
Abstract
This article presents key results from a comparative qualitative Social Policy study of nine African regional economic communities’ (RECs) regional health policies. The article asks to what extent has health been incorporated into RECs’ public policy functions and actions, and what similarities and differences are evident among the RECs. Utilising a World Health Organization (WHO) framework for conceptualising health systems, the research evidence routes the article’s arguments towards the following principal conclusions. First, the health sector is a key component of the public policy functions of most of the RECs. In these RECs, innovations in health sector organisation are notable; there is considerable regulatory, organisational, resourcing and programmatic diversity among the RECs alongside under-resourcing and fragmentation within each of them. Second, there are indications of important tangible benefits of regional cooperation and coordination in health, and growing interest by international donors in regional mechanisms through which to disburse health and -related Official Development Assistance (ODA). Third, content analysis of RECs’ regional health strategies suggests fairly minimal strategic ambitions as well as significant limitations of current approaches to advancing effective and progressive health reform. The lack of emphasis on universal health care and reliance on piecemeal donor funding are out of step with approaches and recommendations increasingly emphasising health systems development, sector-wide approaches (SWAPs) and primary health care as the bedrock of health services expansion. Overall, the health component of RECs’ development priorities is consistent with an instrumentalist social policy approach. The development of a more comprehensive sustainable world-regional health policy is unlikely to come from the African Continental Free-Trade Area, which lacks requisite social and health clauses to underpin ‘positive’ forms of regional integration.
Introduction
Although intra-regional economic transactions occupy the preponderant share of world-regional governance and policy, matters of social governance, policy and development are explicitly present in region-building agendas (Yeates, 2017, 2019; Yeates and Deacon, 2010). Nascent world-regional social policies are evidenced in common regulatory frameworks, promoting (or instituting) social/human rights and undertaking programmes of redistribution across a range of social sectors. Such social policy commitments have ‘thickened’ over time and considerably vary in the forms they take worldwide (Bianculli and Hoffman, 2016; Deacon et al., 2010; Nikogosian, 2020; Robertson et al., 2016; Söderbaum, 2016; Van Der Vleuten, 2016; Yeates, 2007, 2014c, 2019). Northern world-regionalisms, notably the European Union (EU), have attracted the lion’s share of research, but there is increasing interest in and research on Southern social regionalisms (Berrón et al., 2013; Bianculli, 2018; Deacon et al., 2010; Nikogosian, 2020; Olivet and Brennan, 2010; Söderbaum, 2007; Yeates, 2014a, 2017; Yeates and Deacon, 2010; Yeates and Rigirrozzi, 2015). The Sustainable Development Goals’ (SDGs) inclusion of regionalisation processes, regionalist strategies and regional actors has been a source of renewed interest in the potential of more ‘muscular’ forms of world-regional social policy and other sorts of international partnerships supportive of health and social welfare on a regional scale (Yeates, 2017).
For all its advances in recent years, this area of global social policy research remains beset by multiple knowledge gaps, both empirical and theoretical. African regionalisms have been a major feature of the social policy and development landscape, yet they have attracted least research attention among social policy researchers, especially outside Southern Africa. Conversely, while most attention to the significance of regionalism and regionalisation has, predictably, come from Regional Studies, that field has not directed its sights at Social Policy. It is telling that a recent major comparative regional study of African regional economic communities (RECs; Hout and Salih, 2019) made no reference whatsoever to the long-standing and discernable evidence of their social policy content, as charted by Deacon et al. (2010) and, more recently, Van Der Vleuten (2016). Either way, there is little systematic research about how African health and welfare systems are engaged with, or impacted by, such regionalist development processes, nor is consideration given to what this means for citizen health and welfare. Furthermore, although there is now reasonable coverage of many social sectors by literatures on world-regional social governance and policy, health remains far less scrutinised (notably within the comparative study undertaken by Deacon et al., 2010). It is also striking that in a large literature on global health governance drawing attention to an increasingly complex field of multi-level global health actors, institutions and programmes, world-regional health governance and policy remains almost a wholly unopened ‘black box’. Patterson’s otherwise majestic study of Africa in global health governance is a case in point (Patterson, 2018).
The theoretical arguments for stronger world-regional social policy have been well elaborated by Yeates and Deacon (2010). They argued that collective action at regional level can be easier to negotiate and implement than at global level due to a more restricted set of partners who (may) share a common identity and socio-economic circumstances. Similarly, there is greater scope to improve social standards and innovate responses to pressing problems faced by the members at a faster pace and in a more context-specific way than is afforded by global multilateral forms of social policy. Also, they argue, regional-level collective action can enable more effective, coherent responses to pressing social issues than governments acting unilaterally or bilaterally, while also sustaining the interest of prospective partners from outside the region (see also Yeates, 2017; Yeates et al., 2010). But what about the track records of actually instantiated world-regional health policies? The principal comparative study on world-regional social policy (Deacon et al., 2010) had little to say about health, and there has been no international comparative study of health or wider social regionalisms within Africa. Closer examination of RECs’ track records of action in health policy is needed in order to better understand the possibilities and constraints in this sector. Relevant questions include, for example, whether a more concerted and comprehensive regionalist health governance, cooperation and development strategy can substantially contribute to implementing the health and -related SDGs, whether a regionalist transnational organisational structure facilitates greater learning and transfer around health and health policy than other sorts of partnership among nations, and whether regional forms of collective organisation confer strong bargaining power with external stakeholders that can be leveraged in the interests of health.
Closer scrutiny and evidence of RECs’ agendas, discourses and programmes are needed to begin to answer these questions. Such evidence can contribute to improving the knowledge base regarding extant forms and impacts of social regionalism worldwide, and generate new insights into the wide range of forms that health governance and policy takes and the conditions under which it develops in the Global South. For instance, it is now recognised that the management of social welfare and risk in developing countries is mediated by a very different set of institutional conditions than those in richer economies, and that social policies are formulated by a much wider range of policy actors, often existing outside national government institutions (Midgley et al., 2019; Surender and Walker, 2013). However, analysis has typically focused on the impacts and processes of post-colonialism or the role of international development institutions like the World Bank and International Monetary Fund (IMF). In this landscape, actual track records and potential new dynamics flowing from regionalist multilateral actors remain under-researched. This is especially the case in relation to Africa, where, despite the existence of multi-disciplinary social research efforts, there has been next to no dialogue between social policy, health studies, development studies, regional studies and African studies.
