
Abstract
The current COVID-19 pandemic has come to impact all areas of life involving the health, psycho-social and economic wellbeing of individuals, as well as all stages of life from childhood to old age. Particularly, the frail elderly have had to face the gravest consequences of the disease; while reporting measures tend to differ between countries making direct comparisons difficult, national statistics worldwide point to a disproportionate and staggering share of COVID-19 related mortality coming from residential long-term care facilities (LTCFs). Still, the severity of the impact on the institutionalized elderly has not been uniform across countries. In an effort to better understand the disparities in impact on Europe’s elderly living in LTCFs, we review data on mortality outcomes seen during the first wave of the pandemic (months March to June 2020). We then set out to understand the role played by the following two factors: (1) the infection rate in the general population and (2) member state adherence to policy recommendations put forth by the European Centre for Disease Prevention and Control (ECDC) targeting the LTC sector. Regarding the latter, we compare the content of national policy measures in six countries – Austria, Denmark, Germany, Ireland, Spain and Sweden – with those of the ECDC. Our findings establish that infection rates in the general population accounted for most of the variation in mortality among member states, however adherence to EU policy helped to explain the residual variation between cases. This suggests that in order to best protect the institutionalized elderly from infectious disease of this kind, countries need to adopt a two-pronged approach to developing measures: one that aims at reducing transmission within the general population and one that specifically targets LTCFs.
Introduction
The current COVID-19 pandemic has come to impact all areas of life involving the health, psycho-social and economic wellbeing of individuals, as well as all stages of life from childhood to old age. Particularly, older persons have had to face the gravest consequences of the disease; relative to other age groups and across all countries in which COVID-19 has spread, 94% of all fatalities to date are uniformly concentrated in the population 60 years and above (ECDC Public Health Emergency Team et al., 2020). Owing especially to their increased physical vulnerability and close co-habitation, the elderly living in residential long-term care facilities (LTCFs) have been especially at risk of contracting the disease. Preventive measures undertaken in the way of isolating this population have introduced their own psycho-social costs and the trade-off between physical and mental health may prove substantial. Moreover, whereas – in the absence of vaccines – social distancing may be a key to preventing transmission of the virus, in dealing with the LTC population, where physical interaction is part and parcel to good care, providers are faced with a double bind; either compromise the quality of care-giving interactions or put care recipients at increased risk of exposure.
While reporting measures tend to differ between countries making direct comparisons difficult, national statistics worldwide point to a disproportionate and staggering share of COVID-19 related morbidities and mortalities coming from LTCFs (European Center for Disease Prevention and Control (ECDC), 2020d). Still, the severity of the impact on the institutionalized elderly has not been uniform across countries. Even within a single region such as the European Union (EU) – of interest here – substantial differences can be observed (ECDC, 2020a). In an effort to better understand the disparities in impact on Europe’s elderly living in LTCFs, we begin by reviewing data on mortality outcomes seen during the first wave of the pandemic (months March to June 2020). We then set out to understand the role played by the following two potential contributing factors: (1) the infection rate in the general population and (2) specific policy measures to protect residents in LTCFs. Concerning the latter, we review the evolution of evidence-based guidelines put forth by the European Centre for Disease Prevention and Control (ECDC) targeting the LTC sector. We then examine how individual member states responded to the crisis, comparing national policy measures in six countries – Austria, Denmark, Germany, Ireland, Spain and Sweden – with those of the ECDC. The objective is to identify the nature (i.e. timeliness, extent, implementation) of member state adherence to EU policy and to subsequently explore how these relate to outcomes in mortality for LTC recipients. Implicit in this analysis is an assessment of the effectiveness of EU-level policy in improving outcomes during the first wave. Our study concludes by reflecting on the relative contributions made by the two factors (infection rates in the general population vs policy adherence) in driving the differences in mortality observed between countries. We also put forth a number of next steps for research and tentative recommendations for policymaking.
COVID-19’s descent on Europe 1
While the first three cases of COVID-19 found in Europe were recorded on 24 January 2020 in France, by 21 February 2020, the virus had already spread to at least nine other countries involving at least 47 cases (Spiteri et al., 2020). As can be seen in Figure 1 which illustrates the cumulative number of incident cases across a 14-day period per 100,000 people for both the EU-average and for selected countries, by mid-March the region would become gripped by a first major wave of outbreaks (World Health Organization (WHO), 2020). Across the 3-month period that ensued, more than 1 million cases and more than 125,000 COVID-related deaths would be confirmed in Europe alone, rendering it a global epicentre for the spread of the virus. It was not until the end of May that the incidence across Europe would drop substantially (see Figure 1). Up until that point, differences could be observed between countries regarding the intensity, as well as the rapidity of spread. While such developments cannot be attributed to any single factor, disparities in the impact of COVID-19 on the morbidity and mortality of European populations are likely linked to distinct governmental approaches in place in these countries at the time. Indeed, data collected as part of the Oxford COVID-19 Government Response Tracker (OxCGRT) point to substantial differences in the stringency of national policy to control the pandemic (Hale et al., 2020). Such differences may have played an important part in explaining the trajectory of the virus during the first wave seen in countries around the world. By way of example, research establishes the efficacy of physical distancing measures, when implemented early, as a means of reducing the incidence and reproduction numbers of COVID-19 (Islam et al., 2020: 6; Koh et al., 2020: 7). Such findings highlight the significance and relevance of conducting further research into the complex interconnections between specific policy measures and their efficacy in reducing mortality associated with the virus.
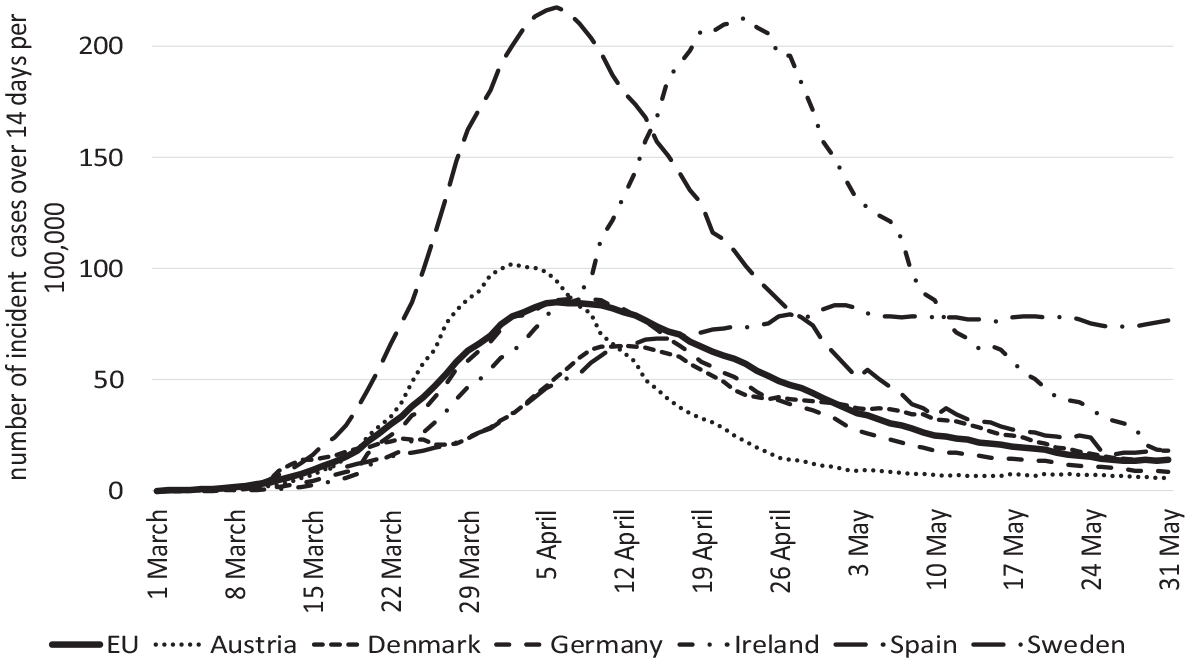
Number of incident cases over 14 days per 100,000 in Europe and select countries from March to end of May.
