
Abstract
Qualitative research methods play a central role in pain and health research, especially in enhancing understandings of lived experiences. This article focuses on the experiences of a researcher living with a chronic pain condition completing in-depth qualitative interviews exploring knee pain and osteoarthritis experiences, treatment and management. Using a collaborative autoethnographic approach, the article considers how the lived experience of the researcher (i.e. I), as a person living with pain and (dis)ability, impacted the research process. To do so, the research team (i.e. we) critically reflect on three important moments in interviews with participants and introduce the notion of hyperembodiment to explore responses that the research process elicited for the researcher. We advocate for hyperembodied reflexive approaches in qualitative research and outline the importance of researcher-centred ethics-of-care frameworks more broadly in health research, and especially in studies involving people with lived experiences of health conditions as researchers.
Introduction
This article contributes to research on pain, and qualitative research more broadly, using a collaborative autoethnographic approach to explore the embodied experience of researching and producing knowledge about pain. We focus on the experiences of a researcher living with a chronic pain condition completing in-depth qualitative interviews exploring knee pain and osteoarthritis experiences and management. Using a reflexive autoethnographic approach, we consider how the researcher's lived experience of pain and (dis)ability, impacted the research process. We focus on three moments in interviews with different participants. For the researcher, these moments involved the elicitation of what we refer to as hyperembodiment, a term we adopt to characterise the experience during interviews of significant visceral, affective evocation of the body and bodily vulnerability. While research has long identified embodied aspects of research processes (Todres, 2008), we use the prefix ‘hyper’ (commonly defined as ‘above’, ‘beyond’ and ‘excess’) (Merriam-Webster, 2025) to make intelligible both the powerful presence and dynamic intrusion of the body and affect into the interview space as part of the research process.
Using hyperembodiment as a conceptual frame, we foreground the important generative role that pain can play in qualitative health research: while the experience of pain places undeniable constraints on a researcher, it can also provide a capacity to be moved by and respond to, phenomena that would be unnoticed (or underplayed) by other researchers. This capacity could enable the generation of data, and consequently knowledge, that may otherwise be overlooked or ignored. We thus advocate for hyperembodied reflexive approaches in qualitative research and outline the importance of researcher-centred care in ethics-of-care frameworks more broadly in health research, and especially in studies involving researchers with lived experiences of health conditions.
Globally, approximately 30% of people are affected by chronic pain (Cohen et al., 2021) and in Australia, chronic pain affects one in five people over 45 years of age, with women more likely to be affected (AIHW, 2020). Social science research has characterised pain in a range of ways, including as a challenging phenomenon to understand (Bullington et al., 2003); a subjective, consuming sensation (Morse, 2015); being omnipresent and fluctuating (Bunzli et al., 2013); and confusing, even for those living with it (Robinson-Papp et al., 2015). Such work also suggests measuring chronic pain ‘intensity’ often fails to capture all dimensions of the lived-experience (Hjermstad et al., 2011; Robinson-Papp et al., 2015). Qualitative research enables exploration of the affective, social and cultural dynamics and impacts of pain, and can provide critical insights into lived experiences. For example, such work has described self-management strategies of people in pain (e.g. Anderson et al., 2021); and drawn attention to the corporeal, temporal, spatial and relational dimensions of lives lived with pain (Stensland and Sanders, 2018). Social impacts have also been well-documented, with pain producing and amplifying feelings of fear, stigmatisation, anxiety and distress, and affecting people's decision-making abilities and social relations (Attridge et al., 2019; Bunzli et al., 2013).
Social science research demonstrates pain experiences are gendered. Women in pain report feeling ignored, and/or their experiences minimised by family, friends and healthcare professionals. The gendered and invisible nature of chronic pain conditions such as fibromyalgia and endometriosis mean women often experience distrust and disbelief, in spite of the profound impact of living with these conditions day in, day out (Juuso et al., 2014; Lightbourne et al., 2024). Implicit gender bias among healthcare providers results in the systematic undertreating of women with chronic pain (Samulowitz et al., 2018). Intersections of gender and race effect how different health topics are treated, with greater stigmatisation of non-white bodies (e.g. Black women) which in turn impacts access to treatment and quality of healthcare (Pryma, 2017). Further, healthcare providers often have limited knowledge around the individual needs of people in chronic pain, with many women in pain who seek help in health and medical services feeling discouraged, diminished or abandoned (Arman et al., 2020; Olsson et al., 2011; Skuladottir and Halldorsdottir, 2011). Women may also endure and hide their pain, due to gendered ideas normalising it as a ‘natural’ feminine experience (Grundström et al., 2018). The normalisation of pain means many women are likely to live with undiagnosed pain conditions or to have diagnosis delayed (Grundström et al., 2018; Seear, 2009). Comparatively, traditional gender roles and masculine norms can shape men's experiences of chronic pain. Men may struggle to express their feelings, are less likely to seek treatment and may be frustrated by feelings of inadequacy, especially if their pain impacts their ability to adequately fulfil traditional ‘masculine duties’ (Montesó-Curto et al., 2024).
Below we introduce our conceptual frame by outlining the role of embodiment and reflexivity in feminist ethics-of-care research approaches, and what we mean by moments of ‘hyperembodiment’. We then introduce the unique location of the field researcher and autoethnographer Nadia Bevan (NB), before presenting our results and discussion. In the sections below we refer to the field researcher adopting the autoethnographic approach as NB. Where first-person pronouns are used (i.e. ‘I’) this also refers to NB, and where collective pronouns are used (i.e. ‘we’), this refers to the collaborative authorship team. The latter is part of most research projects (where the authors reflect on their own positionality within a project), whereas the former – as we see it – acts more as a methodological device, that is, an approach to research and writing seeking to describe and analyse personal experiences in ‘empirical’ terms.
