
Abstract
Introduction:
We studied the effects of angiotensin type 1 receptor blockade (ARB) on formation of new cardiomyocytes, neovascularization and ventricular remodelling after myocardial infarction (MI).
Methods:
Male Wistar rats with MI or sham-operated controls were treated with either losartan or vehicle. Bromodeoxyuridine (BrdU) was given to identify newly formed cardiac cells. Immunohistochemical analysis was used to quantify proliferative and apoptotic cardiomyocytes, vascular structures and c-Kit+ stem/progenitor cells, western blotting to evaluate gene expression, and planimetry and echocardiography to assess cardiac structure and function.
Results:
The number of BrdU+ cardiomyocytes increased similarly in the vehicle and losartan treated MI groups. The number of apoptotic or proliferating cardiomyocytes did not differ between losartan and vehicle treated rats. Losartan induced an increase in capillary and BrdU+ vascular densities in the infarct border zone. Losartan treatment completely prevented post-MI cardiac hypertrophy. In the non-infarcted myocardium the amount of all BrdU+ cells (including non-cardiomyocyte cells) was highest in the vehicle treated MI rats at week 4.
Conclusions:
The number of newly formed cardiomyocytes increased after MI. Angiotensin II blockade neither stimulated nor prevented cardiomyocyte regeneration. ARB treatment increased vascular densities in the infarct border zone and modulated remodelling of the non-infarcted myocardium preventing effectively post-MI cardiac hypertrophy.
Keywords
Introduction
Myocardial infarction (MI) is followed by diverse cardiac structural changes including cardiomyocyte hypertrophy, enhanced formation of interstitial fibrosis as well as loss of cardiomyocytes due to apoptosis.1–3 This post-MI remodelling process aims at compensating the loss of cardiac tissue after MI but is not necessarily able to restore the functional capacity of the heart back to normal 4 depending on the size of the initial myocardial injury. After a large MI, the chronic congestive cardiac failure that ensues is characterized by continuous loss of cardiomyocytes, progressive cardiac dilatation, further deterioration of cardiac function and, finally, poor prognosis.5,6
The traditional concept has long been that mature cardiomyocytes have lost their capacity to divide and are thereby unable to replace and repair the loss of cardiac tissue after myocardial infarction. On the other hand, it has been calculated that continuous apoptotic loss of cardiomyocytes at a rate of 0.1–0.3% would lead to absolute decrease in the amount of cardiac cells and loss of cardiac tissue within a couple of years unless new cardiac cells were generated. 7
Therefore, it has been suggested that a regenerative system must exist to replace the apoptotic loss of cardiac cells. Supporting this concept, recent research has indeed been able to show that the heart possesses regenerative capacity. The heart contains resident progenitor cells (cardiac stem cells) which can be activated to proliferate and to form new cardiac structures after myocardial injury.8–10
The renin–angiotensin system (RAS) has a pivotal role both in the post-MI cardiac remodelling process and in the pathogenesis of cardiac failure. 11 Local cardiac RAS is activated in the infarcted myocardium12–14 and is also involved in the remodelling process of the non-infarcted cardiac tissue after MI. 15 Numerous clinical trials after MI and in patients with chronic heart failure have demonstrated benefits of RAS-blockade either with angiotensin-converting enzyme (ACE) inhibitors or angiotensin type 1 (AT1) receptor antagonists in the treatment of these patient groups.16–18 However, cardiovascular morbidity and mortality are still significantly higher than expected in patients with heart failure as compared with normal ageing despite current optimal medical therapy including a RAS-inhibitor and a beta-blocker. Thus, additional treatment strategies are needed to further reduce the excess morbidity in these patients. Findings on cardiac stem/progenitor cells have opened up completely new possibilities to prevent and treat heart failure after cardiac injury. By combining measures to enhance endogenous cardiac regeneration19,20 with current established treatments for cardiac diseases the treatment results could improve significantly in the future. At the same time, more research is also needed to understand how current cardiovascular drugs influence the cardiac regenerative process.
