
Abstract
Summary
In Québec, social workers face numerous psychosocial risk factors affecting their psychological health, owing to staff shortages, work overload, and lack of recognition within the context of ongoing organizational restructuring. This study uses a systemic framework of individual and collective strategies to analyze those that enable social workers to manage the psychosocial risk factors they face and stay at work. In a qualitative exploratory study conducted between 2020 and 2022, 11 semistructured interviews were conducted with social workers (8 women and 3 men) from different intervention sectors in Québec.
Results
The results reveal that social workers feel unrecognized in interdisciplinary teams. They are overburdened by the clerical nature of the tasks imposed, which distort their profession and affect their clinical judgment. Individual levers and strategies favored include love of the job and adaptability, self-control, prioritizing emergencies, and working overtime. Collective strategies, involving colleagues, seem to encourage social workers to stay at work. Yet the organization of work, based on a standardized vision of social practice, threatens this work collective.
Applications
It is important to consider the work collective as a resource that can promote wellbeing at work and retention of social workers. Establishing conditions at interpersonal and organizational levels would help prevent obstacles to the deployment of strategies that mobilize the collective. Ultimately, a systemic approach to social workers’ health protection strategies would ensure the sustainability of interventions aimed at promoting the psychological health of social workers.
Keywords
Introduction
In Quebec, the profession of social worker encompasses occupations such as social worker in the strict sense, along with social work technician, psychoeducator, specialized educator, delinquency worker, and marital and family therapist (Rondeau & Commelin, 2005). Generally, in this Canadian province, qualifying for this profession requires a college diploma. Additionally, for certain positions with more responsibilities, such as social workers and psychoeducators, an undergraduate or graduate degree may be required. Regardless of their level of education, these professionals can work independently or within diverse public and private institutions, including those providing healthcare and social services (RSSS), schools, correctional facilities, and community organizations (Gouvernement du Québec, 2024). In 2022, over 32,000 people held such jobs (Gouvernement du Québec, 2024). The social work profession, underpinned by the helping relationship, involves intervention with an individual, group, family, or community. Its core values are social justice, equality, and human rights (Oliver, 2013). However, the practice is fraught with paradoxes (Chénard & Grenier, 2012; Gusew &S Berteau, 2011). This can be seen in the gap between the socioprofessional and organizational context, which is “organized, planned, framed, hierarchical, supervised and controlled” (Gusew & Berteau, 2011, p. 5), and the intervention context, which is characterized by uncertainty and gray areas (Gusew & Berteau, 2011).
Social intervention is marked by gender relations. It is associated with innate, so-called “feminine” qualities, and considered care work involving service, care, and support in the domestic sphere (Cresson & Gadrey, 2004). In addition to the emotional labor inherent in care work, arising from daily interactions with the suffering of others (Hochschild, 2003), the profession is characterized by numerous psychosocial risks at work, caused by repeated organizational restructuring (Sarrazin, 2014). These reforms, which value relationships of power and hierarchy, associate the profession with marginalized female workers and female-dominated jobs (Grenier et al., 2021). For example, working conditions and remuneration are lower than in male-dominated occupations such as construction or primary industries (Gosselin, 2021). This phenomenon seems widespread in care professions, where the notion of vocation justifies lower recognition and dehumanizing management practices (Benoit et al., 2022; Houston, 2016). Moreover, the concept of recognition has been extensively studied by Honneth (2008), who proposed three forms of recognition: (1) positive or affective consideration; (2) legal rights; and (3) social esteem from a community of interest. This last form of recognition appears to be the most compromised in the current context of social intervention work, as consideration given largely depends on a person's performance and individual skills (Honneth, 2008). Therefore, Houston (2016, p. 10) argues that social work and its fields of activity, in addition to being undervalued, are “despised by modern society.”
Several studies have shown the impact of organizational restructuring on social workers’ occupational health, particularly their psychological health (Bourque et al., 2018; Lavoie, 2018; Ravalier et al., 2021; Richard & Gervais, 2018). Many hazards identified in these studies constitute psychosocial risks (PSR). These risk factors, linked to work organization, management practices, employment conditions and social interactions, tend to adversely affect individuals’ physical and psychological health (Alcaraz-Mor et al. 2021).
Until recently, however, Quebec's occupational health and safety regime did not oblige employers in the health and social services sector to take action to prevent PSRs (Vézina, 2018). On the one hand, PSRs were unrecognized and therefore made invisible in the Act respecting occupational health and safety (AOHS). On the other hand, this sector was never considered a “priority” under the AOHS, resulting in few inspections and no obligation for employers to implementing prevention mechanisms (Lerouge, 2022). Recently, important changes have been made to the AOHS, 1 including explicit stipulation of the obligation to prevent PSRs and harm to psychological health. Consequently, employers’ initiatives to prevent these risk factors need to be strengthened (Vézina, 2018) and targeted at different levels of intervention, given the complexity associated with preventing PSRs (Martin et al., 2016; Petit et al. 2011).
Studies have shown that social workers are not passively enduring PSRs at work but rather are deploying strategies to address these risks (Astvik et al., 2021; Barbe & Grenier, 2022; Blanc, 2016). For example, in response to work overload and lack of resources, social workers demonstrate vigilance (Larivière, 2008), engage in forms of resistance (Astvik et al., 2021) and make use of digital technologies (e.g., email and videoconferencing) to maintain efficiency and professional connection. While these tools can help these workers navigate daily constraints, they are also used to mitigate the malaise associated with deteriorating working conditions and the resulting loss of meaning (Blanc, 2016). Understudied in the literature, these strategies can shed light on protective factors and obstacles to the implementation of organizational prevention interventions that are adapted to social workers’ work. Therefore, it is important to recognize social workers’ strategies and highlight them within organizations.
This article contributes to existing knowledge by clarifying how PSRs interact with the individual and collective strategies that social workers use to protect their health and remain in the profession. It also prompts reflection on preventive, equitable, and sustainable interventions in occupational health.