Reflexive embodiment
Researcher values and location are recognised as central to qualitative research. Qualitative approaches tend to embrace the subjective role and influence of the researcher on the research process, from inception, including the focus, study design and development of research aims and questions, to data collection, analysis and interpretation. Reflexivity is a critical tool that enhances research processes through engaging with and incorporating the lived experience of the researcher. For example, reflexivity allows researchers to understand and address how personal biases, experiences and interpretations play a role in constructing knowledge. It allows researchers to position themselves as subjects with particular identities, experiences and emotions and consider how they relate to the phenomena under examination with research participants (Ciotti, 2023). Such epistemic approaches to knowledge production often adopt participatory research methods, and recognise knowledge is produced and collaboratively co-constructed by researchers and participants.
Over time, feminist researchers have advanced conceptual tools to help engage reflexively, re-framing how positionality, subjectivities and personal circumstances affect knowledge production (Billo and Hiemstra, 2013). A key intervention is the development of a feminist-ethics-of-care approach, that focuses on the intersection between professional and personal lives and how this affects interactions with participants. Core to a feminist-ethics-of-care is relationality: centralising and valuing human life, and caring for research participants as a political and intellectual project. In these approaches, dualism of ‘us’ (researchers) and ‘them’ (participants) is reframed, and value is attributed to a multi-directional, reciprocity of care in relations between people (Held, 2006; O’Riordan et al., 2023). Embodied experiences inflect research processes and approaches and can be understood as central to a feminist-ethics-of-care approach. Attentiveness to this aspect of the relationality of bodies in the research process necessarily involves reflexive embodiment. That is, practising reflexivity that centres the researcher's body in the process, enables ongoing attentiveness to how their own embodied experiences are intertwined with their positionality. In this vein, we recognise and attend to the positionality of NB as a (dis)abled researcher living with an invisible pain condition researching other people's pain. To be clear, autoethnography was the methodology used to describe and analyse NBs personal experiences; reflexivity is a part of ethnographic methodologies and qualitative research more broadly, and allows researchers to understand our positionality and how it affects knowledge production in research processes (Greschke, 2024).
For the purposes of our reflexive, feminist ethics-of-care approach, NB adopted an autoethnographic methodology to capture and reflect on the embodied reflexive practices throughout the study. This is important, as it enables consideration of how pain can provide a way to experience embodied resonance; a means by which to connect or bond the researcher with a participant (Gendlin, 1962). Similarly, a double hermeneutic approach captures how pain is experienced and contextualised by NB while interpreting how other people view and express their pain experiences in society. As research has shown when participants share their experiences of pain, an empathetic experience may be evoked by the researcher, where bodily sensations and negative emotions can be embodied (Martínez-Pernía et al., 2023). Further, such embodied resonance may be particularly powerful for people who have their own pain experiences, whereby bringing an embodied self can enable a deeper sense of understanding of phenomenon and people (Todres, 2008). Here, we illustrate NBs personal experience of chronic pain was profoundly foregrounded during moments of the research process, altering the researcher-participant dynamic and data generation. We present three such moments, which, we argue, involved the elicitation of hyperembodiment. To the authors’ knowledge, the term hyperembodiment has previously been used in only one study relating to body awareness and alexithymia in people with fibromyalgia (Calsius et al., 2015). Calsius et al. (2015) used the term in daily experiences of people with fibromyalgia, where sudden stimulation can create a sense of being consumed by heaviness in their body. Other concepts used in qualitative pain research, such as (heightened) somatic (or body) awareness, interoception and hypervigilance, show an inward gaze, noticing bodily sensations and internal cues (e.g. McDermid et al., 1996; Schrepf et al., 2016). While our use of ‘hyperembodiment’ carries with it understandings of bodily awareness usefully captured in other concepts, such as (heightened) somatic awareness, and (heightened) interoception, we seek to extend these terms by moving beyond an individuated sense of body awareness. Instead, in locating hyperembodiment as a reflexive tool in qualitative research, we centre the body and body theirstories 1 in dynamic, relational, affective and corporeal processes of knowledge production (see Figure 1). Furthermore, we account for dynamic affective experiences of bodily vulnerability that may be persistent, acute or fleeting in the process of research, but that are always experienced in relation to the research process itself and are central to what and how knowledge is produced. In particular, we identify what are, for many researchers with lived experiences, inevitable yet unanticipated moments of heightened bodily vulnerability, and offer guidance on how to best support the researcher and participants in these contexts.