At present the role of intracardiac RAS in the regulation of cardiac regeneration and repair after MI is not fully understood. 11 Even less is known about the effects of RAS-blockade on proliferation and kinetics of cardiac progenitor cells after myocardial injury. Angiotensin II may have both beneficial and potentially harmful cardiac effects after MI including growth and cell proliferation promoting, pro-inflammatory, pro-fibrotic and angiogenesis-stimulating effects.21,22 Therefore, more information is needed on the effects of angiotensin blockade on the cardiac regenerative process after myocardial injury. The present study was undertaken to explore the effects of losartan, a selective AT1-receptor antagonist, on formation of new cardiomyocytes and vascular structures as well as on left ventricular remodelling after experimental MI in rats. Ki67-staining was used to show and quantify proliferative cells and bromodeoxyuridine (BrdU)-staining19,23 to identify newly formed cells. By giving BrdU after induction of myocardial infarction it is possible to quantify the amount of newly formed cardiomyocytes and other cardiac cells, including vascular cells, as judged by positivity for BrdU and cell-specific markers in immunohistochemical stainings.
Materials and methods
Experimental myocardial infarction and treatments
The left anterior descending coronary artery (LAD) was ligated to produce MI. The experimental protocol was approved by Helsinki University Laboratory Animal Committee and the Province State Office of Southern Finland. Rats were anaesthetized with medetomidine (Domitor, Orion, Turku, Finland; 0.5 mg/kg subcutaneously (s.c.)) and ketamine (Ketalar, Parke Davis, Barcelona, Spain; 60 mg/kg s.c.). The rats were connected to a respirator through a tracheotomy and the heart was exposed through a lateral thoracotomy (in the tenth intercostal space). The LAD was ligated about 3 mm from its origin and the thorax was closed. The anaesthesia was partially antagonized with antipamezole hydrochloride (Antisedan, Orion; 0.80 mg/kg intramuscularly (i.m.)). The body temperature was maintained stable using a thermal plate throughout the operation. Rats were hydrated post-operatively with 5 ml of physiological saline s.c. Buprenorphin (Temgesic, Schering-Plough, Brussels, Belgium; 0.015 mg/rat s.c.) was given twice a day for three days for analgesia. The sham-operated rats underwent the same procedure, except for the ligation of the coronary artery.
A total of 101 Wistar male rats (Harlan Laboratories, Boxmeer, Netherlands) weighing 228–321g were used in the study. Rats were randomized into four groups (MI+losartan, MI+vehicle, sham+losartan and sham+vehicle) 12–16 h after the operation. The number of rats in each group and time point was 10–12. Losartan (MK0954, Merck & Co. Inc., Whitehouse Station, NJ, USA) was mixed into the powdered food 250 mg/kg. Mean estimated dose was 40 mg/kg. The rats in the vehicle groups were given the same food without losartan. 5-bromo-2′-deoxyuridine (BrdU, Sigma-Aldrich, Saint Louis, MO) was added to drinking water 1 g/l. Consumption of food and water was measured to calculate the actual doses. The perioperative mortality rate was 9.87 % and two rats died later during the experiment.
Rats were sacrificed at one or four weeks after the operation under pentobarbital (Mebunat, Orion; 55 mg/kg i.p.) anaesthesia. The relative weight (mg/g body weight) of the heart, lungs and kidneys were determined. Blood samples were collected into tubes containing Na2EDTA and aprotinin. The heart was cut into 2 mm transverse slices below the point where the coronary artery was ligated. The myocardial samples were either frozen in liquid nitrogen and stored at −80oC or fixed in 4% neutral buffered formalin for 24 h, embedded in paraffin.
Echocardiography
Transthoracic echocardiography was performed at one and four weeks (Toshiba Ultrasound, Tokyo, Japan) under isoflurane anaesthesia (AGA, Riihimäki, Finland) in a blinded fashion by the same technician.
Plasma renin activity
Plasma renin activity was determined using angiotensin I radioimmunoassay (RIA) kit (Diasorin, Vercelli, Italy) according to the manufacturer’s instructions.
Western blotting
Protein levels in the infarct areas of rat hearts were studied using Western blotting as described. 24 The membranes were probed with anti-hepatocyte growth factor (HGF-α, Santa Cruz Biotechnology, Santa Cruz, CA, USA), anti-vascular endothelial growth factor A (VEGF-A, rabbit polyclonal, Millipore, Temecula, CA, USA).
