
Abstract
Research on emotion is fraught with methodological limitations, as feelings can have non-discrete, ephemeral, and ineffable qualities. Audio diaries offer a method for capturing the sequential and varied experience of emotions as they emerge from everyday life. Following theory and methodological development in the sociology of emotion, we examine how audio diaries might be used to capture (a) candid emotions that emerge spontaneously and may reflect unpopular or negative social views and experiences, (b) the self as unfinished, and (c) processes of emotional reflexivity that exist alongside the diverse emotions that infuse everyday life. We explore how waveform visualization of audio recordings might be meaningfully combined with qualitative analysis of transcribed data to illustrate emotional contours in situ. We draw on audio diaries collected from 48 nurses from two US hospital systems to explore the possibilities and limitations of using audio diaries in emotion research.
Capturing emotion with audio diaries
Emotion is a slippery concept. How do we isolate and measure distinct emotions in social science research? Can emotions really be ‘measured and sifted like flour’ (McCarthy, 1989: 51)? Scholars in the sociology of emotion have struggled with this dilemma over the course of the field’s development. Technological advances open up new possibilities for measuring emotion through fMRI machines, facial electromyography (EMG), and sentiment mining through web scraping tools (Rogers and Robinson, 2014), but new technologies are often confined to laboratory settings that move the research process further away from the sites where emotions are felt and negotiated across time. Even self-report of emotions can have a detached quality. Events reported through surveys or in interviews might have occurred long ago—dampening their emotional force or encouraging participants to (re)construct a linear narrative surrounding an event or feeling (Smart, 2009: 296).
Audio diary data have the potential to bridge this gap between lived experience and analytic techniques by providing a window into the ‘spontaneous’ (Theodosius, 2006, 2008) and varied experiences of emotion that are difficult to access with survey or interview instruments. In this article, we draw on the diary entries of registered nurses as they reflect on and consider their on-the-job interactions in order to examine the utility of audio diaries as a means of accessing emotions and the self, including the processes by which participants think and feel their way through competing experiences and emotion labels.
In exploring the use of audio diaries as a primary data collection tool, this article extends past work on this unique methodology by illustrating how it: (a) provides access to more private, unpopular, and spontaneous emotions; (b) can potentially illustrate the self as an ongoing and unfinished process; and (c) enables researchers to gain access to participants’ emotional reflexivity (Burkitt, 2012; Holmes, 2010; Rosenberg, 1990) as they consider, frame, and share multiple emotionally salient experiences over time. Finally, we use wavelength visualization software to illustrate how transcripts might be paired with visualization of excerpts to enrich qualitative interpretation. We see audio diaries as providing access to ‘real world’ emotional experience, including more nonconscious and embodied aspects of speech, with the potential to visualize distinctions across types of emotion.
Audio diary process—The CARMA Project
For purposes of illustration, we draw on data from audio-recorded diaries completed by 48 nurses from two US Midwestern hospital systems. These diaries were part of a larger mixed-methods study of hospital-based nurses that focused on the emotional experiences and management practices of health-care workers. The study also included the collection of survey and interview data between 2011 and 2013 (see Cottingham et al., 2015 for details on the survey phase). Audio diaries were used as a method through which participants could reflect on their nursing shifts in an open-ended and relatively unfiltered manner (Monrouxe, 2009; Worth, 2009).
After eliciting informed consent from participants, nurses were provided with a digital voice recorder and instructed to make a recording during and/or after each of six consecutive shifts. Participants could and often did make multiple recordings throughout and even before their shifts (see the case of Leah below). Because emotional experiences and their management were the primary focus of the larger project, participants were asked to reflect on how they felt during and after their shift, to describe who and what influenced their emotions, and how they responded to their emotions or the emotions of others. Participants were compensated with a $75 check for completing the diary recordings. Each shift recording was transcribed in its entirety by the research team, de-identified, and uploaded to a software program for analysis (dedoose.com). The project was approved by the ethics review board (IRB) at the University of Akron and each of the hospital systems.
Audio diary method and emotions
Consistency in the operationalization and measurement of emotion has been difficult because how researchers study emotion is dependent on how they theorize it. Yet theorists across disciplines continue to debate the extent to which emotion is rooted in mind and/or body, is experienced directly or always subject to interpretation, or in fact, transcends these dualisms (see Savage, 2004 for an overview of theoretical approaches). These debates also infiltrate the study of emotion more directly by being linked to prominent research strands that attempt to distinguish between the examination of emotional experience and emotion management or, in the context of paid employment, emotional labor (Hochschild, 1983; Sloan, 2004, 2007; Smith, 2011). More recently, feminist researchers have raised further questions about emotion and reflexivity (Spowart and Nairn, 2014) or the ability of researchers to ‘study’ the emotional experiences of others without simultaneously considering the role of their own emotions along the way (Bondi, 2005; Denzin, 2009; Schurr and Abdo, 2016).