Organizational Restructuring and Psychosocial Risks: Effects on Social Workers' Psychological Health
Over the past decades, Quebec's public institutions have undergone profound changes, including workplace reconfigurations and broader organizational restructuring. These changes in the world of work have been driven by New Public Management (NPM) (Diefenbach, 2009). NPM is a reform aimed at improving the effectiveness and efficiency of public administrations (Lapuente & Van de Walle, 2020). Regarding its new public service management framework, the Government of Quebec stated (Gouvernement du Québec, 1999, p. 1): “The Administration must be simpler, more efficient, faster, focused on citizen service, and evaluated more on the basis of results to be achieved than on rules to be followed.”
With the primary goal of cost reduction, NPM has gradually taken root in the public sector by emphasizing the use of management systems focused on resource economy and the needs of users rather than of producers (Jetté & Goyette, 2010). As Sarrazin (2014) points out, in the health and social services network (HSSN) specifically, work is being transformed both structurally (e.g., the merger of institutions) and functionally (e.g., the redefinition of roles, mandates, and responsibilities).
Several studies that examined the impact of these changes on social workers’ health have found a loss of autonomy and ability to exercise clinical judgment, along with overload and intensification of work (Bourque et al., 2018; Le Pain et al., 2021; Ravalier et al., 2021; Shier et al., 2018). Bourque et al. (2018, par. 9) showed that social worker distress is: “the reflection of political and economic changes leading to the abandonment of the social and professional values to which these actresses have committed themselves: the human cause.” These changes, grounded in productivist principles typical of male-dominated industrial sectors, reinforce gendered divisions of labor by privileging productive over care work (Kergoat, 2005). They thus contribute to the nonrecognition of work performed predominantly by women, and to a loss of meaning in work (“profits take precedence”). Studies have shown that by nature, social workers’ work is associated with great distress (Ravalier et al., 2021), partly owing to an excessive workload (Acker, 2012; Richard & Laflamme, 2016). Further, the new efficiency-based organization of work, driven by NPM, intensifies and accelerates intervention practice (Le Pain et al., 2021; Rey et al., 2020), causing suffering for professionals (Acker, 2012; Le Pain et al., 2021; Richard & Laflamme, 2016; Shier et al., 2018). In addition, a survey conducted by the union that represents social workers (APTS, 2021) shows that, on average, 76.4% of social workers reported psychological distress in connection with their work.
Finally, other studies argue that social workers’ distress stems from changes in their relationship to work and their employer (Auclair-Lemire, 2016; Blanc, 2016; Ravalier et al., 2021). Isolation, role conflicts, lack of support, and insecure work situations thus contribute to ill-being among social workers (Blanc, 2016; Ravalier et al., 2021).
Strategies Deployed by Social Workers in Response to PSRs
In response to the psychosocial risk factors described above, Quebec social workers deploy various approaches and coping mechanisms, presented in this section.
Individual Strategies
First, social workers may come to accept—and ultimately endure—workplace hazards such as the standardization of practices and the imposition of managerial logic, particularly in the wake of organizational restructuring (Roy et al., 2024). Boucher et al. (2018) argued that although social workers adapt to such changes, they often harbor a distrust of management, which can lead to both individual and collective disengagement. When these risk factors are more pronounced, social workers may deploy withdrawal measures such as isolation, absenteeism, and premature retirement, or may even leave the profession altogether (Archambault, 2017; Bourque et al., 2024; Grenier et al., 2016; Larivière, 2008).
In response to a loss of meaning at work and perceived suffering, social workers adopt defense and control approaches. Auclair-Lemire (2016) identified strategies that include adjustment, negotiation, recognition-seeking, and resistance. Adjustment means synchronizing self-perception with organizational expectations, while negotiation refers to acting consistently with one's own values, without opposing the employer's directives (Auclair-Lemire, 2016). Recognition-seeking consists in focusing on recognition from users and colleagues yet believing that the employer invalidates their work. Similarly, Ravalier et al. (2021) showed that service users’ recognition of social worker professionals helps them cope with the challenges of their profession. Further, social workers display resistance by openly rejecting, adjusting, and manipulating assigned tasks (Astvik et al., 2021; Auclair-Lemire, 2016; Bourque et al., 2019). Richard and Laflamme (2016) argue that the suffering is inherent in the current working conditions imposed, forcing social workers to develop defensive and disengagement strategies to “survive.”
In her survey on conditions of practice in social intervention, Bureau (2018) found that most strategies are deployed clandestinely. Social workers thus underreport overtime and circumvent rules to save time or respond to people in distress.
Further, individuals deploy strategies to compensate for what the work environment or team cannot provide (Larivière, 2008; Pelchat & Malenfant, 2004). Such practices include vigilance in situations of work overload, investment in projects defined by social workers, and mechanisms for managing ancillary tasks (e.g., statistical reporting). Further, to avert malaise linked to the under-recognition of their profession, some social workers decide to invest in their career development (university studies, mobility to a higher position) to ultimately benefit from superior working conditions (Gusew & Berteau, 2011; Larivière, 2008).
Social workers may also adopt silent strategies, for example not expressing their concerns and criticisms of work (Morrison, 2014). Regarding the opposition between silent and “voice” strategies (Astvik et al. 2021), practitioners mobilizing “voice” strategies enjoy more positive organizational resources, experience more positive attitudes (job satisfaction, organizational commitment, and retention) and better health than those that opt for silence strategies (Astvik et al. 2021). Further, switching from silence to voice is linked to more positive organizational resources, attitudes and health, while switching from voice to silence appears to have the opposite result.
Collective Strategies
Strategies for modifying working conditions that cause ill-being are often collective: notable examples include dialogue between colleagues (Parazelli et al., 2017) and mentoring of less experienced colleagues (Ravalier et al., 2021). Digital communication technologies (e-mail and videoconferencing) can help social workers reconnect with the collective aspect and rediscover pleasure in work (Blanc, 2016). Consequently, strategies involving interpersonal relationships act as “social capital” in the workplace (Stetten et al., 2018). These strategies help social workers to bridge the resource gap (Ravalier et al., 2021) and reclaim their collective practices.