Infarct size
The infarct size was determined planimetrically from transverse left ventricular sections stained with Weigert van Gieson as the ratio of the infarct tissue or scar to the length of the entire left ventricle as described. 25
Immunohistochemical analysis
To identify cardiomyocytes, vascular structures, new (BrdU+) cells, apoptosis and c-Kit positive cells immunofluorescent staining was performed. Transverse paraffin sections (5 µm) from the mid-ventricular level of rat hearts were used in immunohistochemistry. Two sections per rat heart were studied. To obtain quantitative results, the proportions of the infarct area, border area and remote non-infarcted myocardium of the left ventricle were determined and the results were counted for each of these areas. Viable myocardium extending 0.5–1 mm from the infarct area was considered to represent the infarct border area. The non-infarcted myocardium over 1 mm from the infarct area was determined as remote area. In all sections nuclei were stained with 4′6-diamino-2-phenylindole (DAPI) (Life Technologies, Molecular Probes, Carlsbad, CA, USA). The immunolabelled sections were examined with a Leica DM 4500B fluorescent microscope (Leica Microsystems, Wetzlar GmbH, Wetzlar, Germany) or Zeiss LSM 510 Meta confocal microscope.
Caspase-3 (Casp3) was used as a marker for apoptosis. Double staining with antibodies for Casp3 (rabbit polyclonal, Cell Signaling, Danvers, MA, USA) and cardiac myosin heavy chain (MHC, mouse monoclonal, Millipore, Upstate, Billerica, MA, USA) was utilized. All the Casp3+ and MHC+ cardiomyocytes were counted from the whole section in sham-operated rats or the remote and border area of each section in infarcted rats and compared with the amount of all myocytes in the same area. The amount of total myocytes in a certain section was evaluated by counting the amount of myocytes per mm2 (from 6–15 randomly selected microscopic fields) and comparing this with the size of the whole area.
To identify capillaries and arteries in the infarct area, border area and remote myocardium, double staining for α-smooth muscle actin (α-SMA, mouse monoclonal, Dako Cytomation, Glostrup, Denmark) and von Willebrand factor (vWF, rabbit polyclonal, Millipore, Chemicon, Billerica, MA, USA) was performed. The vascular and capillary densities were analysed from 6–15 randomly selected microscopic fields (200× or 400× magnification) photographed from each of the infarct, border and remote areas.
BrdU positivity was used to identify cells formed after coronary ligation or sham operation. The cells were stained using anti-BrdU (mouse monoclonal, Roche Diagnostics, Mannheim, Germany). Double staining with antibodies for BrdU and troponin I (rabbit polyclonal, Santa Cruz Biotechnology, Santa Cruz, CA) was performed to identify newly formed cardiomyocytes. BrdU+ cells and cardiomyocytes (BrdU+, troponin+) were counted in the same manner as described above for Casp3+ cell counting. In addition the number of newly formed vascular structures was analysed using double staining for BrdU and vWF. C-Kit positive cells were stained with c-Kit antibody (rabbit polyclonal, Dako Cytomation) and counted.
For Ki67 staining, samples were embedded in paraffin and cut into 4-µm-thick sections. Immunostaining was performed using a Ventana Discovery Automate (Ventana Medical Systems Inc., Tucson, AZ, USA). Ki67 (anti-Ki67; Thermo Fischer Scientific, Labvision, Fremont, CA, USA) proliferation-associated antigens were double stained for myocytes using antibody for tropomyosin (Labvision). The Ki67+ myocytes were manually counted from the border and the remote area of each section and compared with the amount of all myocytes in the border or remote area. The number of total myocytes in a certain section was evaluated by counting the number of myocytes per mm2 (from 6–15 randomly selected microscopic fields) and comparing it with the size of the whole area.
Cardiomyocyte size was analysed by measuring the cross-sectional area of 100 cardiomyocytes per heart by using ImageJ software. The cardiomyocytes cut in short axis with a visible nucleus were measured from tissue sections stained with anti-MHC and DAPI.
The secondary antibodies were Alexa Fluor 488- conjugated goat anti-mouse or donkey anti-goat IgG (Molecular Probes), Alexa Fluor 546-conjugated goat anti-rabbit IgG (Molecular Probes) and tetramethyl rhodamine isothiocyanate (TRITC)-conjugated swine anti-rabbit IgG (Dako Cytomation).
Statistical analysis
Data are presented as mean ± SEM. Differences between groups were analysed by one-way analysis of variance (ANOVA) followed by the Tukey test or Student’s t test or nonparametric Kruskall–Wallis test followed by Mann–Whitney U test. Differences were considered significant at p value <0.05
Results
Body weight, infarct size, cardiac weight and pulmonary weight
There were no statistical differences between groups in body weight either before the operation or at the studied time points. The infarct size did not differ between LAD-ligated groups (MI vehicle group versus losartan treated MI rats) (Table 1).
