
Abstract
Objective:
The objective of this paper is to investigate a profile on circulatory renin−angiotensin system (RAS) activity in hypercholesterolemic (HC) patients treated with statins.
Methods:
Eighteen primary HC patients and 18 sex- and age-matched healthy adults were included in this study as controls. Total cholesterol (TC), triglyceride (TG), LDL-C, blood glucose, angiotensin-converting enzyme (ACE) activity, and angiotensin II (Ang II) levels were measured before and four and eight weeks after beginning statin treatment in the HC group. Similar measurements were taken in the control group at baseline.
Results:
At baseline, TC, TG and LDL-C levels, as well as ACE activity and Ang II concentrations, were significantly higher in the HC group than in the control group. Based on the baseline data collection of 36 participants, there were significant positive correlations between ACE activity and TC (r = 0.54) or LDL-C (r = 0.51), and between Ang II level and TC (r = 0.34) or LDL-C (r = 0.27). TC, LDL-C, Ang II (35.46±14.49 vs 71.10±20.47 pg/ml, p < 0.05) levels and ACE activity (108.9±51.9 vs 180.1±71.3 U/L, p < 0.05) were decreased in HC patients eight weeks after starting statin treatment. In HC patients, RAS activity correlated positively with TC and LDL-C levels before and after treatment.
Conclusions:
In HC patients, lowering serum cholesterol with statins is associated with decreased circulatory RAS activity.
Introduction
Hypercholesterolemia (HC) is a well-validated risk factor for the development of atherosclerotic diseases. Activation of the renin-angiotensin system (RAS) has been considered an independent mechanism in the development of atherosclerotic diseases. 1 Apart from a study performed in Watanabe heritable hyperlipidemic rabbits that did not find a significant correlation between blood lipids and angiotensin-converting enzyme (ACE) levels in lung tissue, 2 most data from animal models of atherosclerosis have shown consistently that HC increases significantly the activity of RAS.3–6 This association is also found in human beings. 6
In patients with HC, major therapeutic efforts with statins have been directed at lowering plasma concentrations of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C). Statins also may elicit other beneficial effects, such as anti-inflammation and immunomodulation. 7 Interestingly, a recent study indicated that simvastatin can inhibit ACE activity in rats with aortic stenosis. 8 However, another study in healthy subjects showed that atorvastatin treatment did not influence plasma Ang II or Ang-(1-7) levels. 9
There is little information regarding the dynamic relationship of blood lipids with circulatory RAS activity during statin treatment in HC patients. However, there may be a close association between RAS activity and blood lipid concentrations. To test this hypothesis, we evaluated the relationship between blood lipids and ACE activity, and Ang II concentrations in HC patients.
Methods
Subjects
This study was approved by the ethics committee of the Second Affiliated Hospital of Nanchang University and all participants submitted their consent to this study.
At baseline, blood pressure (BP) and heart rate (HR) were measured and an electrocardiogram was performed on all participants. The inclusion criteria for HC patients were TC ≥ 5.72 mmol/l and LDL-C ≥ 3.64 mmol/l. Patients showing serum cholesterol elevations received appropriate diet education immediately at the beginning of the study, and then serum blood lipids were repeated four weeks later. Patients with two abnormal lipid examinations were included in the HC group. Eighteen HC patients comprised the HC group. Eighteen age- and sex-matched healthy individuals were selected as controls (control group).
The HC patients were randomly divided into rosuvastatin (5 mg/d) and atorvastatin (10 mg/d) treatment for eight weeks. During the observation period, the patients were asked to stay on their usual diet and salt intake, and were not allowed to take any other medications.
Blood sampling and BP measurement
Twenty minutes after resting in the sitting position, fasting venous blood samples were taken to measure TC, triglyceride (TG), LDL-C, high-density lipoprotein cholesterol (HDL-C), blood glucose (GLU), and hepatic and renal function (Olympus AU2700).
Anticoagulated blood with heparin was centrifuged at 3000 rpm for 10 minutes and the plasma was kept in a refrigerator at −70°C. Plasma ACE activity was measured by the enzymatic continuous monitoring method (furanacryloyl-L-phenylalanylglycylglycine (FAPGG) assay) through the Beckman CX7. 10 Ang II level was measured by radioimmunoassay with γ-events-per-unit-time meter (SN-682). The patients remained unaware of the results. Measurements of these parameters were repeated at four and eight weeks after beginning statin treatment in HC patients.
Statistical analysis
All data were analyzed by SPASS 12.0 and expressed as mean ± SD. The main results were examined by the normality test and homogeneity of variance test. The data with normal distribution were analyzed with a t test followed by analysis of variance (ANOVA). Non-normal distribution data were compared group-in-group by Wilcoxon-signed rank test and group-to-group by Kruskal-Wallis H test; linear correlation analysis was used to determine the correlation. Statistical significance was accepted for p values < 0.05.
