
Abstract
Introduction:
Inhibitors of the renin–angiotensin aldosterone system (RAAS) are the basic drugs for treatment of diabetic nephropathy, as to some extent is spironolactone. The aim of the study was to evaluate the effect of spironolactone versus spironolactone plus hydrochlorothiazide in decreasing proteinuria in type 2 diabetic mellitus (T2DM) patients.
Methods:
In a double-blind clinical trial, 60 T2DM patients with nephropathy randomly assigned to three equal groups were enrolled. Spironolactone (50 mg/day) plus placebo, spironolactone (50 mg/day) plus hydrochlorothiazide (25 mg/day), and hydrochlorothiazide (25 mg/day) plus placebo were prescribed, respectively. The duration of treatment was three months for all patients. Urine protein was measured at the beginning and end of the study and analysis of data was performed.
Results:
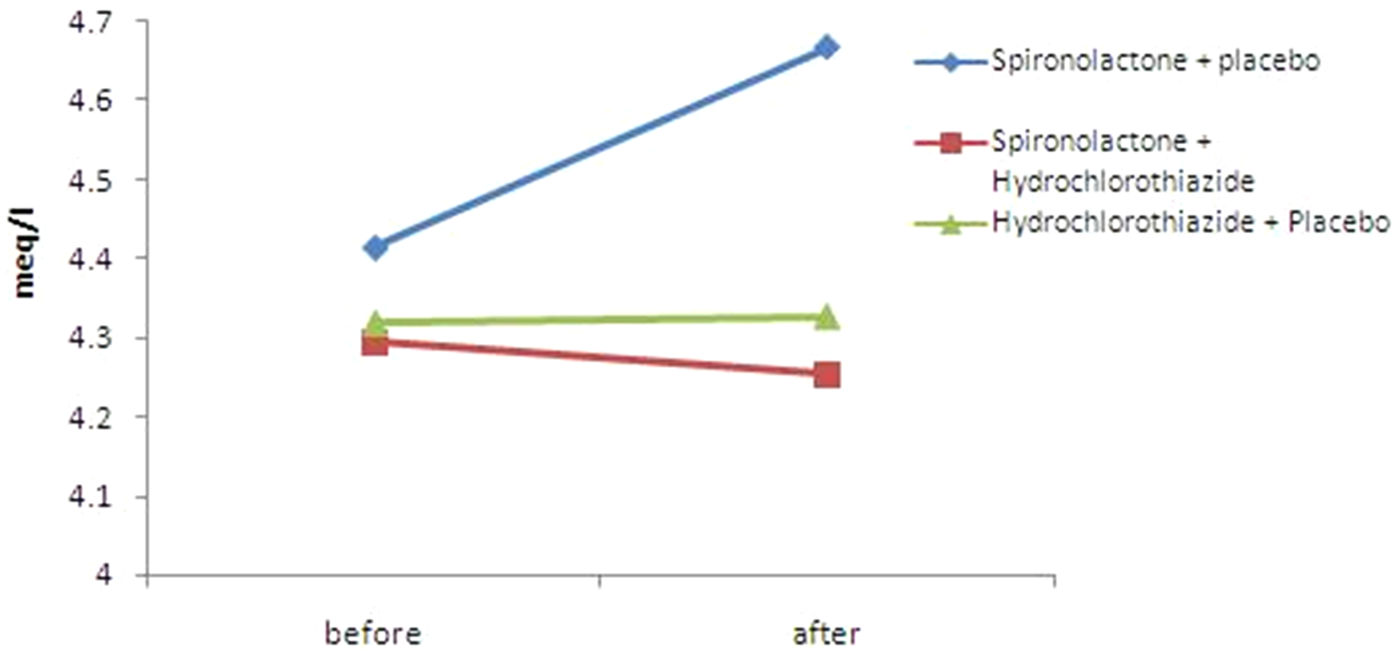
Twenty-six of the patients were male, with a total mean age of 56.8±8.3 years. Mean 24-h urine protein was reduced in patients in groups 1 and 2 compared to the third group (p < 0.001). Serum potassium in the first group showed a significant increase of 0.26 meq/lit with mean 4.64 ± 0.28 meq/lit (p=0.002), but it did not change in the second and third groups.
Conclusion:
Our results showed that spironolactone plus hydrochlorothiazide is an effective and inexpensive modality in the treatment of diabetic nephropathy without increasing serum potassium.