This article presents the results of a comparative study of world-regional health governance and policy in Africa in order to expand the evidence base on African social world-regionalisms and to improve understanding of world-regional structures and processes of cooperation and integration in the health domain, especially in the Global South. Using a systematic content analysis of documentary sources of nine African regional groupings, we identify their health agendas, policy approaches and programmes. The organisations included in this study are the African Union (AU) plus eight RECs formally recognised as ‘building blocks’ of the AU: Arab-Maghreb Union (AMU), Community of Sahel-Saharan States (CEN-SAD), Common Market for Eastern and Southern Africa (COMESA), East-African Community (EAC), Economic Community of Central African States (ECCAS), Economic Community of West African States (ECOWAS), Intergovernmental Authority on Development (IGAD) and the Southern African Development Community (SADC). Country membership of each REC is provided in Supplemental Appendix 1.
The article responds to the following specific research questions.
Focusing on various principal areas of world-regional health governance and policy – service delivery, medical products, health workforce, information, finance and governance – we report results from a wider primary research study of the scope and nature of African RECs’ regional health policies and programmes.
Focusing on health as a specific social sector is important for several reasons, but key among them is that access to health care for all Africans remains a major challenge for the continent’s policy makers. Debates and policy experiments concerning the optimal reform path have increased in urgency in recent years as the continent confronts a significant quadruple ‘burden of disease’ of poverty, non-communicable diseases, HIV/AIDS, and violence and injury (World Health Organization [WHO], 2018). This means that as well as addressing traditional infectious diseases and those stemming from poverty, the focus of delivering health care must also include chronic long-term non-communicable conditions such as diabetes, hypertension and chronic obstructive pulmonary disease. On key morbidity and mortality indicators (and other millennium development goal (MDG) targets), performance is poor across almost all 54 AU countries with high HIV and tuberculosis (TB) infection rates, prevalence of underweight children and child, infant and neonatal mortality rates. Most disappointingly, in several countries, progress has actually been reversed in the past decade. To take just one example, in South Africa, one of the continent’s richest economies, maternal mortality rates have deteriorated and overall life has expectancy reduced since 1994 (STATS South Africa, 2014).
Clearly, social determinants (poverty, income inequality, unemployment and poor living conditions) are an important part of the explanation for the absolute and relative poor health status of Africans. However, as recognised in numerous WHO and World Bank assessments, Africa’s failing health systems (which remain under-resourced and socially inequitable) are also an important explanatory factor in poor health outcomes. Lack of routine availability of medicines and a critical shortage of millions of doctors, nurses and midwives remain a significant problem, illustrated in the statistic that Sub-Saharan Africa has 24% of the global burden of disease but only 3% of the world’s health workforce (WHO, 2018). These challenges have been exacerbated in the past decade by the global economic downturn and less aid from Western donors. It is then perhaps unsurprising, that irrespective of their original mandates, Africa’s regional governance bodies are increasingly prioritising health care as a central issue for public social and economic policy. Our focus on African regionalisms in health responds to this continent-wide policy challenge. A better understanding of the multi-level governance of the health sector and of the diverse spaces across which it plays out will be important in assessing the potential for RECs to be harnessed to achieve the health and -related SDGs.
Method
The data on which this article is based were gathered through a comprehensive documentary review of the ways and extent to which African RECs are engaged with health. 1 The review uses the WHO’s health systems ‘building blocks’ framework (WHO, 2010) which defines a health system as consisting of six core components to codify instances of presence in given health areas. It incorporates a spectrum of policies, activities and actors; some have a more clinical focus, related to health promotion, provision of care and treatment of disease, while others have a stronger governance focus, related to coordination and rule-making. In between sit those that have a wider focus than clinical interventions (e.g. health promotion) and a narrower focus than governance (e.g. health workforce organisation). We incorporated six principal areas of the health sector, with several sub-components of each:
Service delivery: access to health goods and services, health promotion, provision of health and medical infrastructure (e.g. primary health care, hospitals, laboratories);
Medical products, vaccines, technologies, medicines: regulating access, quality, price, distribution, supply chain management, pharmacovigilance;
Health workforce: training of health and medical personnel, quality improvement, performance management, recruitment, retention and distribution of workers;
Health information: collection, processing and coordination of health data, integration of health data systems, medical research;
Health financing: financing public health sector, organisation of health insurance system, other health financing initiatives;
Health governance: registration of medical/health practitioners and corporate health providers, regulation of private and public sectors, provisions for civil society participation in policymaking, support for institutional reform/innovation, creation of new institutions.
This framework is only one of many possible frameworks, including the WHO framework for health systems ‘Performance Assessment’ and the World Bank’s ‘Control Knobs’ framework (Pyone et al., 2017). There are many commonalities in the various strategic frameworks for conceptualising health systems, however, and our choice of the ‘Building Blocks’ schema permits a coherent approach for the range of indicators available and measurement strategy utilised in this study.
We systematically mapped the presence of the RECs across these different components and treated any instance of activity or resource as eligible for inclusion. We assigned instances to more than one category where relevant (e.g. medical research that entails establishing a new health institution featured in Governance and Service Delivery). Noting the blurred boundaries between the categories, the framework nevertheless proved sufficiently concrete for organising the data for the purposes of this study. The survey was completed for each organisation through desk-based research into information provided by RECs themselves. This information was accessed through RECs’ web-portals and included ratified treaties, ministerial statements and speeches, annual reports, research reports and media briefings. This was supplemented as necessary through cross-checking with other publicly available documents from multilateral and bilateral donor and development agencies as well as with research literatures. An instance of activity is recorded as either present or absent, though the significance of the activity is taken into account through qualitative evaluation of the data set from each REC.
For all the strengths of the methodological approach for this study, there are also unavoidable limitations. First, it is reliant primarily on the RECs’ own presentation of their regional health strategies, programmes and projects. Although we would expect them to present in the most favourable light the fullest amount of information, this presentation is, in turn, dependent on the resources they have at their disposal. In this, we found the volume and quality of the information available highly variable. Second, the significance of RECs’ activities can be challenging to interpret. A notable issue is the lack of comprehensive contextual information available to assess the relative priority given to different objectives, including their actual resourcing. Indeed, there are likely to be differences between what RECs are saying they are doing (policy promulgations) and what they are doing in practice (policy implementation). This framework does not capture that difference.
Similarly, although this survey does well in mapping the commitments within and between the RECs and thus drawing an overall view of the presence of health within African regional integration strategies, it is difficult to ascertain the qualitative aspects of how programmes are working within and across member states in practice, including whether they are leveraging innovations and other impacts. This survey, based on what RECs publicly say they are doing, and aiming to descriptively map the range and nature of their activities and commitments across the component areas, cannot fully address these limitations. It is, however, a first important step that starts to fill significant gaps and identifies key themes and issues for further investigation.
