
Abstract
COVID-19 and the corresponding economic lockdown and income loss for large segments of population was something unexpected for all European countries, and their welfare systems were not prepared to protect their citizens from such threats. Social resilience is becoming used in disaster risk analysis, and preferred to that of vulnerability, to refer the ability of the social entities to respond to such challenges, enabling them to cope and adjust to adverse events. It has been more recently used in the context of the European Union (EU) about COVID-19, regarding the creation of the Recovery and Resilience Facility, intended to mitigate the economic and social impact of the coronavirus pandemic. The global nature of this pandemic makes possible and relevant a deeper understanding of social resilience at different levels of analysis: international, national, local and individual/household levels. This article aims to contribute to this by proposing a set of indicators of social resilience in face of COVID-19, supported in a theoretical framework developed herein, and comparing the performance of a selection of EU countries with distinct welfare system configurations, with different roles played by the government, the market, the social organizations and the families. Using comparable statistical data at macro level and data concerning the responses of government to the economic and social effects of the pandemic, we produce a synthetic index of social resilience, combining resilience on coping and resilience on adapting. We relate the differences found in coping and adapting with the welfare system configurations of these countries.
Introduction
This article intends to analyse the differences in social resilience among European Union (EU) countries. For our analytical purpose, social resilience is the ability of individuals, households, civil society organizations and state institutions to cope with and adjust to the pandemic COVID-19 and the economic lockdown and job and income losses that it originated. This analysis, made for a selection of EU countries, uses a set of indicators that reflect our understanding of the concept of social resilience when applied to the research on this topic.
COVID-19 was, since March 2020, the largest global natural hazard in the last few decades. It placed all countries in face to their own resources to cope with it and with the economic and social effects that it originated: the persons had no escape, and the countries could hardly rely on international solidarity because the event was widely generalized. The concept of resilience applies to this event, involving four major levels. First, the individual and household ability to cope with the pandemic and the risk of economic lockdown and income reduction. Second, the requirement of strong civil society and social institutions to deal with the increased need of human support. Third, the need of strong state institutions to cope with the pandemic and income loss, requiring universal action. Fourth, the national/country and international relation dimension, given the rather inter-country competition and the need of international cooperative behaviour of the countries. At the national level, the countries’ welfare systems, mostly bismarkian, faced great challenges to respond to it, since welfare states were created to face social risks that originate income loss and not to face natural hazards of uncertain occurrence.
Unexpected as it was, the COVID-19 pandemic faced unprepared systems of health care and of social protection. This required a great effort of adaptation of state and private organizations to deal with the pandemic and, as well, to compensate for job and income loss originated by the imposed lockdown to control the pandemic. A global virus originated, however, different national responses, due to different medical interpretations of the required action and to different national health and social protection systems.
Social researchers faced the inability to get rapid and robust information to study this event but could count on a good response of some organizations. The information collected by Eurofound (2020a) was of great relevance for this purpose providing an updated knowledge on policy responses by national governments across Europe: the COVID-19 EU PolicyWatch. The same applies to the Oxford COVID-19 Government Response Tracker (OxCGRT; Hale et al., 2020a, 2020b). Until October 2020, around 700 policy measures were implemented at the member state level in the EU intended to support citizens and firms, evidencing different characteristics, widely described in Eurofound (2020a). At the individual and household level, Eurofound (2020b) launched an e-survey across EU countries, called Living, Working and COVID-19, in two rounds, the first in April 2020 (72% of the questionnaires) and the second in July 2020 (28% of the questionnaires), allowing to compare the situation when the lockdown was initiated with that when restrictive measures started to be relaxed. A total of 87,477 questionnaires were validated. 1
This article makes use of the concept of social resilience to analyse the policy responses of the EU member countries to this COVID-19 pandemic, supported in an approach made adequate to this natural hazard. Using the data provided by Eurofound, (2020a, 2020b) by OxCGRT (Hale et al., 2020a, 2020b), and other data from EUROSTAT and ECDC, a set of indicators is proposed with the aim of evidencing differences of social resilience between countries with different types of social protection systems. For this purpose, the following countries were selected: France (FR), Germany (DE), Italy (IT), The Netherlands (NL), Portugal (PT), Spain (ES) and Sweden (SE). These countries, that were differently affected and reacted differently to COVID-19, belong to different welfare systems models: bismarkian (FR, DE), universalist (SE), southern (ES, PT) and mixed in character: bismarkian/universalist (NL) and bismarkian/southern (IT). 2
The article is organized as follows. Section ‘The concept of social resilience in the context of COVID-19 pandemic’ presents the theoretical frame of the article, through visiting the concept of resilience and its discussion when used for the analysis of the COVID-19 pandemic in European countries. Section ‘COVID-19: distinct government strategies’ takes a preliminary look at the distinctive government strategies followed in the countries selected in face of this pandemic. Section ‘COVID-19, social risks and the welfare systems absorptive capacity’ looks at the (new) social risks in the context of COVID-19 and presents the main differences found between these countries’ social protection systems, relevant to their absorptive capacity in relation to the employment and income loss associated to COVID-19. Section ‘COVID-19: the adaptive measures’ makes a full description of the adaptive policy measures adopted by these countries, comparing these and relating such differences to their distinct welfare system type. In section ‘Social effects of the COVID-19 pandemic’, a set of variables is used to assess the different extent of social effects of COVID-19 pandemic in these countries, looking at several social domains. All this information supports the selection of a set of indicators for the construction of composite indices of social resilience, distinguishing its coping and adapting dimensions, enabling a comparative analysis of these countries, presented in section ‘A set of indicators of social resilience for COVID-19’. Section ‘Conclusive remarks’ concludes the article.
The concept of social resilience in the context of COVID-19 pandemic
In materials science, resilience of the material is defined as the amount of energy the material can absorb and still return to its original state. When transferred to the social sciences, this concept keeps its original meaning, but becomes more complex and involve several dimensions. Originally applied to the analysis of ecological systems, Holling (1973) considered that ‘resilience determines the persistence of relationships within a system and is a measure of the ability of these systems to absorb changes of state variables, driving variables, and parameters, and still persists’ (p. 17). Looking at social systems, Adger (2000) argues for their complexity and a lack of analogy of social resilience with ecological resilience. One of the specific characteristics of the social system is the role of institutions, in the broad sense of ‘modes of social behaviour’ and the ‘formal structures of governance or law’, considering that ‘the resilience of institutions is based on their historical evolution and their inclusivity or exclusivity, and hence how effective they are in oiling the wheels of society’ (Adger, 2000: 351).
The concept of social resilience has gained relevance in social sciences in recent years and can be viewed at two different levels: of the individuals in a society, and of the society as a social system. In social sciences, its content is enlarged and becomes more distant to its more strictly ecological meaning of ‘persistability’ (referring to coping capacities, that is, how people cope with immediate threats, with the restoration of the present level of well-being after the occurrence of such threat), rather embracing two other major dimensions: that of ‘adaptability’ (measures that people employ to learn from past experiences, anticipate future risks and adjust their livelihoods accordingly) and of ‘transformability’ (i.e. people to participate in decision-making processes, and to craft institutions that both improve their individual welfare and foster societal robustness towards future crises) (Keck and Sakdapolrak, 2013: 10–11).
Social resilience has been a concept recently used in disaster management, referring to the ability of the social system (a community) to recover, by means of its own resources, to natural hazards (Cutter et al., 2010). Resilience is then the ability of a social system to ensure that the system’s function persists through adaptation and learning, and so it should not be considered as an outcome but, instead, as a process (Doorn, 2015). Nevertheless, this concept has become more widely used to refer to the ability of persons and societies to cope with social insecurities, an issue of a greater political concern in Europe (Eurofound, 2018), challenging the economic measurement of social wellbeing after the publication of the Stiglitz Report (Stiglitz et al., 2009). In this sense, resilience is a broader concept than that of vulnerability, since enhancing resilience requires more than reducing vulnerability – it calls for empowerment and for fewer restrictions on the exercise of agency – the freedom to act. It also requires strong social and state institutions that can support people’s effort to cope with adverse events. (UNDP, 2014: 83)
Although the concept of vulnerability remains relevant in the analysis of this crisis, there is a need to adopt a broader analytical concept that also embraces the power and ability to adapt and react to it. 3
Resilience can be considered a characteristic of a society, which is viewed as a social system, composed of individuals, social relations and interactions among them, and institutions (rules and governance bodies). The above three characteristics of social resilience (persistability, adaptability and transformability) refer to distinct capacities of a resilient society to resist or to react to an external shock or an unforeseen disturbance, and to different degrees of change of the social system, distinct temporal scopes of reaction, with different outcomes (Keck and Sakdapolrak, 2013). The shocks may differ in its intensity and its persistence. In face of similar shocks, different social systems may evidence predominance of some of these capacities, either as an ex-post and short-term response, resisting to it and aiming at to restore the level of well-being before the shock (persistability, or absorptive capacity), or by reacting making small changes in the system, with a long-term temporal scope intending to secure the system of future well-being, a kind of ex-ante (preventive) response to future possible similar external shocks (adaptive capacity). But some societies may also evidence transformative capacities if the system enhance bigger or even radical changes, of transformative character (Manca et al., 2017).
There is a time dimension in the reaction of the social systems to external shocks, so that it is expected that the same society may evidence absorptive capacities as an immediate reaction to the external shock, adaptive capacity in the medium term and transformative capacities in the long-run, as in Figure 1, in the case of COVID-19 shock. The temporal character of resilience should be stressed, with relevance in this case. Shock-absorption is the most immediate reaction and reveals the readiness and the institutional and material availability to act. Adaptation means the short and medium-term readiness to change rules and behaviour, by accommodating them to the new situation. Resilient transformation is some more in-depth change in the society, supported in the previous efforts at immediate shock-absorption and the medium-term adaptation. In this article, analysing the period of the first COVID-19 wave shock, one cannot grasp this transformative dimension yet.