Research design and methods
Objectives
Bearing in mind the findings of the OxCGRT, as well as national differences in incident cases illustrated in Figure 1, this study explores the relationship between the spread of the virus in the general population, as well as policy measures specific to the LTC sector, and COVID-19 related mortality for institutionalized care recipients. Accordingly, we begin by conducting regression analysis (chapter 4.1) to establish the correlation between the spread of the virus in the general population and the mortality of residents in LTCFs. This helps to shed light on the extent to which mortality outcomes for the target population can be explained in terms of trends seen in the broader population. We then review the evolution of COVID-19 related policy recommendations for the LTC sector made by the ECDC and explore how these were put into place during the first wave of the pandemic in select member states (chapter 4.2). In a final stage of analysis, we bring together the qualitative and quantitative findings of our study to identify how the adoption of sector-specific policy impacted the mortality of residents (chapter 4.3). This leads us to identify a number of important limitations in extant data that come to bear on the robustness of our findings (chapter 5). Bearing these in mind, we conclude by drawing a number of tentative conclusions on how to better protect the frail elderly in future waves of this or other pandemics (chapter 6).
Data, case selection and methods
For the purposes of the regression analysis, the impact of the pandemic on residents in LTCFs draws on data provided by ltccovid.org (Comas-Herrera et al., 2020b). This includes mortality statistics up until 26 June 2020. For data on the impact of the pandemic on the general population, we rely on the ECDC (2020a) as a source. In order to strengthen the validity of the findings of the regression analysis, we also include data for countries falling outside the European region to maximize the number of observations. To analyse the correlation between the spread of the virus in the population and the mortality of residents, we adopt a linear regression model. Comas-Herrera et al. (2020b) describe two different ways to measure the mortality of residents in LTCFs: first, one can refer to the number of residents who died with the virus compared to all COVID-19 related deaths in the general population; second, one can refer to the number of residents who died with COVID-19 compared to all residents. In an effort to make the best of comparable data, we analyse both indicators and decide afterwards which one is the best as an indicator for the dependent variable, resident mortality, in our regression. Meanwhile, concerning the independent variable – the spread of the virus in the general population or ‘general impact’ – we refer to the following two indicators: (1) cumulative cases per 100,000 people and (2) cumulative deaths per 1,000,000 people, not including deaths of residents in LTCFs. Data for indicators for both the dependent and independent variables fall within a shared period of observation – that is, months March through June 2020.
Meanwhile, as concerns information on measures specific to LTCFs, here we look to the authors of the said recommendations – the ECDC once again – as a source (ECDC, 2020b). We then review country reports published by ltccovid.org , which follow the adoption of EU measures in individual member states. For some cases, we also supplement data from the country reports with additional sources. These are reported in the results. Our analysis subsequently focuses on a subset of six countries for which comparable data on the impact of the pandemic on residents of LTCFs, as well as on sector-specific policy measures are available: Austria, Denmark, Germany, Ireland, Spain and Sweden. In addition to the availability of comparable data as a selection criterion, the six cases represent considerable variation on the dependent variable (to be discussed). Our choice of cases also reflects the tradition in comparative welfare state scholarship to capture and compare a range of system types: here, social health insurance systems (Austria, Germany) and national health services, organized centrally (Ireland), regionally (Spain), and communally (Denmark, Sweden; see, for example, Schölkopf and Pressel, 2017). However, it is important to note that unravelling the potential implications of the system type on mortality during the pandemic is beyond the scope of this study.
Results
Correlation between spread in the population and mortality of residents
In the 21 countries under scrutiny in this study, the average number of COVID-19 related deaths among residents of LTCFs as a percentage of all COVID-19 related deaths in the general population is about 50% – with an interquartile range (IQR) between 34% and 61%. On one hand, this is indicative of the particular vulnerability of residents in LTCFs irrespective of context. On the other hand, a good deal of variation emerges between the countries. Upon closer examination, however, it becomes evident that this variation is strongly correlated with the percentage of the population living in a LTCF (r = 0.74, p < 0.01). The indicator is, therefore, not particularly useful as a comparative measure of resident mortality. Accordingly, we restrict our focus to the indicator ‘COVID-19 related resident deaths as a % of all residents’ in what follows. As illustrated in Figure 2, data for this indicator are available for 18 countries worldwide. Residents who died with COVID-19 as a percentage of all residents vary between 0% (Malta and Jordan) and 6.1% (Spain); with a bottom quartile of 0.3% and a top quartile of 3.0%; a median of 1.0%; and a mean of 1.9%, revealing a skewed distribution. The coefficient of variation is 1.02.
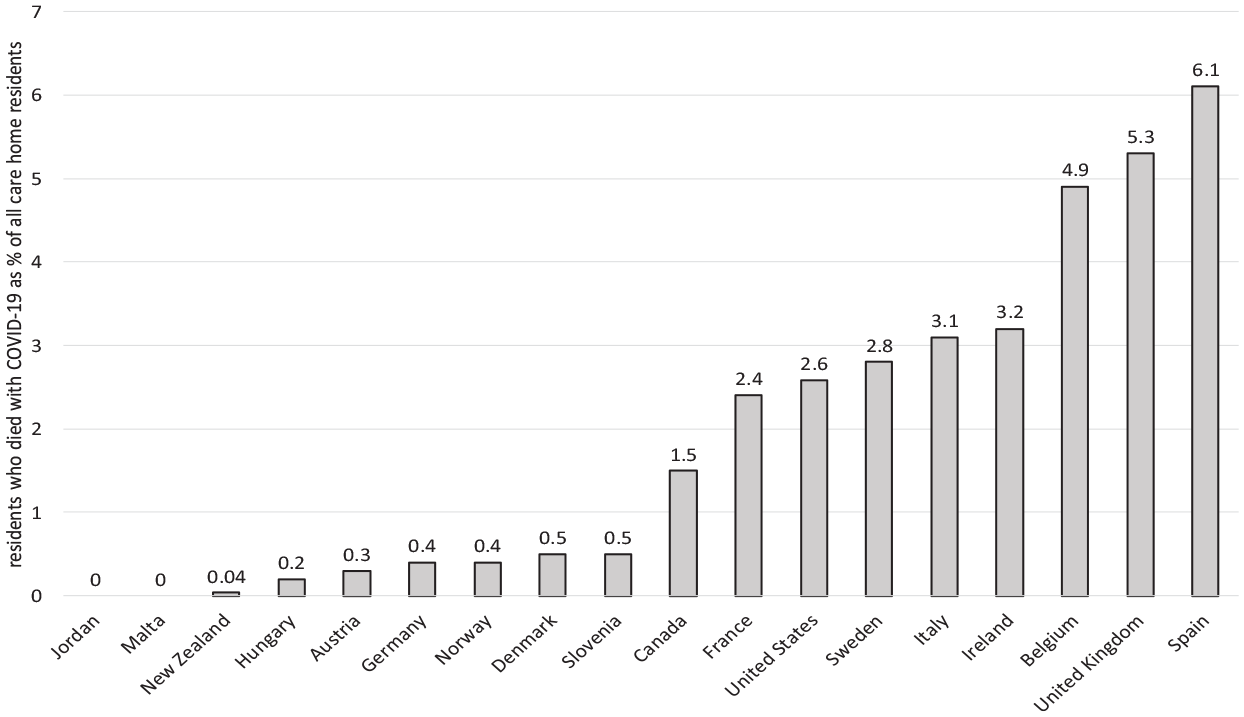
Mortality of residents in LTCFs in the middle of June 2020.
The results of a linear regression model carried out for the dependent variable, resident mortality, can be found in Figure 3. Summarizing the findings here, both explanatory indicators (cumulative cases per 100,000 population and cumulative deaths per 1,000,000 not including resident population) correlate significantly with the number of residents who died with COVID-19 as a percentage of all residents (dependent variable): both p < 0.001, with a high (r2 = 0.66) or even very high (r2 = 0.92) share of the variance accounted for. Excluding outliers from the analysis, r2 for both cumulative cases (r2 = 0.59) and cumulative deaths sinks (r2 = 0.91) and a highly significant positive correlation emerges (both p < 0.001). Nevertheless, some unexplained variance remains (r2 < 1).