Results
There were no significant differences in systolic blood pressure (SBP), diastolic blood pressure (DBP) and HR between the two groups at baseline (Table 1).
Comparison of general data between the hypercholesterolemia and control groups.
HC: hypercholesterolemia; F/M: female/male; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate.
At baseline, the concentrations of not only TC, TG and LDL-C, but also of ACE and Ang II, were significantly higher in the HC group than in the control group. In the HC group, statin treatment in the first four weeks significantly decreased TC and LDL-C concentrations. ACE activity and Ang II levels were also reduced. After eight weeks of treatment, the above parameters were similar between the HC and control groups. The serum GLU level did not change significantly after eight weeks of treatment in the HC group (Table 2).
Blood lipids and RAS parameters between the control and hypercholesterolemia groups.

RAS: renin−angiotensin system; HC: hypercholesterolemia; W: week; TC: total cholesterol; TG: triglyceride; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; GLU: blood glucose; ACE: angiotensin-converting enzyme; Ang II: angiotensin II; ND: not done; acomparison with control; bcompared with W 0: p < 0.05.
Figure 1 shows the correlations between blood lipids, ACE activity, and Ang II levels in all 36 participants at baseline. Positive correlations were shown between ACE activity and TC or LDL-C. Similarly, positive correlations were also shown between Ang II and TC or LDL-C. However, both TG and HDL-C were not significantly correlated with Ang II level or ACE activity.
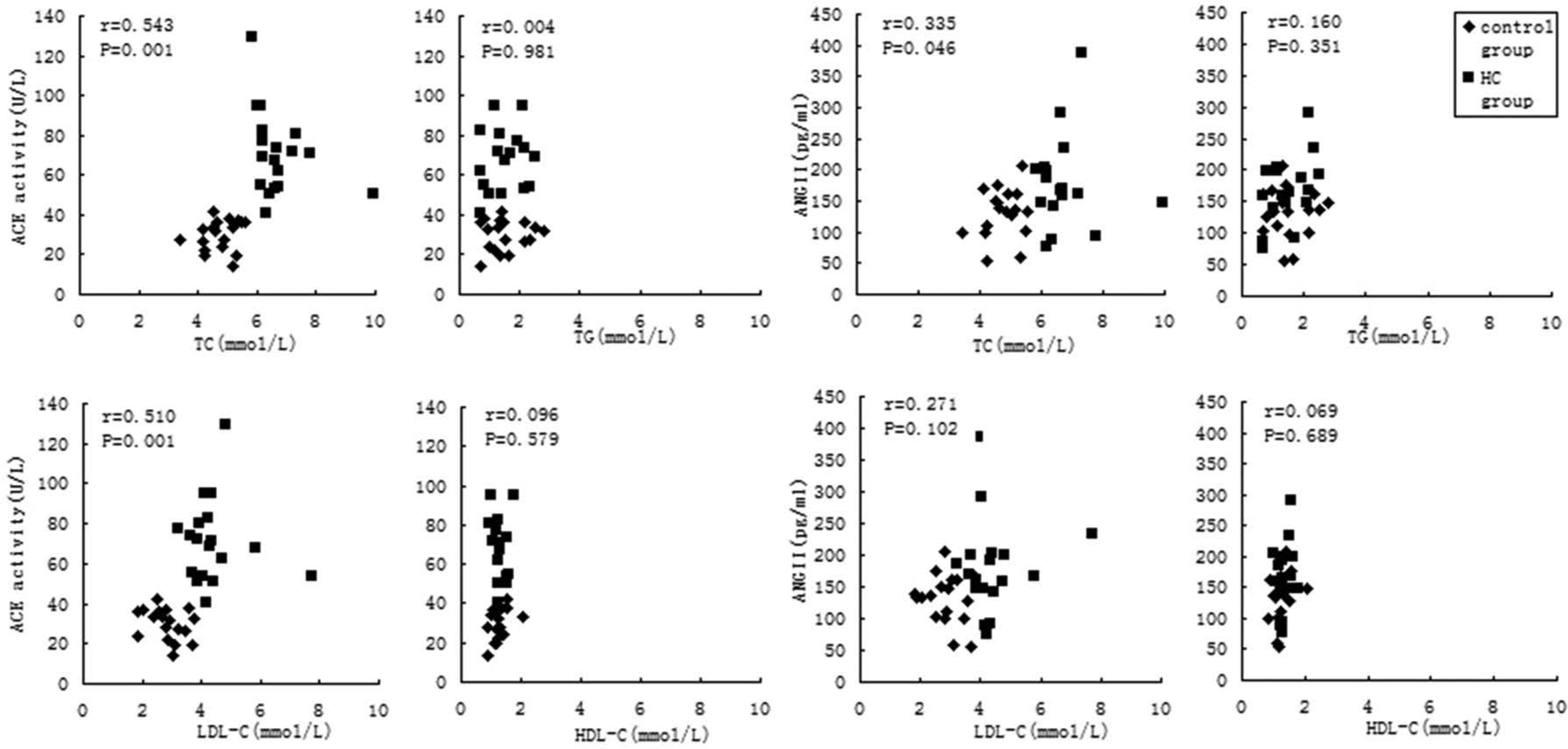
The correlation between blood lipids and ACE activity and Ang II levels in all 36 subjects at baseline.