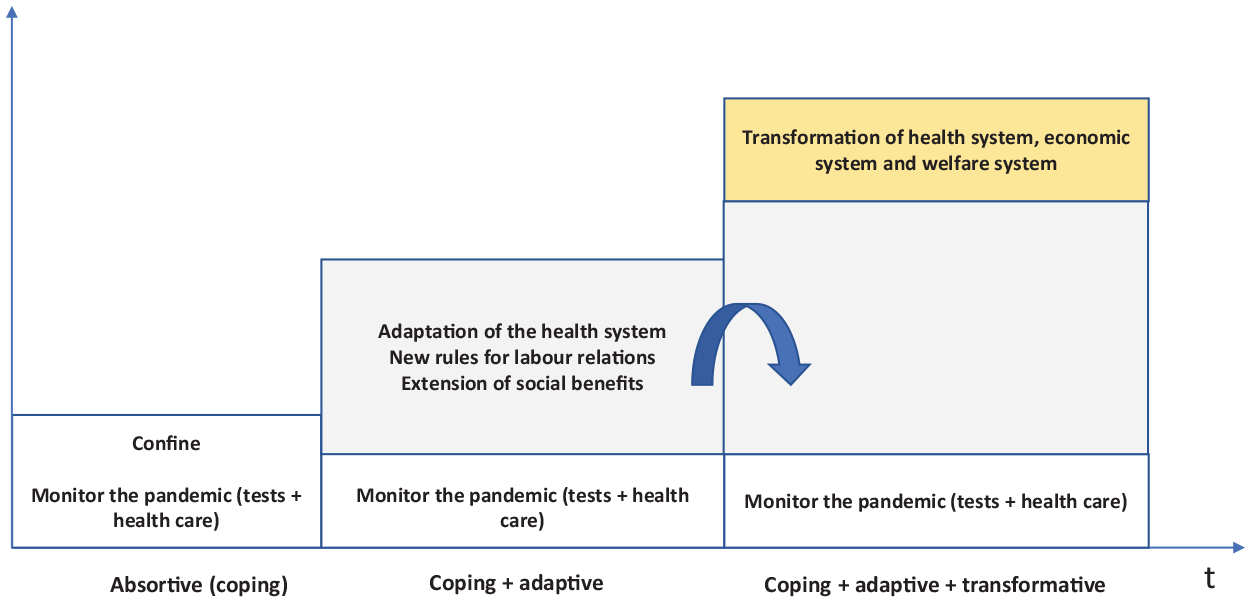
Capacities/stages of COVID-19 social resilience.
Figure 1 illustrates a typical time profile of a country on dealing with the pandemic COVID-19, as a national response to such a generalized virus. The short-term public response to the emergence of the first infected people with the new coronavirus was to make virus tests to locate waves of infection, to count the number of the infected people and their geographical location, to prepare the immediate response of the health system to attend these people, namely, those more serious, and to allocate the available health care resources to COVID-19 sick people. The private sector tried to respond to the rising demand by producing masks and antiseptic alcohol with gel, adapting the productive structure for this aim. After locating and counting the number of infection waves and infected people, some governments decided to confine population, imposing strict rules for public personal relations, intending to control the infection waves. In different ways, the countries tried to cope with the new pandemic, evidencing absorptive capacities in the very short run. It should be noted that these absorptive capacities depend on the initial conditions of the individuals and of the households, and on the capacity of the social protection systems to absorb the shocks. At this stage, these capacities were mainly evidenced by people, to whom was required unexpected sacrifices for survival. The decision for confinement has created serious problems for some sectors that ceased their economic activities (namely personal services, tourism, artistic activities, etc.).
The governments faced a serious trade-off to deal with the population health (and then to confine, at the expense of the economic activity) or to keep the economic activity (with negative effects on population health). To prioritize health goals required the adaptation of working hours, the implementation of teleworking and the introduction of changes in working relations (lay-off). New rules were adopted, intending the adaptation to the new situation of the country and the priority conferred to health objectives. The need to take care of the COVID-19 sick people required the adaptation of the health care system, enlarging the capacity of the hospitals for the expected new COVID-19 sick people. The economic lockdown of many firms led the governments to introduce short term measures related to the access of the affected population to social benefits and to take temporary measures to keep jobs unaffected as much as possible. All these kinds of measures reveal the adaptive capacities, either by government or by firms, in addition to the adaptive capacities by population, that extended the absorptive capacities revealed in the previous stage.
Although we are facing an international pandemic, this article is mainly focused on the nation-state responses to it, since it was the required immediate instance of reaction. However, in the EU, the serious economic effects of the pandemic originated great political pressure for the EU institutions to provide financial support to the economies that became fragile after several months of economic lockdown. As a matter of fact, the suspension of compliance with the budgetary rules of the Stability and Growth Pact and the massive fiscal solidarity that occurred in the EU are evidence of resilience at the international level in this case. The application to approved funds require the preparation and approval of the Plan of Economic Recovery and Resilience. Transformative capacities are then required, now at the nation-state level, to prepare the national economies to face the consequences of this pandemic.
The EU countries that followed the above policy sequence have, however, implemented different policy responses, originating or revealing different levels or kinds of the above resilient capacities. These differences will be explored in the next sections, identifying, when appropriate, possible relations with the welfare system characteristics of these countries. On the other hand, the social risks that emerge from COVID-19 and the abilities of these countries to face them will be scrutinized considering relevant characteristics of their welfare systems.
COVID-19: distinct government strategies
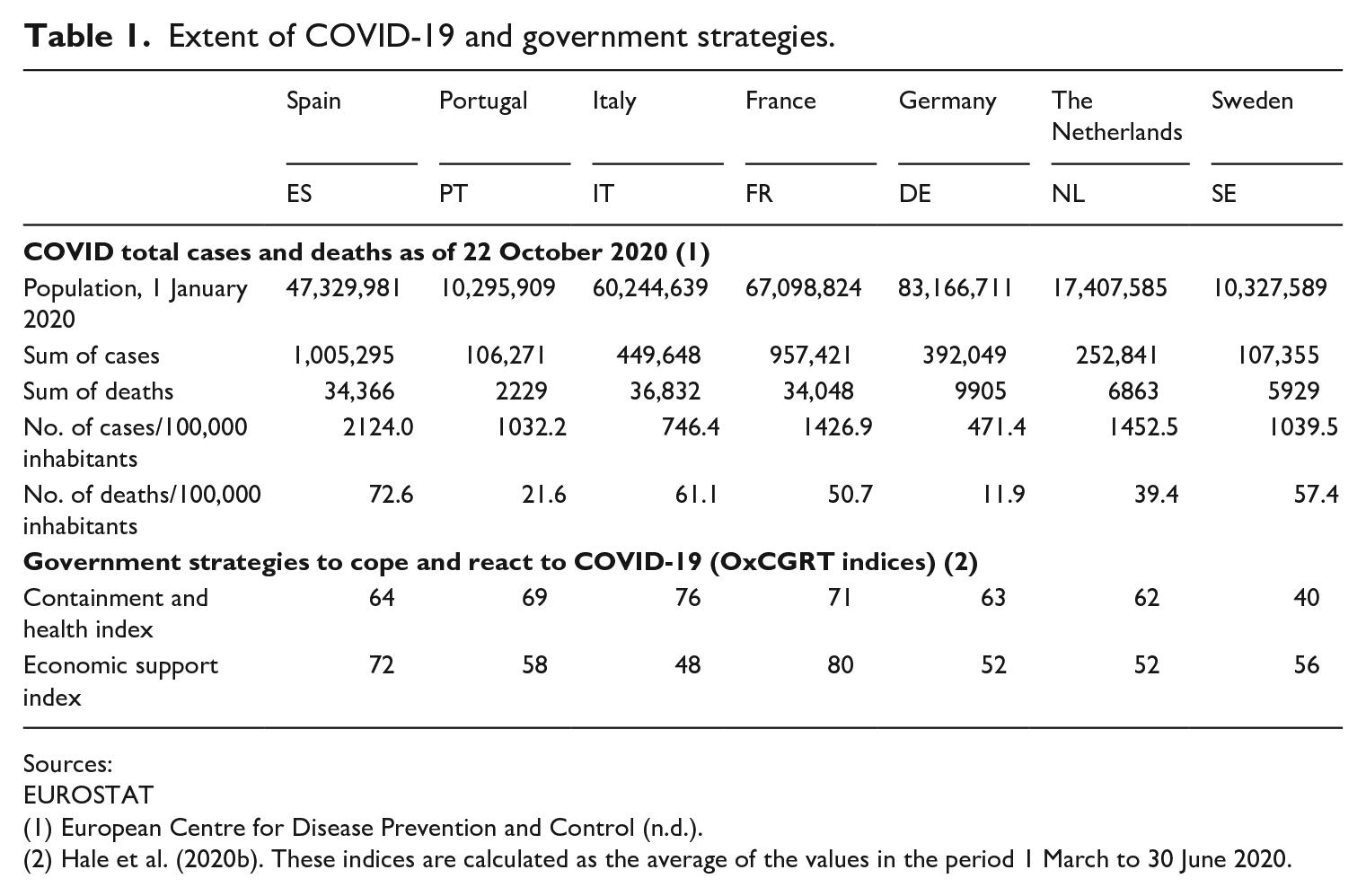
Table 1 provides a preliminary picture of the extent of COVID-19 related cases and deaths in these countries, evidencing blatant differences between them, notwithstanding this is often considered a democratic virus, since it may infect equally everyone.
Extent of COVID-19 and government strategies.
Sources:
EUROSTAT
(2) Hale et al. (2020b). These indices are calculated as the average of the values in the period 1 March to 30 June 2020.
The differences observed in COVID-19 incidence and in COVID-19 mortality rates between these countries may be attributed to the combined effect of several factors: economic factors (that explain different health risks related to different productive structures and job skills, with different exposures to virus risk), cultural factors (with different social rules of human conviviality), different levels of economic and social development (living conditions, poverty levels, income inequality), different regimes of welfare state (which provide different extents of social protection to such health risks and its social effects) and, obviously, the different strategies followed by these countries to cope with the pandemic and to react to its effects in the society. Among these consequences are those of economic origin due to economic lockdown with effects on employment and labour income.
The OxCGRT tracks governments’ policies and interventions using a series of indicators intending to measure the extent of policy responses to the COVID-19 pandemic, and the inter-country variations (Hale et al., 2020a, 2020b). Such indicators are grouped into four policy indices: (a) containment and health index; (b) economic support index; (c) stringency index; and (d) overall government response index (which aggregates the other three). Figure 2 compares these countries considering these four indices, calculated as national averages in the period since 1 March to 30 June 2020, but the containment and health index and economic support index are of great relevance, since the economic support provided to the population affected by this pandemic was a great concern of public policy in this COVID-19 pandemic time and originated different government strategies in these countries (Table 1).