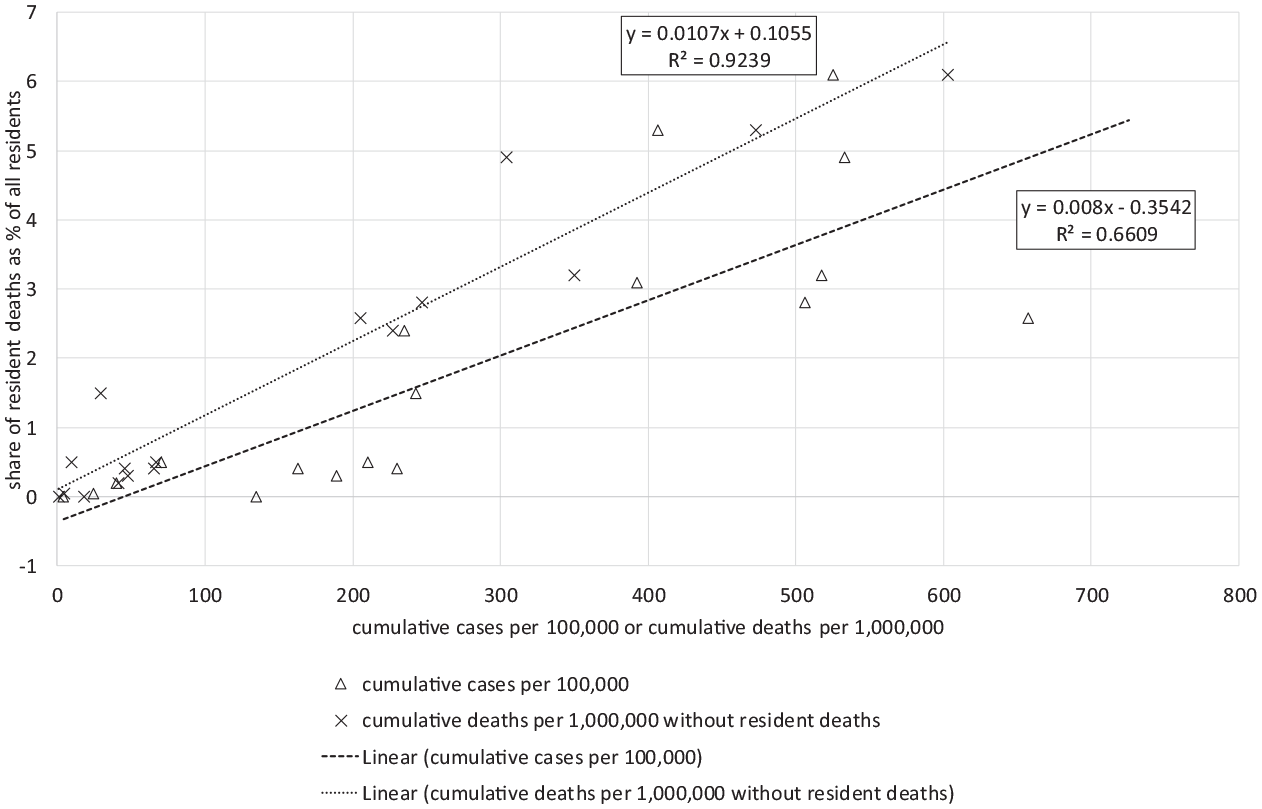
Correlation between general impact and number of resident deaths as a percentage of all residents.
As concerns the independent variable, a significant correlation can be detected between both indicators (r2 = 0.37, p < 0.01), which is taken as evidence of their validity as measures of the occurrence of infection in the general population. However, this is not to suggest that they offer 100% validity, especially given the fact that figures for both infection and mortality depend greatly on the nature of testing and reporting practices in a country. This is especially true of the indicator ‘cumulative cases per 100,000 people’ for which under-reporting is likely to be most problematic due to poorer detection of cases compared to deaths. For this reason, and owing to the high value of explained variance offered by the indicator ‘cumulative deaths per 1,000,000 without resident deaths’ (see Figure 3), we restrict our focus to this indicator in the analysis that follows.
Bearing these findings in mind, we now assess what has been done within Europe to protect residents in LTCFs, beginning with recommendations put forth by the ECDC. We then evaluate how select member states have implemented these guidelines during the first wave of the pandemic, and, what impact, if any, this has had on the mortality outcomes observed earlier.
ECDC guidelines on preventing the spread of COVID-19 in LTCFs
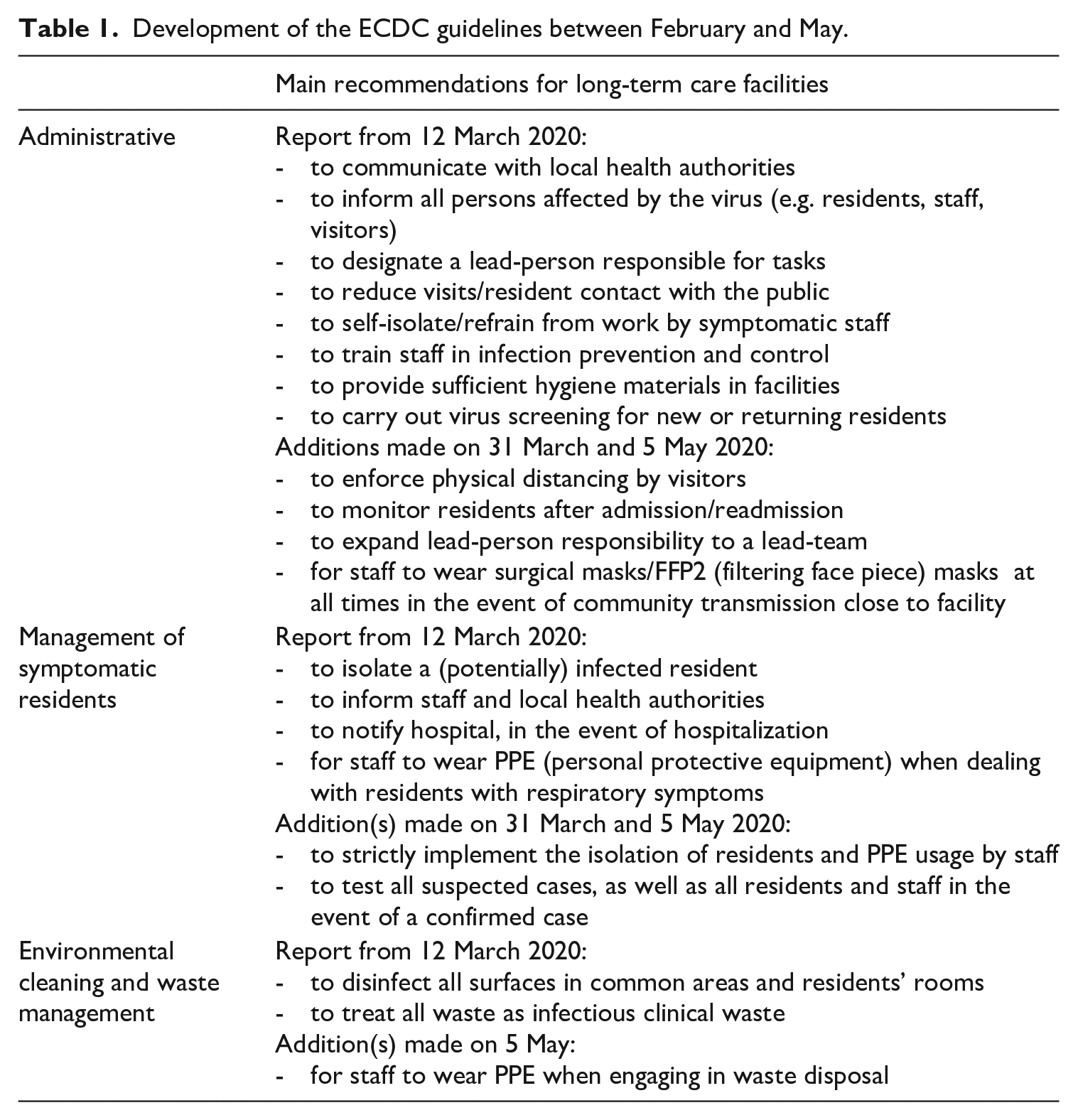
ECDC guidelines on infection prevention, control and preparedness for COVID-19 in healthcare settings were first published on 2 February 2020 and subsequently updated five times (as of 23 October 2020): on 12 March, 31 March, 5 May, 3 July and 6 October. As the present analysis concerns developments falling within the first wave of the pandemic, in what follows, we focus on the content of the first four iterations of the report, tracing especially evolving measures targeting the LTC-sector. Crucially, the earliest version of the ECDC’s (2020c) guidelines on 2 February 2020 does not make explicit mention of measures specific to LTCFs. These first appear in the update on 12 March. Although the structure of all subsequent reports varies somewhat, three relevant sections can be found in each and include regular updates over time – namely, administrative measures, management of residents with symptoms of COVID-19 and environmental cleaning and waste management. Table 1 shows the development of the ECDC guideline specific to LTC between February and May.