Body weight, infarct size, relative heart weight, myocyte cross-sectional area, relative lung weight and plasma renin activity one and four weeks after sham operation or coronary artery ligation.

Values are mean ± SEM.
p<0.05 versus vehicle treated sham group at corresponding time point.
p<0.01 versus vehicle treated sham group at corresponding time point.
p<0.05 versus vehicle treated MI group at corresponding time point.
p<0.01 versus vehicle treated MI group at corresponding time point.
p<0.001 versus vehicle treated MI group at corresponding time point.
n.d.: not determined; MI: myocardial infarction.
Relative heart weight was significantly higher in the infarcted rats compared with sham operated controls at both time points. In the losartan treated MI rats, the heart index was lower (2.71±0.064 g/kg, p<0.001) compared with vehicle treated-rats with MI (3.501±0.173) at four weeks (Table 1). The relative lung weight was higher in infarcted rats compared with sham-operated rats at one week (Table 1).
Cardiac function (echocardiography)
When comparing MI and sham operated groups, expected echocardiography changes were found. At four weeks both end diastolic and systolic volumes increased significantly in MI rats (Table 2). In addition, fractional shortening was lower and ejection fraction tended to be lower in MI rats at week 4. No statistically significant differences were found between losartan versus vehicle treated MI rats at weeks 1 or 4 (Table 2).
Cardiac function determined by echocardiography at one and four weeks after sham operation or coronary artery ligation.

Values are mean + SEM.
p<0.05 versus vehicle treated sham group at corresponding time point.
p<0.01 versus vehicle treated sham group at corresponding time point.
MI: myocardial infarction; EF: ejection fraction; CO: cardiac output; FS: fractional shortening; EDV: end diastolic volume; ESV: end systolic volume; IVSTd: diastolic intraventricular septum thickness; IVSTs: systolic intraventricular septum thickness; LVIDd: diastolic left ventricle internal dimension; LVIDs: systolic left ventricle internal dimension
Cardiomyocyte hypertrophy
At week 4 the myocyte cross-sectional area increased in MI groups compared with sham operated groups (Table 1). In losartan treated MI rats the myocyte cross-sectional area tended to be smaller compared with vehicle treated MI rats but differences were significant neither at week 1 nor at week 4.
Plasma renin activity
As expected, treatment with the angiotensin type 1 antagonist losartan stimulated plasma renin activity (Table 1), reflecting blockade of the RAS. There were no differences between sham operated and MI groups in plasma renin activity.
Cardiomyocyte regeneration, neo-vascularization and apoptosis
The number of BrdU+ cardiomyocytes (Figure 3(a) and 3(b)) increased four- to eight-fold (p<0.05 and p<0.01 versus sham) in the infarct border zone after MI at weeks 1 and 4 (Figure 1(a)). Losartan treatment neither stimulated nor prevented neoformation of cardiomyocytes after MI (Figure 1(b)).

The number (%) of BrdU+ cardiomyocytes (a) and all BrdU+ cells (b) in the left myocardium after myocardial infarction (MI) (n=9–10 at weeks 1 and 4, respectively).
The number of proliferative (Ki67+) cardiomyocytes (Figure 3(d)) increased five-fold in the infarct border zone at week 1 (p<0.05 versus sham) after MI (Table 3). The number of Ki67+ cardiomyocytes did not differ between losartan and vehicle treated MI rats. Only sporadic c-Kit+ progenitor cells could be detected in losartan and vehicle treated groups and therefore statistical differences between the groups could not be evaluated.
Amount of proliferating and apoptotic cardiomyocytes at one and four weeks after sham operation or coronary artery ligation.