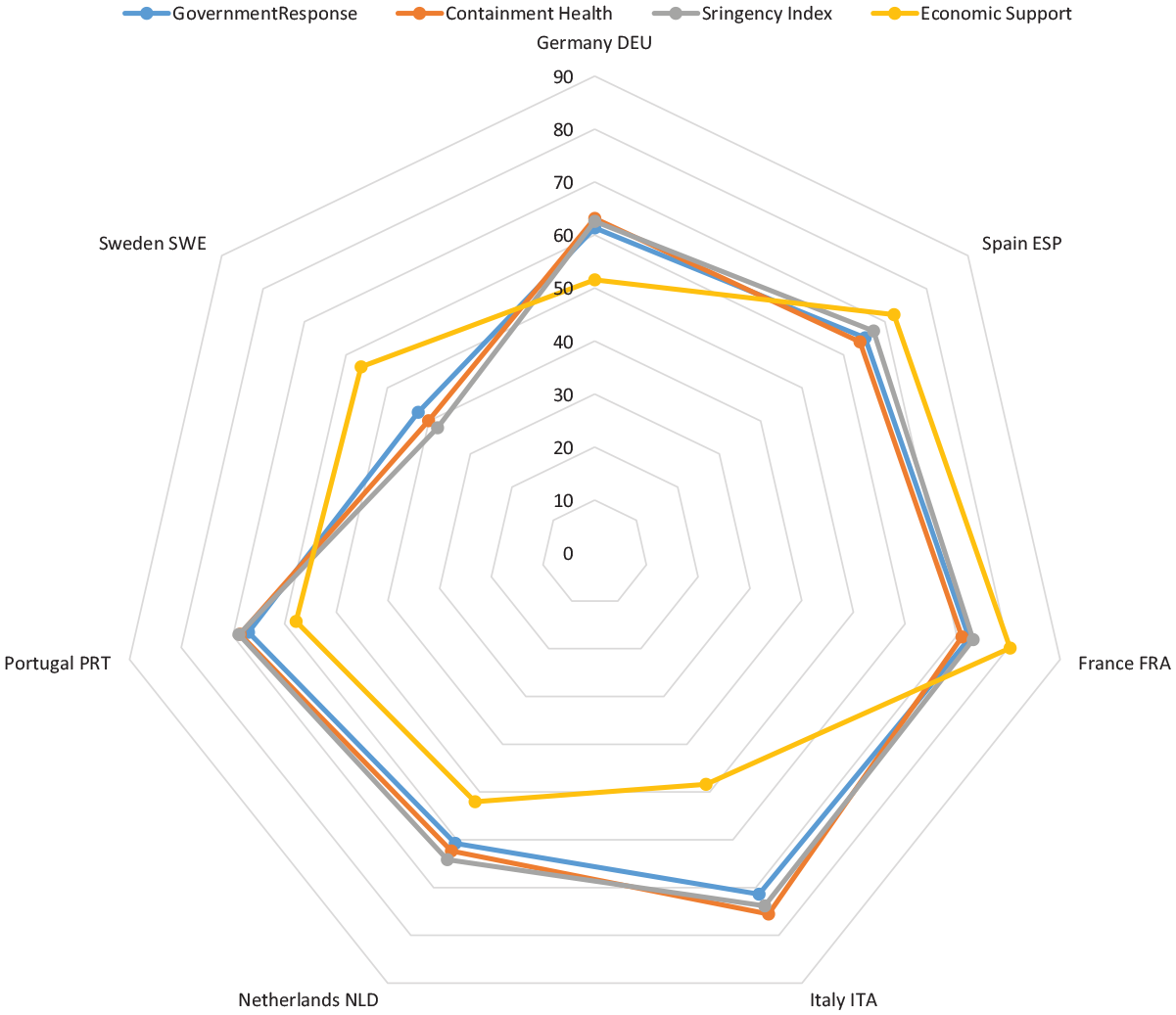
Health strategies to COVID-19.
The containment and health index aggregates variables like school closing, workplace closing, cancel public events, restrictions on gatherings, close public transport, stay at home requirements, restrictions on internal movement and international travel controls, and public information campaigns, testing COVID, contact tracing and facial coverings. The economic support index includes two variables: income support (it records if the government is covering the salaries or is providing direct cash payments, universal basic income or similar, of people who lose their jobs or cannot work, includes payments to firms if explicitly linked to payroll/ salaries) and debt/contract relief for households (it records if government is freezing financial obligations, for example, stopping loan repayments and preventing services like water from stopping or banning evictions). The timeline patterns for each of these countries, for the period since 1 March to 30 June 2020, are shown in Figure 3.
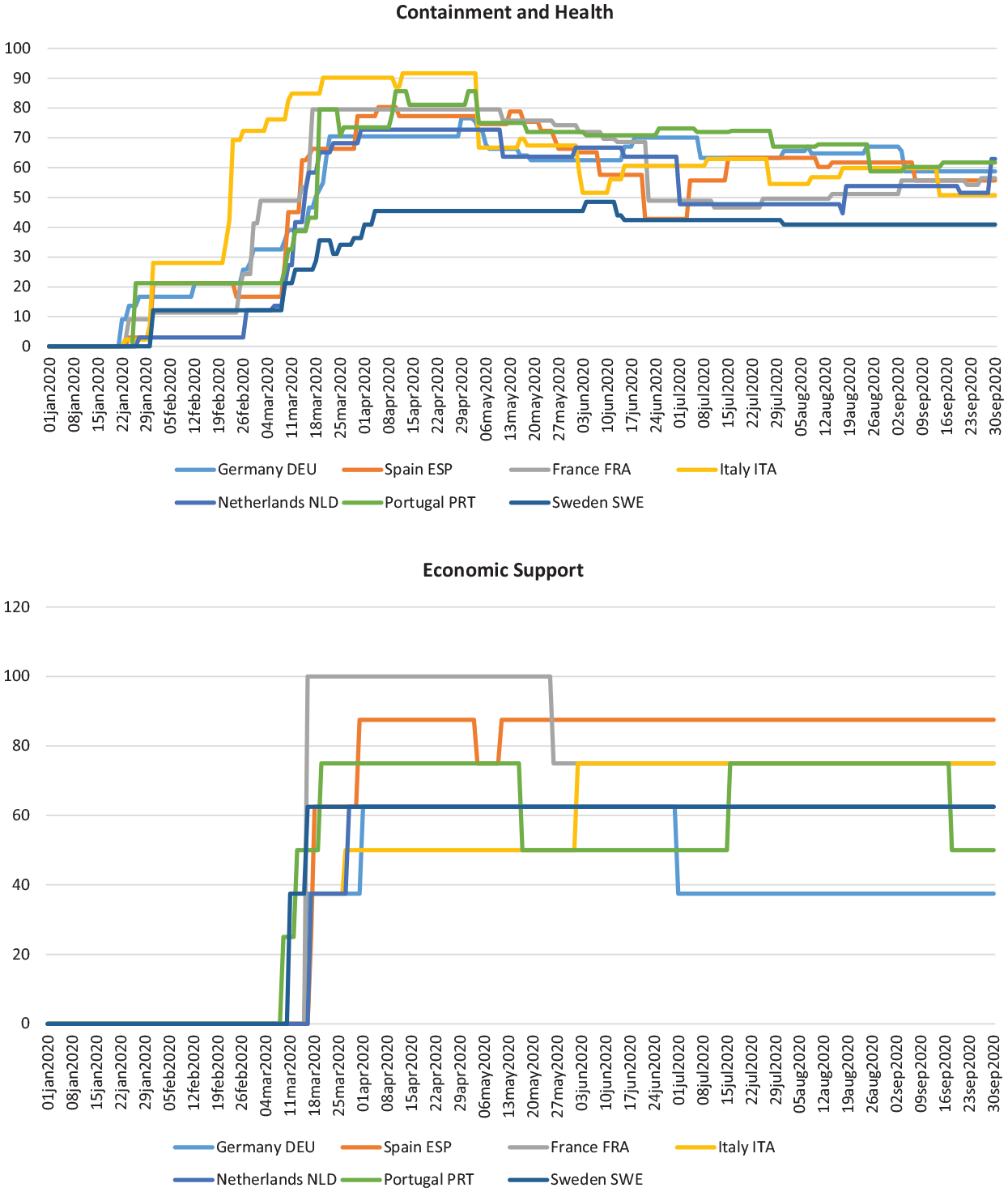
Timeline of health and economic support policy measures.
These indices display differences in COVID-19 strategies between these countries regarding the role attributed to health and economic support of the population. There are differences between countries on containment and health (Italy as the highest, Sweden as the lowest and the other countries in the middle) and, as well, on economic support (France and Spain as the highest, and the Netherlands, Germany and Italy as the lowest). If we look at both (health control and economic support), Italy and Sweden look as opposite: Italy is the country that favoured health control, while Sweden privileged economic support (Table 1 and Figure 2). The time pattern for such indices also reflects such differences between these two groups of public policies (Figure 3). The time of initiation of containment and health policies are not the same for all these countries, as are the economic support measures, initiated later in all of them and evidencing rather distinctive patterns among themselves. The contrast of the containment and health policies in Sweden and Italy again are evident in Figure 3.
COVID-19, social risks and the welfare systems absorptive capacity
Anticipating the 16th edition of the annual World Economic Forum’s Global Risk Report, the insight report World Economic Forum (2020) produced very relevant material for thinking on the social risks which can be originated by COVID-19. Supported on a COVID-19 risks perception survey addressed to 350 senior risk professionals, it provides an important insight into the analysis of the adequacy of the concept of social resilience to assess the scope of differences among countries on their ability to cope and react to the COVID-19 pandemic and their effects.
One decade after the 2007–2009 Great Recession, the COVID-19 pandemic originated the Great Lockdown followed by a prolonged global recession. The economic risks are on the top of the worries, namely the risks of bankruptcies and failure of firms to recover, originating massive structural unemployment and rising demands for the welfare systems to protect jobs and containing income falls, thus generating rising government budget deficits and rising debt ratios (World Economic Forum, 2020). Two other concerns are mentioned in the report, which are relevant as additional risks for sustainable growth: on one hand, the risk of shortfall of investment in climate action and, on the other hand, the rising cybernetic risks due to a higher dependence on digital technologies. But the risks in the social dimensions are of great concern too. And these are important challenges to the welfare systems of these societies.
The COVID-19 pandemic originated a great dilemma both for the individuals and for the families and the policy makers. Working individuals had to choose between staying at home to protect themselves and their families from virus contamination or, instead, to go to work to protect the job and family income. But this dilemma emerged only for some families, while others had no choice. Some working individuals had to stay at home because their economic activity had stopped and the firm lockdown, while others had to go to work, in risk of virus contamination: the essential workers (doctors and nurses, transportation workers, etc.). This dilemma, work versus health, originated some changes in working conditions for some workers (telework, adaptation of working hours), but also generated new inequalities in our societies, which are different from those existing before, the classical inequalities.
But policy makers also faced a dilemma considering two conflicting policy objectives: to take measures of confinement to protect the citizens’ health, controlling the virus dissemination and then the stress on the national health systems or, instead, leave economy to work, reducing job losses and income declines, with higher risks of virus dissemination in the society and higher demands for the national health systems. Different countries had followed different strategies, but some sectors escaped from such dilemma, since some sectors had to remain working (health care, education), while others could not escape to the lockdown: arts, entertainment and recreational activities; tourism-related activities; accommodation and food service (restaurants) activities; non-essential retail sectors; and so on. The social risks present in such dilemmas are mostly located in two areas of public policy, which became crucial in this context: labour market and health care. It is in these two areas that are located some of the most serious social risks originated in the COVID-19 pandemic identified by COVID-19 risks perception survey respondents.