Development of the ECDC guidelines between February and May.
Member state adherence to ECDC guidelines
In what follows, we present an overview of measures introduced by select EU member states during the first wave of the pandemic. In some cases, measures refer to actions mandated by national governments. In others, they comprise non-binding recommendations. Given the difficulty in discerning the real impact of either (e.g. compliance might be low even where measures reflect mandates, particularly if capacity to implement and enforcement is lacking; alternatively, compliance with recommendations might be high if political will and resources allow), we do not systematically account for this distinction in our analysis that follows. Meanwhile, in an effort to validate the accuracy of our data-source (i.e. country reports by ltccovid.org ), before beginning our analysis, we crosschecked the content of three reports with that of the original guidelines put forth by the respective national governments: Austria (Bundesministerium Soziales, Gesundheit, Pflege und Konsumentenschutz (BMSGPK), 2020), Germany (Robert Koch-Institut (RKI), 2020) and Ireland (Health Protection Surveillance Centre (HPSC), 2020). In doing so, we found that the reports in question successfully captured the main measures adopted in these countries, even if they at times lacked in detail. This supported our decision to rely upon ltccovid.org as a source for English-language policy reporting in the six cases included in the study. It bears noting that just as national guidelines vary among member states, so too does the content of the information included in reports, making direct comparisons between countries difficult at times. We, therefore, summarize policy measures for each case individually, before drawing them into comparative perspective in the section to follow. In our analysis of member state adherence to ECDC guidelines, we focus especially on three aspects: (1) the timeliness of measures adopted, which we define in terms of the number of days elapsing between the start of the pandemic’s outbreak in a country and the introduction date of measures. In line with Hartfield and Alizon (2013), as well as Koh et al. (2020), to mark the beginning of a pandemic, we refer to the date on which 100 persons are diagnosed with the virus; (2) the extent or number of ECDC guidelines addressed by national measures in reports reviewed; and (3) the nature of member state support for the implementation of measurers in line with the ECDC standards. For each of these dimensions, we provide a rating from one to three (+), with three representing the highest level of performance. We then add all points together for a final value for each country (see Table 2). This is intended to serve the reader as a simple overview of policy in the member states. However, it is important to note that we do not assign any additional weight to any of the three evaluative dimensions. Instead, we assume that in order for policy to be effective that it has to be timely, reflect evidence-based guidelines, and be well implemented. Hence, all three aspects are held to be equally important in our analysis.
Member state adherence to ECDC policy (+ low adherence; ++ medium adherence; +++ high adherence)
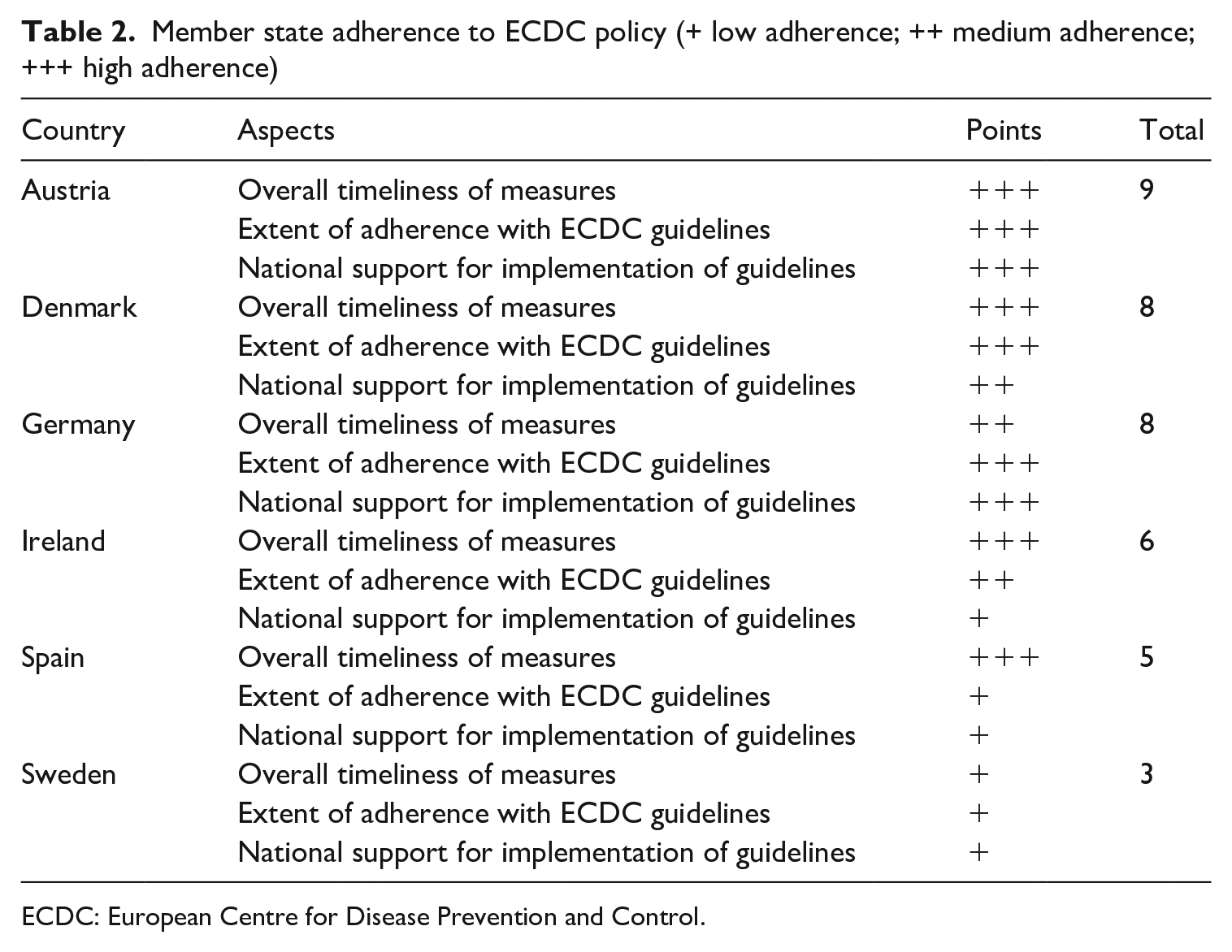
ECDC: European Centre for Disease Prevention and Control.