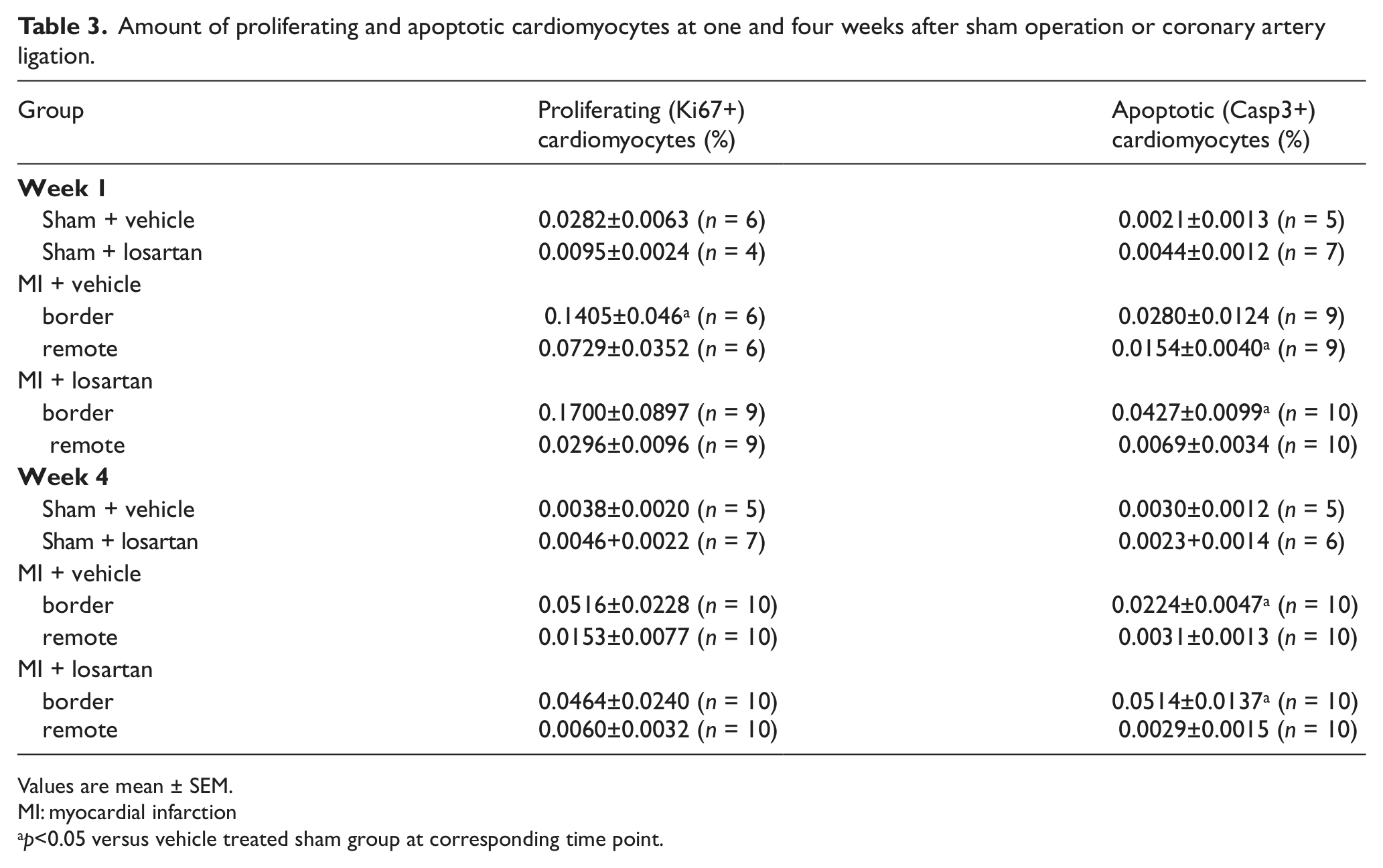
Values are mean ± SEM.
MI: myocardial infarction
p<0.05 versus vehicle treated sham group at corresponding time point.
Compared with vehicle treated MI rats, losartan treatment induced formation of new vascular structures (Figure 3(c)) in the infarct border zone. Capillary density (vWF+) was 1.3-fold higher in the losartan MI group (1418±61.2, vessel count per mm2) compared with vehicle treated MI rats (1072±160, p<0.05, Table 4) at week 4. The amount of newly formed vessels (BrdU+, α-SMA+) was five-fold higher in the losartan treated MI group (3.85±1.19, % of total) versus the vehicle treated MI group (0.749±0.508, p<0.05, Table 4).
Vascular density and neovascularization four weeks after myocardial infarction (MI).

Values are mean ± SEM and results are reported as vessel count per mm2.
p<0.05 versus same area in vehicle treated MI group.
The amount of all BrdU+ cells (including also non-cardiomyocytes) was increased in the infarct border zone of MI rats at week 1 compared with sham operated controls (p<0.05, Figure 1(b)). At week 4 the amount of BrdU+ cells increased also in the remote zone (p<0.01 versus sham). Losartan treatment did not affect the number of all BrdU+ cells in the infarct border zone (Figure 2(a)). At week 4, the total number of new cells in the remote zone tended to be lower in the losartan MI group (3.11±0.53%) compared with vehicle treated MI rats (5.16 ±1.02%, p=0.08, Figure 2(b)).