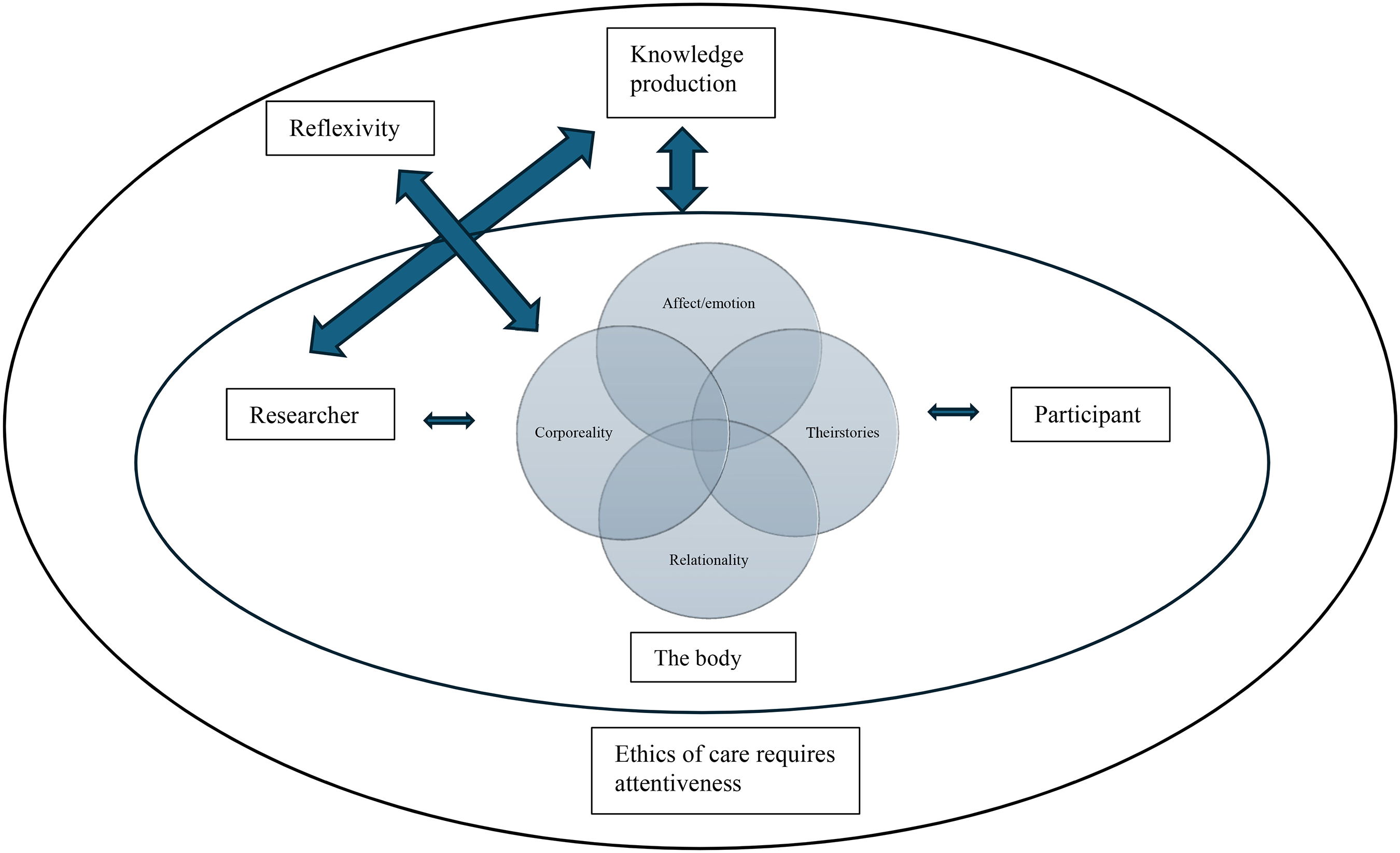
Hyperembodiment conceptual framework.
Being attuned to hyperembodiment, and associated discomforting dimensions is, we argue, important for practising an ‘ethics-of-care’ approach. This aligns with Guillemin and Gillam's call to engage reflexively with ‘ethically important moments’ in research: ‘the difficult, often subtle, and usually unpredictable situations that arise in the practice of doing research’ (2004: 262), and for which procedural ethics can never fully account. Although procedural ethics addresses physical, emotional or social harm that may arise for participants, researchers themselves must possess a certain level of skill to navigate uncomfortable or unexpected topics, tensions and emotions during the research. Pillow (2003) refers to these discomforts and complexities as ‘messy’ in qualitative research (Supski and Maher, 2023). Emotional care through the messiness of qualitative research is integral to reflexive research for both participants and researchers alike (Malacrida, 2007). Empathy can be integral to an ethical process (Coplan and Goldie, 2011), and hyperembodiment, we argue, provides a lens through which to explore the visceral dimension and empathy.
The researcher: Working with (dis)ability and pain
Since my early adolescence I have lived with fibromyalgia, a complex condition of unknown aetiology, usually characterised by symptoms such as musculoskeletal pain and fatigue. My pain experience has included debilitating flare ups where I am unable to do much more than simply exist on a couch or in bed for days or weeks at a time. Daily, I wake up unrefreshed, with discomfort or pain, and with a heavy emotional and mental load– this is due to the need to do everything I can to minimise flare ups, which requires significant daily thought-processes and emotional labour. Chronic knee pain has been part of my pain experience, with my adolescence riddled with acute sharp pains in my knees, restricting my movements. For example, I would avoid stairs, since every step would induce crippling pain. One of the many health professionals I sought help from said I likely had some mild knee arthritis and another opined it was patella-femoral syndrome. Since adolescence, my symptomatology has minimised, as my knowledge of my body and what supports it best has increased management of my symptoms. Yet, pain and fatigue consistently permeate my consciousness. I experience fluctuations in muscular and cognitive fatigue, and knee pain is one of my first signs of a fibromyalgia flare-up.
Many people in my life do not know I have a (dis)ability. Like many chronic conditions, fibromyalgia is invisible. Although I often hide my authentic self through masking, I can also choose when to disclose my ill identity. My work is also part of my identity. Albeit at times painful and challenging, work provides an opportunity to maintain a level of control and confidence in what I can achieve. A feminist-ethics-of-care approach acknowledges the link between my professional (researcher) and personal (person with a (dis)ability) lives. My work and (dis)ability identities intersect, and therefore the weight of my fibromyalgia is in every interaction, thought and feeling in my research. Similarly, my identity as a researcher does not stop once an interview is complete; rather, it imbues every day, being intertwined with who I am. The exposure of my (dis)ability identity is a constant tension within and beyond my research. ‘Coming out’ with a (dis)ability in an ableist society and in academia – which values cognitive ability and clarity – entails navigating challenging terrain. I must ensure as a researcher and a person with a (dis)ability I protect myself, especially from the emotional toll of qualitative interviewing. Although I consider it a privilege to hear participants’ experiences, it can also be heavy and exhausting when speaking of pain; a common human experience, but which infiltrates my daily existence.