One of those risks is the rise of inequalities and the emergence of new forms and sources of inequality (World Economic Forum, 2020). Some extents of such inequalities are those referred above, about the dilemmas work versus health. But others were originated by solutions found to solve these dilemmas. One way of reconciling economic activity with health control consisted of adopting remote work, teleworking and adjusting the working hours, for those sectors and occupations that could do it. Gender inequalities may arise or become deeper with this solution, because those occupations that require physical presence of the worker or with less flexibility in working hours become excluded from the advantages of such solutions, and female work is predominant in some of these. The higher use of digital technologies may also, in this context, rise the gap between high-skilled and less-skilled workers. Also, the risk of rising intergenerational inequalities that this pandemic crisis generates, given the educational and employment challenges faced by the youth also highlighted in the report, originating the labelling of the present youth as the ‘Generation Great Lockdown’ (World Economic Forum, 2020: 36).
Another area of concern is the risk of worsening the quality of the social rights. The rise of the deficit of the government budget that pandemic originates is a constraint for reinforcing social protection by adjusting it to the new social needs. This includes income transfers (like public transfer for lay-off decided to prevent unemployment, the adjustment of the eligibility rules for unemployment allowances or mechanisms of guarantee of minimum income). But it also includes public services, like the need of reinforcement of the health care systems, not deteriorating the other medical services beyond COVID-19, namely, those that may originate additional demand, like mental health.
Finally, the report highlights risks and concerns related to other domains of human, civil and political rights, that are affected by COVID-19 pandemic. The decision of confinement by national authorities limits the freedom of movements, the access to services and the functioning of social relations. The unclear rules for health regulation, the competitive behaviour of institutions in the international relations and the evolution of the figures on COVID-19 contamination tends to reduce the trust on authorities, the government and the EU institutions.
Welfare systems are then facing, in case of COVID-19, new social risks. This pandemic, an unexpected and uncertain natural chock, originated great demand in three substantial domains: on health care (it was originated in a coronavirus highly and quickly disseminated all over the world), on the economy (the great depression caused by the lockdown) and on human and social rights (on freedom and trust on institutions, on inequality and on the quality of human and social rights). To face it requires a coordination of economic policy, health policy and adequate social protection.
The welfare states have proved to have adaptive capacities in face of unexpected shocks (Hemerijck, 2013: 1–22). The emergence, in early 2000s, of the so-called New Social Risks (NSR) school of social policy analysis, is the academic response to the need of the welfare states to adapt to the economic and social changes in the societies, that changed the supportive basis of the construction of such welfare states as happened after the II World War. Such new risks, that characterize the transition of modern societies to a post-industrial model, have been associated to some major dimensions of changes: deindustrialization, the rising participation of women in labour market, population ageing, the technological progress that has tightened the link of education and employment, flexibilization of the labour markets and the expansion of the private services (Taylor-Gooby, 2004). These changes originated new forms of vulnerability, new vulnerable groups in our societies and thus demanded new forms of dealing with them. Some of these vulnerabilities are present in the context of COVID-19. But others are new, as was evident from the above sections, regarding the social effects of an unexpected pandemic of an uncertain occurrence. Policy makers are called to new forms of governance in conditions of economic uncertainty (Crouch and Keune, 2012). The experience of social policy governance in the months that followed March 2020 is as example of how the different countries (as in Figure 2) reacted, at the national level, to this global/universal health crisis, how prepared they were, or not, to deal with them and how differently they reacted to face such new needs.
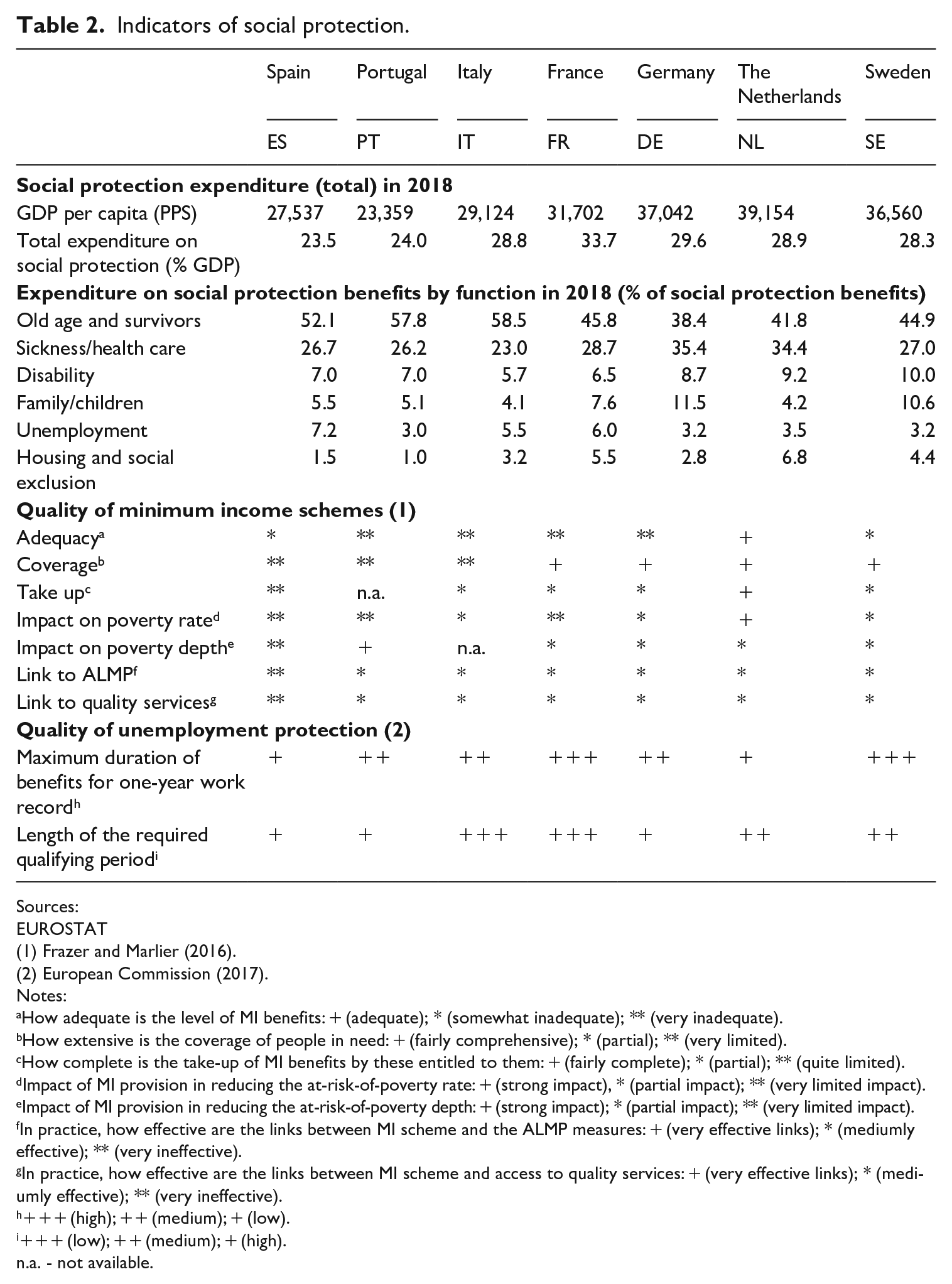
All these countries faced the same external natural shock, but their initial conditions were different in many aspects. Their national responses reflect, to some (or great) extent, the specific characteristics of their welfare systems. Some are evident in Table 2, altough it is a rough and rather incomplete picture of the national differences. Apart from the fact that all have public pension systems, although with different characteristics, and a large share of expenditure on old age and survivors, national health systems and a large share of expenditure on sickness/healthcare and disability, and social protection in unemployment, differences are evident in other social funcions. In social protection of the family and children there is a higher share in Germany and Sweden and a lower share in the Netherlands and Italy, in housing and social exclusion there is a bigger share in France and the Netherlands, a lower share in southern countries (mainly Spain and in Portugal).
Indicators of social protection.
Sources:
EUROSTAT
Notes:
How adequate is the level of MI benefits: + (adequate); * (somewhat inadequate); ** (very inadequate).
How extensive is the coverage of people in need: + (fairly comprehensive); * (partial); ** (very limited).
How complete is the take-up of MI benefits by these entitled to them: + (fairly complete); * (partial); ** (quite limited).
Impact of MI provision in reducing the at-risk-of-poverty rate: + (strong impact), * (partial impact); ** (very limited impact).
Impact of MI provision in reducing the at-risk-of-poverty depth: + (strong impact); * (partial impact); ** (very limited impact).
In practice, how effective are the links between MI scheme and the ALMP measures: + (very effective links); * (mediumly effective); ** (very ineffective).
In practice, how effective are the links between MI scheme and access to quality services: + (very effective links); * (mediumly effective); ** (very ineffective).
+++ (high); ++ (medium); + (low).
+++ (low); ++ (medium); + (high).n.a. - not available.
Two areas of social policy are of great relevance to assess the ability of these countries to cope with unemployment and income loss as they resulted from the COVID-19: the unemployment protection measures and the minimum income schemes (Table 2). Looking at the quality of the unemployment protection, the lower qualifying period in the welfare systems in Italy and France, and also in Sweden and the Netherlands, contrasts with those longer in the southern countries (Portugal and Spain), meaning a lower ability of the southern countries to cope with unemployment in case of temporary jobs. The maximum duration of benefits for 1-year work record, which is larger in Sweden and France, enables to keep living standars of unemployed for longer in these countries (European Commission, 2017). Looking now at the quality of the minimum income schemes in these countries, they are not equally prepared to face such a crisis. The coverage of such schemes is lower in the southern European countries, and the adequacy and impact on poverty rate are higher in the Netherlands. From what is said, one may say that these countries have welfare systems that are not equally equipped to cope with COVID-19: the southern european countries are in disadvantage in comparison with the bismarkian or the universalistic welfare systems. The latter are those more prepared to cope with it.
COVID-19: the adaptive measures
The social consequences of COVID-19 pandemic, along with the working of the mechanisms of social protection already in place to absorve the first impacts of this health crisis, originated the need to adopt specific measures. The differences among these countries regarding the number of policy measures and its nature, depend on the extent of the economic and social effects of this health crisis and on the ability of the existing social protection systems to cope with them without changes. The gaps found in the ability to cope with the crisis required the decision on measures of adaptation of the welfare systems.