Although this latter topic is beyond the scope of the current paper, it raises a central point that we do wish to make in examining the methodological possibilities of using audio diaries for studying emotion; that is, examinations of emotion—and the methodological tools used to conduct them—must attend to the intimate connection between emotion, self, and interactions with others. As we will discuss below, audio diaries allow researchers to capture the ways that emotions are both social and social psychological experiences. They enable researchers to ‘see’ agentive self-processes at work while illustrating the ways that emotional experience and management are connected to one’s relationships with others and the surrounding structural and cultural context.
The use of audio diaries in research represents a hybrid between research-generated and naturally-occurring data (Paulus et al., 2013: 70). The research project itself elicits the data, but the form and content of the audio diary was determined largely by each participant and constrained only by the practical limits of the digital voice recorder used to record diary entries. When guiding in-depth interviews, researchers often shape the topic and dynamic of participants’ responses—‘“talk” in interview settings is a co-production, directed to a greater or lesser extent by the interviewer and the research focus’ (Smart, 2009: 300). By contrast, audio diaries can provide data less directed by an interviewer, though still directed by the instructions participants are initially provided. For example, in her longitudinal study of medical students’ identity formation, Monrouxe (2009) demonstrates how audio diaries can be used to examine the macro, structural element of lived experience as well as the more microsociological elements of language and social interaction.
Capturing emotional candor
Our experience with audio diaries parallels that of Theodosius (2006: 901), in that the use of diaries prompted ‘more personal disclosure of private emotions and feelings’ than might be possible with other methods (see also Brennan et al., 2010). We saw this in the experiences of racism reported by the nurses of color in our sample (a more thorough discussion of this theme is taken up in Cottingham et al. 2018. Racism operates through overt racist aggression as well more subtle forms of microaggression (Sue, 2010). Using audio diaries, we were able to capture these microaggressions even though these themes were never taken up with the same degree of candor in the follow-up interviews we conducted with nurses. This suggests that audio diaries, when recorded by nurses during relatively private moments, may provide a feeling of safety and anonymity that allows participants to open up about everyday frustrations and problems. Interviews, by their nature, cannot convey the same sense of privacy as an individual alone (or with family) with a recorder. Recorders are taken into the homes and private areas of participants, allowing participants to capture reflections in the relative comfort of bedrooms, cars, and around kitchen tables rather than in public spaces surrounded by strangers.
We can see this level of intimacy between the recorder and the participant and the resultant candor in several examples from our study of nurses. Tracy, a young nurse begins her second recording by saying,
So I would rate my day with just the patients probably about a B plus however its other events that occurred at work today that made feel the way that I’m feeling. And I almost feel like I have nobody to talk to about it, so I’m talking to a recorder because I really am kinda [too] embarrassed to even tell my husband. (Tracy)
Too embarrassed, even to tell her husband, Tracy goes on to elaborate the events that led to her embarrassment in detail. In a later shift, she tells the recorder that she stays in her car after work sometimes so that her kids do not see her crying. Audio recordings allow us to capture multiple ‘back stages’ (Goffman, 1959). In hospital and hospice settings, the conference room may provide one backstage for nurses away from patients and family members (Cain, 2012), but the car may provide another backstage, away from patients, coworkers, and family members. Audio recorders can travel across multiple front stages and back stages to capture layered emotions and their management.
In another example that highlights the emotional candor that audio diaries can elicit, Lianna, another young nurse, begins to cry while she relays a story of a patient’s gratitude in one of her recordings:
So I think, um you know that almost made me cry, it might make me cry now. Because um (pause) I think that it’s- (sigh) (pause) it’s rare for um patients to recognize your hard work (sniffle) um and, and that you’re trying your best and that you’re actually um being effective. Sorry um I don’t typically cry- it’s this recording—um but I don’t know why that- that statement just kinda struck a chord. (Lianna)
Noting that she doesn’t ‘typically cry,’ relaying the event at the end of her shift seems to provide a safe place to express her feelings no matter how atypical they may be.