As a qualitative researcher, I interview people about their lived experiences, interactions and perceptions of certain phenomena. In this study, the participants with whom I spoke variously reflected on their own experiences and views on pain, (dis)ability and self-management strategies. After a few interviews it became apparent this involved discussions of living with pain and associated (dis)ability that were challenging for me. For this reason, and after deliberation and discussion with the other research team members, I adopted the explicitly reflexive, feminist ethics-of-care approach we advocate here, as a means to explore my responses and their impact, and to care for myself and the participants. This involved ongoing reflexive engagement that centred my own body as a health researcher and its herstories (a feminist viewpoint) of pain in the research process.
Methodology
Knee joint pain and knee osteoarthritis are common chronic musculoskeletal conditions, contributing to a global burden of disease (AIHW, 2023). The findings and reflections reported here are from semi-structured interviews completed as part of research exploring experiences and perceptions related to knee joint pain and osteoarthritis, including management options. At the time of writing, three cohorts had been recruited for interviews: ‘physically active’ people with no knee pain or injury (n = 15); people who had experienced some type of undiagnosed chronic knee pain or diagnosed knee condition/injury, such as patella tracking issues, meniscus strains and torn anterior cruciate ligaments (n = 19); and; people living with osteoarthritis (n = 4). In the first two cohorts, all participants were 18 to 40 years old: those in the osteoarthritis cohort being between 24 and 76. The interviews addressed motivations for physical activity and experiences, perceptions and understandings of knee health, pain and/or osteoarthritis, and, where relevant, views on and experiences of management of knee injury, pain and/or osteoarthritis.
We took a collaborative autoethnographic approach, allowing for multiple authors to enrich and contextualise the pain phenomenon, enabling a critical analytical lens beyond NBs perspective (Chang et al., 2016). The research team's cross-disciplinary expertise (e.g. physiotherapists, health sociologists and psychiatry) provided rich sociocultural analysis in the collective context of people's lived experiences of pain. Compatible with the autoethnographic paradigm, NB paid special attention to, and recorded experiences of embodied responses to the participants during interview conversations, explaining: While undertaking interviews, I felt bodily phenomena and emotional valence change. I became aware of my bodily sensations and attuned to small adjustments, such as my blood feeling cold, chest constrictions or heat in my face. When these, and/or emotional responses were evoked, I was closely attentive to them. I gave myself time to ‘sit with’ the response, and to ‘trace’ their changing visceral and affective dimensions. This was particularly powerful in a state of fibromyalgia flare-up, where my senses and pain were already heightened and any small changes felt potent. I then described the sensations, emotions and herstorical relevance via a process of note-taking immediately after the interview, and often after further reflection and processing in my own time, for example, through walking or breathing exercises to acknowledge, recognise and reflect on my embodied experience and what may have shaped it.
Guided by Chang's (2016) standards for autoethnography (see below) (Anderson, 2006), this approach had advantages. It enabled exploration of how the researcher's lived experiences of pain connected NB with ‘others of similarity’, ‘others of difference’ and ‘others of opposition’ (Chang, 2008: 26). It helped situate NBs embodied experience as a (dis)abled researcher within a wider cultural, theirstorical and social context, especially with respect to meanings, experiences and understandings of individual responsibility for health, management of pain and beliefs and (stigmatised and/or stigmatising) views on (dis)ability (Adams et al., 2014; Ellis and Bochner, 2000). The alignment with Chang's (2016) five standards for autoethnography is as follows:
Authentic and trustworthy data: Does the autoethnography use authentic and trustworthy data?
Personal memory is not necessarily trustworthy; however, to maintain as much authenticity and trustworthiness as possible, I wrote reflective notes immediately after I completed interviews to capture my thoughts, feelings, emotions and embodied experience (Braun and Clarke, 2021). I sought to capture visceral reactions, memories, emotions or thoughts, especially those that reflect sociocultural biases. When I went back and read my reflections, I questioned my interpretations. For example, does this feel like an accurate representation of my embodied experience and what I believe I can recall from different periods within my life, as well as my current state of being?
Later, these reflections were shared with the research team. Although they cannot provide triangulation of the data per se, the collaborative team can ask questions of my lived experience and the surrounding sociocultural phenomenon, due to their extensive experience as cross-disciplinary qualitative researchers. Therefore, they contributed their collective experience with research methodologies, including interviewing people with chronic and acute pain, reflections and the evidence around pain, (dis)ability and ableism.
Accountable research process: Does the autoethnography follow a reliable research process and show the process clearly?
Once interviews were completed, my first step was to email participants with resources to help support some of the discussion points (e.g. with information about osteoarthritis). This was followed immediately by writing reflective notes. The data familiarisation process continued when interviews were uploaded to an online transcription service (sonix.ai). I then ‘cleaned’ them, providing another layer of analysis before coding commenced (Braun and Clarke, 2021). During the cleaning and coding process, I noticed certain passages and concepts remained with me. I reflected on the interviews with the research team at different points. I used collaborative de-briefing sessions to reflect on the language I adopted to explain my (embodied) experiences, including any discomfort I experienced in interviews, re-reading transcripts, and when interpretating the data I had collected.
Ethics toward others and self: Does the autoethnography follow ethical steps to protect the rights of self and others presented and implicated in the autoethnography?