Introduction
Diabetic nephropathy (DN) is the most common cause of end-stage renal disease (ESRD) worldwide. 1 The stages of DN are glomerular hypertrophy, microalbuminuria, overt albuminuria, and finally a gradual decrease of glomerular filtration rate (GFR). DN occurs in 20% to 30% of diabetic patients, with the same frequency in diabetes type 1 and 2.2–4 Proteinuria is a known risk factor of the progression of renal and cardiac diseases, and decreasing the rate of proteinuria may also slow the rate of GFR decline.5–11 Angiotensin-converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs) are the main treatment for patients with diabetic nephropathy; however, some other therapies, such as allopurinol, have been used to prevent or reduce proteinuria in diabetic patients. 12 To prevent or treat DN, lowering blood pressure to less than 130/80 mmHg has been recommended, especially in patients with proteinuria of more than 1000 mg/day. Continuation of treatment with ACEi may lead to increased serum renin to the same level as before treatment by a mechanism called the escape phenomenon.13–18 Diuretics such as hydrochlorothiazide and furosemide can activate RAAS by decreasing the blood volume, thereby leading to decreasing the efficacy of RAAS blocking agents. Spironolactone (a potassium-sparing diuretic) is an inhibitor of spironolactone receptors in collecting tubules with a weak diuretic effect, therefore it has been combined with other diuretics to increase efficacy. It is primarily used for treatment of heart failure, secondary hyperaldosteronism (cirrhosis), and primary hyperaldosteronism (Conn’s syndrome). 19 In some studies, it is applied in diabetic patients to decrease albuminuria; however, due to its common side effect (hyperkalemia), its usage is limited.20–24 On the other hand, thiazide diuretics can cause hypokalemia and hyperglycemia and may also disturb control of diabetes. 25 Combining a thiazide diuretic and spironolactone for treatment of DN might be effective with a lower frequency of hyperkalemia. This combination was used in a few studies with different results; therefore, the aim of our study was to evaluate the efficacy of combining spironolactone and hydrochlorothiazide versus monotherapy with these drugs.
Materials and methods
In a randomized clinical trial in the Specialized Emam Ali clinic in Shahrekord, 60 type 2 diabetic (T2DM) patients in three groups were enrolled. Twenty patients randomly entered each group. Inclusion criteria were: age greater than 40, proteinuria ≥ 150 mg/day, GFR ≥ 30 mlit/min (Cockgroft-Gault (CG) formula), and K < 5 meq/lit. Exclusion criteria were: non-cooperation during the study, New York Heart Association (NYHA) class 3 and 4 heart failure, history of hypothyroidism, change of dose of ARBs or ACEi during the study, serum K ≥ 5.5 during the study, use of pentoxifylline, and any significant or acute complication of drugs.
In patients in the first group, spironolactone 50 mg/day plus placebo, in the second group spironolactone 50 mg/day plus hydrochlorothiazide (HCTZ) 25 mg/day, and in the third group HCTZ 25 mg/day plus placebo were prescribed for three months. Before and after the study, fasting blood sugar (FBS), two-hour post-prandial blood sugar (2HPPBS), 24-hour urine protein, serum K, blood urea nitrogen (BUN), and creatinine (Cr) were checked. These laboratory tests were conducted by Biotechnica Instruments (BT 3000) and Flame Photometer (Corning 480) Nyocard Reader II. The patients were taking insulin or oral hypoglycemic agents on an individual basis. All patients used renoprotective drugs (ACEi or ARB) and dosage of these drugs was not changed during the study. The patients were seen one week after the beginning of the study and then monthly for control of blood pressure (BP) and check of serum K (see Figure 1). Study data were collected with a questionnaire, entered using SPSS software and then evaluated by Chi square test, Kruskal–Wallis test, paired-samples t test, and Wilcoxon Signed Rank test. This study was approved by the ethics committee of Shahrekord University of Medical Sciences, Iran.
Serum K+ of patients during study.
Results
The mean age of the patients was 56.8±8.3 (41–81) years. Twenty-six (43.3%) of the patients were male. There was no difference between the three groups of patients based on age, gender, body mass indexes (BMI), systolic and diastolic BP, and duration of diabetes mellitus at the beginning of the study, but diastolic BP decreased significantly in the second and third group at the end of the study (Table 1). There was no significant difference between patients based on the dose of ACEi and ARBs. In the third group (hydrochlorothiazide + placebo), FBS increased significantly compared to the baseline. There was no significant difference between groups based on the 2HPPBS, 5 PM blood sugar (5PMBS), and hemoglobin A1C (Hb A1c) (Table 2). Lipid profile (total cholesterol, high- density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol, triglycerides) in the three groups was the same (p > 0.05). Serum Cr increased 0.1 mg/dl and GFR decreased 6 mlit/min in the second group (spironolactone + placebo) at the end of the study (p < 0.05). Serum uric acid in the three patient groups did not increase significantly. Corrected serum calcium increased 0.11 mg/dl in the third group (p < 0.05) and 0.06 mg/dl in the second group (p > 0.05). Serum phosphorus decreased significantly in the second and third groups, as did 24-hour urine protein (Table 3 and Figure 2). Serum potassium increased significantly in the first group but it did not change in the two other groups (Table 4). The highest level of K in patients was 5.1 meq/lit.