Grouping at the workplace, for example, in a union, can counter the issues created by NPM (Barbe & Grenier, 2022), social workers thus build a space to construct meaning at work (Faulkner, 2015) and fight for social recognition (Caillouette et al., 2013). Participating in a union collective action enabled social workers to enhance the recognition of their profession (Barbe, 2019). The grouping of social workers within formal (e.g., union) and informal (e.g., social networks) structures is another negotiation strategy in response to organizational constraints (Roy et al. 2024). Unions offer support and innovation in improving working conditions for social workers (Aronson & Sammon, 2000). Further, social networks have become a discussion space where social workers can compensate for the lack of institutional support (Aronson & Sammon, 2000; Ravalier et al., 2021).
Framework for Analyzing Social Workers' PSR Reduction Strategies
The studies reviewed highlight the need for a holistic understanding of social workers’ strategies to inform the development of PSR prevention interventions. We therefore propose a systemic framework based on the concept of regulation strategy, defined as “behaviors, know-how, and attitudes that individuals mobilize to maintain a balance between who they are and their environment,” including organizational expectations (Major & Vézina, 2011, p. 50). While this article emphasizes collective approaches, it is also important to acknowledge a range of individual strategies employed by social workers, such as commitment, coping, resilience, self-compassion, self-care, and individual professional agency.
Our framework also incorporates the concept of room for maneuver, referring to the space in which individuals can adjust their work to maintain a balance between their health and the achievement of work objectives. The strategies workers deploy reflect how they navigate tasks, depending on contextual levers and constraints (Major & Vézina, 2011), including PSRs (Alcaraz-Mor et al., 2021; Vézina & Chénard, 2016), and can be individual or collective.
Collective strategies are analyzed through the lens of the collective organization of work, or work collective (Caroly & Clot, 2004), defined in the French ergonomics literature as a group sharing a common vision of quality work and the rules to ensure it (Caroly, 2011; Caroly & Barcellini, 2013). Although individual strategies play a role, the work collective offers broader room for maneuver and is central to understanding the profession and promoting a sustainable balance (Caroly & Clot, 2004).
This article therefore aims to:
Identify the PSRs social workers face and the strategies they use to address them and Analyze how these strategies relate to their work, interpersonal relationships, and health.
Methodology
Based on a qualitative exploratory design (Boughzala et al., 2019), the study was carried out between 2020 and 2022 in partnership with Regroupement, Échanges et Concertation des intervenantes et formatrices en social (RÉCIFS) (Network for Grouping, Dialogue, and Coordination of Women Practitioners and Trainers in Social Work, our translation), a group of professional social workers in Quebec. An invitation to participate in a semistructured interview lasting around 60 minutes was sent out via the organization's private Facebook group, which served all RÉCIFS members. The initial design also included direct observation of work activity, which was precluded by the pandemic.
Purposive sampling (Fortin & Gagnon, 2016) was done with two participation criteria: holding a college or university degree in a related specialization (social work, special education, delinquency, psychoeducation, or psychology) and having at least 6 months’ work experience in the trade.
Semistructured interviews were conducted by the lead author on themes such as participants’ perception of the main psychosocial risks at work and the means they used to cope with them. The interviews were stopped when the data sampling did not provide any new information to answer the research question (Pires, 1997). The interviews were conducted by videoconference, given the health regulations in force. The audio recordings were transcribed with the participants’ consent. The university ethics committee approved this research project (2021–3337), and every precaution to protect data confidentiality was taken throughout.
A total of 11 full-time social workers took part in the study, comprising eight women and three men (Table 1), in line with the predominance of females in the profession. To protect the participants’ confidentiality, a code was assigned according to the chronological order of the interviews (P1, P2,…, P11). All the participants held diplomas or degrees in social work, as reflected by their job titles: social worker (n = 2), social work technician (n = 6), and special education technician (SET) (n = 3). In the Quebec context, social work technicians typically hold college-level qualifications and provide front-line psychosocial services under the supervision of a licensed social worker, while special education technicians support individuals with behavioral, emotional, or developmental challenges, often working in schools or care settings. The participants represent different sectors of intervention: youth (n = 4), intellectual and physical disabilities or autism spectrum disorders (ID/DP/ASD) (n = 3), the elderly (n = 1) or people losing their independence (n = 1), and general social work with multiple clienteles (n = 2). Thus, most participants were from the health and social services sector (HSS) (n = 7), while others worked within community organizations, private organizations, or school service centers.
Profile of Participants.