Audio diaries can elicit data from people’s natural life contexts
Yet, nurses were often candid in their experiences of frustration, annoyance, irritation, and anger—emotions that carry varying degrees of moral consequence, especially for women and nurses of color (Wingfield, 2010). Expressions of hate can be particularly taboo in the health sector where caring for others is emphasized (Stacey, 2011). Yet, hatred of, for example, floating to other floors (Andrea) was explicitly referenced. As Andrea says:
But I just truly hate floating [working on another floor], and I know hate is a strong word but it’s just horrible to float cause most times when you float, you get the worst assignment, nobody is really helpful for real. (Andrea)
Even a hatred of nursing emerged, albeit somewhat indirectly in the case of Ashley:
and both them [other nurses] said, they’re like basically “I hate being back here, I hate being in the step down [unit].” And the one nurse even said “I hate being a nurse.” Like you know, “this- this is kind of getting ridiculous.” Kind of the things that we have- you know have to put up with every day, and you know it’s (short pause) there gets a point where it just [be]comes like so draining. . . (Ashley)
Even patients—for whom nurses should have compassion—could be the source of negative emotions. Janet, a nurse manager who works once a month in the emergency unit, notes,
I forget that, you know, how rude and mean patients can be. You know, when you walk in the room trying to get them assessed so um they’re like, ‘I’ve already talked to people. I’m not answering your questions’ and puts your hand in my face, and it’s like, ‘You know what you are? Rude. You are nasty’ (Janet)
These examples from Tracy, Andrea, Ashley, and Janet, along with the microaggressions experienced by nurses of color (Cottingham et al., 2018) suggest that audio diaries have the potential to capture numerous ‘back stage’ expressions of negative emotions, including sadness, frustration, and hate—all emotions that can be quite taboo for care workers to express (Bolton, 2001). Additionally, the recorder can travel across multiple back stages to capture spontaneous and unpopular emotions that participants might otherwise wish to keep hidden.
Capturing the unfinished self
In addition to capturing candid emotions, as illustrated above, audio diaries can be a tool for documenting the self as an unfinished project. Similar to other qualitative approaches, we view the narrating of personal emotions as part of a broader project of the self ‘in which the narrating “I” retells and restructures experience and the experience of the self’ (Smith and Sparkes, 2006: 173). But this narrative is ongoing and never finished. Audio diaries allow us to capture identity as ‘multiple, fragmentary, and unfinished. Identity is a performative struggle, always destabilized and deferred’ (2006: 175). Emotions are a key feature of the self (Boyns, 2006; Shott, 1979). Yet they are similarly multiple and complex. As Bericat (2016: 494–495) notes:
The study of emotions is never simple, because emotions are part of an active process and can undergo multiple and enigmatic transmutations that are both voluntary and involuntary, or conscious and unconscious [. . .] In addition, it is obvious that we do not experience isolated emotions, one at a time, nor do the emotions constitute static states in time (Williamson, 2011). Our emotional lives are dynamic processes of multiple sequences and emotional structures.
Traditional qualitative methods such as interviews can create fixed narratives in which participants reflect back on and reconstruct a coherent story with a singular dominant emotion. But in the moment, such coherence might be elusive and individuals might experience multiple and even contradictory emotions simultaneously.
We can see this complexity illustrated with the audio diary method, particularly when participants made multiple recordings over the course of a single shift. Below we draw on several excerpts from a nurse in her 20s (Tracy) to illustrate the unfinished nature of the self and the emotions captured in audio diaries. An initial event triggers a range of reactions: Tracy is asked by another nurse to help move an obese patient to a bariatric bed. Introduced above, Tracy explains that the nurse requesting help was not prepared when the others joined her, causing the following outburst:
And it was just like, I don’t know, I [was] just really annoyed at that point. I was like “oh my god. Jesus Christ, we’ve been in here 20 minutes. This is ridiculous. Like, where I came from [highly-ranked research hospital] everybody had their stuff together before they called somebody else in to help them.” So for me it was kinda a little annoying. I don’t know, like, don’t invite other people in if you’re not even ready because we don’t have time to be standing here. We have things to be doing on our own patients. (Tracy)
Continuing to reflect on the event, Tracy begins to piece together the reasons for her saying what she said:
And so you know I was anxious, I was kinda irritated, and I said the wrong thing. And I know I shouldn’t have said that. I know that’s what everybody else in there was thinking cause I could see their facial expressions as we were holding him over [so that she could dress wounds] as she was like doing this and this. So I know it wasn’t just me in what I was thinking. And you know afterwards I kinda felt bad, but I don’t know, I really did feel pretty bad for saying that cause I don’t- I just got annoyed. I was hot [temperature-wise] at the same time and those two just don’t mix. And I was anxious at the exact same time because I had all this stuff to still do. And I don’t know, the whole situation kinda came together and I think it kinda forced me to say whatever, you know. And since I could tell everybody else was thinking the same thing I thought it was okay to say and really it probably wasn’t the best choice. Sometimes I think- I think out loud and that’s not good but . . . (Tracy)
In this quote, we see the multifaceted nature of the self in process as Tracy tries to explain her annoyance while maintaining a sense of self that is reasonable and helpful to her colleagues. Her uncertainty comes through in her repetition of ‘I don’t know’ throughout this diary entry (and others).