Contextual overview of African RECs
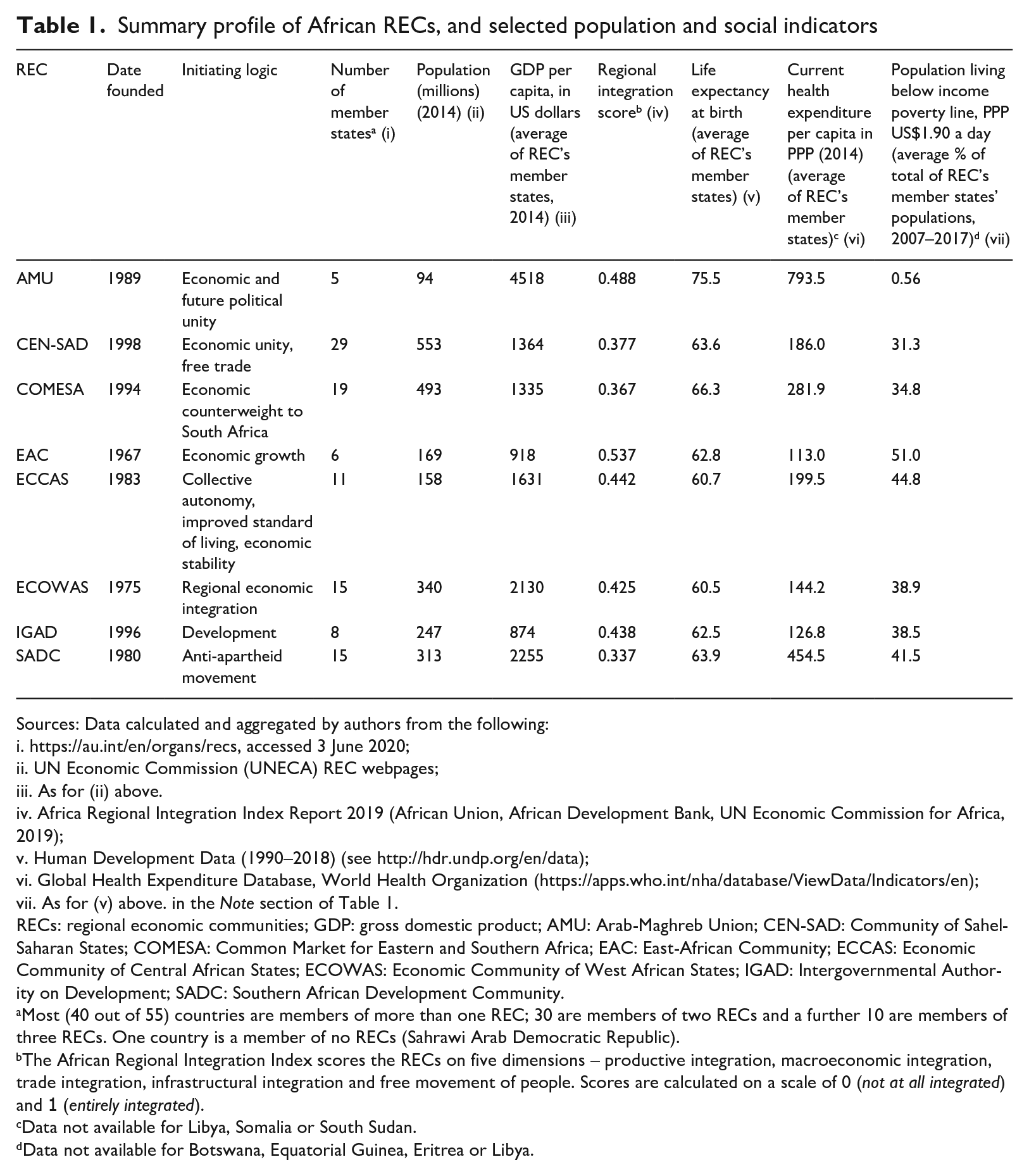
Although the continent currently has 14 inter-governmental organisations, each working on regional integration issues with numerous joint treating and protocols, the AU recognises just eight RECs. These eight inter-governmental partnerships differ markedly in their histories, size, degree of integration achieved, and social, economic and health profiles. Table 1 summarises their profiles (see Hout and Salih, 2019, for a comprehensive overview of general aspects of African RECs).
Summary profile of African RECs, and selected population and social indicators
Sources: Data calculated and aggregated by authors from the following:
https://au.int/en/organs/recs, accessed 3 June 2020;
UN Economic Commission (UNECA) REC webpages;
As for (ii) above.
Africa Regional Integration Index Report 2019 (African Union, African Development Bank, UN Economic Commission for Africa, 2019);
Human Development Data (1990–2018) (see http://hdr.undp.org/en/data);
Global Health Expenditure Database, World Health Organization (https://apps.who.int/nha/database/ViewData/Indicators/en);
As for (v) above. in the Note section of Table 1.
RECs: regional economic communities; GDP: gross domestic product; AMU: Arab-Maghreb Union; CEN-SAD: Community of Sahel-Saharan States; COMESA: Common Market for Eastern and Southern Africa; EAC: East-African Community; ECCAS: Economic Community of Central African States; ECOWAS: Economic Community of West African States; IGAD: Intergovernmental Authority on Development; SADC: Southern African Development Community.
Most (40 out of 55) countries are members of more than one REC; 30 are members of two RECs and a further 10 are members of three RECs. One country is a member of no RECs (Sahrawi Arab Democratic Republic).
The African Regional Integration Index scores the RECs on five dimensions – productive integration, macroeconomic integration, trade integration, infrastructural integration and free movement of people. Scores are calculated on a scale of 0 (not at all integrated) and 1 (entirely integrated).
Data not available for Libya, Somalia or South Sudan.
Data not available for Botswana, Equatorial Guinea, Eritrea or Libya.
The oldest, ECOWAS, was established in 1975, while the youngest, CEN-SAD, was formed more than two decades later in 1998. Many were borne from longer periods of regionalism. For example, IGAD superseded the previous IGADD (Drought & Development) while EAC was previously the Permanent Tripartite Commission for East African Cooperation. Their initiating logics also differ. SADC emerged from liberationist (anti-apartheid) struggles, COMESA aimed to create an economic counterweight to South Africa to help counteract the destabilising economic (and other) impacts on southern African states, while IGAD was more explicitly a development partnership from the outset. CEN-SAD, ECOWAS and EAC all have economic objectives at their heart, though AMU also has ambitions for future political unity.