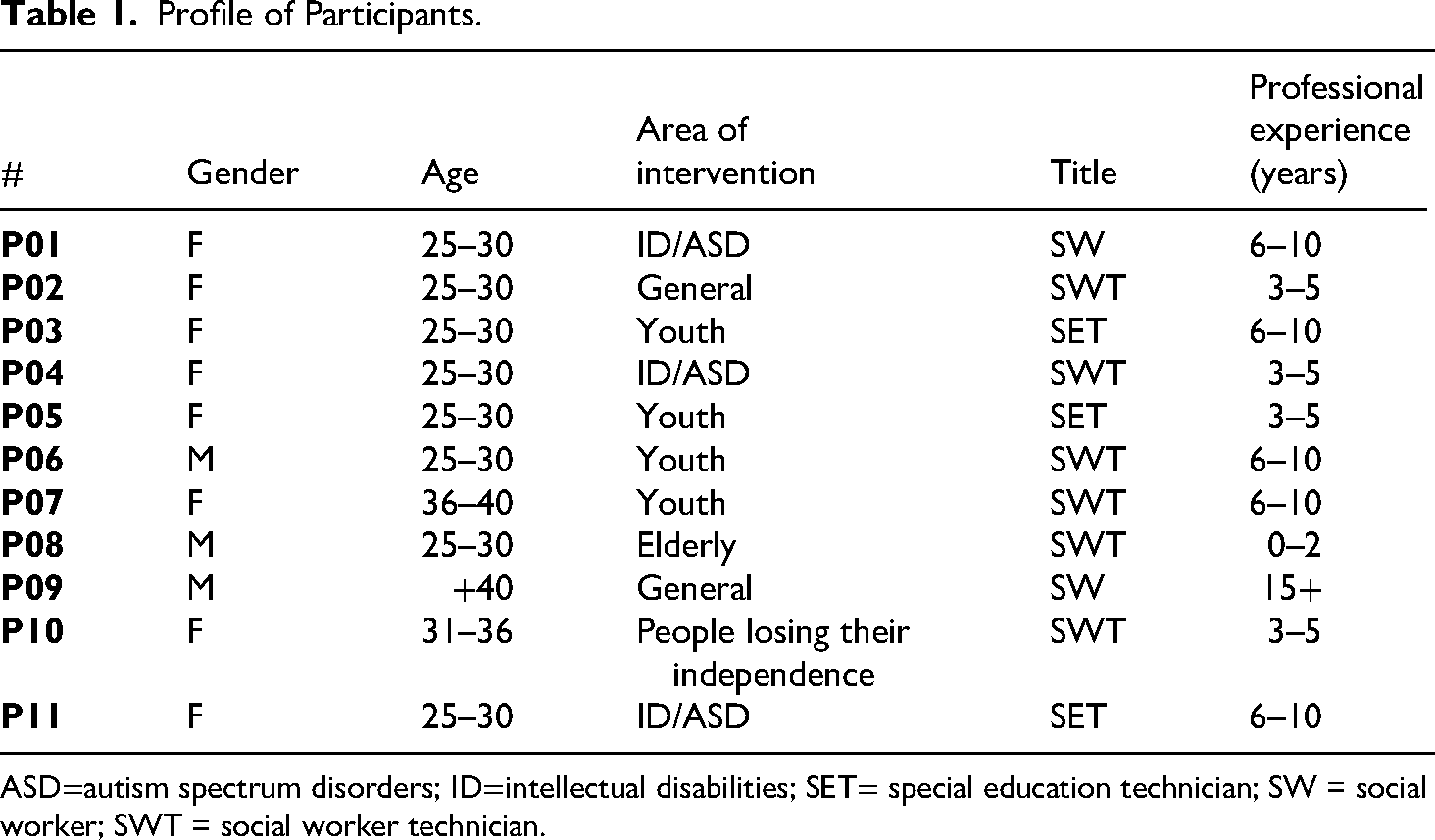
ASD=autism spectrum disorders; ID=intellectual disabilities; SET= special education technician; SW = social worker; SWT = social worker technician.
All the interviews were analyzed by the lead author and her research supervisor as part of her master's thesis to ensure the internal consistency of the data (Huberman & Miles, 2002). The transcribed interviews underwent thematic analysis using NVivo software. The first coding process was exploratory and nonformalized, in order to identify the main fragments in the verbatim transcripts (Paillé & Mucchielli, 2021). A second, more specific coding stage followed, to determine the main and significant themes that emerged from the interviews. This coding suggested thematic categories linked to both the initial concepts of the conceptual framework and the themes emerging from the data collection, in order to preserve flexibility specific to the qualitative approach (Sabourin, 2009).
Results
This section presents participants’ perceptions of the PSRs experienced in social work, along with the main individual and collective strategies mobilized, with emphasis on gender dynamics given the composition of the sample (eight women and three men). Participants are characterized as follows: (participant number-title-gender).
Psychosocial Risks
Various psychosocial risks emerged from participants’ discourse related to perceptions of work organization and relations with managers, colleagues, and service users.
An Ever-Increasing Workload
The social workers reported tension between relational and human work, and the organizational performance demands of NPM: “Most of the time, you feel powerless because whether you’re a social worker or a technician, you’re working for the network and not for the user” (P08-social work technician-M). This type of hazard is by far the most frequently observed: it was mentioned in all the interviews. The changes brought about by the reforms within the establishments have intensified social worker's work, as one participant explained: “Since the merger with the hospitals, the demand for tasks is much more difficult, the workers are at the end of their rope, too many things are asked of us” (P07-social work technician-F). This phenomenon stems from a long-standing staff shortage.
This lack of resources has increased the workload considerably. Several participants complained of unstable work teams and being unable to exchange ideas and strengthen relationships due to insufficient time: “We don’t always have the opportunity to talk to each other during our shifts because it's often a rush … it's difficult and it takes time to develop friendships …” (P05-SET-F). This instability inevitably hinders social workers’ abilities to maintain a work collective.
The social workers find themselves alone or accompanied by different colleagues every day, procured either from the recall list or from personnel agencies, because the resources in place do not allow for sufficient recruitment to stabilize the work team: “Recruitment everywhere at the HSSN is difficult at the moment. In terms of the balance and stability of the floor, this plays a role. We’re starting to get used to it, we’re adapting with what we’ve got …” (P11-SET-F).
The lack of sufficient resources at work has a direct impact on the workload demanded of social workers, forcing them to increase their workload to compensate for staff shortages: “Since I joined the team, I haven’t had a stable team. If you don’t have a stable team, if your team is missing players, then you have to run around” (P08-social work technician-M).
Standardization of Work and Record Keeping
Participants describe how NPM has led to standardization of practices without added value: “The OCCI 2 is a long document to fill in … We have to do it because we have no choice, but does it help in our practice?” (P10-social work technician-F). This standardization includes the obligation to measure the work done via indicators: “We’re supposed to do three stats a day … two in person and one by phone. But in all that, you have to make notes and calls, and I’d have to do my evaluation pretty much all the time” (P01-social worker-F).