The research was undertaken with ethics approval, and adopted all necessary protections to ensure, procedurally, the protections and rights of participants. Pseudonyms are used here for anonymity. Due to the nature of autoethnographic research, even though pseudonyms have been used, some people may be identifiable (Benoot and Bilsen, 2016). Therefore, these people (e.g. NBs psychologist) have been consulted and consented to being acknowledged in this study.
Procedural ethics alone do not necessarily address all ethical concerns and conduct. Our ethics-of-care approach recognises this: it emphasises the important role of reflexivity in identifying and attending to the relationship between the participants, the research team, the research itself and the products of the research (Blakely, 2007). This included reflexive practices, namely, reflective note taking and observations of my thoughts, emotions, biases, practices and processes. I met with the research team regularly to collaboratively discuss the emerging findings. I aimed to make it clear to participants that we valued their time and input. I thanked them for sharing their experiences and emotions with us. Many participants likewise thanked me after the interview, stating that it provides a platform for them to share their experience, reflect on things they may not have previously considered, and for completing a study, as they believe it to be important.
The Australian National Statement on Ethical Conduct in Human Research focuses solely on participants; there are no structured support mechanisms for researchers to support their emotional labour (Seear and McLean, 2008). Researchers are, in effect, responsible for taking care of their own (and their teams) emotional wellbeing (Malacrida, 2007). When it initially became apparent that I found discussions of pain and (dis)ability during interviews to be challenging, I did ponder whether I was comfortable with an autoethnographic approach: internally, I grappled with the idea of disclosing my invisible (dis)ability (of which some of my friends and family members are unaware). Was this something I really wanted to do, catapulting something I had masked for so long into an openly public and critical sphere? I was worried about the emotional toll of reflecting on my embodied experience as a (dis)abled person in an ableist society. I spoke with members of the research team about the value of an autoethnographic approach. I also spoke with my psychologist, who challenged my initial reservations and hesitations. After some consideration, I first contacted a colleague who was supportive and encouraging, and who provided me with space to come to terms with my (dis)ability ‘coming out’ (Finlay, 2002). She continually reminded me that at any time I could stop, if that was needed.
Sociocultural analysis and interpretation: Does the autoethnography analyze and interpret the sociocultural meaning of the author's personal experiences?
Living with an invisible (dis)ability in an ableist society means many of my experiences have been shaped by notions of being perceived as being young, fit and healthy – a sociocultural norm in which these notions are synonymous. Yet, some participants also spoke of times when they had visible differences (i.e. on crutches) and felt othered. Sociocultural norms suggest as you age, experiences such as pain are to be expected, as your body will not function as well. In this study we speak of osteoarthritis and many participants believed this – and the type of associated pain and (dis)ability – to be something associated only with older people. These notions are perpetuated through an ableist society, focussed heavily on youth and appearance where (dis)ability is portrayed as ‘othered’, and age/ageing is aligned with increasing decrepitude (Carney and Gray, 2015; Moser, 2000). These norms were reflected in the interviews, and they felt potent to me because I was prompted to reflect on my own pain and associated invisible (dis)ability. I could see how self-stigma, and my own masking of my (dis)ability, was influenced by prevailing norms.
Scholarly contribution: Does the autoethnography attempt to make a scholarly contribution with its conclusion and engagement of the existing literature?
This collaborative autoethnography aims at making a scholarly contribution in two ways. First, it adds to the literature around the embodied experience of a (dis)abled qualitative health researcher. Second, the notion of hyperembodiment is introduced, with a call to action for researchers to engage in reflexive processes in pain and health research. This call is arguably important given the current emphasis on consumer involvement in research, which includes empowering consumers to lead and do research. My research team and I suggest the concept of hyperembodiment that emerged through this collaborative autoethnographic work, may be a useful conceptual tool to support consumer-led research, and health research more broadly. It offers insights into the powerful role of the body in research processes, and helps to identify and address the valuable and potentially negative and challenging (embodied) impacts of doing research for people living with health conditions.
Findings
Three ethically-important moments in the research process
The findings we present draw on three interviews that can be understood as ‘ethically important-moments’ (Guillemin and Gillam, 2004) due to the strong visceral reactions they evoked in the interviewer. An acute awareness of bodily sensations, emotions, herstories, thoughts and actions were powerfully shaped by the complexity of NBs lived experiences of pain and (dis)ability. While experiences of hyperembodiment in the research process were not isolated to these examples, they were selected to explore their meanings and implications as they had the most affective force for NB.
Jessica
Jessica was a white woman in her mid-30s who was recruited for the physically active cohort. For people who have not experienced any knee injury or pain, we pose a vignette proposing hypothetical knee pain, and their possible actions, feelings and thoughts. When speaking through the vignette, Jessica said: ‘I guess I'm nervous, like, I think the worst thing in the world for me would be … to be, like if I were, like, handicapped or disabled in any way, um, like, that terrifies me’. In hearing this, I felt confronted with a visceral response, pulling away from the screen, and thus Jessica. I allowed myself a moment to recompose, with some (hidden) deep breaths and focus on the interview guide, reminding myself she has a very different lived experience. She perceives pain or (dis)ability to be the worst thing in the world. Comparatively, I, as a person who lives with chronic pain/(dis)ability, navigate this in my daily life. At a later point she once again said, ‘I guess the prospect of, you know, someday not being able to play tennis or not being able to walk around or control my own, or like have complete control to do as I please I guess, um, terrifies me’. In reflecting on these excerpts, I can see the fear she has around this perceived loss and how she values, and potentially takes for granted, being able-bodied. Why then, I wonder, does this individual fear pain or loss of movement so very much? Possibly because it poses a threat, and perceives she would not be able to do the physical activities she enjoys and values with pain experiences.