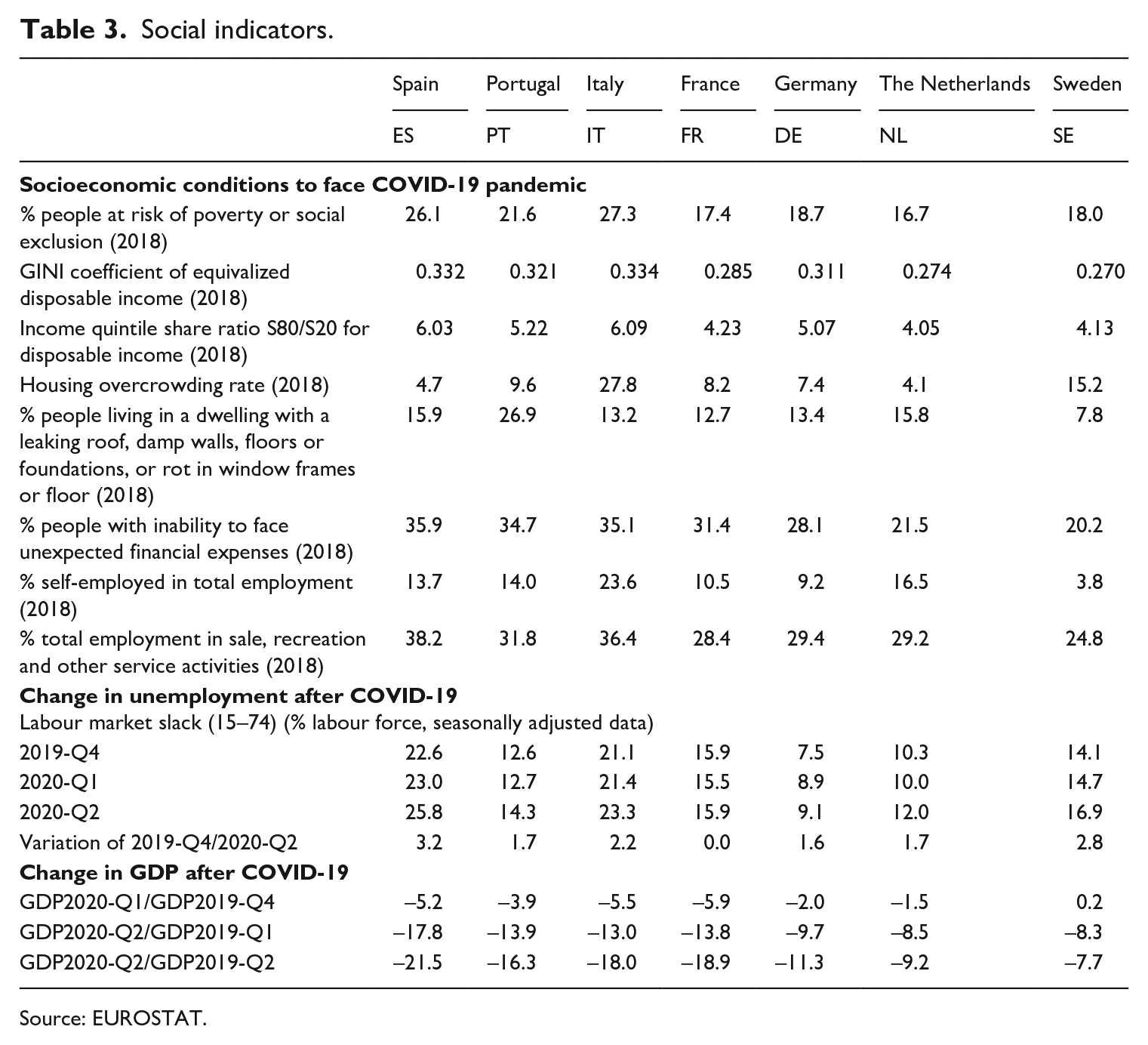
We now turn to the variables that may provide a picture of intercountry differences regarding the effects of the pandemic in several social dimensions of the population of these countries. Table 3 initiates this analysis, comparing the different exposures of the population to the risk of virus contamination. Although described as national means, there are differences among countries regarding the exposure to the risk of infection and to the negative economic effects of the health measures, either due to the characteristics of the productive structure and the related dominant organization of work, or due to the dominant forms of social behaviour in the societies. The higher poverty rate in the southern european countries, higher income inequality and worse housing conditions allow to understand why in the southern european countries the households face less capacity to cope with a pandemic and also higher risks of exposure to it. It is in these countries that a higher percentage of households (around 35%) are not able to face unexpected expenses. The productive strucure of the southern european countries also may explain the higher risk of virus dissemination, also facing higher negative effects of the lockdown: the higher percentage of employment in services with great exposure of workers with people (sale, tourism), what justified the need of locking down firms in these activities.
Social indicators.
Source: EUROSTAT.
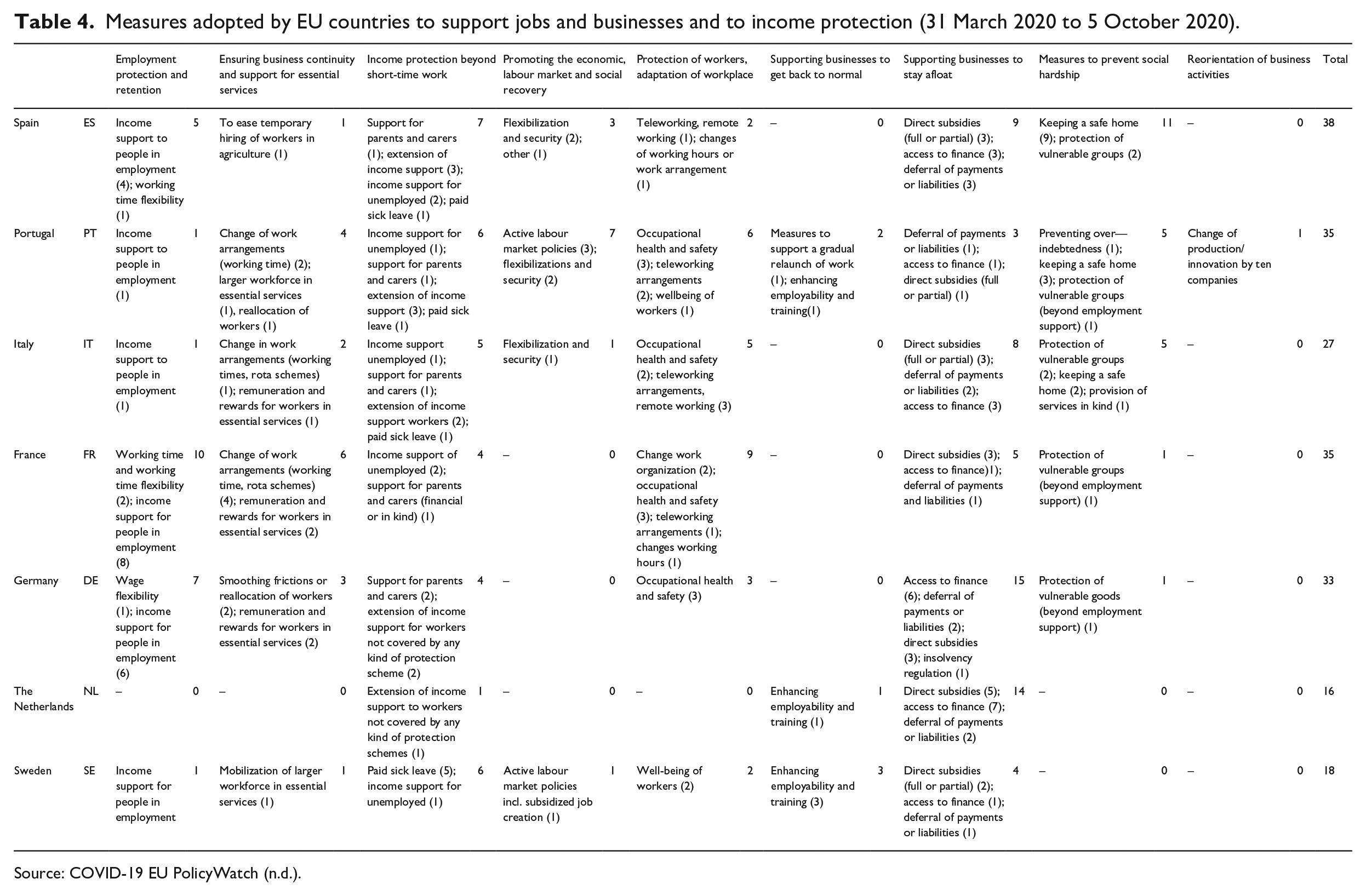
It is then important to investigate the nature of the measures adopted by the national governments to mitigate the social consequences of such health and economic and social crisis, through adaptive actions of the welfare system in these countries. Table 4 describes the set of policy measures (grouped into nine distint categories) decided and implemented in these seven countries in the period since 31 March to 5 October 2020, a total of 702 in all 27 EU countries, identified in COVID-19 EU PolicyWatch database.
Measures adopted by EU countries to support jobs and businesses and to income protection (31 March 2020 to 5 October 2020).
Source: COVID-19 EU PolicyWatch (n.d.).
The high number of measures adopted in such a short time (26 measures per country, on average) is an indicator of the urgency and gravity of the health crisis and its effect on the economic activity and social welfare and, as well, of the unpreparation of the countries’ welfare systems to react. Apparently some countries evidence higher absortive capacity, were better prepared to cope with the pandemic crisis, since the number of measures implemented is quite below the average: it is the case of Sweden (18) and the Netherlands (16). The negative impact on GDP was the lowest in these countries (Table 3). But such differences are more evident when looking at the nature of the measures adopted.
The more urgent, short-term, measures adopted were those intended to prevent social hardship, including those measures to protect vulnerable groups more severely afected (beyond employment support), to keep a safe home and to provide services in kind and to prevent overindebtedness. The southern countries (Spain, Portugal and also Italy) were those countries that adopted more policy measures of this nature. The universalist countries (Sweden and the Netherlands, of mixed character) have not adopted any policy measure of this character. As mentioned above, these countries allocate a bigger share of social expenditure to social exclusion/safety net measures and, as well, to housing, what may explain that they were better prepared to face the social consequences of this pandemic. Altough with a less pronounced pattern, the same argument applies to the measures of income protection beyond short-time work, with higher relevance for southern countries (Portugal, Spain and Italy), which include measures like income support for unemployed, extension of income support for workers not covered by any social protection scheme and income support for parents and carers. The welfare systems of these countries have better unemployment protection policies and, as well, better minimum income schemes, as said above. The southern countries are less prepared to face such needs, what required policy measures for adaptation of their welfare systems.
Another distinctive pattern that distinguish the southern and the universalist countries is the role of the policy measures to promote the economic, labour market and social recovery: for the whole seven countries analysed, 83% of such measures were adopted in the southern countries (Spain and Portugal). This set of policies include measures such as the prohibition of dismissals and tripartite agreements intending special unemployment protection and to promote economic and social recovery. The lower relevance of active labour market measures and unemployment protection in these countries, when compared to the universalist countries, in addition to the differences on their labour markets and productive structures, may explain why these countries are less prepared to face such a crisis. It is remarkable that Portugal, a southern country, is the only one that supported 10 firms to make a reorientation of business activities to change production of plastics into goggles for protection, which were missing in the market.