The RECs also vary considerably in size – the smallest in terms of member countries and population being AMU and the largest CEN-SAD. Variation is also seen in the extent of regional economic integration actually achieved. The most integrated, according to the African Regional Integration Index (ARII), are EAC and AMU; the least integrated are SADC and COMESA. The ARII is limited to economic sector integration however, and says nothing about the extent of regional integration in the social sector. Drawing on other data, however, we can get a sense of the overall standard of living for each region, and thus the social policy challenges they face (columns 6, 8–10). Using gross domestic product (GDP) per capita as a proxy for standard of living, AMU stands head and shoulders above all other RECs; equally, IGAD and EAC are the poorest. These disparities are mirrored in social indicators of life expectancy, health expenditure and poverty where AMU is by far the most socially wealthy region in this sense. EAC stands out as the region that is least wealthy, economically (column 6) and socially (columns 9, 10), and is among the regions with the lowest life expectancy. Although EAC is also the region with the highest degree of integration (column 7) and AMU the (second) highest, it is beyond the scope of this article to comment on the relationship between regional economic integration and regional standard of living.
The AU is a regional formation on a continental scale and of a different order than the eight African RECs. It is not included in Table 1. Officially launched in 2002 to succeed the Organisation of African Unity (OAU), the new continental organisation sought to refocus attention from the previous prioritisation of decolonisation and defeating apartheid, towards increased growth and economic development among its 55 member states. Nevertheless, Article 3 of its constitution explicitly includes the social well-being of people and ‘the eradication of preventable diseases and the promotion of good health on the continent’ (AU, 2000: 6). Through its Social Affairs Division and Division of Health, Nutrition and Population, the AU provides a leadership role and works in collaboration with AU member states and the eight RECs to coordinate health programme development, implementation and monitoring, including diseases and disaster surveillance, preparedness and response. The AU also coordinates the sharing of laboratories and diagnostic services and promotes collaboration and networking between member states around these resources. Almost all current REC health frameworks and public documents endorse and seek to work in tandem with the AU’s Africa Health Strategy 2016–2030 (AU, 2016), the primary consolidative document for all African commitments in the health sector.
Finally, it is important to note that memberships of the different groupings often overlap, signalling that governments see little contradiction in membership of more than one regional grouping. For reasons of manageability, however, we treat these regional groupings as distinct partnerships with clear boundaries. It is outside the scope of this article to consider interaction in regional policy development that could conceivably come from such overlapping memberships. It is also important to understand that the RECs are not organisations of the United Nations (UN) system, the World Bank or regional development banks. While the presence of multiple multilateral regional agencies working in any given area is a source of potential strength, stimulating debate and innovation, it also compounds complexity in policymaking (Yeates, 2017).
Findings
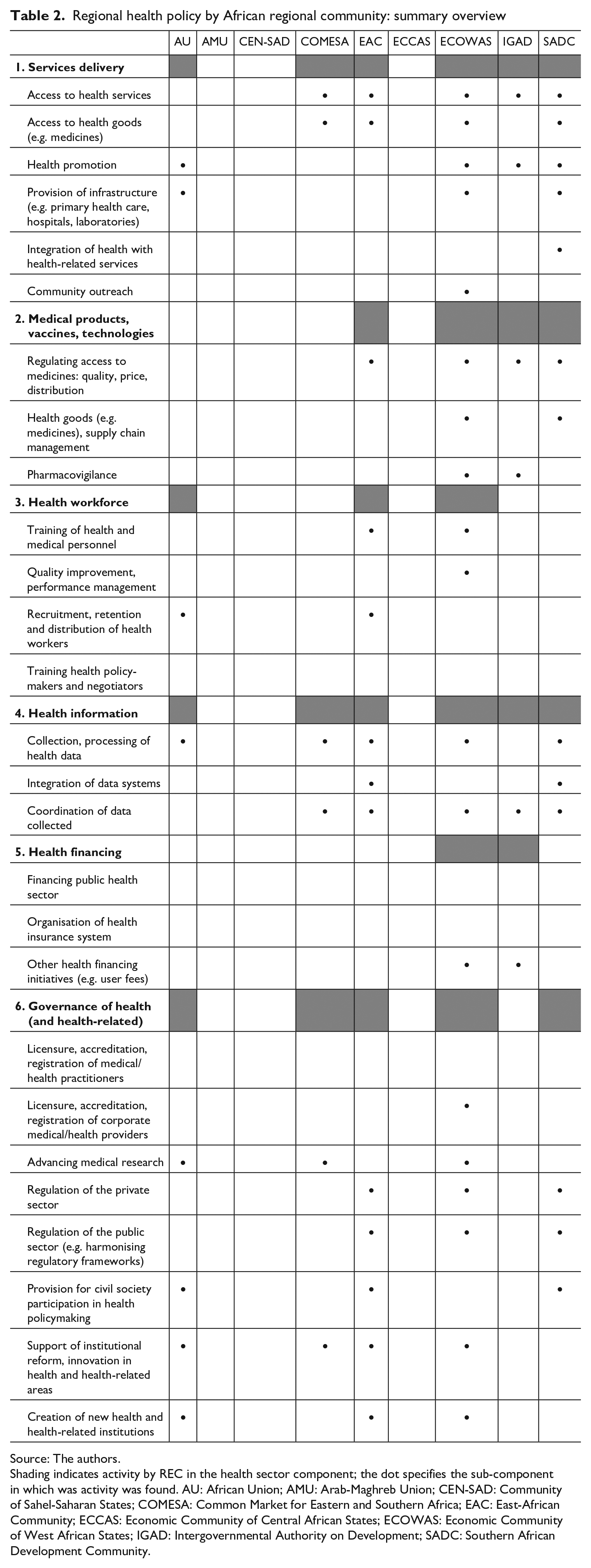
Table 2 sets out in matrix format summary findings for each of the RECs, including the AU. It indicates the degree of variation and selectivity as to which areas and sub-components of health policy feature in RECs’ regional health policies. AMU, CEN-SAD and ECCAS have no appreciable health policy. Among the remaining RECs, EAC, ECOWAS and SADC regional health policies are the broadest in terms of the number of areas and sub-components they comprise. Of the six components, service delivery (especially access to health goods and services, health promotion and provision of health infrastructure) and medical products are most likely to be incorporated into RECs’ regional health policy. These two areas feature in all active RECs. Health workforce has a relatively low degree of incorporation (just three RECs are active here: EAC, ECOWAS and AU), though there is some overlap with the health governance components of accreditation and registration activities. Health information is an intermediate area of REC regional health policy in the sense that all six RECs are involved, with most of them involved in collecting, processing and coordinating data; two RECs (EAC and SADC) have become involved in integrating data systems on a regional scale. Health financing is only minimally incorporated, with just two RECs (ECOWAS, IGAD) active. Here, donor sources predominate. Health governance in terms of accreditation and registration features across all RECs provision; civil society participation or institutional reforms (e.g. a recalibration from tertiary to primary care led service, or universal provision) are largely absent. The discussion now expands on these findings and highlights the key issues to emerge from the thematic analysis.