The effect of losartan treatment on the formation of BrdU+ cardiomyocytes (a) and on the number (%) of all BrdU+ cells in the left myocardium (b) after myocardial infarction (MI) (n=10 at weeks 1 and 4). C: control; refers to corresponding vehicle treated MI rats (n=9–10 at weeks 1 and 4, respectively).
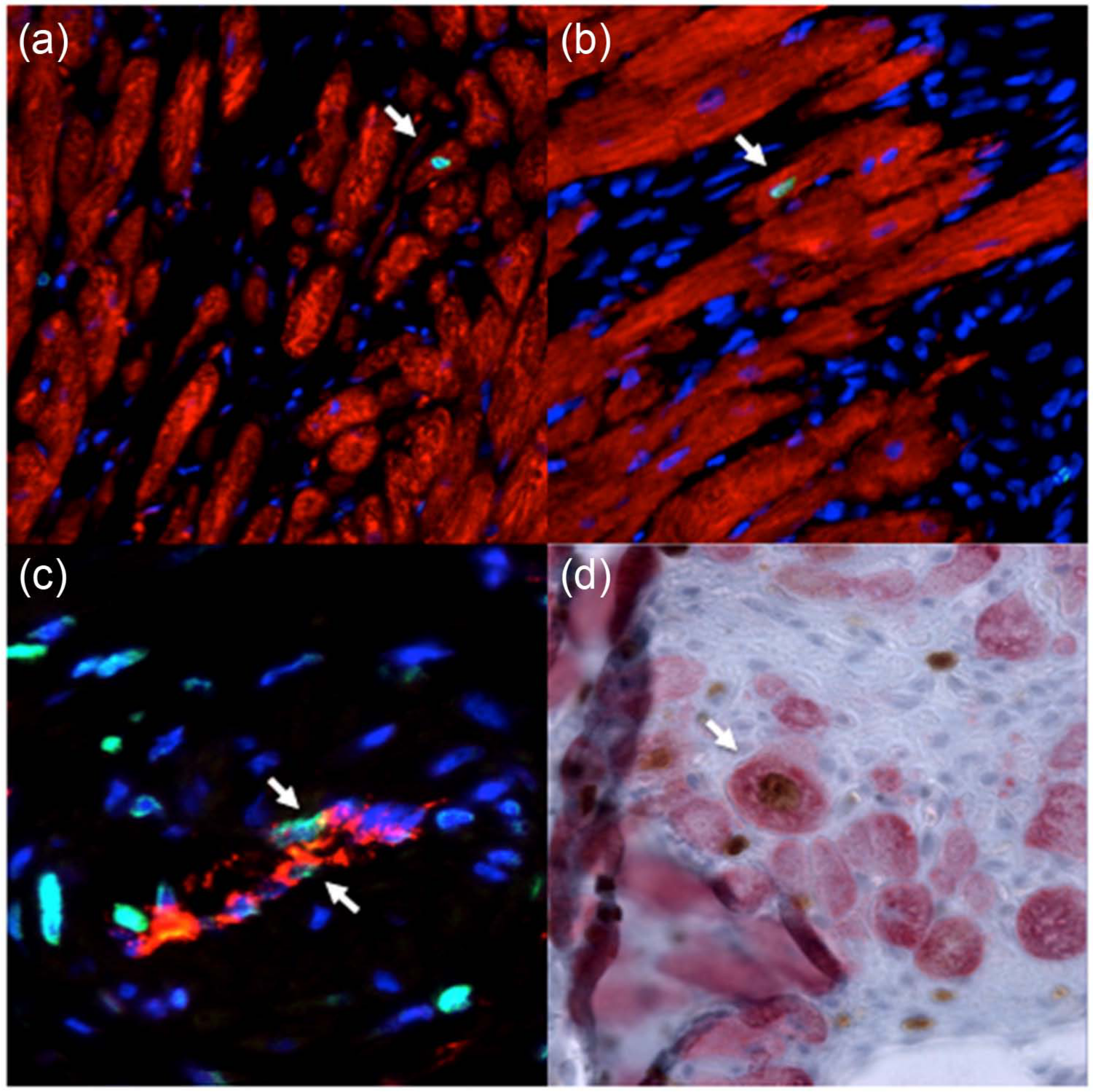
Cardiomyocyte regeneration and neo-vascularization after MI. (a) and (b) Newly formed BrdU+ (green)/troponin+ (red) cardiomyocyte (arrow) in the infarct border zone after MI. (c) Newly formed BrdU+ (green)/vWF+ (red) vascular structure (arrows) in the infarct border zone after MI. (d) Proliferating Ki67+ (brown) and MHC+ (red) cardiomyocyte (arrow).