On several occasions, Tracy relays her conflict with other nurses and an overwhelming concern with what her coworkers think of her (‘I don’t want my coworkers to think anything bad about me’). This comes through in her efforts to frame the above event initially as ‘another part of the day that happened. . .’ and the ‘whole situation. . .forced me to say whatever.’ She cites the situation as the cause of her response—an external force that includes a mix of temperature, anxiety about her own tasks, and irritation—and thus, not a reflection of who she really is. This event is one that seems to compound her sense of conflict with the other nurses—coworkers that Tracy’s preceptor says dislike her (also detailed in a later recording). This sense that her coworkers do not like her is ultimately the source of the embarrassment that she cannot discuss even with her husband (described above, ‘I almost feel like I have nobody to talk to about it so I’m talking to a recorder because I really am kinda [too] embarrassed to even tell my husband’). Using audio diaries, we can see the unfolding of events, their construction and reconstruction, across multiple scenarios in Tracy’s workday. In constructing the project that is the self, Tracy considers the environment, events, and her reactions as pieces of a puzzle that she must reconcile—a process that remains ongoing and is captured as such in candid reflections within her audio recordings.
Capturing emotional reflexivity
In addition to being able to capture candid, situated emotions and the complexity of the unfinished self, the use of audio diaries may also provide an answer to Holmes (2010) and Burkitt’s (2012) call to capture the emotional dimensions of reflexivity. As modernity ushers in new sources of uncertainty, risk, and fear, social theorists such as Anthony Giddens (1990), and Ulrich Beck (1992) highlight modern reflexivity as a primary theoretical concern at the close of the 20th century. Although these concerns may be well-founded, Burkitt and Holmes find fault with the overly rationalized and individualistic approach to reflexive processes that dominate theoretical conversations. Each further turned to symbolic interactionism as key to conceptualizing reflexivity in emotional terms, grounding reflexive processes in relationships with others (i.e. in the ‘social’ or what Holmes, 2010: 143 terms ‘relationality’) rather than reproducing self-society dualisms. Surprisingly, however, neither Holmes nor Burkitt cite interactionist Morris Rosenberg’s (1990) discussion of ‘emotion and reflexivity.’ In what follows, we outline the commonalities among these conceptualizations of ‘emotional reflexivity’ and illustrate how the audio diary method constitutes one way to empirically capture ‘how reflexivity is emotionalized’ (Holmes, 2010: 150). Consistent with the quotes from Tracy presented above, we further illustrate how self-feelings cannot be separated from relational experiences with others. Taking this approach, audio diaries have the potential to center the reflexivity of the research participants’ selves.
All definitions of reflexivity include references to self-reflections. For Burkitt, Holmes, and Rosenberg, however, these self-referential processes include grounding in emotions. Burkitt (2012) states that emotions motivate reflexivity, infusing reflexivity itself in a way that connects emotions back into the interactions and relationships in which they arise. Similarly, Holmes (2010) defines reflexivity as simultaneously an embodied, emotional, and cognitive process in which individuals try to understand their lives in relation to significant others and to the surrounding social environment that includes an array of generalized others. In contrast, Rosenberg (1990) flips the proposed relationship between emotion and reflexivity to point out that reflexive processes pervade every important aspect of human emotional experience. Here, Rosenberg points out that while the reflexive role-taking process that underlies Mead’s (1934) self-development, Cooley’s (1902) ‘looking glass,’ and most conceptualizations of agency, is most often portrayed as a cognitive process, internal states of physiological arousal or embodied feeling can also be ‘worked over’ (Rosenberg, 1990: 3) by reflexive processes and thereby take on a different character that blurs the line between physiology and interpretation.
These ‘social’ approaches to emotional reflexivity are critically important to the smooth functioning of society in that they constitute the basis of social control, role performance, and interpersonal interaction (Rosenberg, 1990; also see Shott, 1979). In addition, Rosenberg suggests that reflexive processes can be shown to influence emotional identification or interpretation (e.g. What am I feeling?), emotional display (e.g. What emotion should I show?), and emotional experience (e.g. Now that I’m thinking about it, what do I feel?). The potential to identify these varied social psychological processes and outcomes reflect some of the reasons that Holmes (2010: 148) sees a real need to ‘hone’ the measurement tools that are able to capture the emotional dimensions of reflexivity. As Theodosius (2006, 2008) illustrated in her study of emotional labor among nurses, audio diaries are able to capture these key theoretical facets of emotional reflexivity.