The policy measures intended the adaptation of the work place, changing work organization, such as teleworking arrangements and the promotion of remote working and changing working hours, and as well policy measures on occupational health and safety, are less related to differences on their welfare systems. These are specific measures addressed to the specific characteristics of this crisis, of pandemic nature, so that it is not surprising that does not exist an evident pattern related to distint welfare regimes. The same argument applies to the measures of business continuity and support for esssential services, that involves change in work arrangement and rewards for workers in essential services. But in some countries (the Netherlands, Germany, France, Italy, Spain) the policy measures for supporting businesses to stay afloat and for employment protection and retention were more significant.
Social effects of the COVID-19 pandemic
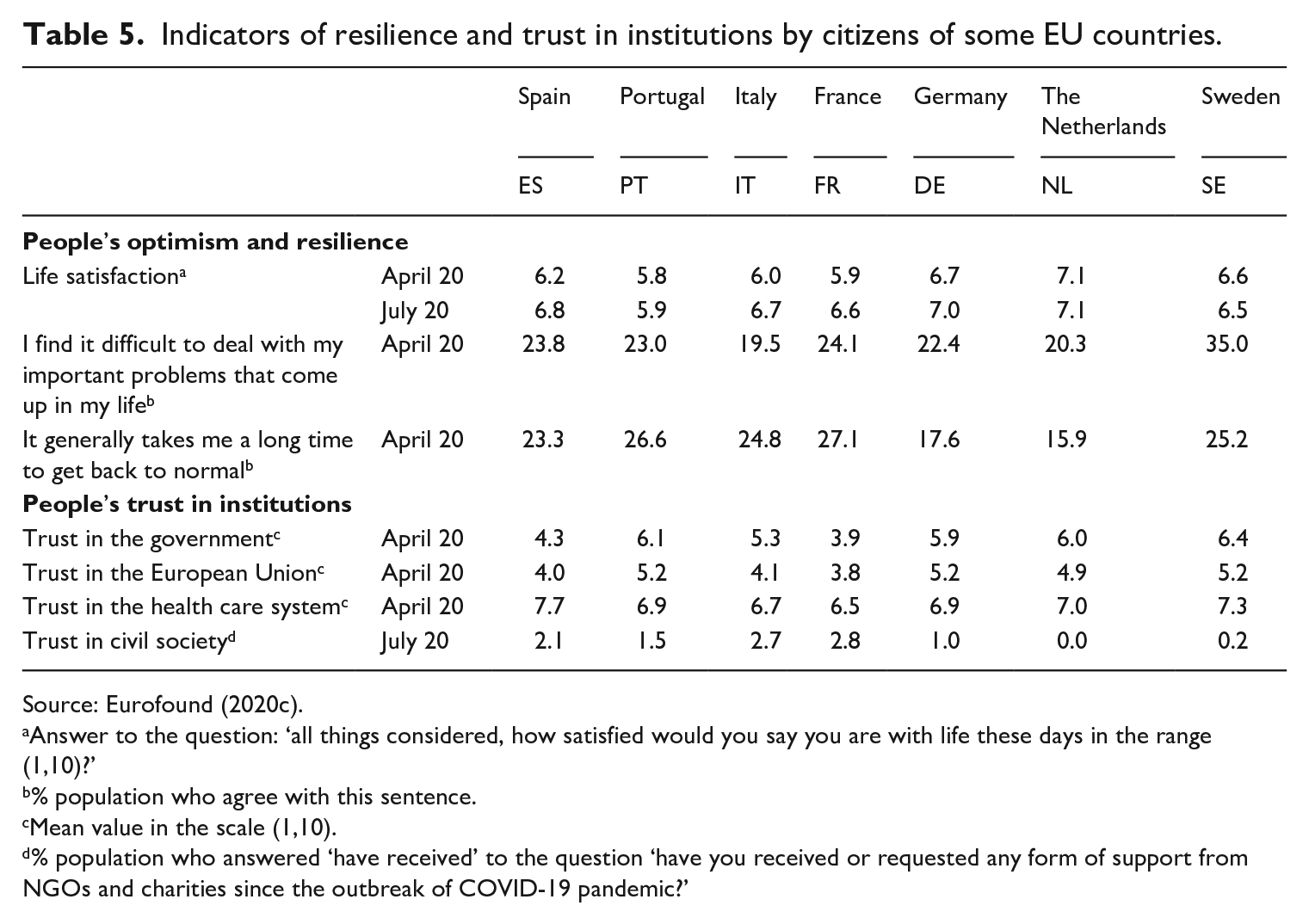
Table 5 gather some indicators of individuals/households’ ability to cope with (absorb and react to) the negative consequences of this pandemic in their countries. It provides a preliminary picture, at the individuals/households’ level, of the resilience of these countries, in two different dimensions. First, the personal optimism and resilience in face of a problem in general, including the mean life satisfaction in the peak of the pandemic (April 2020) and when most countries had already initiated deconfinement (July 2020). Second, the feeling of trust in institutions, that is the confidence that population has on the ability of these institutions (the national government, EU, the national health care system and the national civil society) to deal with this crisis.
Indicators of resilience and trust in institutions by citizens of some EU countries.
Source: Eurofound (2020c).
Answer to the question: ‘all things considered, how satisfied would you say you are with life these days in the range (1,10)?’
% population who agree with this sentence.
Mean value in the scale (1,10).
% population who answered ‘have received’ to the question ‘have you received or requested any form of support from NGOs and charities since the outbreak of COVID-19 pandemic?’
There are no major differences among countries regarding the life satisfaction, 4 but some light differences emerge when we compare the improvements in life satisfaction in the period April/July among countries. It is important to remark that all countries’ population improved their feelings of life satisfaction, except for the Netherlands and Sweden (that remained unchanged), those countries that confined less in this period. It was mainly in Spain, Italy and France that the improvement in life satisfaction was larger, those countries that faced the most problematic figures on the pandemic evolution.
The trust in the institutions and in the society are relevant variables that account for the different feelings that population has on the ability of such institutions to cope with the pandemic and to react to it, that is, of their resilience. There is higher confidence in the health care system in all countries, than that in the government (it is the lowest in Spain) and in the EU (it is the lowest in Spain and France). The indirect indicator of trust in civil society reveals to a great extent the population feelings on the availability of society to provide help in case of need. In the Netherlands and in Sweden such feeling is null, and in the Latin countries it is higher. 5
The trust on health care should be compared to the feelings of fairness of health policy measures in Table 6. The feeling that some needed medical care examinations were not provided was high in Portugal, evidencing the stress effect on the health care system, leaving some non-COVID sick people without medical care.
Indicators of health risks and fairness of health policy measures in some EU countries.
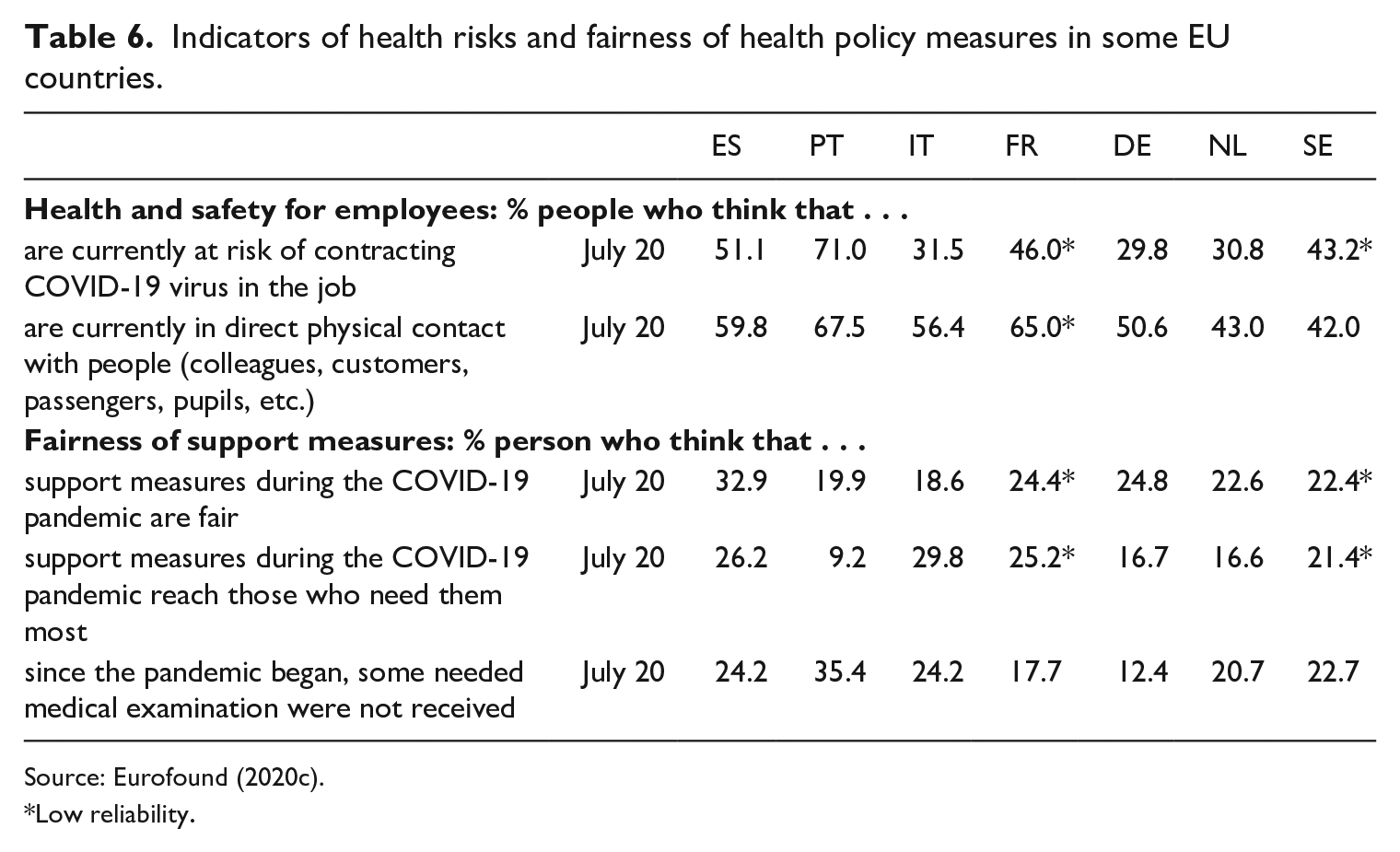
Source: Eurofound (2020c).
Low reliability.