Social workers are expected to support people facing difficulties by working with them. Standardization makes this relational work impossible, as social workers grapple with numerous administrative and clerical tasks. The many organizational prescriptions, linked to record-keeping, progress notes, monitoring intervention plans, etc., weigh heavily on their work: “Lots and lots and lots of administration. Little intervention. It's something everyone in the HSSN hates, because we’d really like to offer more, but we don’t have the time” (P07-social work technician-F). Most of the participants feel powerless in this situation. Considerable time is lost not only in writing up numerous follow ups, but also in entering extensive notes in users’ files: “I have a lot of trouble keeping up to date with my evaluations … I manage to keep up to date with my interventions, my notes, my calls and my statistics … But doing evaluations on top of that doesn’t work” (P01-social worker-F).
Some social workers work with the computerized clinical pathway tool (OCCI), designed to help them make decisions in line with public standards for clienteles (Touchette, 2018). However, the participants think this tool hinders their work: “When you do the OCCI it's really long. You have to know the needs and everything, so it's really more bureaucratic. The tool gives us a rating. The OCCIs are calculated and based on this, a program receives an amount” (P01-social worker-F).
Some participants mentioned that the standardized aspect of this tool distorts the profession, since it is mainly used to obtain funds for their program. The organization of work is increasingly based on a bureaucratic logic, where accountability and funding needs supersede providing care to users: “The statistics we fill in are just used to get money, to prove that we need it … But then again, that makes us focus less on the user” (P01-social worker-F). This need to settle a maximum number of cases—that is, to process as many files as possible, often at the expense of service quality for beneficiaries—creates inconsistency in social workers’ practice: In these situations, you feel powerless, and that's upsetting because you know the assessment and you’ve done it, you’ve told everyone, but no one wants to hear you because that's not the network's objective … it's to reduce the number of people in hospital or avoid relocations. (P08-social work technician-M)
Several participants believe that the tool mostly benefits the HSS. Their clinical judgment, central to their professional practice, then becomes subordinated to the tool: It's really not human. You put a number on a person according to their physical and cognitive skills … the judgment is really based on the number. I don’t think it's professional or ethical. In the end, you’re the one who puts your name on it, you’re the one who fills it in. (P08-social work technician-M)
Tensions Between the Code of Ethics and Organizational Guidelines
The NPM-driven restructuring of social work practice also undermines the normative framework of the profession, as ethical standards often clash with managerial directives. Administrative demands from managers create tensions with social workers’ professional obligations, which they perceive as particularly burdensome due to the volume of tasks and the level of detail required in case handling. Professional obligations are thus occasionally flouted in the interest of meeting organizational expectations of productivity: “Some do a two- or three-page assessment because they’re short on time. But then again, does that satisfy the [professional corporation]? No, because it's not complete enough” (P01-social worker-F).
The deadlines imposed by the professional corporation also represent a psychosocial hazard: “You can’t afford for your assessment to be late, otherwise you’re in breach of an order, and therefore illegal in this person's life …” (P07-social work technician-F). Imposed service user response times, between 24 and 48 h after receiving a call or e-mail, reinforce the feeling of accountability: “If we don’t meet the deadline, the service user could complain to the Complaints Commissioner, claiming that we’re not returning their calls. So you really have to ‘guarantee’ that” (P07-social work technician-F).
Insufficient Managerial Support
Some managers apparently do not offer social workers support, even in crisis situations: “If anything happens with the users, my boss won’t be there to support me” (P06-social work technician-M). Further, managers’ attitude may be harmful if their decisions and imposed directions clash with social workers’ concept of quality work, leading to a conflict of values: No matter how much I told my boss, she said ‘no! That's the game, you relocate the elderly person.’ At that point I felt helpless …That's when you really question what you’re doing, and your role as a caregiver: Are you there for the family? Are you there for the person? Are you there for the network? Who are you there for in the end?. (P08-social work technician-M).
In addition to these internal tensions, the participants also reported problematic relations with managers. One participant even questioned the meaning of their work: A real intervention is to intervene directly with the user, to see them regularly, to ask them how they’re doing, to be human, I’d say. The least real intervention is the steps we take for the user [such as] notes and follow-ups. Unfortunately, our work leads us more toward this type of intervention. (P08-social work technician-M)
Unpredictable, Even Violent Service Users
A final form of psychosocial hazard reported concerns the clientele, whose specific characteristics influence the social workers’ work environment. Participants underlined the high unpredictability of interventions adapted to users’ distinct needs: “A 100% easy day has never happened to me because you often manage other people's emotions, you manage crises, the unexpected … Sometimes we called the fire department” (P03-SET-F). In the rush of your work, you often have situations that require you to react immediately. (P05-SET-F).
This unpredictability compromises social workers’ safety in cases of violent or aggressive behavior, instilling a climate of fear in the workplace: “It's crazy how scared people are, it's not normal” (P02-social work technician-F). Some people instinctively flee crisis situations, fearing that they will be attacked: “When the attack was going to happen, you could feel it, and the worker who was with me just hid in the kitchen” (P02-social work technician-F). Most of the people we met had experienced or witnessed episodes of violence: Psychological and verbal violence is our daily lot. Physical violence is rarer, but when it happens it causes a lot of damage … broken bones, physical and psychological damage. Some people who this happened to never came back to work. (P05-SET-F).
Protective Factors and Strategies Mobilized
Participants also shared their perceptions of protective factors in their environment and strategies for coping with these hazards.
Individual Level
First, the strong enthusiasm for social work among all participants seems to influence how they experience PSRs. The social workers who claimed to enjoy their work, feel recognized by service users and make a difference in people's lives also reported high satisfaction: “I love what I do so much that it doesn’t seem like a burden. […] I feel that I’m useful, that I’m making a difference” (P03-SET-F). Despite the many difficulties, their love of their profession motivates them to continue: “In five and a half years, I’ve never felt at the end of my rope … I love my work, so it helps me get through the difficulties” (P11-SET-F).