The number of apoptotic (Casp3+) cells was higher mainly in the infarct border zone as compared with sham-operated controls (p<0.05, Table 3). The rate of apoptosis did not differ between losartan versus vehicle treated MI groups.
HGF-α and VEGF-A
No differences in HGF-α (HGF-α/actin: MI+losartan 1.22± 0.32 at week 1, 1.01+0.16 at week 4 vs. MI+vehicle 1.00±0.28, 1.15±0.37, respectively) and VEGF-A (VEGF-A/actin: MI+losartan 1.10±0.53 at week 1, 1.33±0.25 at week 4 vs. MI+vehicle 1.50±0.38, 1.48±0.31, respectively) levels were found between losartan and vehicle treated MI groups at weeks 1 or 4.
Discussion
Formation of new cardiomyocytes increased markedly in the infarct border zone after coronary artery ligation, confirming previous findings on regenerative potential of the heart. Several studies have shown that the heart contains stem/progenitor cells that are capable of activating, proliferating and forming new cardiac cells and structures after myocardial damage.8–10,19 We used continuously administered BrdU, an easily detectable compound for DNA-labelling during cell division, 23 to obtain a cumulative estimate of new cardiomyocytes and other newly formed cardiac cells during the post MI period. We found that significant amounts of BrdU-labelled cardiomyocytes and vascular structures are formed in the infarct border zone after MI but not in the remote, non-infarcted myocardium compared with sham operated control rats. The formation of BrdU positive cardiomyocytes continued throughout the four week post-MI study period, being three-fold higher at week 1 and eight-fold higher at week 4 compared with sham operated controls. This finding was confirmed by Ki67-staining giving an estimate of proliferating cells at the time points studied. The amount of Ki67 positive cardiomyocytes was increased during the early post MI period at week 1 post MI in the infarct border zone but not in the remote myocardium.
The fraction of cardiomyocytes labelled by Ki67 was higher than the fraction of BrdU-labelled cardiomyocytes. This somewhat unexpected finding may result from the fact that BrdU was administered in drinking water instead of daily injections. Slow delivery of BrdU from drinking water might favour its uptake in rapidly proliferating tissues, limiting its actual delivery to cardiac cells.
Treatment with the AT1 receptor blocker (ARB) losartan did not further increase the formation or proliferation of cardiomyocytes in the infarct area compared with vehicle treated rats with MI as judged by BrdU and Ki67 stainings. The BrdU method may underestimate the total number of new cardiomyocytes generated during the study period if apoptotic or necrotic cardiomyocyte loss is accelerated at the same time. However, the rate of apoptosis in the infarct border zone did not differ between losartan and vehicle treated MI rats. The number of c-Kit positive cardiac stem/progenitor cells remained unchanged as well. No clear sites of accumulation of c-Kit positive cells were found in the MI rats at the areas and time points analysed in the present experiment.
The role of the RAS in the regulation of cardiac remodelling and repair after myocardial injury is complex and still poorly understood. 11 Expression of several components of RAS, including AT1-receptors, is up-regulated in the infarct area13,14 suggesting an important role for the local cardiac RAS in the scar formation, inflammatory response and repair of the damaged myocardium after MI. 21 In theory, AT1-receptor blockade may have both negative and positive effects on the cardiac reparative process after MI. By inhibiting the well established growth promoting effects of angiotensin II ARBs could even prevent neo-formation of cardiomyocytes. On the other hand, the effects of angiotensin II and other angiotensin peptides on non-AT1 receptors, notably AT2 and angiotensin 1-7 (Mas) receptors, are not blocked by ARBs. These non-AT1-mediated effects have been suggested to counterbalance the AT1 receptor mediated effects of angiotensin II. 22 Thus, the net effect of RAS blockade using specific ARBs like losartan on the myocardial healing and repair after MI is likely to be complex and multifaceted. According to present results treatment with an ARB does not specifically influence the generation of new cardiomyocytes after MI.