Regional health policy by African regional community: summary overview
Source: The authors.
Shading indicates activity by REC in the health sector component; the dot specifies the sub-component in which was activity was found. AU: African Union; AMU: Arab-Maghreb Union; CEN-SAD: Community of Sahel-Saharan States; COMESA: Common Market for Eastern and Southern Africa; EAC: East-African Community; ECCAS: Economic Community of Central African States; ECOWAS: Economic Community of West African States; IGAD: Intergovernmental Authority on Development; SADC: Southern African Development Community.
Structures of regional health policy
Although the original treaties to establish the RECs do not explicitly reference health as a key focus, most RECs have subsequently developed a major health policy framework or a strategic development plan and identified health as an important area of work for the organisation. For example, SADC’s Health Policy Framework, Protocol on Health and rolling 5-year Strategic Development Plans propose policies and priorities for health research and surveillance, health promotion and education, disabilities, and violence and substance abuse, and outline key objectives, targets and actions. These include bold objectives such as 15% of national government budgets to be allocated to health and tackling the restrictive abortion laws in most member states. Despite differences in the level of detail and specificity of objectives and strategies, all REC health frameworks include aspirations to promote public health and other preventive actions, address common challenges related to cross-border health issues, share information and use of evidence and standardise protocols and guidelines. Even CEN-SAD, one of the RECs with little overt activity in this area, identified health as a strategically important policy area.
As CEN-SAD argued:
Since it was created in 1998 under the initiative of Colonel Kadhafi, CEN-SAD has endeavoured to set an economically progressive community relying on peace, security, states’ stability, free circulation of goods and persons as well as right for work and property. In order to achieve these goals the organisation has created five main institutions . . . and four ministerial committees (health, security, finance and economy committees) have been set up to back the work of those institutions. (au.int/en/recs/censad, accessed 4 June 2018)
The leading justification for focusing on health outlined in all of the RECS’ strategic frameworks or charters is that it is necessary for the enhancement of human capital, economic productivity and development. Strategic cooperation and regional coordination between member states to address common health challenges are crucial, according to most REC mission statements, to achieve wider and sustainable economic and social progress. ECOWAS and SADC are typical in this. Thus,
. . . the activities to be conducted by WAHO [West African Health Organisation] . . . are aimed at ensuring improved health for the region’s populations, as a key ingredient for economic development and regional integration. Indeed, a healthy population is a source of productivity and of production, and therefore of increased wealth creation. On the other hand, epidemics can compromise every effort made by ECOWAS to promote free movement of persons and goods, thereby jeopardizing the whole concept of regional integration. (ECOWAS, 2016b: 10) A healthy population is a necessary catalyst for economic and social development. As Southern Africa improves industrial capacity and economy, the health of its citizens remains paramount in ensuring a sustainable future. (SADC, 1999: 5)
There is, however, considerable variation in how health is institutionally located and prioritised. AMU, CEN-SAD and ECCAS appear to have little or no indication of regional health infrastructure or activity, that is, services, policies or programmes. Lack of resources and non-payment of subscription fees by member states seem to be the main factor as well as political conflict between individual member states. ECCAS, for example, was essentially inactive for several years until 1999, despite the existence of a formal treaty, due to inter-state conflict between the Democratic Republic of Congo (DRC), Rwanda and Angola. Similarly, in CEN-SAD, a proposal by the Libyan state which attempted region-building through health initiatives eventually gave way under the pressure of relentless international political conflict focused on the lead state and which destabilised the region. In other RECs, arrangements for health policy and programmes appear fragmented, variable and patchy. Health has typically been a recent addition and occupies a lower and less powerful status organisationally, lacking a dedicated or large Directorate or Division to parallel other powerful sector Directorates such as agriculture, security, disaster management or economics. COMESA’s health and HIV/AIDS programmes fall under its Gender and Social Affairs Directorate and exemplify this institutional organisation. SADC and IGAD are unusual in according ‘Health’ a discrete and independent Division. They are also unusual in that, like COMESA, they hold annual Health Forums or meetings of Health Ministers.
Annual activity reports of most RECs indicate that implementation of planned health activities is routinely hampered by delayed disbursement of funds by member states and weak coordination of decisions and resolutions by the regional body. Even in the case of ECOWAS, which has established a specialised regional health institution (the West African Health Organisation [WAHO], mandated to harmonise health activities), we learn that ‘implementation of planned WAHO activities were hampered by . . . limited annual budget growth . . . and disbursement of financial resources to WAHO’ (ECOWAS, 2013). COMESA also announced that despite being approved by the Council of Ministers in 2016,
. . . The launch and implementation of the COMESA Health Framework and Regional HIV/AIDS policy have been affected by the lack of sufficient funds . . . The seemingly limited availability of funds has also affected the establishment of the Health Desk at COMESA Secretariat which would be instrumental in promoting regional level interventions in the health sector. (COMESA, 2017)
Service delivery
Across all ‘health-active’ RECs and the AU, the paramount concern and emphasis in the health sector are directed towards control of pandemics, epidemics and ‘vector-borne’ communicable diseases. Malaria, TB and HIV/AIDS feature most prominently historically, alongside Ebola since 2014. The outbreak of Ebola in West Africa in 2014 was particularly key in triggering the stepping up of recent investment and epidemic control activity. Protocols, guidelines, strategic frameworks and plans, information exchange systems and public health mobilisation campaigns concerned with disease eradication or containment are prominent in REC policy statements and websites. A dedicated ‘Division of AIDS, TB, Malaria and Other Infectious Diseases’ was established early within the AU’s Social Affairs Directorate; it was joined more recently by the new Pan African Centre for Disease Control in 2017. Several RECs hold annual activities and regular campaigns for raising public health awareness around HIV/AIDS and other diseases (such as SADC’s ‘Annual Malaria Day’ and ECOWAS’ synchronised campaigns of seasonal malaria prevention), and most have established technical and advisory groups or Centres for Disease Surveillance. SADC’s statement of the prevalence of communicable diseases in the regions instantiates the link between such diseases and development that all RECs must tackle. Thus:
Communicable diseases are a serious concern for social and human development in the region. The SADC region accounts for one-third of all people living with HIV/AIDS worldwide; member states are among those countries with the highest rates of TB and 75% of the SADC population is at risk of contracting malaria. This trio of diseases is a major threat to sustainable development in the region. (sadc.int/themes/health/communicable-diseases, accessed 10 May 2018)
In terms of resources and provision of infrastructure, the main emphasis is on cross-border challenges and issues, especially containment of the spread of disease among and by mobile populations (notably, transport or sex workers, refugees, internally displaced persons) and populations living in close proximity to borders. Examples include the Botswana Cross Border Wellness clinic within SADC (SADC, 2018); IGAD’s HIV/TB/Malaria programme funded by the Global Fund to address common challenges related to cross-border health problems at 13 refugee settlements within the region (IGAD 2016a); and state-of-the-art health facilities built at the borders of three ECOWAS member countries affected by Ebola (Guinea, Liberia, Sierra Leone) (ECOWAS, 2016a). Similarly, major achievements of the health sector during the lifetime of the EAC’s Fourth Development Strategy Plan (2011–2015) include an integrated policy plan for cross-border interventions on disease surveillance, joint outbreak investigation, public health and sanitation (EAC, 2017: 45).
