults. Some of these genes have been characterized: PKD1 and PKD2 play an important role in renal epithelial development; TSC2 and TSC1, the genes implicated in the pathogenesis of tuberous sclerosis. 18
In addition, genetic variants of the renin-angiotensin-aldosterone system such as variants in the angiotensinogen gene AGT have been intensively studied in different populations with conflicting results in relation to high blood pressure.19-21 Several studies have demonstrated a significant relationship between M235T genotype and hypertension in different human populations. For example, Jeunemaitre et al. found that the T allele was significantly more frequent in patients with hypertension than in controls.20,21 To the best of our knowledge, this is the first study in patients with hypertension and simple renal cysts to show a significant association between the AGT-TT genotype and these clinical entities. This finding suggests an additive role for the AGT gene in the renin-angiotensin-aldosterone system and the process of hypertension and simple renal cysts formation. Moreover, no significant associations were found in the present study between the risk of hypertension (without simple cysts) and the variants of the renin-angiotensin system genes AGT, AT1R and ACE1.
In a meta-analysis of 32 case-control studies, 22 hypertension or a history of hypertension was significantly associated with the T allele. 23 However, when different races were studied separately, the association with hypertension was significant only in Caucasians but not in Asians or blacks.24–27 Because our study population is located in Asia, our results confirm these findings. This variation in the associations highlights the importance of studying these polymorphisms in diverse populations.
Conclusion
Our results, in light of earlier research, show that AGT variants in patients who have both simple renal cysts and hypertension have an important role in the pathophysiology of these clinical entities. Furthermore, the TT variant of AGT in the population of Shiraz (Iran) is an obvious genetic marker for this status, which can be used in personalized and molecular population-based medicine for both treatment and prevention. Although our results comprise the first evidence of an additive role for the TT genotype of the AGT gene in the process of hypertension and simple renal cyst formation in our study population, further studies are needed in different populations.
Footnotes
Acknowledgements
We are grateful to all faculty members and staff of the Medical Genetics Department at Shiraz University of Medical Sciences for their sincere support. We also thank K. Shashok (AuthorAID in the Eastern Mediterranean) for improving the use of English in the manuscript.
Conflict of interest
None declared.
Funding
This work was supported by a research grant from Shiraz University of Medical Sciences. All funding resources in this project were provided by the University of Medical Sciences, Shiraz, Iran.