During this interview, I was in a fibromyalgia flare-up, where sitting at the computer was exhausting and painful. This likely contributed to my feeling affronted and misunderstood. I had a desire to share my experience that physical activity can support and manage pain and (dis)ability. While I stayed on track, following the interview guide, several times Jessica's fear of loss of movement due to pain or (dis)ability re-surfaced. I sat with my visceral discomfort – a sense of heaviness coursing through my body. Later in the interview she reiterated that losing her ability to move pain-free is a scary notion: ‘As I mentioned earlier, if I were, you know, the worst thing for me, I think, is to kind of lose my ability to move. Um, so that would scare me’. I imagine being scared and terrified of loss of movement and physical pain is likely common in those who have not been afflicted by this very human phenomenon. At the end of this interview, I undertook my reflexive processes, note-taking and breathing, however, I did not debrief with my team. For several days after Jessica's interview and continuing to be in a state of fibromyalgia flare-up, I sat with my discomfort and percolated on notions of (dis)ability and acceptance of pain, both my own and others. Ultimately, I resolved that pain is part of life. Curiously, we both have fears around pain and (dis)ability, albeit different.
Sarah
Sarah, a white woman in her late adolescence was recruited for her lived experiences with knee pain and injury. This was an extremely emotional online interview. Within ten minutes, when asked about her knee pain experience, she instantaneously welled up and tears flowed. Her voice wavered and she said ‘sorry, like, I get really emotional about, talk about [sic]’. Throughout the interview, Sarah was crying on and off when discussing her traumatic knee injury, what it meant to her aspirations for elite-level sport, and fear around re-injury, which she felt was inevitable, and did eventuate. My natural tendency was to cry with her and comfort her. Yet showing my tears felt like contraindicating my professional manner and so I withheld my emotions throughout the interview while desiring to create a safe space for her, as she appeared to be transported back to her pain.
While I sat in discomfort and desire to be empathetic to Sarah, I continued to gather information. My natural tendency was to speak to her experiences and emotions alone. With an awareness she had to get to work after the interview, and feeling time pressured; I felt torn and compelled to complete the interview guide. This created discomfort and messiness between emotional turmoil – both for Sarah and myself – and the task. My priority was Sarah. I was trying to be empathetic and acknowledge her emotions by allowing her the opportunity to disclose as much as she wanted, and reinforcing it was okay to cry. I attempted to support her through the language I used, where I encouraged her to speak about her experience, but only if she was comfortable. For example, when asking about the impact of her injuries on her life, I softened my questions to allow her the opportunity to feel comfortable in not answering what I perceived may be an emotional question: ‘I guess can you just talk, if you're happy to, if you're okay to, a little bit about that and the feelings around that and that impact of your injuries on your life?’ I thought about asking her if she would like to stop the interview, but I felt that may invalidate her emotions, which I had no desire to do.
Sarah had dreams of being an elite-level athlete, dreams she acknowledged would never be fulfilled. In her young life, she has suffered severe trauma to her knees and it has clearly affected her – physically, emotionally, socially and in re-shifting her priorities – where now she was focussed on achieving daily physical activities: ‘Just being able to like, live day to day and not be in pain and just like do, things like hikes, and go on holidays and participate in activities that everyone does without being restricted’. I felt proud of Sarah for acknowledging and attempting to accept her new reality, yet my heart ached for her. I was not in a state of fibromyalgia flare up in this interview, yet I embodied a sense of gravity and grief and deeply empathised with her pain experiences and desire to do ‘normal’ daily activities. Despite personally going through a very different journey, the interview brought me back to my adolescence, living in pain and dealing with my body's limitations. I could see how hard it was for her to accept the lived experience of pain, while also changing her future direction and sporting identity. Accepting pain and/or (dis)ability as part of one's life and identity can take time, especially when you are not able to do activities you want to and compare yourself to peers when you are unable to engage in similar activities. This is especially pertinent when people think you can, and define you as ‘young and healthy’, insinuating they think you are able-bodied. These (mis)perceptions can evoke feelings of shame, such as the following excerpt, where Sarah details her embarrassment when she re-injured her knee: ‘So I felt embarrassed that people would think, I'm just making a big deal, “oh, she's on crutches again,” like I had people say that to me, oh, you're on crutches again, like, why are you on them again? Like I was like, it's not my fault, I didn't choose it [sic]’. This interview finished somewhat abruptly since Sarah had to go to work. Immediately after I took reflexive notes and inwardly gazed. I acknowledged my emotions, such as grief and sadness, yet also hope for Sarah's future and performed deep breathing exercises to calm myself.
Steve
Steve was a white man in his early 30s who was part of the knee pain and injury cohort. Steve was very physically active, with a curiosity to investigate new and potentially ‘not the norm’ solutions to health. He seemed invested and focussed on his health, including being a student in a health-related industry, listening to podcasts, and exploring research on treatments. This was illustrated by the comment: ‘like I said, like anything that's going to improve my health for the better, … I'm the type of person that if you gave me the option to live forever, I'd probably take it’. Steve associated certain things such as running fast, with a youthful identity. ‘Um, for me, also like running fast specifically is, I see it as a very youthful thing. Like for me, the day that I can't run or sprint anymore would be a very depressing, sad day. So, like I will do anything to be able to keep running [sic]’. I saw this as an interesting notion – youthful identity intwined with the ability to run fast. I also felt torn as it was contradictory to my younger, sicker years. The concept around youthful identity and ‘fit and healthy’ is something that is often presented and reiterated in society – something I have personally felt offended by. There is a sense that ‘young’ people must not know what physical pain or (dis)ability are, as has been expressed in the sentiment ‘you’re young and healthy’ constantly through my lifetime. I may have been chronologically young, but through most of my life my body has felt ‘othered’; exhausted, fatigued, sore, unable to perform many tasks society tells me I should be able to do. This may have been exacerbated due to feeling fatigue and pain at this point of time, and thus, I had a heightened sensitivity towards such comments about youth and health. Yet, something about Steve's curiosity for health resonated positively with me.