Demographic characteristics of patients before and after study.

DM: diabetes mellitus; BMI: body mass index; BP: blood pressure.
Glycemic characteristics of patients before and after study.
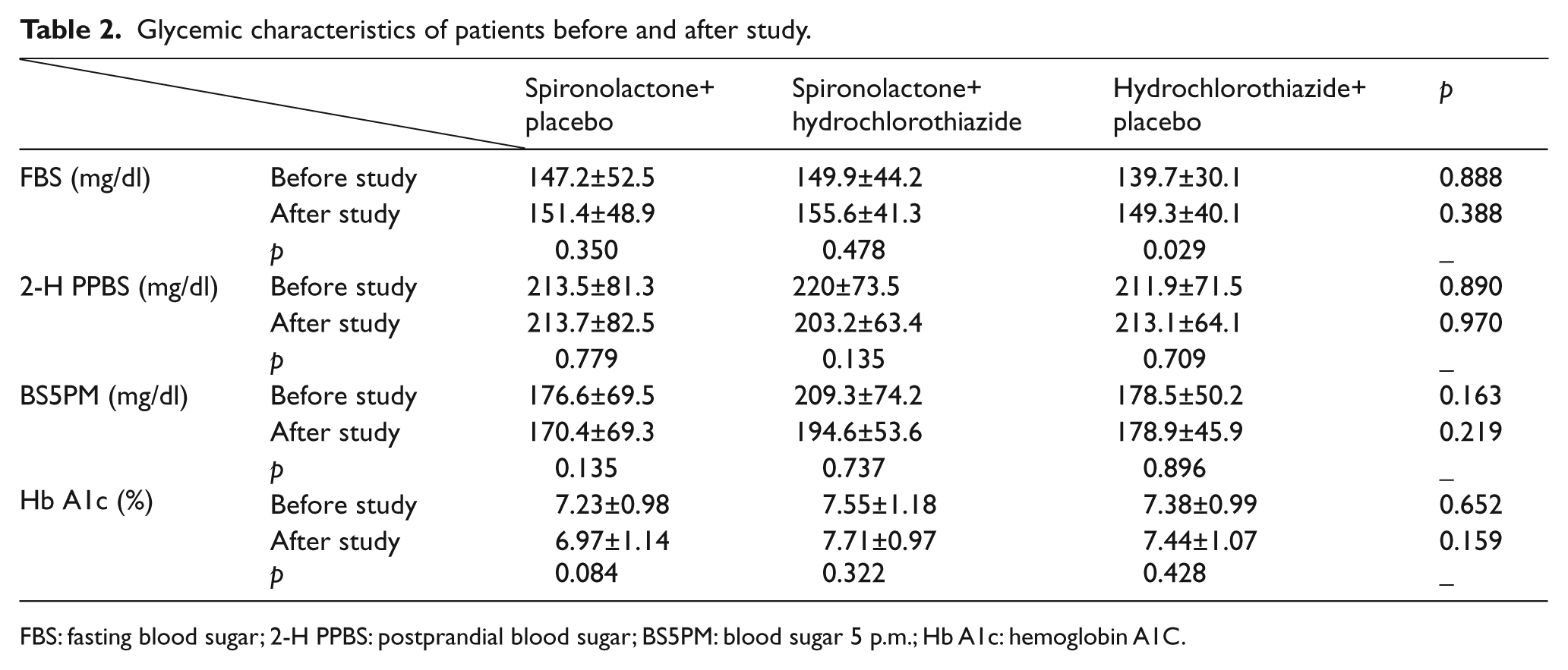
FBS: fasting blood sugar; 2-H PPBS: postprandial blood sugar; BS5PM: blood sugar 5 p.m.; Hb A1c: hemoglobin A1C.
Renal function test indices in patients before and after study.

BUN: blood urea nitrogen; GFR: glomerular filtration rate.

Twenty-four-hour protein of patients during study.
Serum electrolytes of patients before and after study.