Austria
In Austria, an official set of governmental guidelines on addressing COVID-19 in the LTC sector was first published on 1 April, just 23 days after the onset of the pandemic in the country (BMSGPK, 2020; Schmidt et al., 2020: 9f). However, the restriction of visitors to facilities was introduced even earlier on the 21 March – only 9 days after similar recommendations were made by the ECDC in its first updated report (12 March). In terms of the extent to which national measures generally followed in line with ECDC policy, a look to sources for Austria (BMSGPK, 2020; Schmidt et al., 2020: 9f) point to the adoption of nearly all European guidelines. In some instances, Austrian measures even precipitated or were more rigorous than those of the ECDC. For example, the aforementioned restrictions on visitors to LTCFs translated to a full prohibition of visitors in some regions. Meanwhile, the national guideline on wearing surgical masks was introduced more than a month prior to the ECDC’s own issuing of the recommendation. In contrast, Austrian policy has not yet attended to the ECDC’s call for increased monitoring of new admissions and releases in the LTC sector. However, some regional governments in the country have advanced the use of restrictions – even a complete stop – on admissions. With regard to the use of testing for suspected cases, here the use of a systematic strategy is mentioned in the country report but this is not elaborated in detail. Finally, as concerns national support for the implementation of measures, the Austrian government allotted €100 million to the LTC sector at the beginning of the pandemic to facilitate the implementation of guidelines. Additional measures were also undertaken in order to provide LTCFs with the necessary resources (e.g. for hygiene and protective materials) and to speed up bureaucratic processes. This appears to have been effective, as the Austrian report does not point to any evidence of poor access to materials or testing in facilities. Given the highly timely (even prescient), extensive adoption of ECDC guidelines, which received generous support for implementation, in Table 2, we characterize the Austrian response to the LTC sector with a total of nine out of nine points (i.e. three + signs per category).
Denmark
In Denmark, the first official guidelines to prevent and control the spread of COVID-19 in LTCFs were introduced on 17 March, only 5 days after those of the ECDC and 7 days following the onset of the pandemic in the country (Rostgaard, 2020). By 8 April, the majority of European recommendations had been co-opted into national policy. In some instances, Danish measures even exceeded the stringency of ECDC guidelines (e.g. all visits to LTCFs came to a halt for a period of several days). As concerns the testing of residents and staff within LTCFs, guidelines in Denmark were announced 1 month prior to those issued by the ECDC. Moreover, the country introduced a policy for testing all residents and staff members, not only in the event of confirmed contacted to an infected person, but also wherever contact to a suspected case is established. National policy called for testing to take place within 24 hours, with repeated testing 7 days later. This strategy was expanded by additional measures introduced on 4 and 20 May, reflecting the country’s heavy emphasis on expedient and comprehensive testing to control the spread of the virus within the LTC setting.
As concerns support for the implementation of measures in line with ECDC guidelines, these mainly took the form of legally binding recommendations to facilities, the implementation of which would be monitored by the local administrative bodies. Notably, the Danish country report points to a number of severe implementation problems characterizing the outset of the pandemic. For example, LTCFs across the country faced shortages involving protective materials (e.g. masks, gloves) owing to the priority given to the hospital sector. In a similar vein, while the country’s testing strategy was ambitiously formulated, de facto access to tests for the LTCF population (residents and staff) was poor relative to other groups. Among the factors favouring implementation, the decentralization of specific measures, as well as financial support (100 million DKK) for local authorities to carry out or monitor measures come to the fore in Denmark. Taken together, the Danish policy response can be described as highly timely (+++) in its overall responsiveness, extensive in its adoption of ECDC guidelines (+++), however, somewhat lacking in support for implementing measures to improve access to crucial hygiene materials and testing for the LTC sector (++).
Germany
The first governmental guidelines addressing the stationary LTC-sector were published on 15 April in Germany, marking 45 days after the start of the pandemic in the country (Lorenz-Dant, 2020; RKI, 2020). National policy largely followed in step with ECDC guidelines. In some instances, national measures even predated their European counterparts, such as in the wearing of surgical masks in LTCFs which was introduced 3 weeks earlier in Germany. In other instances, the country’s guidelines also exceeded the ECDC’s in rigour: for example, German policy on new admissions and transfers called for the isolation of even asymptomatic residents for a 14- and 7-day period, respectively. Close clinical monitoring of both residents and staff was also urged. This included the testing of suspected cases – a measure introduced 3 weeks prior to the ECDC. In the event of a positive test result, the screening of all residents in regular 2-week intervals was advised. Meanwhile, from the 2 April, many German states prohibited visitors to LTCFs for up to several weeks, once again going beyond recommendations by the ECDC. As concerns governmental support for the implementation of measures, guidelines defined by the Robert Koch Institute, which is the government’s responsible scientific agency for infectious diseases, were treated as non-legally binding recommendations. To support their voluntary implementation nevertheless, national efforts to lessen the financial and bureaucratic burden on LTCFs were put into place. This included the temporary lifting of the minimum wage law for LTC personnel, as well as a one-time bonus payment made to nursing staff to supplement their income. Regarding the implementation of measures to assure adequate access to protective and hygiene-related materials, as well as the availability of testing, the German country report makes no mention of deficits, but in an additional study by Wolf-Ostermann and Rothgang (2020: 269f), a shortage of PPE at the beginning of the pandemic in German LTCFs was reported. The same study also established that most LTCFs adhered closely to national recommendations which corresponded closely with ECDC guidelines (Wolf-Ostermann and Rothgang, 2020: 270f). Taken together, Germany’s policy response to the crisis can be described as moderately timely, owing to the longer lag between the pandemic outset and national response compared to Austria and Denmark (++), highly extensive in its adherence to ECDC guidelines (+++) and strong in its support of implementation of measures (+++).
Ireland
The earliest measures to protect the institutionalized elderly against the spread of COVID-19 were restrictions on visits to LTCFs, introduced on 6 March (HPSC, 2020; Pierce et al., 2020). These were issued shortly before the country’s first set of broader guidelines on 16 March, the National Action Plan (NAP), released just 1 day after the pandemic took off in Ireland. In the weeks that followed, the NAP underwent several updates and was amended by additional recommendations. In terms of content, the country report (Pierce et al., 2020) makes references to the adoption of many ECDC recommendations (e.g. hospital transfers, testing strategies), however detailed information as to how this was achieved is often lacking. A number of important divergences from ECDC guidelines were observed however. These especially concerned differences in the so-called cocooning of persons from ages 70 onward, as well as family members and other risk groups. Cocooning refers to the minimization of all social contacts for risk groups, including prohibitions on leaving one’s domicile, which also encompasses LTCFs. Furthermore, restrictions on visitors were implemented so strictly in the country that even routine inspections by authorities were not permitted. As concerns testing, national guidelines did not specify concrete actions to be taken. However, from the 26 March, Irish national policy addressed this area with references to the prioritization of testing of residents and staff in LTCFs can be found. As regards the specification and implementation of hygiene-related measures, detailed information is not provided by the report (Pierce et al., 2020). Instead, reference is made to the existence of national guidelines for infection prevention and control which are said to be compatible with international standards.
In terms of support for the implementation of measures, LTCFs in Ireland were provided with checklists and tele-mentoring by the government. Moreover, some financial resources were freed for LTCFs to purchase equipment, as well as to conduct recruitment campaigns for new LTC personnel. Reporting for Ireland points to substantial deficits in testing capacity, making the aforementioned prioritization of testing in LTCFs difficult to realize. In summary, Irish adherence to ECDC guidelines, based on current evidence, points to a highly timely response by government in terms of the formulation of policy to address the pandemic in LTCFs (+++), a strong but not complete alignment with European recommendations in the content of measures (++), but relatively weak support for policy implementation, manifesting in poor access to testing for the target population (+).