AT1 receptor mediated effects of angiotensin II have been found to stimulate angiogenesis in several disease models. 26 However, studies elucidating the role of AT1 receptors in the regulation of angiogenesis after MI have been contradictory, suggesting both stimulatory 21 and suppressive 27 effects of angiotensin II on angiogenesis in the infarcted myocardium. In the present study, AT1 receptor blockade with losartan induced an increase both in capillary density and in BrdU+ vascular density in the infarct border zone compared with vehicle treated rats with MI. We also studied gene expression of VEGF and other potential factors mediating the effects of angiotensin II on angiogenesis utilizing real time RT-PCR, RT-PCR array (unpublished results) and Western blotting, but no changes in the gene expression of proangiogenic cytokines or growth factors in losartan treated MI rats compared with vehicle treated controls were found. This suggests that other factors are also involved in the regulation of neo-vascularization in the peri-infarct area after MI. Alternatively, the time points chosen, that is, one and four weeks after coronary ligation, were not optimal to demonstrate the possible link between angiotensin II and proangiogenic cytokines after MI in the present experiment.
As expected, cardiac systolic function was compromised in coronary ligated rats with MI, which averaged 35–40% of the left ventricle in the present experiment. Losartan treatment did not improve systolic function, evaluated by echocardiography, during the early post-MI period studied. It is tempting to speculate that this result in fact reflects the lacking efficacy of losartan on cardiomyocyte regeneration in this experiment. This is in line with clinical post-MI studies in which no clear benefits with ARBs, at least when compared with established treatment of post-MI heart failure including ACE-inhibitors,28,29 have been obtained.
The effects of angiotensin blockade on cardiac tissue after MI appeared to be different in infarcted and non-infarcted myocardium, as suggested by Sun. 11 Contrary to the less evident effects of losartan on cardiac tissue changes in the infarct zone, losartan treatment influenced the non-infarcted, remote myocardial in several ways. The observed increase in relative cardiac weight after MI in vehicle treated rats was completely prevented in rats treated with losartan. The myocyte cross-sectional area tended to be smaller in losartan treated rats, suggesting inhibitory effects on cardiomyocyte and left ventricular hypertrophy as reported previously in experimental and clinical studies with ARBs.16–18,30 In addition, the overall increase in cell proliferation after MI, as judged from the amount of all BrdU positive cells in the remote myocardium outside the infarct area, did not differ from sham-operated controls in the losartan treated rats with MI. These effects on post-MI cardiac remodelling and cell proliferation are in agreement with previous studies showing that treatment with ARBs modulates the adverse remodelling of the non-infarcted myocardium after MI.31–33 ARBs have also been shown to prevent development of interstitial and perivascular fibrosis after MI (not studied in the present experiment). Interestingly, relative lung weight was lower in losartan treated rats with MI compared with corresponding vehicle treated controls, suggesting improved overall cardiac function, although separate echocardiographic parameters did not differ significantly between losartan and vehicle treated MI groups. In the long term treatment of chronic heart failure following myocardial injury the modulating effects of AT1 receptor blockade on post MI remodelling are considered to be beneficial in reducing the occurrence of adverse cardiac events.15,18
In summary, the number of BrdU-labelled cardiomyocytes increased markedly in the infarct border zone after coronary artery ligation. The enhanced formation of new cardiomyocytes continued throughout the four-week post MI study period. Treatment with the AT1 receptor antagonist losartan neither stimulated nor prevented cardiomyocyte regeneration. On the other hand, AT1 receptor blockade stimulated formation of new vascular structures, inducing an increase both in capillary and BrdU+ vascular density in the infarct border zone compared with vehicle treated rats with MI. In addition, losartan effectively influenced remodelling of the non-infarcted myocardium, preventing completely post MI cardiac hypertrophy. In future studies, RAS blockade should be tested in combination with specific tools to stimulate cardiac regeneration,19,20 aiming at both prevention of the adverse remodelling of the non-infarcted myocardium and, at the same time, facilitation of repair of the injured peri-infarct zone after myocardial infarction.
Footnotes
Acknowledgements
We thank Riina Hatakka and Irina Suomalainen for expert technical assistance.
Conflict of interest
None declared.
Funding
This work was supported by the Hospital District of Helsinki and Uusimaa, the Finnish Foundation for Cardiovascular Research, the Sigrid Jusélius Foundation, the Paavo Nurmi Foundation and Finska Läkaresällskapet.