Approximately ten minutes into this interview, I recognised I felt a sense of commonality with Steve, which enabled a more ‘natural’ dialogue between us. We both had a desire and curiosity to optimise our health. When speaking to his experience of his meniscus tear, which was quite debilitating, he saw it as an opportunity to try health-practices he otherwise may not have had a chance to. For example, he said: ‘I think the, the curiosity of trying to fix it. Like I like the challenge of trying to fix it myself. Like as much as I hated the situation, I enjoyed a new avenue of being like, hmm now I can kind of play around a bit here and see what I can do with it, like, like ozone reading about these things and finally getting a chance to actually try and put it to practice and see if it works. That was actually quite interesting to me’. I strongly identified with this statement as it echoed and shared striking commonalities with my own experiences. At several points, I have sought to improve my health by adopting unconventional or purportedly ‘pioneering’ methods (e.g. medicines, diets) but, at times, with severe consequences that were detrimental to my health. Hence, when Steve described adopting this arguably experimental self-driven management of his condition, it evoked strong feelings of fear and hesitancy that surprised me. At this moment, I felt envious that Steve had the ability to try new things with fewer repercussions, but concerned for his health too – I did not want him to suffer any ill consequences for trying to improve his health like I had. Navigating this affective response felt easier with Steve than some other participants, based on a shared curiosity for health and jovial repertoire. There was an ability to speak about serious topics such as how Steve's meniscus tear affected him, and concerns over future injuries, yet ease and flow in the dialogue. It appeared Steve also felt this way, as he spoke in what seemed to be a comfortable manner within the range of topics discussed, at times he swore and at different periods laughter ensued. Thus, despite a visceral reaction to moments in Steve's injury journey, and especially those that resonated strongly with my experiences, these feelings appeared to have a less confronting impact on me and I was able to conduct the interview in a relaxed, free-flowing way, compared to others. Notably, they prompted considerable reflection, especially in the process of cleaning, coding and interpreting the meanings of the data and my responses to it.
Discussion
Underpinned by Chang's standards for autoethnography (2016), three ethically important moments captured how NBs hyperembodied experience affected her and the generation of knowledge on pain. Jessica's fear of pain, (dis)ability and loss of movement evoked a visceral retraction; Sarah's free-flowing emotion created a caring, carefully guided shift in questioning; while Steve's sense of identity, youth and curiosity in health allowed for a natural flow in dialogue, calming the interviewer's immediate discomfort in her traumatic memories from past health experiments gone wrong. These examples show the messiness and discomfort researchers can experience during qualitative research (Supski and Maher, 2023). They also offer insight into the role of the body, and especially the importance of being reflexively attentive to heightened responses in the body, during the research process. We suggest these experiential embodied moments in the research process can be usefully understood as forms of hyperembodiment that play an important role in generating knowledge, especially in health research on pain and (dis)ability.
Hyperembodiment – that is, the researcher's herstory, corporeal, affective and relational reality of (dis)ability and lived experience – critically shaped the data generation process, especially with respect to her reacting and responding to participants’ accounts of their experiences of pain and (dis)ability. Similarly, but extending beyond Calsius et al. (2015) affective and corporeal responses, NB had moments of hyperembodiment where she became aware of her responses in unexpected ways which influenced the research process, as described above. Understanding what it is like to be a young person living with chronic pain, which at times can be debilitating, allows for care, empathy, compassion and framing within the research process. This is especially pertinent when embodied resonance is stimulated within the body during the research process. Hence, NBs hyperembodiment and fluctuating pain experience shaped knowledge production in the interviews and data analysis.
In an ethics-of-care approach to herself, NB made an active choice not to disclose her invisible (dis)ability/pain unless participants directly asked, and she felt comfortable disclosing. Jessica, Sarah and Steve were unaware of NBs invisible (dis)ability. At times, disclosure of hidden identities (e.g. pain/(dis)ability) may support a transparent and open, honest interview. However, disclosure can be vulnerable, challenging and exhausting (Dickson-Swift et al., 2007), and at these ethically important junctures, researchers can shift the course of knowledge production. Indeed, disclosure of NBs pain and (dis)ability may have modified interviews where potentially Sarah and Steve may have resonated with NBs lived experience or Jessica may have been more cautious in her language use, instead of assuming NB was able-bodied. Instead of disclosing, with a body herstory of pain and (dis)ability, NB experienced an empathic response at times of hyperembodiment and thus affective and corporeal responses were greater, or different, than might be expected from researchers who have not had such pain experiences.
At times, pain can be consuming – ‘a relentless force that incessantly intrudes and dwells in one's body’ (Stensland and Sanders, 2018: 1438). The absence of pain goes unnoticed (Thomas and Johnson, 2000); thus it is important for researchers who have pain experiences to be involved in research processes to capture the nuances of participants’ lived experiences. For example, since NB was a young person living in pain, she was attuned to and empathised with Sarah's story and therefore was well equipped to facilitate a comforting, supportive space for Sarah to express her emotions and explain her experience. Comparatively, Jessica's fear of (dis)ability and restriction of movement evoked an affective response where NB retracted herself physically and emotionally. Further, Steve's sense of investment in bettering his health through a willingness to explore and risk alternative treatments created a juxtaposition of concern and similarity. The three interviews show the researcher had times ‘of similarity’, ‘of opposition’ and ‘of difference’ (Chang, 2008). These responses also prompted reflections of NBs body location within wider socio-cultural discourses perpetuating notions of youth and health/fitness and stigma of (dis)ability and invisible pain. These perceptions were evident in participants’ excerpts, and are deeply rooted in the structures, systems and discourses on ableism (Moser, 2000), promoting feelings of shame, self-stigma and ‘otheredness’, but also ‘of similarity’.