In the measurements before and at the fourth and eighth week after statin treatment in the HC group, positive correlations were shown between ACE activity and TC or LDL-C, as well as between Ang II level and TC or LDL-C. Similarly, neither TG nor HDL-C was significantly correlated with Ang II level or ACE activity (Figure 2).
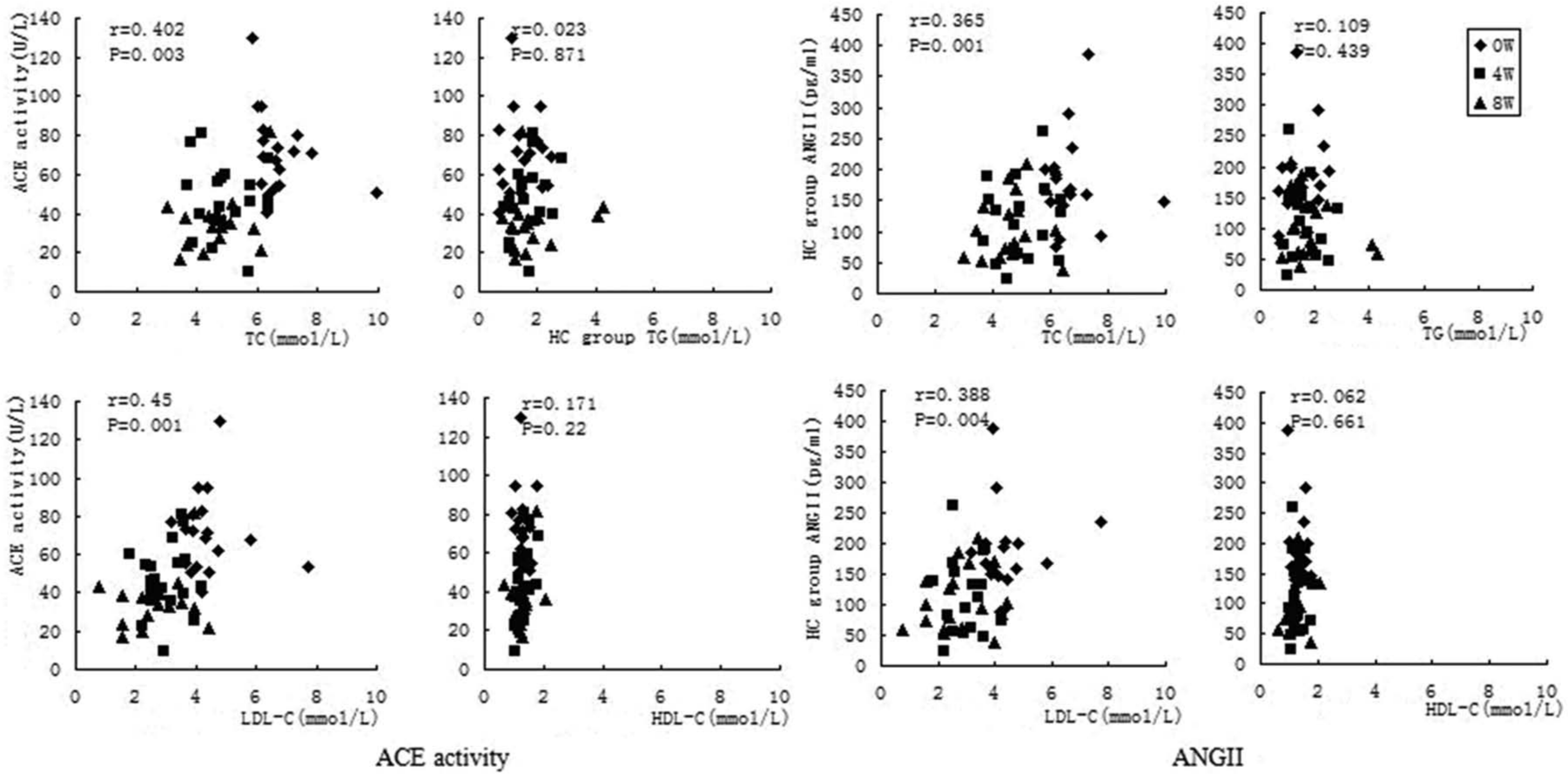
Correlation between blood lipids and RAS activity during the observation period in the 18 HC patients.