To further illustrate the methodological potential of audio diaries, consider an example from Leah, a nurse in her mid-50s. She relays the following reflection:
. . .just leaving the unit. I got halfway through the meds and this one patient asked me to give her- her eye drops. Well we’re not really supposed to give stuff that’s not specifically ordered in the dialysis unit. I got in trouble once doing that cuz I was trying to help somebody out, so now I had to tell her “no,” and she’s like “ok well I’ll just do it myself” but I know Trevor gives them to her and it’s like, ok, so Trevor looks good, I look like a bitch, I can’t help it. I don’t like it though, I feel bad (Leah)
Leah’s negative self-feelings emerge from her reflection about how her behavior is viewed by the patient in comparison with coworker Trevor as well as eliciting the recognition that the same behavior is evaluated more negatively by supervisory ‘others’ when she performs it than when Trevor does. Here we see Leah reflecting back on herself through the eyes of others (‘I look like a bitch’), not with cognitive dispassion but infused with negative affect (‘I don’t like it though, I feel bad’). Audio diaries can capture these moments of rich reflexivity and their emotional dimensions.
Another example of self-reflexivity and emotions that audio diaries can capture comes from Carrie, a nurse in her mid-50s who serves as the ‘care coordinator’ for her unit. Carrie begins her diary by noting the ‘power struggle’ that she experiences with night nurses who are slow to initiate giving her report when she arrives for her shift. Later in the same recording, she returns to the issue:
And I came back from that meeting feeling pretty good and finished up doing- getting some more handouts together for some more patients that were coming um later in the afternoon and I didn’t feel like I dumped any of the care coordinator’s job on a bedside nurse and as I said I was leaving an hour and 15 minutes earlier than I am supposed to, but I had made an emergency doctors appointment since I haven’t been feeling well for several weeks. So I- I felt good that everything fell into place today. Um I am a little, thinking about it, I’m a little nervous because I did not look to see who the nurses are on tonight so I’m not sure which nurses I will meet in the morning and whether I will have the power struggle over [other nurses] com[ing] and giving me updates. I know I need to learn to relax more but I don’t know how well that’s going to happen uh considering my age. I’ve never- I’m 55, I’ve never been a relaxed sort of person. (short pause) And at least I know that I don’t shout at people if they’re not in there right away. I wait and I wait but I- I do a slow burn inside which uh doesn’t feel too good either. . . (Carrie)
This quote from Carrie is rich in many ways. Here we see the embodied aspect of her reflexivity in reference to her health (she has an emergency medical appointment because she has not been feeling well) and her age—‘I’m 55. I’ve never been a relaxed sort of person.’ But we also see the looking-glass self in action as she compares her emotional experience of anger as a ‘slow burn inside’ that is more acceptable than other possible responses: ‘at least I know that I don’t shout at people.’ Her framing suggests that she is in compliance with the feeling rules—professional norms about what to feel and how to express it—of nursing (see Erickson and Grove, 2008; Virkki, 2007 for further discussion of feeling rules in healthcare and the emotional labor of nurses). Through this comparison to a more extreme response, she is able to reflect back on the self and see herself as legitimate in her feelings and emotional expressions as a nurse.
Visualizing emotion
Above, we highlighted three ways in which the audio diary method aids in capturing emotion, including its ability to capture (a) spontaneous, candid emotions, (b) the multiple emotions involved in constructing the self, and (c) processes of emotional reflexivity. Using audio data can facilitate analysis of not only what is said, but also how it is said. Diaries—as a hybrid between researcher and participant-generated data—offer recordings in which participants themselves exert a notable degree of control over the emotional tone and dynamic of the content, in contrast to interviews where interviewers steer the discussion and type of data collected more directly (Smart, 2009). One way to capture how content is conveyed is to go beyond transcription notations, by analyzing patterns in the waveforms of audio clips (Paulus et al., 2013: 151–152). Such visualizations are one way to return to the ‘texture’ of spoken word that is often lost in the transcription process (Bird, 2005; Smart, 2009: 296). Using waveforms or spectrogram output from audio software can provide a visualization of sound—including frequency and duration of pauses (absence of noise), volume, and frequency of speech. Comparing two segments of an audio diary from one participant, we might detect crude differences in mood using such visualizations. Comparing sound visualizations on their own adds little to the analysis, but comparing visualizations in relationship to the emotions referenced directly by participants suggests differences in volume and speed of talk that are more readily captured in a visual wavelength display.