Looking at the impact of the pandemic COVID-19, some of the most relevant changes occurred in the working conditions, with differences between these countries. Table 7 presents those differences, reflecting the initial decisions of confining, or not, by national health authorities. A high percentage of people shared the opinion that the number of working hours decreased a lot, except for the Netherlands and Sweden that confined less, having then a weaker effect on labour market. Many people lost their jobs, temporally and permanently. Remote work was also an experience promoted by public policies, widely disseminated over the countries, and well accepted by the population.
Indicators of working conditions in some EU countries after COVID-19 pandemic.
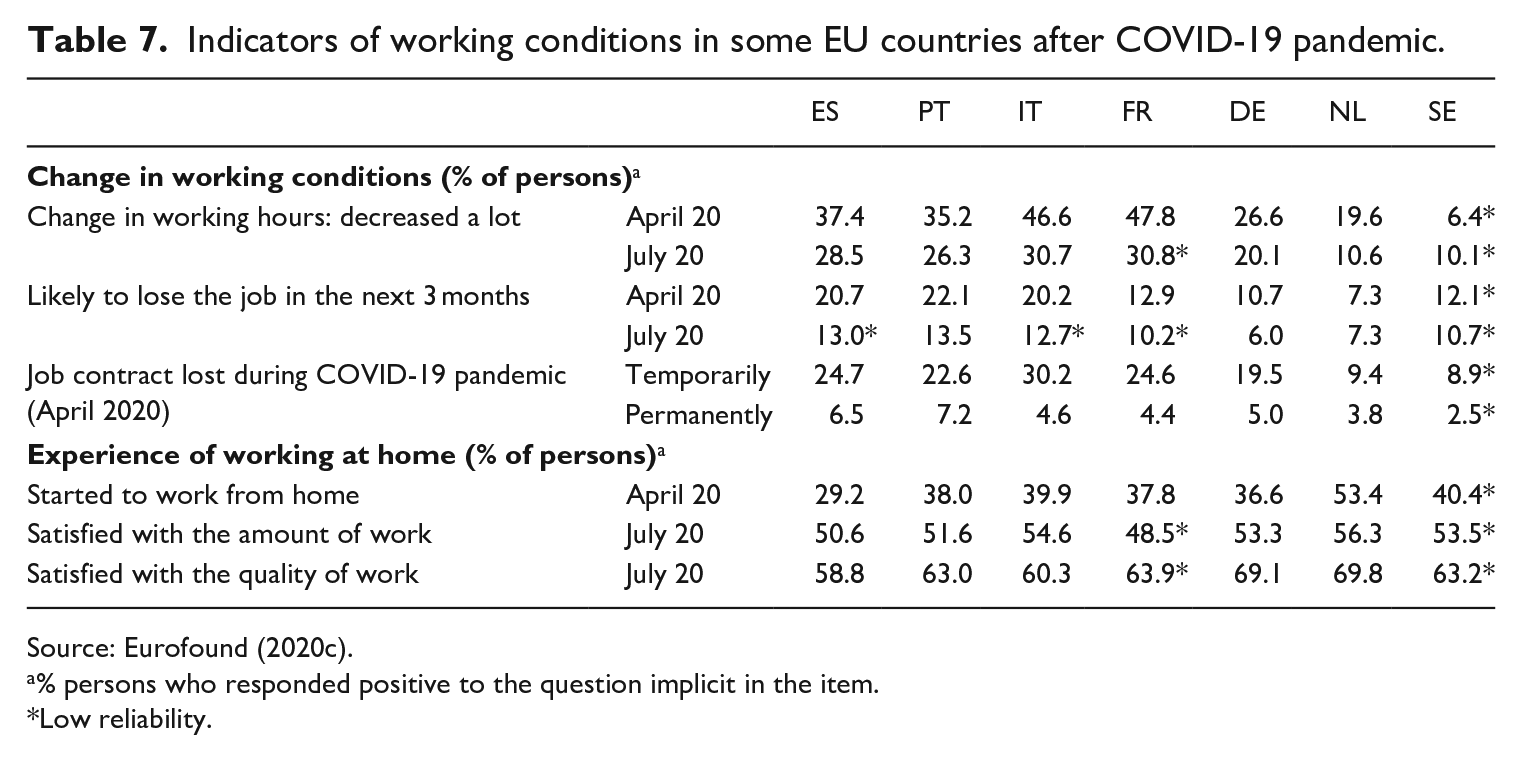
Source: Eurofound (2020c).
% persons who responded positive to the question implicit in the item.
Low reliability.
Table 8 provides information on the financial situation of the population in the initial stage of the pandemic COVID-19 and, as well, on the effect of some policy measures adopted in each country. There was a generalized great reduction in the living conditions, once measured using several indicators of material deprivation. The southern countries (Spain, Portugal and Italy) were those that faced a more severe financial worsening.
Indicators of financial situation and support measures in some EU countries.
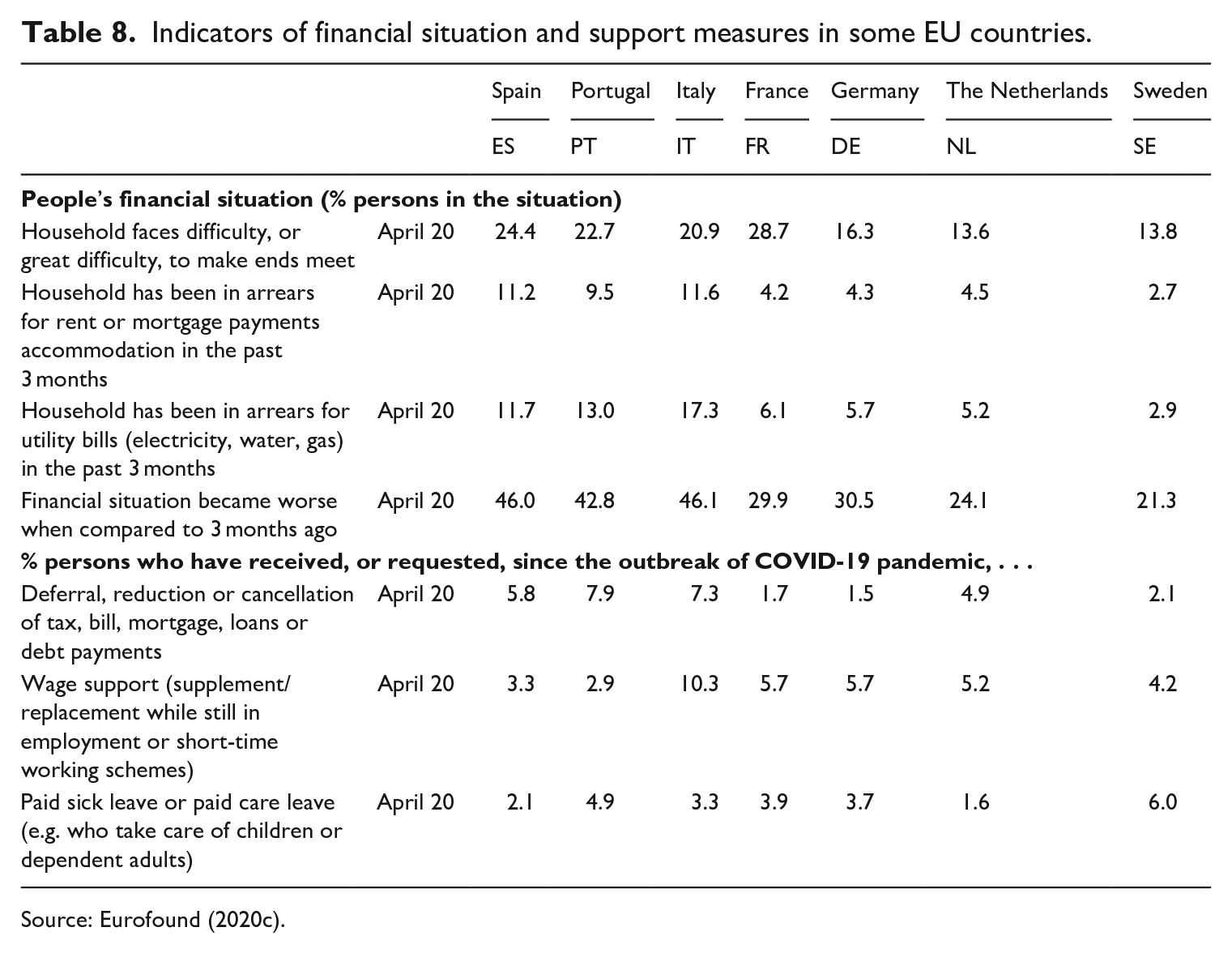
Source: Eurofound (2020c).
Some measures were implemented to face such deficits in the household financial situation. Three of the most relevant policy are described in the table, and distinct pattern emerge for each of them. The implemented measures on deferral, reduction or cancellation of tax, bill, mortgage, loans or debt payments were more relevant in the southern countries (Portugal, Spain and Italy), while the measures of wage support (supplement or replacement of wages while still in employment) were of greater relevance in the bismarkian countries (France, Germany) and Italy. Measures of paid sick leave or paid care leave (as in the case of care to children or dependent adults) are of higher relevance in Sweden (already found above in Table 4, on measures of income protection beyond short-time work), but also in Portugal.
A set of indicators of social resilience for COVID-19
The creation of a system of indicators of social resilience has already some tradition in the EU, mainly from the research made by the Joint Research Centre (JRC) since 2015, intending to provide support to policy making (Alessi et al., 2019; Giovannini et al., 2020) and supported in a conceptual framework designed to make it adequate to specific kinds of adverse shocks (Manca et al., 2017). A good survey of literature on the construction of indicators of vulnerability and resilience can also be found in Tapsell et al. (2005).
Our purpose is more limited in scope, when compared with these approaches. We are strictly intending to make use of new data, collected to cover the COVID-19 phenomenon in several relevant dimensions during COVID-19, that is, in the period since April to July 2020, namely, qualitative information collected on policy measures implemented in this period. Our approach is rather exploratory and consisted of using some of the above data to propose a set of indicators of resilience and to essay a summary index that allows to rank the countries included in the analysis. This was made and the results are presented in Table 9.
Indicators of COVID-19 resilience.