Unsurprisingly, all ‘health active’ RECs have a dedicated HIV/AIDS programme and policy unit irrespective of whether they have an independent Health Division. The epidemic is widely acknowledged as the biggest health challenge for Sub-Saharan Africa and is blamed for halting progress and economic development across the continent. As the AU states,
. . . there is concern that in spite of the tremendous progress made in the fight against HIV/AIDS [since 2000], Africa still remains one of the most affected regions in the world . . . thereby constituting major threats to national and continental socio-economic development, peace and security, among others. (AU website: Special Summit of the African Union on HIV/AIDS, Tuberculosis and Malaria, Abuja, Nigeria, accessed 5 June 2018)
COMESA’s multisectoral programme on HIV/AIDS (financed through a grant from the Sweden and Norway’s development cooperation agencies, SIDA and NORAD, respectively) and its Regional HIV/AIDS policy represents the view of most RECs that:
In the field of health, the HIV/AIDS pandemic is one of the greatest challenges facing the region. According to WHO estimates, 90% of all AIDS cases are on the African continent with disproportionate social and economic implications . . . in terms of loss of labour and productive time and human suffering. (COMESA, 2005: 98)
Moreover, the subsequent decade of unprecedented development across Africa coincided with the dramatic results in the AIDS response. Reduction of the epidemic and mitigating its impacts are essential for investment and growth in the region.
Medicines, drugs and pharmaceuticals
After epidemics and communicable diseases, the next most prominent health priority and activity are medicines, drugs and the pharmaceutical industry. Most RECs have established regional regulatory mechanisms or harmonisation programmes for the pharmaceutical sector. They include registration (approved lists) of essential medicines, quality assurance regulation (monitoring and controlling substandard products, illicit drugs and illegal trade of medicines) and protection of traditional African medicines. They also involve protectionist policies to deter dependency on pharmaceutical imports, further illustrating that health (at least, in terms of the pharmaceutical industry) is envisaged as a vital element of a broader industrialisation strategy. Strategies to increase indigenous pharmaceutical production and reduce dependence on imported medicines mainly entail the development of national and regional private-sector bodies to manufacture and supply medicines together with the promotion of continent-wide trade.
A key focus across the continent is regional trade and supply chain management for competitive regional pharma industry, with the aim of ensuring that the supply of sustainable and affordable essential medicines produced in the region substantially expands by 2020. Pharmaceutical plans of all RECs emphasise strengthening regional pharma industry capacity together with promoting inter-regional trade, the principal objective being economic growth. The 2nd EAC Pharmaceutical Manufacturing Plan of Action 2017–2027 is typical of this in defining itself as a ‘regional roadmap’ to guide the community towards ‘evolving an efficient and effective regional pharmaceutical industry that can supply national, regional and international markets with efficacious and quality medicines’ (EAC, 2018: 3). The plan sets high-level goals with specified targets for the development of the pharmaceutical sector to decrease dependency on pharmaceutical imports from outside EAC and support the expansion of product portfolio of EAC firms. Purchases by national medicines procurement agencies are to be sourced from EAC pharmaceutical manufacturers, and EAC companies are incentivised to produce more advanced pharmaceutical formulations (e.g. delayed release formulations, small volume injectables, double-layered tablets; EAC, 2018).
Similarly, the 2012 and more recently updated 2017 ECOWAS Pharmaceutical Good Manufacturing Practices Roadmap (launched with United Nations Industrial Development Organisation (UNIDO) aims to establish which medicines in West Africa are produced and by who (ECOWAS, 2017). The document addresses the issue of unequal distribution of manufacturing facilities within ECOWAS, which requires different policy measures between countries and serves as a standard for monitoring purposes. It supports local pharma manufacturers to achieve international standards and develop regional frameworks for guiding national approaches. It also serves as a strategic tool of national regulators to ensure that industries meet stipulated criteria, and to strengthen regulatory capacity for the inspection of manufacturing facilities and guide the set-up of new facilities in countries wishing to establish or expand their pharma manufacturing sector.
Health workforce
Few RECs have developed policies or guidelines concerned with harmonisation of training, accreditation and licencing of health personnel or – somewhat surprisingly – the movement of health personnel between member states. Where regional initiatives for health personnel training exist, they are typically funded as discrete projects by external donors. Examples are the financing of specialism training of ECOWAS doctors and nurses in Brazil and a South Korean programme to train physicians and nurses from the EAC. The AU has established an Africa Commission for Diseases Control and Prevention (CDC) Mobile Response Team to be deployed as first responders to member governments who request assistance during public health ‘events’ and has identified an initial cohort of health professionals (AU, 2018). These are, however, isolated and small-scale projects and nowhere near significant enough to address the scale of the challenges given the human health resources crisis across the continent (WHO, 2006, 2016; Yeates and Pillinger, 2019).
Health information
Despite ambitious policy statements, there appear to be relatively few practical examples of actually integrated regional health data systems or region-wide health projects. Two notable exceptions are IGAD’s US Agency for International Development (USAID)-funded Health Data Project, focusing on specific border areas to ensure continuity of care for border populations, especially women and children, and ECOWAS’ WAHO health data warehouse, established in 2013 to share evidence and best practice on a regional scale. Regional Centres for Disease Surveillance and Control were evident in three regions: ECOWAS, EAC and SADC. Most of the activity in this area seems to have been relatively recent, developed in the wake of the 2014/2015 Ebola outbreak, and is focused on developing an emergency regional health worker corps (see ‘Health workforce’ section).
Health financing
Despite few references to government fiscal targets or commitments, there is evidence of substantial collaboration between RECs and non-African external donors – both traditional donors and new Southern partners – for the financing of many initiatives and services, in particular where the construction of new infrastructure is required. Examples include specialist health laboratories funded by the World Bank and US Centers for Disease Control and Prevention in the EAC, high-quality diagnostic services funded by the UN in IGAD and telemedicine, data systems and platforms in several regions. In addition to engagement with traditional Western bilateral (in particular the United States) and multilateral donors such as the World Bank, WHO and the EU, there is increasing involvement with new ‘Southern’ donors, including Cuba, Brazil, Venezuela, South Korea, Japan and Kuwait (though notably there appears to be relatively less activity from China). In addition to government funding, there is also a significant presence of private philanthropies such as the Gates and Rockefeller Foundations.