Discussion
This study was performed on 60 T2DM patients, and the results showed that the combination of spironolactone and hydrochlorothiazide could decrease proteinuria without adverse effects such as hyperkalemia. GFR was decreased in the spironolactone group but not in the other two groups. In other studies similar results were reported; for example, Schjoedt et al. 23 and Saklayen et al. 26 showed that spironolactone could decrease GFR, and in a study by van den Meiracker et al., 24 spironolactone caused a transient decrease of GFR. Similarly, Bianchi et al. 21 showed that the reduction of GFR due to spironolactone is transient, and after one year of constant use GFR was higher than in the placebo group. Nevertheless, in studies by Chrysostomou et al. 27 and Mehdi et al., 28 spironolactone did not decrease GFR in patients. The cause of GFR loss by spironolactone is not fully understood, but may be due to the decline of serum level of aldosterone and its effect on the retention of salt and water in the kidney.
A not-significant increase in serum uric acid seen in the third group may be due to mild volume loss and increased reabsorption of uric acid in the proximal tubule. The increased serum Ca and decreased serum phosphate was due to the effect of hydrochlorothiazide on renal tubules that was significant only in the third group. Proteinuria was decreased significantly in the first and second groups, possibly because of the effect of spironolactone.
A few studies have been conducted about the antiproteinuric effect of spironolactone in diabetic patients; for example, in the study by Chrysostomou and Becker, 29 in which a prescription combination of ACEi, ARBs, and spironolactone versus ACEi and ARBs in combination reduced proteinuria in diabetic patients significantly. In another study on chronic kidney disease in patients with proteinuria who had been under treatment with renoprotective drugs (ARBs or ACEi), Bianchi et al. 21 added spironolactone 25 mg/day for eight weeks and concluded that in these patients proteinuria decreased approximately 1000 mg/day versus the control group, and after discontinuation of spironolactone proteinuria returned to basal level. In a similar study by Tylicki et al. 30 of 18 proteinuric patients, spironolactone reduced proteinuria approximately 700 mg/day compared with the control group. Also in a study by Navaneethan et al., 31 patients who were treated with spironolactone had less proteinuria compared with other patients. In addition, in Rossing et al.’s study, 22 spironolactone caused a 33% decline in proteinuria and 6 mm Hg in systolic BP compared to a placebo group, and similar results were also obtained in a study by Schjoedt et al. 23 Reduction of albumin to creatinine ratio in patients who received spironolactone was greater compared to patients with sisapril in a study by Rachmani et al. 32 Furthermore, aldosterone escape occurs in some patients under treatment with RAAS blocker drugs. In Sato et al.’s 20 study, aldosterone escape and its effect on proteinuria was evaluated; after prescription of ACEi for 40 weeks and in 18 patients, if there was any favorable response to treatment, spironolactone 25 mg/day was given and proteinuria decreased significantly. Mehdi et al. 28 in their study showed that spironolactone can reduce proteinuria in diabetic patients under treatment with ACEi. Saklayen et al. 26 and van den Meiracker and colleagues 24 also demonstrated that spironolactone was effective in reducing proteinuria. As in the patients on treatment with ACEi or ARBs, serum level of renin and plasma renin activity would increase; we could not check these characteristics in our study. In the patients who received these agents, the serum level of aldosterone decreased significantly because of a substantial decline in the amount or effect of angiotensin 2 on its receptors, so the effect of spironolactone on decreasing proteinuria might be due to other mechanisms such as an antifibrotic effect. 33 In our study serum K+ increased significantly in the first group but not in the two other groups; nevertheless, except hyperkalemia (K+=5.7 meq/lit) in one patient in the third group, maximum K+ in all patients was not increased more than 5.1 meq/lit. Serum K+ was not different in the spironolactone versus control groups in Saklayen et al.’s study; 26 however, in the study by Bianchi et al., 21 serum K+ was 0.8 meq/lit greater than in the placebo group. Also in a meta-analysis by Jennings et al., 34 a similar result was obtained.
Some thiazide diuretic side effects are hyperlipidemia, hyperuricemia, hypokalemia, and hyperglycemia. Glucose intolerance is probably due to the inhibitory effect of hypokalemia on insulin secretion and is less common with serum K+ greater than 4 meq/lit. 35 Thiazide-induced hypokalemia, hyperglycemia, and hyperuricemia are dose dependent, and daily doses of 12.5 to 25 mg hydrochlorothiazide produce fewer side effects than doses of ≥ 50 mg.35–37 We prescribed a low dose (25 mg/day) of HCTZ, and hypokalemia or hyperuricemia did not occur in the patients who received HCTZ plus spironolactone.
Conclusion
Spironolactone plus hydrochlorothiazide is an effective modality for treatment of DN especially in combination with ACEi or ARBs. Hyperkalemia as a common adverse effect of potassium-sparing diuretics was not seen with this combination; therefore, we suggest using these drugs for DN, especially in refractory cases.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by the deputy director of research at Shahrekord University of Medical Sciences, Shahrekord, Iran (Grant number 933).