Discussion
This study demonstrates that the circulatory RAS is activated in patients with HC, as demonstrated by the significantly higher ACE activity and Ang II levels in the HC group. These results are consistent with those reported in previous studies, not only in animal models but also in humans.6,7 In addition to circulatory RAS, local RAS is also activated by HC; for instance, cholesterol-rich diets can increase ACE activity by two to five times in rabbit arteries and significantly up-regulate cardiac AT1 receptors in post-myocardial infarction rats. 3 However, Orfanos et al. found that pulmonary endothelial ACE activity was significantly lower in Watanabe heritable hyperlipidemic rabbits than in age- and sex-matched New Zealand White rabbits. 2 This difference indicates that the relationship between HC and RAS activity may vary among animal species and organs.
In addition, this study demonstrated that TC and LDL-C, but not TG and HDL-C, were associated with activation of circulating RAS in the HC group. Similar results have been shown in other experimental studies. 11 Some researchers have proposed that cholesterol-induced RAS activity could result from either native or oxidized LDL (Ox-LDL-C) up-regulating ACE in endothelial cells, thus increasing the conversion of Ang I to Ang II.12,13 In cultured macrophages, elevated cholesterol concentrations may promote the secretion of angiotensin peptides. 14 Meanwhile, other researchers suggested that cholesterol’s metabolites can activate various components that are needed for the synthesis of angiotensin peptides. 6 Furthermore, vascular endothelial cells activated by HC can subsequently secrete inflammatory cytokines to further activate the RAS.14,15 However, no evidence exists to suggest that cholesterol has a direct effect on any of the proteins in the angiotensin peptide biosynthesis pathway; the exact mechanism of these effects is unknown at present.
Furthermore, the present study demonstrates that the decrease in TC and LDL-C levels was associated with a decrease in RAS activity in HC patients within eight weeks of statin treatment. Many studies have shown that statins have pleiotropic effects on the cardiovascular systems, such as anti-inflammatory and antioxidant effects, and improving nitric oxide bioavailability.16,17 The effect of statins on the RAS activity is not fully understood, especially in humans. Meanwhile, there remains a controversy regarding statins’ effect on RAS activity. For example, one study showed that simvastatin can inhibit ACE activity in rats with aortic stenosis, 8 while another study in healthy individuals showed that atorvastatin treatment did not influence plasma Ang II or Ang-(1-7) levels. 9 Based on these studies, we suggest that the beneficial effect of statins on RAS could depend on baseline RAS activity. HC can activate RAS, and statins could have an RAS-inhibiting effect. On the other hand, when the baseline RAS is not over-activated in healthy persons, statins would not have such an effect.
Our study provides a reason for the association of cholesterol lowering with a reduction of the RAS activity, suggesting that it may be the decrease of blood LDL-C concentration induced by statins. Another potential reason is the antioxidant effect; statins can attenuate the development of reactive oxygen species (ROS) by down-regulating the expression of nicotinamide adenine dinucleotide phosphate (NADPH), and then decreasing Ox-LDL-C concentration. 18 Unfortunately, the interaction between cholesterol and RAS at the metabolic level is unclear. Further studies are needed to determine the changes in cellular cholesterol homeostasis on the RAS activity.
Clinical implications
This study demonstrates an important correlation between HC and activated RAS, and suggests a potential inhibiting effect of statins on the activated RAS. These results may provide an explanation for an apparent greater cardiovascular benefit from statins compared with treatments that only lower serum lipid-concentration. Our results also support the strategy of combination therapy with statins and RAS inhibitors in coronary artery disease.19–23
Limitations
Although our results showed a positive correlation between TC and LDL-C and RAS activity, more investigation is needed to demonstrate whether it is a cause and effect relationship and to interpret the underlying mechanism. Furthermore, larger sample-based investigations and randomized trials are needed to classify the relationship found in this study.
Another limitation of this study is the lack of measurements of plasma renin activity and 24-hour urinary sodium excretion rate. As a normal diet was restricted for all participants, especially for HC patients in the observation period, the daily variation in salt intake might not have an influence on the conclusion of this study.
Conclusion
Circulatory RAS is active in HC patients. TC and LDL-C, but not TG and HDL-C, are associated with the activated RAS. Using cholesterol-lowering statins is associated with a decrease in circulatory RAS activity.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by a grant from the National High Technology Research and Development Program of China (863 Program, No. 2012AA02A516).