Below is one example of how wavelength visualization can illustrate emotional reflections and capture more of the nuance of the spoken diary that is lost in its reduction to text. Tamara is a nurse in her late 30s. She describes a particularly memorable situation that caused her to feel ‘ticked’ and ‘P.O.’d’ (pissed off, angry). We can compare this to a visualization of a later recording that she made at home after her shift in which she describes feeling emotionally drained and guilty. Using the software program Audacity (http://www.audacityteam.org/), visual wavelengths were created for each segment of similar length (both are roughly 1-min and 45 s in length) and screen captures of the wavelengths were taken to store them as images.
Tamara shows the visualization of her ‘ticked’ segment—the description she uses after a quick, high-pitched laugh that peaks the wavelength just after the 30-s mark (Figure 1). The wavelength peak just after the 1:15 mark is as she says the word ‘why’ with notable agitation in ‘I’m not sure why. Maybe cuz I’m Black. I don’t know.’
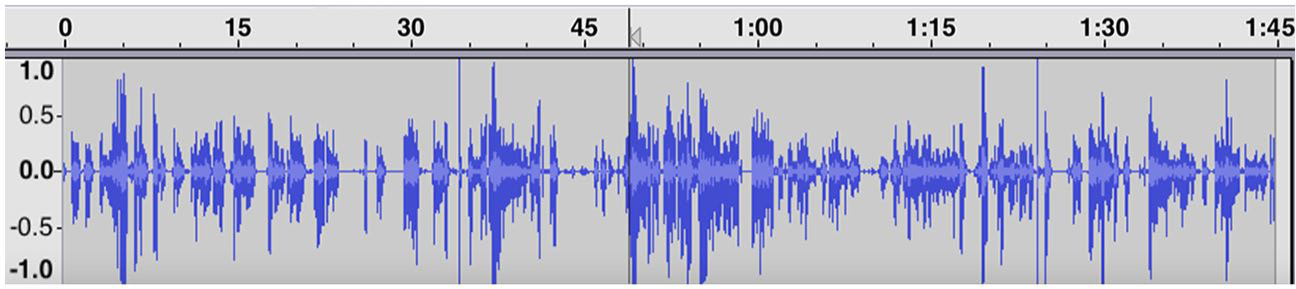
Tamara’s ‘ticked’ segment (shift 2, part 1).
We can compare Figure 1 that visualizes Tamara’s feelings of anger and confusion with the visualization of emotion in Figure 2. ‘Draining’ is the description Tamara gives at the beginning of this segment shown in Figure 2. The peak just after the 15-s mark is from a breathy laugh as she describes her sister ‘who has MS is sitting on the bedside commode’ when she gets home from work. The second peak after the 45-s mark is when she has a similar breathy laugh but in conjunction with the word ‘compassionate’ as she says ‘I’m trying to be as empathetic and compassionate as I want to be, but I know I’m really not. So I feel kinda crappy, guilty maybe about that.’ Just before the 1-min and 30-s mark she draws out the words ‘draining’ and ‘frustrating’ before finishing with ‘because you leave it and you come home to it. . .you know. . .yeah.’ Visually, we can see that the segment ends with longer pauses, muted remarks, and sighs, suggesting low energy and visually representing the drained feelings she expresses, particularly in comparison to the lively energy seen in the first figure when she discusses feeling angry. More on Tamara’s experience can be found in Cottingham et al. (2018).
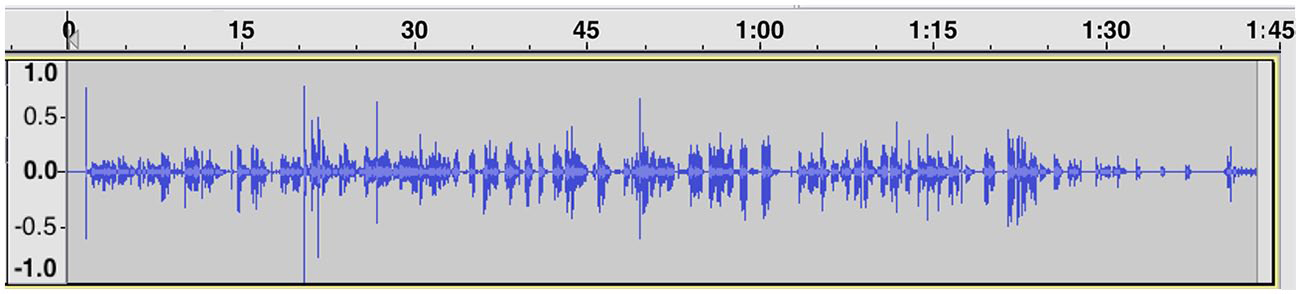
Tamara’s ‘draining’ segment (shift 2, part 2).