There is also a strong orientation towards partnership with the private sector in all RECs. Policy frameworks and ministerial announcements affirm that private-sector partnerships are needed to complement public resources and that active involvement of member states with private-sector stakeholders is actively encouraged. The IGAD Institutional Strengthening Action Programme (ISAP) is very typical of other RECs in describing its corporate development agenda:
IGAD recognises the need for the necessary and sufficient institutional capacity to deliver its mandate and meet stakeholder’s expectations . . . [and] equally acknowledges that gaps in its capacity are considerable and . . . require sustained external support from various partner agencies and institutions, including private sector partners and Specialised Institutions . . . Development Partners and other results-oriented organisation. (IGAD, 2016a: 27)
Similarly, the First Progress Report (2018) of the African Centre for Disease Control and Prevention states that,
Africa CDC is pursuing a mechanism for sustainable financing through businesses, the private sector, and African philanthropy. The Africa CDC private sector and philanthropy engagement strategy has . . . a priority focus . . . on identifying African companies dealing in telecommunications and other sectors . . . and African philanthropists who have given historical support to the African health agenda. (AU, 2018: 10)
Health governance
While an emphasis on communicable diseases and pharmaceuticals is anticipated, the narrowness of regional health agendas and the absence of other health priorities and aspirations are nevertheless surprising. In particular, few RECs discuss or appear to have designated strategies for institutional reforms for health system strengthening or sector-wide approaches (SWAPs) to health care. SADC and the EAC are unusual in explicitly emphasising a health systems approach in their policy frameworks. A primary-led health care approach is especially absent. Instead, policy goals are typically addressed through narrowly defined ‘vertical’ policy instruments such as financing and promoting investments in new tools such as vaccines and supply chains or targeted interventions for key populations, such as Vitamin A supplementation (ECOWAS, 2016), distribution of long-lasting insecticidal nets (EAC, 2017) as well as expansion of anti-retroviral therapy and treatments for drug resistance for TB (IGAD/Global Fund Programme, 2017; IGAD, 2016b).
Even more conspicuous is the relative under-emphasis of single payer universal health care across most regions, including the AU which instead promotes ‘a stronger private sector which can contribute to . . . achieving universal health care in an efficient and affordable manner’ (Africa Health, 2019: 5). Where an explicit vocabulary of universal health care is used, as in SADC’s 2004 Health Protocol (SADC, 1999) or EAC’s ‘Vision 2050’ (EAC, 2015), statements are typically understated and form part of a long list of health goals rather than an overarching and strategic framework or set of principles. In a similar vein, the vocabulary of health inequalities, social justice and social solidarity is also largely absent. Where the language of rights is used, it is usually framed as human rights (AU, 2016: 16).
Discussion and conclusion: advantages and limitations of regionalisation for health improvement and implications for policy analysis
By its very nature, world-regional social policy takes markedly different forms compared with national social policy. This article provides further evidence of the presence of social policy in African region-building processes. It has brought new evidence to bear regarding the presence of health within African RECs’ strategies, and in doing so has extended literatures on world-regional social policy, comparative (African) regionalisms and global health governance. Based on original research, it has shown the degree to which RECs have incorporated health into their regional-level policies and region-building strategies, and illuminated the multiple forms that African RECs’ health policies take. Our focus on health has extended the evidence base on varieties of world-regional social policy, the significant presence of multi-level health governance and policy for low- and middle-income countries, and the significance of RECs’ health policy as an important feature of African responses to disease and health systems challenges. It is outside the scope of this article to document RECs’ health policies and programmes’ impacts on policy actors and health systems, or the agentic characteristics of RECs in global or national health governance, though our analysis offers an important evidence base to build on, notably from our qualitative insights into RECs’ trajectories of development.
There is little doubt that according to the public documents and statements of RECs themselves, the advantages of regional institutions for addressing health needs concur with many of the in-principle arguments in favour of regionalist strategies set out by Yeates and Deacon (2010) earlier in this article. There is evidence that world-regional forms of international organisation create the opportunity to connect individual member states programmes and projects to longer term visions, resourcing and outcomes that transcend any one country. The RECs in our study reported several practical benefits, including maximising cross-border control of diseases, response to outbreaks, regional economies of scale and pooling of risks for large-scale, costly specialist treatment and/or diagnostic centres. Regional health infrastructures and networks of medical laboratories allow resource sharing among member states, more rapid diagnoses, health surveillance and responses – and, for some poorer states, access to services that would be impossible otherwise. According to REC statements, sharing health data and research facilitates the dissemination of best practice more efficiently, while a regional structure allows a focus on region-specific issues and priorities and local ownership in establishing a strategy, agenda and plan of action. Finally, work with development partners at political and technical levels suggests a preference by those partners for the ‘value-added’ of a regional body. Several RECs have been successful in attracting donor funding and mobilising resources on a regional scale, establishing regional centres of excellence (e.g. specialist cancer centres, research laboratories) and mainstreaming development partners’ programmes and projects into regional health plans. Our findings substantially extend research findings by Deacon et al. (2010, especially the chapter by Yeates and Deacon) and Yeates (2014b), while also providing necessary specificity and granularity mostly lacking in studies of world-regionalism emanating from the fields of comparative regionalism, global politics and global health governance.
As demonstrated in this study, the Ebola outbreak in West Africa in 2014 was a notable spur to the development of RECs’ health policy – most especially in ECOWAS but also SADC and the AU. The outbreak spurred a significant mobilisation of funds from the international community, mainly for strengthening critical health infrastructures such as regional centres for disease control, regional diagnostic facilities and other institutional infrastructures necessary to coordinate responses among member states. A decidedly regional solution was required in a context where the weaknesses of national health systems in the region and WHO responses were exposed and the transborder dynamics of Ebola posed an immediate wider risk to population health in West Africa and beyond. Unlike other health crises (including severe outbreaks of meningitis and measles) in Africa, Ebola was deemed a very real threat to the continent’s health security and to that of the world more generally.
Despite the important benefits such regionalist health strategies confer, our analysis nevertheless suggests fairly minimal strategic ambitions of the RECs as well as significant limitations of current regionalist approaches to advancing effective and progressive health reform in Africa. Some of the barriers flow from complex and fragmented organisational structures, lack of resources and an absence of strong political leadership exemplified by the lack of dedicated and powerful Health Directorates. However, we argue that many of the limitations flow more fundamentally from the underlying normative logic of the RECs themselves, namely, that ‘health’ is justified in terms of instrumental and productivist logics (growth and economic development), rather than in terms of social justice or normative goals such as the right to health. This social policy paradigm is instantiated by the fact that the RECs are first and foremost economic partnerships.