In addition, social workers mentioned specific capabilities that help them manage hazards. Adaptability is one example. Practitioners thus learn to adapt to the ever-changing environment of social work. Participant 1 described how she has gradually adapted, and the ensuing self-confidence. Similarly, one participant described her evolution within a professional team: “When I started out, I wasn’t really comfortable expressing my point of view. But as time goes by, the bolder I become. I’m not an expert in education either, but I can come up with good ideas” (P03-SET-F). To cope with sometimes contradictory tasks, participants rely on self-regulation practices. First, setting limits is a fundamental individual skill that helps social workers stay at work. This self-control also implies letting go: “I was able to cut things off. Listen, I couldn’t do everything today … I only work 7 hours, so that's normal” (P01-social worker-F).
In response to the lack of recognition within the profession, another form of self-control strategy, reported solely by the male participants, entailed furthering their education to attain positions that offer better working conditions and, consequently, greater professional recognition: “But that's almost one of the reasons why I’m doing my Bachelor's … I think I could be more competent than my boss who asks me to wash lockers. I don’t want washing lockers to be an option at my job [laughs]” (P06-social work technician-M). Obtaining a university degree lets participants prioritize areas of intervention that are better recognized. More broadly, changing practice settings may also represent a deliberate strategy for gaining professional recognition. For instance, one participant has rejected repeated offers of positions in the HSSN due to difficult working conditions: You see, even if I could go back to work in the health and social services network tomorrow morning, I wouldn’t go. No way. The network is sick. Hugely, quite, quite sick…I’m doing more social work at the moment. I like it, that's what I do. But I don’t work in the public network. And I could work in the network, I get requests and offers as a manager. But I’m just not interested at all. (P09-social worker-M)
Finally, in response to work overload, social workers mobilize individual strategies such as prioritizing emergencies and keeping an up-to-date planner. However, the only strategy that really seems to work is to extend working hours to complete the work, which implies working overtime: “Theoretically, the schedule is from 8:30 a.m. to 4:30 p.m., but I get to work at 7:30–45 a.m. and get home at 7:30 p.m” (P07-social work technician-F). Lastly, some participants report using personal life strategies, such as skipping meals, to save time: “I often don’t eat dinner, because I’m swamped” (P08-social work technician-M). In addition, some use alcohol, drugs and medication: “I smoke cannabis … so far it's always helped me … it really lowers my anxiety” (P05-SET-F). “I was taking melatonin to go to sleep … During my post-traumatic shock I took drugs, big drugs that would just knock me out so I wouldn’t think about it” (P02-social work technician-F). All of these strategies serve to help participants manage work overload.
Collective Level
The results emphasize that support from colleagues is a crucial protective factor in coping with organizational constraints and difficult relationships with managers. All participants underlined the importance of the group in managing risk factors at the workplace. As one participant put it: “It helps to vent with someone who understands your reality” (P11-SET-F).
Social activities played an important role in strengthening bonds among colleagues and maintaining morale. Participants described how they organized informal activities as a team—for example, celebrating birthdays, going out to restaurants, or doing team activities on weekends: “This summer we had barbecues, little activities together, restaurants, things like that” (P05-SET-F). These gatherings allowed workers to get to know one another outside the pressures of work, building a sense of belonging and mutual support.
Colleagues also relied on structured or semistructured spaces for emotional and informational support. Many created Messenger or WhatsApp groups to stay in touch between shifts or to vent frustrations. Others used informal physical spaces, such as conversations around the coffee machine or retreating to an office with colleagues to cry. These spaces were seen as essential for offering and receiving reassurance: “We talk among ourselves a lot because we actually understand each other. We’re the only ones who can really understand each other and what we’re going through” (P05-SET-F). Such spaces served as a protective outlet to express emotions and share experiences in a supportive environment.
A third form of support involved adjusting work collectively to respond to colleagues’ needs and energy levels. For example, when one worker felt fragile, the others reallocated tasks to support her: “Often we tell each other when we can’t do it anymore, and our colleague takes our place. We share the work well” (P03-SET-F).
Beyond emotional support, colleagues also offered instrumental support by sharing tools and exchanging advice: “If I have questions about a situation, I’ll turn to my colleagues for an answer before I rush over to the director” (P03-SET-F). They pooled resources in a common “toolbox,” which eased daily tasks and helped new staff integrate more effectively: “In social work, we have a toolbox where we put all our forms, share them with our colleagues and keep our information for the next workers” (P10-social work technician-F).
Overall, participants viewed mutual support among colleagues as decisive in their willingness to remain in a team: “That's really what's going to make someone stay in a team or not. Support. Being able to help each other. Teams where there isn’t any, well there's turnover all the time” (P07-social work technician-F).
Discussion
The study results provide a tangible illustration of the use of a systemic framework to analyze the concept of strategies in order to better understand the PSRs that social workers face in their day-to-day work. By considering social workers’ strategies through their interactions with factors at the individual, organizational/interpersonal, collective, and macro levels (Major & Vézina, 2011), this study identifies protective factors in the form of levers and obstacles to implementing psychosocial risk prevention interventions for social workers in the health and social services sector in Quebec.
The first important contribution of this study is that it sheds light on risk factors arising from both the intensification of work inked to NPM and from heightened service user needs. The results show that the heavy workload reported by social workers stems from factors such as staff shortages, insufficient time, anticipation of overload, and lack of managerial support, which is nevertheless considered a protective factor against PSR (Martin et al., 2016). These elements create a value conflict that social workers interpret as a contradictory injunction where relational work is compromised by bureaucratic tasks (Pauzé, 2016). To protect themselves from these injunctions, social workers prioritize organizational prescriptions, which have greater short-term impacts than noncompliance with the code of ethics. Roy et al. (2024) view these responses as forms of negotiation, in that social workers voluntarily decide to circumvent the existing rules to maintain professional practice consistent with their values.