Embodied resonance and hyperembodiment contribute to shaping research about pain. Although we do not desire researchers living with pain to carry the heavy load, it is undeniable how lived experience contributes to knowledge production in pain research. At times when researchers experience hyperembodiment it is important they have emotional care and structured support mechanisms in place, including reflexive practices such as journaling, note-taking and opportunities to speak openly and comfortably with colleagues. Similar to previous recommendations by researchers with other chronic conditions, we urge researchers to use reflexive practices to help support themselves and their colleagues, with further structured support required by academic institutions (e.g. Malacrida, 2007; Seear and McLean, 2008; Wilkinson and Wilkinson, 2023). Effective support mechanisms are critical within an ethics-of-care framework. Health researchers should engage with ongoing reflexive practices (Ciotti, 2023), especially since hyperembodiment may result in greater affective responses (e.g. empathy) by researchers with lived pain/(dis)ability experiences. We advocate caring for the researcher is as important to caring for participants in an ethics-of-care framework.
Chronic pain is prevalent, thus it is germane to explore how understandings and experiences of pain are shaped by those who live with, and research, pain. This is particularly pertinent for women since they have greater rates of invisible chronic pain conditions (Osborne and Davis, 2022). Every part of their daily existence can be affected by pain and healthcare providers, family and friends and researchers without pain conditions may disbelieve or not understand the lived experience (Grundström et al., 2018). In this paper, we showed understandings, perceptions and experiences of pain and how a researcher's hyperembodied pain experiences can facilitate knowledge production. In turn, hyperembodiment could be applied to other areas of health research. For example, researchers with heart disease or mental health conditions could explore their hyperembodied experience of researching such a phenomenon.
Limitations and conclusion
In this paper we articulate three ethically important research moments showing hyperembodiment experienced by the researcher. Notably experiences of hyperembodiment in the research process were not limited to these three moments, especially when NB was in a fibromyalgia flare-up, but were selected due to their shared intensity yet differences in relational dynamics that prompted them. Notably, Sarah, Jessica and Steve were all white, middle-class, educated young people potentially enhancing resonance with NB because of her comparable social location. Research has demonstrated that significant pain care inequities exist across racial and ethnic populations, including across pain experiences, coping and stigma and racial bias by healthcare and medical practitioners (Meints et al., 2019; Wakefield et al., 2024). Future research that addresses how factors such as race, ethnicity, age, gender, class, (dis)ability and other social locations intersect and shape hyperembodied experiences, and their impacts and implications, would be of considerable value to and beyond pain and (dis)ability research. We encourage all scholars, both with and without lived experiences of pain and (dis)ability and across intersectional identities to be reflexive about their hyperembodied experiences in research processes. Being attentive to and sharing affective experiences of corporeality that are elicited in relation to our participants, yet grounded in longer theirstories of our bodies, is key to how knowledge is produced, and to research that prioritises the care and wellbeing of both participants and researchers.
Footnotes
Acknowledgements
This research is supported by an NHMRC-MRFF Stem Cell Therapies Programme Grant MRF2017213. The authors wish to acknowledge the research participants who shared their experiences and the wider ARISTOCRAT research team.
Author contributions
Nadia Bevan: project design, data collection, coding, analysis, interpretation, presentation of data, drafting, revising and editing. Claire Tanner: project design, data analysis, interpretation and presentation, drafting, revising and editing. John Gardner: project design, data analysis, interpretation and presentation, drafting, revising and editing. Nora Shields: data analysis, interpretation and presentation, revising and editing. Samantha Bunzli: data analysis, interpretation and presentation, revising and editing. David Castle: data analysis, interpretation and presentation, revising and editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research was conducted according to the Declaration of Helsinki for medical research involving human participants and was approved by Monash University Human Research Ethics Committee (ID: 35563). A feminist ethics-of-care approach was used, and all participants gave their consent to participate in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Medical Research Future Fund (MRFF2017213) as part of the Stem Cell Therapies Mission.
Informed consent
Informed consent was obtained from all participants involved in the study.
Notes
Author biographies
Nadia Bevan is a research fellow in sociology. Her research is focused on improving health and social outcomes for minority groups, and especially to identify and address barriers to enable physical activity and sport participation.
Claire Tanner is a senior lecturer in sociology and gender studies. Her research is focused on enhancing understanding of people's health experiences and the interventions and technologies they turn to for help, especially for those living with serious health and medical conditions.
John Gardner is a sociologist and Science and Technology Studies scholar. His research is focused on bioethics, the ethics of medical innovation and the future of healthcare.
Nora Shields is a Research Director at the Olga Tennison Autism Research Centre. The aim of her research is to improve the health and wellbeing of people with disability by increasing their participation in exercise and physical activity.
Samantha Bunzli is a senior research fellow and physiotherapist. Samantha's research is focussed on equipping people with musculoskeletal pain with the knowledge, skills and resources they need to participate in active, healthy lives.
David Castle is Professor of Psychiatry at the University of Tasmania and Co-Director of the Tasmanian Centre for Mental Health Service Innovation. His wide clinical and research interests include schizophrenia and related disorders, bipolar disorder, cannabis abuse, OCD spectrum disorders and disorders of body image.