Spain
The first COVID-19 related guidelines for the LTC sector were published in Spain on 5 March and soon elaborated on the 15th of the month. Meanwhile, the first legally binding guidelines were passed on 21 March, with amendments following on the 4 and 16 April. The national response, therefore, spanned a period of 2–44 days following the onset of the pandemic (Zalakaín and Davey, 2020). The large majority of ECDC recommendations can be found in Spanish policy. However, detailed information is at times missing in the country report (e.g. on proper usage of protective materials and monitoring). With regard to explicit departures from European guidelines, these mainly concern Spanish testing strategies: at the start of the pandemic, authorities only called for the testing of persons in cases where a suspected infection might lead to hospitalization. For symptomatic staff, testing was advised, however, only with referral by a primary care physician. In recommendations later passed, a 2-week quarantine for staff with contact to suspected cases was mandated. Moreover, priority was given for the testing in LTCFs. A clear testing strategy, however, is not detailed in the report (Zalakaín and Davey, 2020). Additional guidelines adopted in Spain pertain to the isolation of suspected cases, which was elaborated (21 March) to include contact persons. In a similar fashion, the usage of masks was only recommended and later required by law (on 21 March) in instances in which suspected cases were involved. However, here too detailed information on masks is missing in the country report (Zalakaín and Davey, 2020). An important departure in the Spanish response from EU policy concerned dealing with new or readmissions from hospital into LTCFs. At the start of the pandemic, positively tested patients could still be admitted to LTCFs if they were isolated and monitored.
As concerns national support for implementation, this mainly took the form of legally binding guidelines that were accompanied by control mechanisms to insure adherence. Moreover, health authorities were given authority to take over the management of affected LTCFs. The government also made financing available to facilities in order to facilitate the realization of measures. Still, problems concerning a shortage of protective materials, as well as the poor coordination of such resources (including tests) were reported. Crucially, the impact of the pandemic was amplified by ongoing deficits in the LTC sector in Spain, such as poor access to health services for residents, limited space, staff shortages, poor crisis management and so on. National measures taken at the time did little to compensate for these problems. Finally, it bears noting that systematic, national reporting of COVID-19 cases in LTCFs began only on 21 March, and only when more than one case was identified. Reporting for all LTCFs was only introduced on 4 April. With a view to this evidence, the Spanish national response can be described as highly timely (+++), but with loose adherence to ECDC guidelines specific to the usage of masks and testing and drastic differences concerning admissions or transfers from hospital (+). As concerns support for implementation, here governmental reliance on legal mandates and monitoring was strong. However, de facto implementation was hampered by shortages in supplies and ongoing deficits in the institutional landscape of the country’s LTC sector that could not be offset by government action at the time (+).
Sweden
The first governmental response to the COVID-19 pandemic specific to the LTC sector was issued on 1 April in Sweden. This entailed the occasional prohibition of visits to LTCFs. It was not until 7 May that additional measures would be introduced and subsequently elaborated on 25 June. Accordingly, the government initiated action 25 days after the onset of the pandemic, however, more sizable steps were taken only 61 and 110 days later (Szebehely, 2020). In terms of the content of measures, many ECDC guidelines were either not taken up by the Swedish government or otherwise went unreported. Up until 7 May, the main recommendation involved the strict application of hygiene rules in LTCFs, met occasionally by the aforementioned halt on visitations. Then, from May onward, Swedish guidelines began to differ substantially from those of the ECDC, particularly as concerned the use of masks; whereas, some support for the measure was mentioned by the Public Health Agency (PHA) report on 7 May, the decision to wear masks was still left to LTCFs in conjunction with regional infection control units. Instead, stress was placed on proper public hygiene. It was only on 25 June that PHA would recommend the use of shields or facemasks when caring for suspected and confirmed cases. Accordingly, the Swedish policy on wearing masks was considerably lagging with respect to ECDC guidelines which had been passed on 12 March.
With regard to testing, information for the Swedish case is largely missing (Szebehely, 2020). However, reference is made in the country report to the low prioritization of residents and staff in LTCFs. It is important to note that the national guidelines were largely held to be non-legally binding recommendations. Still, to facilitate their implementation, LTCFs were provided with guidance by regional administrative bodies. Meanwhile, of the factors cited as impediments to implementation, a shortage of protective materials and test capacities come to the fore. This was accompanied by problems related to the use of under-trained ‘casual workers’ in the LTC sector. Based on evidence reported for the Swedish case, the national policy response can be described as slow (timeliness+), largely non-adherent in terms of overlap with ECDC guidelines (+), and poor in its support of implementation (+). To evaluate the situation in the LTC sector, the Swedish Government initiated a commission which published a first report in December. The main conclusion of the report is that measures taken by the country during the first phase of the pandemic were both late and insufficient (Statens Offentliga Utredningar (SOU), 2020: 2).
Aggregation of data
Having established the relationship between the impact of COVID-19 on the general population and mortality outcomes specific to residents of LTCFs, as well as explored the nature of member state adherence to ECDC guidelines in six cases, we now bring our findings together to address how differences in national policy responses may have contributed to the mortality outcomes observed for Austria, Denmark, Germany, Ireland, Spain and Sweden. To do so, we begin by revisiting data in Figure 1. As can be derived from the graph, the first wave of the pandemic hits all six countries between mid-March and start of April. While some slight differences in the dates of peaks can be seen, by end of April, the number of incident cases (over a period of 14 days) decreases for all countries with the exception of Sweden. Larger differences can be observed concerning the level of incidence and the rapidity of increases. While Spain reaches its climax on 6 April at 218 cases and Ireland on 23 April with 213 cases (per population 100,000), all other countries present only half or less than half of these numbers: Austria reaches its climax on 2 April at 102 cases, Denmark on 12 April at 65 cases, Germany on 9 April at 86 cases and Sweden on 2 May at 84 cases. Sweden, notably, demonstrates a slow increase at the start of the wave, resulting in no decreases later in the wave.
As summarized in Table 3, the cumulative cases (per 100,000) and cumulative deaths (per 1,000,000) following 3 months after first 100 cases reflect substantial differences in the amount and rapidity of COVID-19’s spread during the first wave (Figure 1). With approximately 200 cumulative cases, Austria, Denmark, and Germany are far less impacted by the virus than Ireland, Spain and Sweden at the time (516, 511 and 432 cumulative cases per 100,000, respectively). For a closer understanding of these numbers, it is necessary also to compare the test rates and the test positive rates in these countries for the period of observation, as a higher number of cumulative cases can simply be the result of more testing done in one place versus another. A low number of tests and a high number of positive tests would suggest an underestimation of the number of cumulative cases. As illustrated in Table 3, the number of tests per 100,000 people 3 months after the pandemic outbreak (i.e. 100 cases reached) is comparable in Austria, Germany, Ireland and Spain. However, there were more than twice as many tests per 100,000 people in Denmark. The differences in the test positive rates suggest that the probability of an underestimation of cases in Ireland and Spain is higher than in the other countries. The cumulative deaths per 1,000,000 in the countries with a low number of cumulative cases per 100,000 are considerably lower as well. It bears noting, however, that while Ireland shows the highest number of cumulative cases, the number of cumulative deaths is lower than in Spain and Sweden (Table 3).
Comparison of select member states.