A second example of visualizing emotion with waveforms comes from Leah (from her second shift). At the beginning of her recording—made in her car as she is driving to work—Leah discusses her anger—being ‘pissed off’ because she has to work on a day that she was not originally scheduled to work. We can see this visualized in the waveform shown in Figure 3.
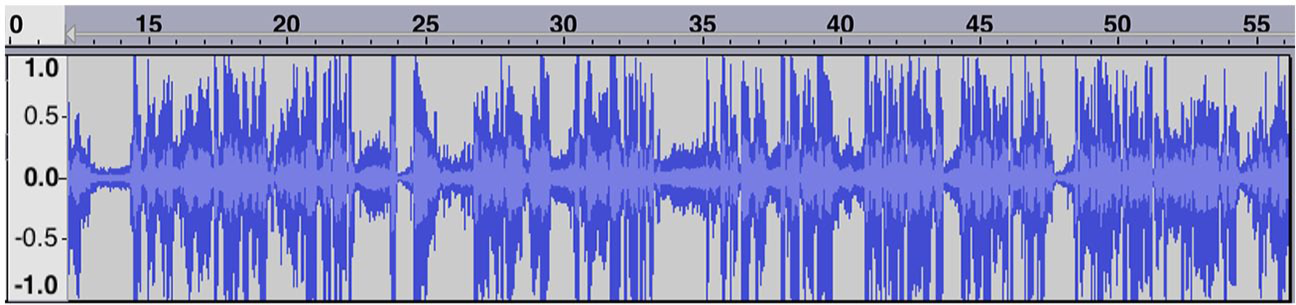
Leah’s ‘righteous indignation’ segment (shift 2, part 1).
The following quote corresponds to the 44-s segment shown in Figure 3:
[. . .] I am mildly pissed off because of the schedule being screwed up, this was supposed to be a day off and it’s a nice day. But um what I am going to do is shift gears and by the time I get to work concentrate on just taking care of my patients and taking care of what’s going on there and not getting into all that. I just need to retain enough righteous indignation so that when I am talking to my manager or whoever is going to be dealing with this schedule [. . .] (Leah, shift 2, part 1)
We can compare this segment from the beginning of her shift with a segment of recording of similar length (46 s) made at the end of that same shift. Similar to Tamara, we can see the fatigue visualized in the waveform in Figure 4. In contrast to her earlier discussion of being pissed off and working to ‘retain enough righteous indignation,’ we see a different configuration of emotions. Within the second segment, she describes her lack of enthusiasm for continuing the shift. She reflects on this lack of desire (‘I don’t want to stay’) by stepping outside her own feelings and contrasting them with the dire circumstances of her young patient. This reflexivity leads her to conclude that she has reached the human limits of one’s ability to be compassionate. In the quote below, she indicates the normatively applied human limit through her pronoun shift from ‘I’ to ‘you’ to ‘I.’
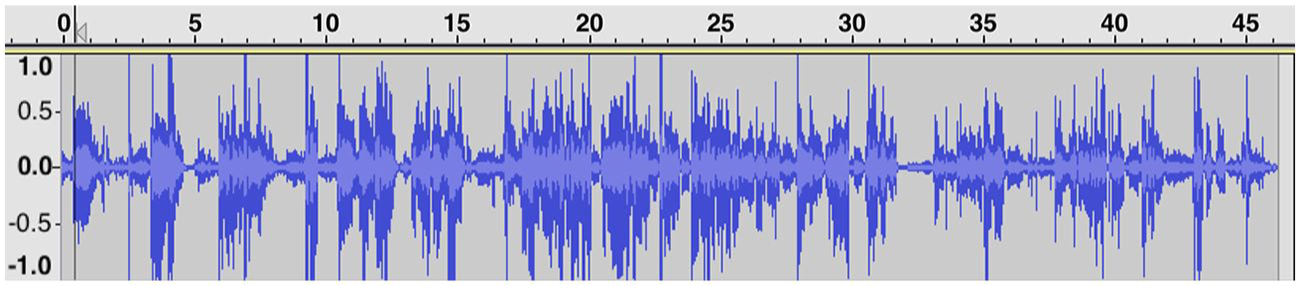
Leah’s ‘lose your ability to be compassionate’ segment (shift 2, part 3).