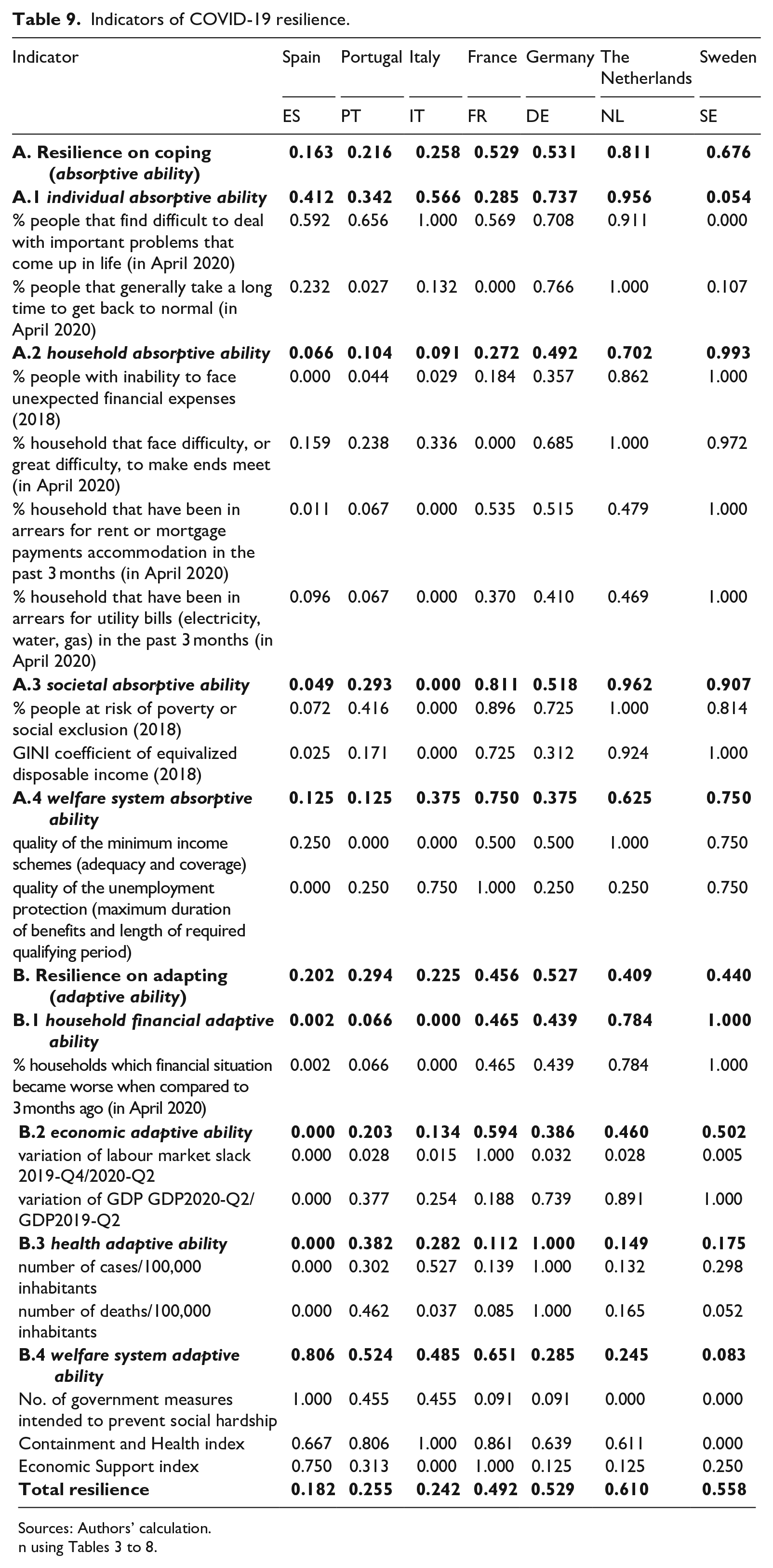
The proposed indicator of resilience is a composite indicator obtained as an aggregation of 18 single indicators obtained from variables already analysed in previous sections of this article. Two transformation were required intending to generate indices reflecting resilience. One of such transformation was made in order that all have a direct/positive relation to resilience. In case that such relation is inverse/negative, an inverse transformation x = 1/y was made. Another transformation was a normalization procedure so that each single indicator has values in the range [0, 1]. A very simple method was used, making the normalization of the original variables, as follows:

and making simple arithmetic averages to aggregate into a composite index.
A distinction was made of two groups of indicators, that correspond to two distinct capacities/stages of social resilience: absorptive/coping (resilience on coping) and adaptive (resilience on adapting). The total resilience index is obtained as a simple arithmetic average of two composite indices: index of resilience on coping and index of resilience on adapting.
The index of resilience on coping intends to measure, for each country, the capacity of the whole society to cope with the social effect of the pandemic, that is, its absorptive ability, considering aspects of the initial situation/conditions as indicators of the ability to absorb or to mitigate the negative consequences of the external shock on individuals/household wellbeing without introducing policy changes.
A distinction was made of four dimensions of such capacity: the individual absorptive ability (extent of optimism and capacity to return to a ‘normal’ situation after the shock), the household absorptive ability (ability to face unexpected expenses, to make ends meet, not to be indebted), the societal absorptive ability (level in terms of wellbeing deficit: the poverty rate, or social cohesion: Gini of household income) and the welfare system absorptive ability (the quality of minimum income schemes and the quality of unemployment protection).
The index of resilience on adapting is intended to measure the extent of the ability of the society to react to the shock, adapting (reinforcing) such abilities, in four dimensions: the economic and health aspects of change, and at the household and welfare system levels of adapting. It should be noted that the selected indicators are of two different kinds: some variables are indicators of resilience of outputs and outcomes, revealing those changes with higher impact on personal wellbeing, while others are indicators that reflect the working of policy measures intending to reinforce the health system, the economy, and the welfare system to react to the pandemic crisis and to its direct and indirect social effects.
A distinction was then made of four dimensions: the household financial adaptive ability (the worsening of the financial situation), the economic adaptive ability (changes of unemployment and of GDP), the health adaptive ability (measured by the relative number of infected cases and of deaths by COVID-19) and the welfare system adaptive ability (‘adaptive resilience of the engine’). In this later dimension, of great relevance for our purpose, it was considered the number of policy measures adopted with the aim of preventing social hardship (from Table 3: although a still rough indicator, it is illustrative of the relevance of such objective of the government policies), the containment and health index and the economic support index (from Table 1).
The results of such procedure are shown in Table 9 and a ranking of the countries by the three indices (coping, adapting and total) is charted in Figure 4.
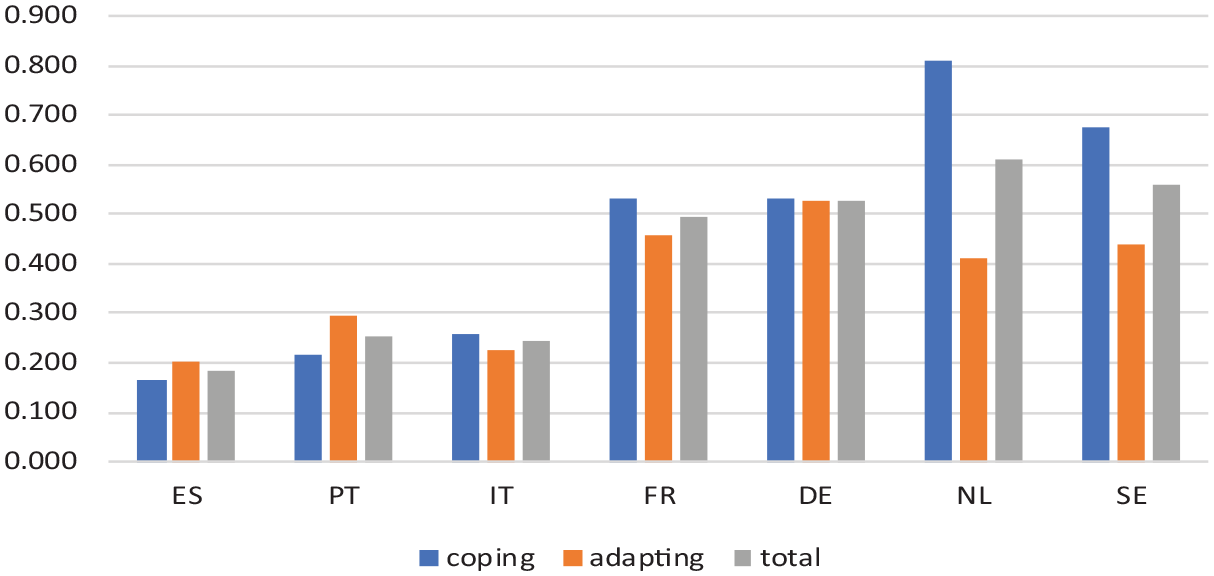
Resilience index.
Figure 4 reveals three distinct groups of countries: those with high resilience (the Netherlands and Sweden), the medium resilience countries (France and Germany) and the low resilience countries (the southern countries: Spain, Portugal and Italy). And other evidences emerge from this figure, namely the fact that in the universalist countries, but mainly in the Netherlands, the resilience to coping is higher than the resilience on adapting, suggesting a higher adequacy of their welfare systems to deal with this COVID-19 pandemic. The southern countries (Portugal and Spain), evidence a distinct pattern, suggesting a higher adaptive ability in comparison with the absorptive ability to react to the COVID-19 pandemic and its direct and indirect social consequences.
Conclusive remarks
This article explored recent data on COVID-19, aiming a preliminary grasp on the ability of European welfare systems to cope with this pandemic and to react to its economic and social effects. We call this social resilience, and the method used consisted of exploring the recent information collected to investigate it: the Eurofound’s COVID-19 PolicyWatch, OxCGRT (Hale et al., 2020a, 2020b), data from EUROSTAT (poverty, inequality, expenditure on social protection) and ECDC (number of cases and mortality due to COVID-19) and specific sources for indicators on welfare system absorptive ability. These data permitted to produce evidence revealing the differences among countries on the capacities of their welfare systems to face the social effects of this pandemic, and the required policy measures for adapting their welfare systems with this aim. The selected cases covered countries that followed different strategies of health policy and belong to different types of welfare systems. Considering the initial conditions of these countries, looking at the occurred changes in outputs/outcomes and the adaptation measures adopted, the evidence presented also reveals that some of these regimes (the southern welfare systems) are less prepared, while others (universalist welfare systems and, to a less extent, the bismarkian ones) are better prepared to cope with COVID-19. Such differences in their welfare system also looks related to different patterns of policy responses to the pandemic when looking at the intensive policy making process by these countries.
The attempt to produce a synthetic index of social resilience in COVID-19 was still exploratory, aiming at a preliminary approximation using these administrative and survey data. The results that emerged from this research reveal the different characteristics of these countries and the different contributions, among these countries, of coping and adapting their welfare systems to respond to this health crisis. It is to be considered as a contribution to the analysis of the countries’ and their welfare systems’ ability to cope and react to uncertain shocks with great social effects. But these results are provisional, since only the first wave of the pandemic was considered. The time dimension of the social resilience requires to explore the adaptive resilience in the waves that follow this one, investigating the time pattern of the adaptive capacity of the welfare system and the differences among countries with distinct welfare regimes, and to observe the expected transformative resilience in these countries, what only may occur in the medium-long term.
Footnotes
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.