Indeed, while the economic impacts of infectious diseases and pandemics on the productive capacities of African populations have been undeniably devastating, the narrowness of the social investment response drives priorities and shapes objectives which, we argue, weaken the development of a more long-term and sustainable world-regional health policy. A principal example in this regard is the absence of universal health coverage as an overarching goal; at best, it is framed as one among many goals. Rather than investing in comprehensive and community-based health programmes which tackle some of the wider determinants of poor health, this economic rationale means that RECs’ practical work is systematically driven by the defined short-term issues and prioritisation of those (working age) populations most needed for economic development. It has led to ad hoc and reactive responses which, as ongoing health statistics reveal, have proved insufficient for addressing the complex health needs and challenges of the continent.
Few, if any, of the RECs appear to be challenging or overcoming the legacy of vertical, disease-specific approaches to health care. Instead, policy instruments appear to favour outdated ‘silo’ programmes developed in a ‘non-political’ vacuum. The result is myriad disease-specific programmes and structures existing within and across each REC, sometimes in duplication, as donors scale up their preferred interventions in several different countries. The RECs’ health policy seems to be driven largely by piecemeal donor funding which has ‘chased’ new scientific and technical discoveries, especially for drugs and medical supplies, rather than funding broader health care infrastructures. This approach distorts and diverts from long-term planning; the patchwork of projects and programmes accentuates the large intra- and inter-regional inequalities.
Moreover, the approach is out of step with current recommendations and discourses from both the Washington and Geneva international development organisations and European bilateral donors, which are increasingly emphasising health systems development, SWAPs and primary health care as the bedrock of health services expansion (WHO, 2010, 2018). While many UN institutions, and the WHO and ILO (International Labour Organization) in particular, have for a long time promoted equitable access and strong universal health systems founded on the human right to health, the new global commitment to ‘health for all’ signals a significant departure from targeted interventions. The new drive to bring universalism to the fore is perhaps best exemplified in the 2015 Agenda for Sustainable Development. However, this step change is not articulated forcefully across the RECs, which, despite some advances, ultimately do not incorporate the SDGs’ emphasis on universal health care. The lack of attention to human resource capacity and the possibilities afforded by greater regional pooling of health workforces is just one example of the gaps which flow from a lack of planning or systems coordination.
However, the emphasis on global public-private partnerships, private-sector actors and philanthropists may not be merely the result of ‘chasing’ the available funding; it may in part flow from the normative view that the state is seen largely as a ‘last mile implementer’. We observed that private and philanthropic donors are viewed by most RECs as offering more flexible resources and innovative development solutions – despite growing criticism that new donor funding is undermining efforts to create more planned, systemic and sustainable health reforms (Youde, 2018). The lack of visible engagement with civil society organisations or equivalent stakeholders by most RECs is especially noticeable in this context. Despite occasional statements about welcoming their involvement, there is little indication that this is a priority. Arguably, this economically driven productivist approach risks undermining efforts to democratise RECs, increase government accountability and sustain greater regional activism to address urgent health goals that have been so much a part of civil society activism (Berrón et al., 2013; Olivet and Brennan, 2010).
In this sense, the African RECs’ approach to health policy predominantly as a matter of industrial strategy and economic growth differs from rights-based approaches seeking to tackle inequality, political exclusion and alienation. Operating outside the UN system and thus also its normative human rights framework further confounds this situation. Against this background, an absence of commitment to citizens’ rights to health enshrined in regional law and enforcement mechanisms is, perhaps, unsurprising. More disconcerting is that, despite the flagship project of Agenda 2063 (AU, 2015), the African Continental Free-Trade Area (ACFTA) that was launched in March 2018 contains no social clause, social policy agenda or other ‘positive’ forms of integration. Indeed, ACFTA promotes the goal of economic integration and attendant degrees of freedom mainly for cross-border capital movement. It reinforces some of the indications of this study and may signal continued direction of travel.
Our finding that RECs differ in relation to the scale and nature of activities they undertake within the ambit of regional health policy is not, we suggest, only to be understood just in terms of numbers of members and size of the regional community being built, it is also about different mandates and varying financial and political resources available to them. In this, it matters that ECOWAS has a regional hegemonic power in Nigeria and that SADC has one in South Africa (even if SADC is effectively dependent on Northern donor funding and South Africa is as much preoccupied with its relations with other regional hegemons through the Brazil, Russia, India and China (BRICS) alliance as it is with its partners in the SADC region (Yeates, 2019)).
Finally, this study speaks to the growing interest within both social policy and development literatures in understanding the extent to which the traditional theories and models of comparative welfare policy and advanced welfare capitalism are analytically applicable to the developing and transitional worlds of the South (Surender and Walker, 2013). The historic and relative weakness of the state in lower- and middle-income countries has made it susceptible to exogenous ideas and influences and, as highlighted above, opened up spaces for external actors to shape social welfare. As demonstrated in this study, the health sector relies more than most on international donors and actors who exercise a discernable influence over world-regional health policies and approaches. In a context where social policy analysis is increasingly questioning how relevant ‘Northern’ classical political economy models (which emphasise the nation state, class mobilisation and democratic feedback loops as explanatory variables for determining policy) are for understanding welfare arrangements in the South today, and most attention until now focusing on the role of powerful Western bilateral and multilateral organisations, our study highlights the presence of a ‘new’ multilateral institutional actor not yet accorded sufficient attention in the health or wider social policy literatures. Given the new and potentially significant role of African regional governance institutions in health and welfare arrangements that this research article has drawn attention to, a key research task will be to develop theoretical models that capture and explain these institutions’ role(s) when considering the construction, evolution and transformation of health and wider social welfare arrangements in Africa and across the Global South.
Supplemental Material
sj-pdf-1-gsp-10.1177_1468018120961850 – Supplemental material for Southern social world-regionalisms: The place of health in nine African regional economic communities
Supplemental material, sj-pdf-1-gsp-10.1177_1468018120961850 for Southern social world-regionalisms: The place of health in nine African regional economic communities by Nicola Yeates and Rebecca Surender in Global Social Policy
Footnotes
Acknowledgements
The authors thank the anonymous referees and Editors of this journal for their helpful comments on an earlier version of this paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preliminary research for this paper was carried out with support from the UK Economic and Social Research Council (ESRC), Grant Ref. ES/L005336/1, and further developed with support from The Open University and Oxford University.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
![]() .
.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.