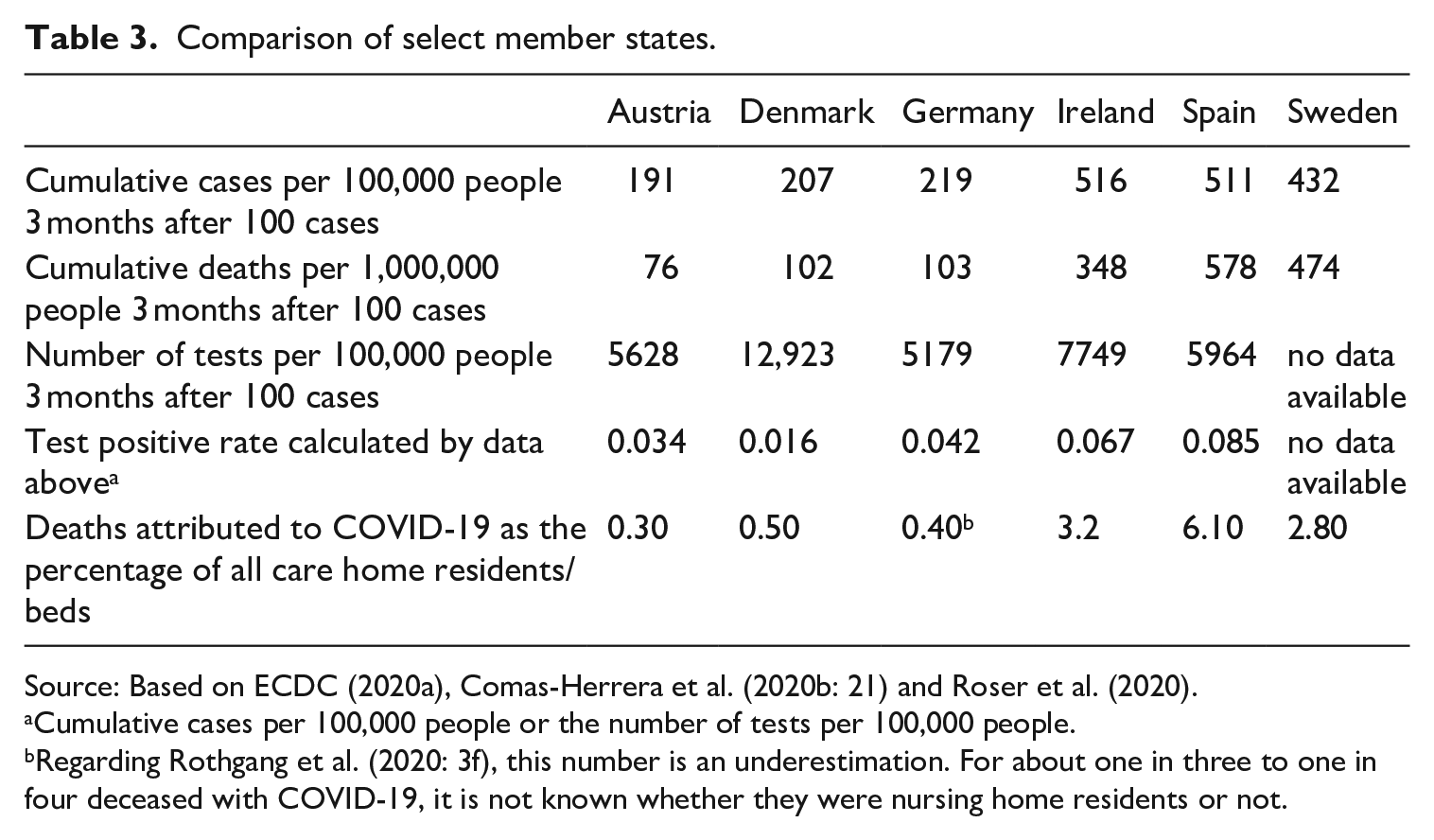
Source: Based on ECDC (2020a), Comas-Herrera et al. (2020b: 21) and Roser et al. (2020).
Cumulative cases per 100,000 people or the number of tests per 100,000 people.
Regarding Rothgang et al. (2020: 3f), this number is an underestimation. For about one in three to one in four deceased with COVID-19, it is not known whether they were nursing home residents or not.
Drawing on data from Comas-Herrera et al. (2020b 21) (see also Figure 2), Table 3 illustrates differences between countries specific to the resident mortality in LTCFs. 2 The data show that deaths attributed to COVID-19 as the percentage of all residents or beds differ between less than a half percentage to 6%. Austria, Denmark and Germany demonstrate far better outcomes in mortality than can be seen in Ireland, Spain and Sweden.
To better understand the role that policy measures may have played in affecting mortality outcomes among residents, we use the results of our regression analysis, that is, the regression equation to predict values and compare these with actual values. In other words, we prognosticate the mortality of residents in line with the significant correlation established between general impact (cumulative deaths per 1,000,000 without resident deaths) and residents who died with COVID-19 as the percentage of all residents (see chapter 4.1). The underlying assumption being, that where actual numbers of deaths are lower than predicted based on general impact of COVID-19 in the broader population, this can be attributed to the role of member state adherence to ECDC guidelines.
As can be seen in Table 4, the relationship between predicted and actual values for mortality vary strongly from member state to member state; whereas actual mortality as a share of predicted lies at around 50% for Austria, Denmark and Germany, in Ireland, Spain and Sweden the share ranges from 83% to 102%. In line with our assumption, if the relation between the predicted and actual values is indicative of the influence of policy measures undertaken by member states, then lower actual numbers reflect the efficacy of national responses. Accordingly, measures taken in Austria, Denmark and Germany appear to have been more effective than in Ireland, Spain and Sweden. This corresponds well with scores for member state adherence observed earlier for these countries (see Table 2); in countries where adherence is higher, the actual values are lower in relation to predicted numbers.
Comparison of actual and predicted mortality.
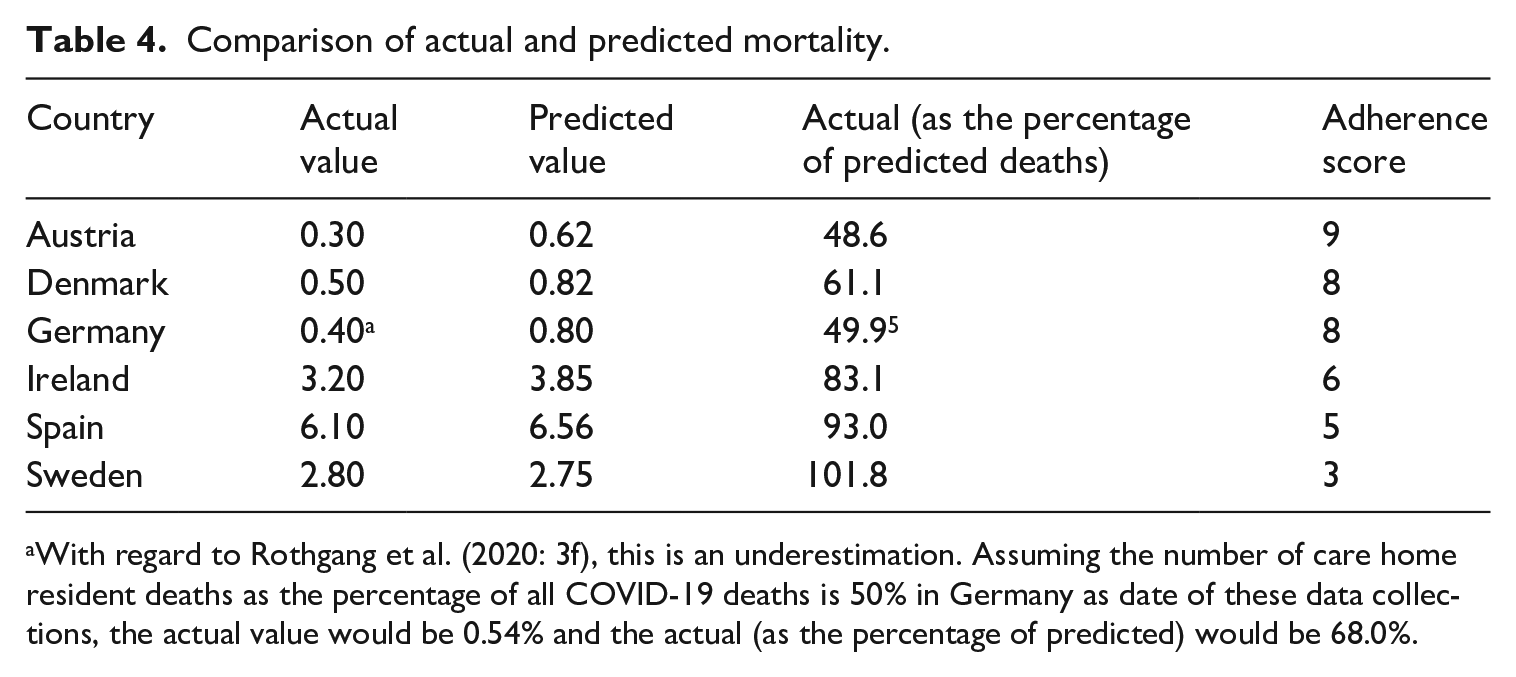
With regard to Rothgang et al. (2020: 3f), this is an underestimation. Assuming the number of care home resident deaths as the percentage of all COVID-19 deaths is 50% in Germany as date of these data collections, the actual value would be 0.54% and the actual (as the percentage of predicted) would be 68.0%.