A gendered perspective offers valuable insights into the PSRs arising from heavy caseloads and client-perpetrated violence. Social work constitutes care work (Cresson & Gadrey, 2004; Müller, 2019) and is often compared to a vocation rather than a job (Iori & Nicourd, 2014). The profession is therefore affected by gender stereotypes and invisible health risks (Gonin et al., 2013; Paperman & Laugier, 2015). Professionals accept these disadvantaged work conditions, while their employers trivialize the violence and risks posed by service users, because such conditions are normalized in care work (De Gaulejac, 2009). Note that the male and female participants alike reported similar risk factors, suggesting that the gender stereotypes associated with care professions are not salient in this case.
A second major contribution concerns the key role of individual and collective approaches in helping social workers cope with numerous workplace hazards. The results indicate that social workers regain room for maneuver through protective factors and practices that emerge from their own attitudes and collaborative efforts alike. At the individual level, personal characteristics such as adaptability, resilience, work-specific skills, and previous experience act as protective factors against PSRs.
These findings affirm the idea that people need to build resistance to work constraints in order to maintain a lucid relationship with reality (Dejours, 2016). They also underline the need for social workers to demonstrate creativity and strong adaptability in their practice (Bourque et al., 2019). However, these strategies are not foolproof and may not suffice to keep social workers at work. As our results show, managing emergencies and struggling with overtime work can lead to emotional exhaustion and compassion fatigue. For some social workers, the strain is so great that they decide to reorient their careers. These caregivers lack room for maneuver to maintain a balance between their health and their work, thus compromising the protective role of their strategies (Major & Vézina, 2017).
Finally, a gendered interpretation of the strategies reported highlights that only the male participants reported self-control strategies (Gusew & Berteau, 2011; Larivière, 2008). This finding reflects their rejection of the status quo, their pursuit of recognition, and their aspiration for greater autonomy in choosing their work environment and the types of risks they are willing to assume. This avenue is worth exploring in future research.
A third key contribution highlights the importance of collective dimensions of work and the strategies that act as protective factors against PSRs reported by social workers. The collective strategies described, focusing on informal and supportive relationships between social workers, are considered essential for creating and maintaining bonds between colleagues (Chouinard & Couturier, 2006; Larivière, 2014). Our results show that this informality takes several forms, including activities between colleagues, physical and virtual discussion spaces and the establishment of informal collective rules marking the presence of a work collective (Caroly & Clot, 2004). These team activities apparently let the social workers strengthen their bonds and overcome psychosocial risks. They make it easier to get to know colleagues better, with whom they develop a bond of trust, which social workers rarely have time for during working hours. Not only do these activities let social workers disconnect from difficulties at the workplace, but they also compensate for the lack of day-to-day resources in their work. As Caroly (2011) points out, through cooperative teamwork, the work collective provides an opportunity not only to develop skills, but also to preserve and build health.
Work collectives contribute to preserving the health of social workers, notably by supporting the construction and reinforcement of their professional identity. This protective function is particularly relevant in institutional contexts such as hospitals, where social workers often find themselves in a minority position within health-dominated teams. Indeed, social workers tend to have a different vision of intervention situations than do other health and social services (HSS) professionals (Pauzé, 2016). By contrasting their roles with those of occupational therapists, nurses, or orderlies, the social workers in our study underscored this distinction. As noted by Morin et al. (2018), the “social” dimension is often relegated to a secondary status in hospital settings, which compounds social workers’ efforts to differentiate themselves from their colleagues. The shared use of a distinct professional vocabulary reinforces a sense of belonging to the social work identity, which would protect social workers from various health issues that characterize their profession (Iori & Nicourd, 2014).
Beyond these individual factors, the work collective plays a crucial role in fostering mobilization among social workers. Our findings point to two complementary ways in which this mobilization unfolds. First, confidence in the organization fosters cooperation. As Bourque et al. (2014) noted, “if this faith disappears, the willingness to cooperate diminishes and the collective is inevitably undermined” (p.106); this situation may currently be observed in the network. Second, the emergence and sustainability of the collective are strongly influenced by organizational constraints, which appear to fuel a cycle of “destructuring of solidarities between employees” (Dejours, 2003, p. 48) associated with NPM. Organizations must therefore assume their responsibilities not only by recognizing the violence and risk exposure that social workers face, but also by actively implementing sensitive and regular emotionally supportive supervision, both individual and group-based. Such supervision plays a crucial role in fostering resilience and collective strength.
Moreover, organizations have a responsibility to provide quality opportunities for workers to discuss and share experiences through both formal and informal channels, thereby nurturing a work environment that encourages mutual communication and solidarity. Currently, however, the organization of work often hinders the collective, which negatively impacts social relations and the wellbeing of social workers. Addressing these organizational shortcomings is essential to restoring effective collective action and healthier workplace dynamics.
Another important insight from this study is the adoption of a gendered perspective to examine the composition and functioning of the work collective. In a profession largely dominated by women, the work collective often consists of female colleagues exclusively. Our results suggest that this gender homogeneity may foster a shared understanding and a sense of recognition among social workers, reinforcing the collective as a potential safe space to reflect on and regulate work. However, this raises important questions about the inclusiveness of such collectives for individuals whose sociodemographic characteristics differ from those of the dominant group. How does this diversity influence the protective potential of the collective, particularly in relation to PSRs?
At the same time, numerous organizational constraints, such as heavy workloads, administrative demands, and lack of time, limit social workers’ collective ability to support one another emotionally and to develop shared strategies to manage their ever-increasing caseloads. These constraints not only undermine the protective function of the collective, but also contribute to the devaluation of the profession itself (Sanchez-Mazas & Casini, 2005), while hindering the implementation of effective PSR prevention measures (Vogel, 2015). Taken together, these findings point to the need for future research to better understand how gender dynamics and organizational conditions shape the collective's capacity to serve as a source of recognition, support, and protection for all its members.