The following quote corresponds to the 46-s segment shown in Figure 4:
Ummmm, and you know what, I don’t want to stay at night to finish off this kid in the PICU [Pediatric Intensive Care Unit] (0:14) and you know what, here’s this kid who’s probably dying and his family’s all around him and they’re concerned and I’m over here upset because I might have to stay late and that’s really kind of a nasty feeling to feel that way, but (0:30) that’s how I feel. [pause] Sometimes you just lose your ability to be compassionate and I think [small pause] I’ve hit it. (Leah, shift 2, part 3)
Within the last 16 s of the segment (:30-:46), Leah says only 19 words (starting at ‘that’s how I feel’) compared to the 44 words she uses in the previous 16 s. Her first long pause (just after the 0:31 mark) is after stating ‘that’s how I feel.’ She lets the weight of that statement sit for a moment before slowly drawing out the word ‘sometimes.’ A second, shorter pause appears at the end before she ends with the peak at the 43-s mark saying ‘I’ve hit it’ (note: the peak at 0:45 is actually background noise).
To be sure, waveform visualizations cannot provide definitive proof about the presence of some emotions over others nor are they able to fully capture the sighs, deep inhales, uses of sarcasm, or many of the other subtle features of spoken diary entries that convey emotional meaning. They do, however, offer some insight into how speed, pitch, and pauses correspond to different emotional expressions and, arguably, levels of emotional energy (Collins, 2004) that vary across time and interactional episode. While there is little that can serve as a substitute for hearing the recordings directly, the need to protect participants’ confidentiality compels us to turn to other means to convey these nuances of spoken feeling. Visualization of audio wavelengths, in combination with transcripts, can lend themselves to further qualitative interpretation of these subtleties, conveying the emotional energy of a segment to others who do not have direct access to the recordings themselves.
Limitations of audio diary method
Despite the outlined strengths of using audio diary methods, this form of data collection and analysis is not without logistical and design limitations. As already discussed, researchers relinquish a degree of control over the data collection process when they remove themselves during participants’ use of recording devices. Being physically absent means that the recorder might capture more candid and private moments of emotion and reflexivity, but this assumes that participants understand and feel empowered enough by the research process to turn on the recorder and share their stories—a process that requires the cultivation of some level of trust and rapport between participant and researcher. Without understanding, empowerment, and trust, diary entries might remain superficial and infrequent. Being absent at the point of data collection also limits the ability of the researcher to interject and ask for clarification or elaboration of a particular point. Probing questions, a powerful technique in eliciting rich data during interviews (Miller and Crabtree, 2004), are difficult to implement in an audio diary study. Audio diaries are but one tool in the qualitative toolbox.
Audio diary methods can also raise important ethical concerns. At numerous points in the data collection process, it sounded as though participants were making recordings while driving and also seemed to capture the voices of other coworkers and family members during recordings. These present real challenges about the obvious risks of handling gadgets while operating a vehicle and the issue of confidentiality of those who did not agree to be a part of the research project and yet become involved due to the participants unhindered use of the recorder. Both such issues would emerge in the elicitation of audiovisual recordings, though with visual recording of faces, the sense of breached privacy might be even higher. We did instruct nurses to avoid recording others and chose to only paraphrase rather than transcribe any background conversations between participants and non-participants.
Additionally, the transcription process required multiple team members and discussions on conventions for this particular type of data. Audio diary transcription might be more straightforward compared to the use of other audiovisual data (Rose, 2004). But long and sometimes disjointed monologues as well as the background features of beeping medical equipment, music, traffic noises, sounds of participants walking, sighing, laughing, and crying, all demanded intense scrutiny during the transcription process. These difficulties are not necessarily unique to transcribing audio diaries, as Bird (2005) also highlights the challenges of transcribing focus group recordings.
Conclusion
Emotion research has progressed across the social sciences, but has often been hampered by the three methodological limitations we highlight here: the need to capture (a) spontaneous, and even unpopular, emotional experiences that might highlight (b) a fragmented and unfinished self in relation to (c) the overlapping processes of reflexivity. Addressing these gaps, we drew upon a sample of US nurses who completed audio diaries before, after, and throughout six consecutive nursing shifts. Using examples from these data, we illustrate the methodological possibilities of audio diaries for researching emotion. Digital recorders are innocuous gadgets that are small, easy to use, and transportable from the hospital bedside to the private spaces of cars, kitchens, and bedrooms. Ethically, participants should be instructed to refrain from recording others (knowingly or unknowingly). Audio diary data offer novel possibilities for analyzing emotional speech using waveform visualization. Certainly, recent theorizing in the sociology of emotion suggests that emotion and cognition are only analytically distinct domains of investigation (Jasper, 2014) and audio diary data can capture how cognitive and emotional modes overlap one another in reflexive processes of thinking and feeling through different emotional states and cognitive interpretations.
Footnotes
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported here uses data from a larger study, “Identity and Emotional Management Control in Health Care Settings,” funded by the National Science Foundation (SES-1024271) and awarded to Rebecca J Erickson (PI) and James M Diefendorff (Co-PI).