Discussion
In attempting to describe and explain differences between countries in mortality outcomes for the institutionalized elderly seen in Europe during the first wave of the COVID-19 pandemic, we have encountered several important limitations that require closer attention here. First, pertaining to the quantitative analysis, in measuring the independent variable, general impact on the population (i.e. both cumulative cases and cumulative deaths), data used may paint a skewed picture of reality due to differences in testing and reporting strategies in place across member states. This may have contributed, for example, to an underestimation of cases for Ireland and Spain (see Table 3). Concerning Sweden, missing data make estimates of real cases even more difficult to ascertain. A better indicator of the pandemic’s impact is the number of deaths in a country. However, this too is problematic, depending on how well the virus is detected and reported as a cause of death. With respect to the dependent variable, mortality outcomes for residents in LTCFs, similar problems arise; as described by Comas-Herrera et al. (2020b: 3), reliable and comparable data is lacking for many countries. This can be seen, for instance, in the number of deaths reported for residents in Germany, which is at times estimated as a lower limit only.
As regards issues surrounding the qualitative analysis of member state adherence to ECDC guidelines, these mainly result from a possible under-reporting of national policy responses. That is, although in most instances, the content of country reports indicates strong overlap with European-level policy, detailed information on the actual measures put into place in countries, as well as the nature and gravity of problems faced in implementation are often missing. In some cases, we have been able to fill in the blanks based on information from other sources (e.g. in the case of supply shortages for protective gear in Germany). However, this has not been done in a systemic manner for all countries, and therefore, cannot serve as a strong basis upon which to build robust evidence. For this reason, the rating of member state responses in line with ECDC guidelines, as presented in Table 2, can serve as only a summary of tentative observations rather than a validated, comparative evaluation of measures to protect the institutionalized elderly. In terms of issues arising as a result of our sampling method, it bears noting that our selection of cases for this analysis, which proceeded in line with the dependent variable (residents who died with COVID-19 as a percentage of all residents), may have introduced a positive selection bias. That is, in only one of the six member states included (Sweden) was the actual value for mortality higher than the predicted. In comparison to the regression model (see Figure 3), we would expect a ratio of about 2:1, because there were 11 countries below versus six countries above the regression line.
One final issue bears mentioning when considering (potential) limitations affecting this study – namely, the definition used to identify the onset of the pandemic in a country. In adopting the 100 case threshold as the starting point, our work draws on earlier research by Hartfield and Alizon (2013), as well as Koh et al. (2020) which establishes the utility of the indicator in studying outbreaks of infectious diseases. Its use here, however, does raise a number of important concerns. For one thing, if taken to estimate the timeliness of national policy responses, the indicator does not take into account that some countries, by virtue of having been impacted later by the pandemic than others, have the benefit of learning from those around them. This may result in a timelier and effective policy response than seen in countries hit first. Moreover, as established by the present analysis of ECDC guidelines, these too have benefitted from the passing of time and the availability of more knowledge about the virus. Indeed, when comparing European recommendations, both past and present (as of 23 October 2020), with the current state-of-the-art on controlling the spread of COVID-19 in LTCFs, 3 it is apparent that earlier measures put forth by the EU fall short of extant evidence-based guidelines. This also means that member states hit later during the first wave also benefitted from improved policy guidance on behalf of the EU.
On account of the various limitations discussed here, the results of our analysis are not very robust. Still, they provide important insights into areas for further research. First, the analysis confirms that the share of resident deaths of all deaths is very high, evidencing the particular vulnerability of this societal group during the pandemic. Second, this study points to a positive correlation between the general impact and the share of resident deaths associated with COVID-19 as a percentage of all resident deaths; if cumulative deaths per 1,000,000 (not including resident deaths) increases by 100, the same share of COVID-19 related resident deaths as a percentage of all resident deaths tends to increase by 1.07 percentage points. The r-square for this model, which confirms earlier findings by Comas-Herrera et al. (2020a: 26f), is very high. Third, there is nevertheless some variance left. In order to explain this part of the variance, we analysed the specific measures taken to address COVID-19 in nursing homes.
As concerns our analysis of ECDC guidelines and member state adherence, several points are worth emphasizing: first, the EU was quick to formulate guidelines directed at the LTC sector, suggesting early problem recognition by policymakers. ECDC recommendations have evolved in their comprehensiveness and stringency over time, reflecting the severity of the situation on the ground and growing knowledge about the virus. Second, in terms of the responsiveness of national governments, here the timeliness, adherence and support for implementation varies across our six cases. Such differences in national responses to the pandemic may have important consequences for the mortality of the target population. Indeed, the amount of time transgressing between pandemic outbreak and policy adoption can shape the trajectory (level and speed of spread) of the virus in countries. However, as Langins et al. (2020: 81f) say, the formulation and adoption of guidelines are not the whole story, as much depends on the nature of implementation – that is, whether countries do a good job at translating guidelines into effective practices that are well implemented.
The successful implementation of evidence-based measures is likely to depend heavily upon circumstances characterizing the LTC sector in a country prior to the pandemic. By way of example, in a meta-analysis conducted by Stiller et al. (2016: 7), a correlation between room sharing in LTCFs and higher infection rates among residents was established. This is also evidenced in a Canadian study that pointed to the significance of crowding in driving-up infection rates: in LTCFs where residents shared a room, the risk of infection was twice as high, than for single room residents (Brown et al., 2021: E6). This may help to shed light on findings for the Spanish case, where mortality outcomes for residents were highest and where room sharing is the norm (Zalakaín and Davey, 2020: 10). Meanwhile in Sweden, LTCFs that relied more heavily on under-trained casual workers also experienced higher infection rates in the first wave than those using professional staff (Szebehely, 2020: 13). Such insights point to the need for policy measures that not only address improvements to the LTC sector in countries during periods of pandemic, but also well before. As concerns measures taken during acute crises, these may prove helpful, however, in attenuating the impact of the pandemic on the institutionalized elderly. Indeed, the present findings suggest as much: the more stringently the analysed countries applied EU guidelines, the lower the actual numbers of deaths among residents compared to predicted values (see Table 4). However, it bears repeating that the strength of these findings is highly constrained by the aforementioned data issues (e.g. resulting from different testing strategies).
Conclusion
The findings of this study provide important insight into better ways of protecting residents of LTCFs in future pandemics: first, the greatest protection that can be afforded to the institutionalized elderly lies in reducing the transmission of infectious disease in the general population. Second, the timely, close adherence to well implemented policies along the lines of the ECDC guidelines can help mitigate the impact on resident mortality. However, the efficacy of such measures is subject to the aforementioned spread of the virus in the broader society. This suggests that policies only targeting the LTC population are not sufficient, if viruses similar to COVID-19 are otherwise widespread throughout a country. This was especially evident during the first wave of the pandemic, when vaccinations and rapid tests were not yet available. Looking forward, the dramatic developments of this period stress the necessity for a two-pronged approach to policymaking during a pandemic involving a novel virus: first and foremost, one that addresses the risk of exposure in the general population and second, a set of measures specifically tailored to those most vulnerable – in this case, the frail elderly. Beyond this, our research sheds light on a number of deficiencies in extant international and national data-sources, pointing to the dire need for better methods of measurement and reporting within Europe. This requires the use of shared concepts and methods, as well as standardized approaches to testing and reporting on cases across member states. It is only by improving our access to reliable and comparable data that we can develop more effective, well-informed policies that allow us to be better equipped to dealing with future crises of this kind.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – Projektnummer 374666841 – SFB 1342.