On a practical level, this study contributes to knowledge of social workers’ work from a PSR prevention perspective at a time when all Quebec workplaces are legally obliged to identify these hazards and, generally, to implement preventive actions. The organizational, interpersonal, and individual issues highlighted in the results confirm the complexity of PSR prevention, which requires action at multiple levels (Martin et al., 2016). In addition, a thorough understanding of work is necessary to identify both levers and obstacles, by taking actual work practices into account (Coutarel et al., 2015). In this regard, our results challenge the current tendency to focus on individual interventions for PSR prevention, such as mindfulness and other activities that foster emotional detachment, resilience or stress management. Social workers already deploy diverse individual strategies that fail to protect them from work-related PSRs in the long term. We must therefore eliminate risks at source by targeting aspects such as workload, recognition, and support from superiors rather than placing the burden of the prevention approach on workers, who must adopt specific behaviors and attitudes. Developing conditions and activities that foster the emergence of a work collective, such as allocating time and space for team support and collegial exchange, could serve as an effective strategy to promote workplace health and improve the retention of social workers. This is particularly important given that the recruitment and retention of social workers is crucial, with high turnover rates negatively affecting not only team cohesion and institutional memory, but also significantly compromising the continuity and quality of care. The study findings suggest that fostering collective dimensions of work, through supportive organizational conditions, may address these challenges by promoting worker wellbeing and professional commitment. Further research should therefore explore how collective strategies can contribute to stabilizing the workforce and, in turn, strengthening the care relationship with users.
Limitations
The first limitation is linked to the fact that participants were recruited solely through the RÉCIFS private Facebook group. That being said, the final sample was diverse and provided rich insights. Second, the small number of participants (n = 11) does not allow the generalization of results, yet it supports the exploratory goal of this study. The richness and depth of the results obtained may provide avenues for further research that can examine the links between variables with more representative samples.
A longitudinal approach to the mechanisms, such as gender relations, ethnicity, and career stage, that shape the individual and collective strategies central to social workers’ work activity could add valuable nuance to this exploratory portrait. Because many strategies may be unconscious (Major & Vézina, 2017), combining direct observation with autoconfrontation interviews—where workers are invited to reflect on video recordings of their own activity to access implicit dimensions of their actions (Mollo & Falzon, 2004)—could help reveal implicit aspects of work practices (St-Vincent et al., 2014). A multiple-case study approach could allow comparison of the emergence of individual and collective strategies according to the characteristics of diverse contexts and consideration of interactions with other actors. The PSR prevention interventions could then be adapted to the specific features of the environment and the people therein. In addition, the pandemic context may have influenced the nature of certain responses, including the perception of organizational support and workload, given the great pressure exerted on all HSS staff. It would be interesting to update this portrait by measuring certain dimensions explored with a larger sample, via a questionnaire. It is essential to take stock of the health status of social worker professionals in Quebec, and to examine the link between organizational and sociodemographic variables, along with the extent of exposure to psychosocial hazards in this professional category. Therefore, given that social workers value managerial support highly, it would be worth exploring managers’ perception of hazards inherent in social workers’ work, such as emotional strain, exposure to client violence, and work overload, as well as the repercussions of PSRs on their own work and on the employer–employee relationship. Comparing the risk factors experienced by managers and social workers is a promising avenue for identifying obstacles to the implementation of PSR prevention measures. Lastly, to extend our findings on the role of the work collective, we could analyze formal and informal discussion forums (e.g., Facebook groups, community of practice forums, and co-development meetings) as a space that fosters understanding between social workers, co-development and, ultimately, well-being, to shed light on best practices related to the conditions conducive to nurturing a work collective. On a larger scale, the role of support provided by social workers’ family and friends is also worth examining further.
Conclusion
This study highlights the importance of examining the impact of tensions between the shifts in emphasis introduced by NPM and the meaning that social workers assign to their work. Organizational factors such as the current organization of work, obstacles to teamwork, and prescriptive management tools and practices that impede work activity all lead to work overload, a lack of organizational support and conflicts of values.
Our research affirms that building the work collective appears to be the most valuable strategy that social workers can adopt to address psychosocial workplace hazards. However, organizational factors and PSRs may threaten the viability of this work collective given the tensions between NPM's managerial expectations, ethical obligations, and the instability of work teams caused by staff shortages and constant turnover. Our findings suggest that the institutional organization of work harms the collective organization of work, leaving some social worker professionals with no choice but to leave their organization. By tackling the root causes of PSRs (overload, lack of recognition, and ethical dilemmas) and their interactions with social workers’ satisfaction regarding the quality of the care work provided to service users (Lévesque & Negura, 2021; Negura & Lévesque, 2022), organizational interventions could support initiatives to attract and retain social workers in the health and social service sector.
In conclusion, individual resilience is insufficient to protect social workers as they carry out their essential duties. Indeed, systemic and sustainable interventions are required, to restore their room for maneuver. Our study underscores the need to recognize the collective strength of social workers and the fundamental value of their contribution to public services.
Footnotes
Acknowledgements
We would like to thank the participants in the study, our partner organization RÉCIFS, professors Annie Camus and Martin Chadoin for their role in directing the dissertation project, and professor Amélie Guèvremont for her involvement in the production of this article. We also thank the two reviewers for their constructive input throughout the evaluation process.
Ethics
Ethical approval for this project was given by Université du Québec à Montréal (UQAM) [ref number #2021-3337].
Consent to Participate
All participants provided written informed consent prior to participating.
Consent for Publication
All participants provided written informed consent prior to publish the study.
Authors’ Contribution
RP was involved in data collection and RP, ML, and JR in data analysis and interpretation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was carried out with financial support from the Interdisciplinary Research Team Health-Gender-Equality (FRQ-SC grant) https://doi.org/10.69777/343424.
Declaration of Conflicting Interest
The authors declare that they have no potential conflicts of interest regarding the research, writing and/or publication of this article.