
Abstract
Summary
“Recurrent care,” where parents repeatedly appear in care proceedings and have multiple children removed from their care, carries a high cost in both human and financial terms. The objective of this literature review was to identify the evidence of their impact, cost savings generated, and outcomes produced for birth parents. Searches were undertaken to identify evaluations of recurrent care services involving cost savings calculations. Thirteen articles or reports in total were found, all using mixed methods approaches. Four of these were excluded due to duplication. Participants across the 9 studies totaled 844 birth parents.
Findings
This first-ever review of the effectiveness of different services to support recurrent care experienced parents found that these services can generate significant cost savings through avoiding care proceedings and placements of children taken into care. In addition, the parents working with these services have a range of positive outcomes as well as some areas (mental health needs) where more support would be required.
Applications
If regional or national funding is not provided for recurrent care services, then local authorities should seriously consider doing so themselves to benefit from the substantial savings they can achieve. More targeted psychological support is required once mothers have been enabled to meet their basic needs and re-establish trust with professionals.
Keywords
Introduction
“Recurrent care,” where parents repeatedly appear in care proceedings and have multiple children removed from their care, has been identified as a national issue for the UK that carries a high human cost, as well as a high cost for state welfare budgets: in the UK, these costs are principally borne by local government in the form of local authorities. The multiple removals of children from the same parent are also reported in countries with similar child protection systems such as Australia (Hinton, 2018; Taplin and Mattick, 2015), Canada (Novac et al., 2006), New Zealand (Office of the Children's Commissioner, 2020), and the US (Grant et al., 2014). Broadhurst et al. (2015) in their analysis of a national dataset of 43,541 birth mothers identified that recurrent care proceedings represent a high proportion of all care proceedings in England. Nearly one in four birth mothers appearing in English care proceedings are likely to go through a subsequent set of care proceedings within 7 years, with 13.2% of them being likely to go through repeat proceedings between 1 and 2 years after the initial proceedings.
It is only within the last decade that services to support birth parents who have lost a child (or children) through care proceedings have been developed, despite these parents experiencing multiple challenges stemming from substance misuse, mental health issues, and/or domestic abuse. These “revolving door” cases, whereby the same parents lose a number of children in subsequent care proceedings, represent a significant financial cost to local government in the UK as well as a high emotional cost to those involved.
Individuals with care experience have often experienced a range of adversities in life, resulting in greater challenges in their life across various aspects. They have lower levels of adaptive and cognitive functioning than their peers living at home with their families as well as more behavioral problems (Goemans et al., 2016). They have poor educational outcomes (DfE, 2020; Jay and Mc Grath-Lone, 2019) with attainment and progress being lower at each key stage of education for children who had had any social work intervention compared with those who had had no intervention and the gaps widening according to the level of social care intervention (Berridge et al., 2020). They are more likely to have mental health difficulties (DfE, 2019; Meltzer et al., 2003); to have serious behavioral problems; to misuse alcohol and drugs; and to be involved with the criminal justice system (Jones et al., 2011; Meltzer et al., 2003). Those who were in care as children are more likely to experience adverse outcomes in adulthood (National Audit Office, 2015) and have higher mortality rates (Murray et al., 2020). If we think that by removing child after child for the same reasons without addressing the same problems we are doing right by the children and the families, we delude ourselves. (Nick Crichton, retired District Court Judge, Inner London Family Proceedings Court and member of National Pause Board, 2015)
Since the issue of repeated removals to care was first formally identified around 12 years ago, a considerable number of specialist services to support these parents have been developed in the UK. These include the Pause model within England and Reflect services covering all of Wales applying top-down policy-driven approaches, along with many other smaller services developed locally from the ground up. Other broad forms of services have developed to tackle families at risk of care proceedings (including recurrent care) such as Family Drug and Alcohol Court (FDAC) schemes in London and elsewhere and midwife-led schemes targeting pregnant women on “pre-birth risk registers” or similar. In addition, the Supporting Parents virtual Community of Practice was established in 2020, funded by Public Health England, to provide a forum for discussion, peer support, training, and sharing resources for all practitioners working in this area.
A total of 73 recurrent care services have been identified across England: 28 Pause practices in 35 local authorities and independent services covering an additional 38 local authority areas, delivered by at least 29 providers. However, there are still significant gaps in provision as there appears to be no service in 49 local authority areas and there is no information about another 30 areas, which would suggest that around half of the local authorities in England do not have any services to support recurrent care experienced parents (Mason & Wilkinson, 2021).
While the Reflect services are funded at a national level, most of the locally designed services delivered by local authorities are funded directly by these authorities and are included in mainstream budgets, but a minority has no specific funding stream. Funding for services that are delivered by the third sector often rely on a range of sources, including charitable trusts and local authorities (Mason & Wilkinson, 2021). The locally designed services that do exist are, as a result, commonly under-resourced with insecure and uncertain funding, which impacts on their sustainability (Boddy et al., 2020; Mason & Wilkinson, 2021). Local authority professionals interviewed by Boddy et al. (2020) stated: “we recognise the benefits but we just don’t have the money.”
One significant reason why local authorities do not fund such services is that they fall between children's and adult’s services. Another even more significant reason is that all English local authorities have seen huge reductions in their budgets in the last decade, with their core spending power cut in 2024/25 by 23.3% in real terms compared to 2010/11 (LGA, 2024). At the same time, they have experienced huge increases in their spending on housing, which is one of their statutory obligations.
The aim of this literature review was to identify evaluations of recurrent care services and to provide evidence on their impact, the potential cost savings generated, and the outcomes, including clinical benefits, they have produced for birth parents. This article summarizes the evidence obtained from these evaluations.
Methods
This article reports on a narrative literature review undertaken using the results from database searches in February 2024. All literature was included if studies were published during any timeframe and written in English. This included articles published in peer-reviewed journals and gray literature such as evaluation reports published online. The databases used were MEDLINE, SCIE online, Social Services Abstracts, and CINAHL, supplemented by resources on the Supporting Parents website and searches using Google Scholar and Google.
The search terms used were “recurrent care” OR “repeat care proceedings” OR “repeat removals” AND “evaluation.”
Inclusion criteria were studies published within the last 15 years, available in English, and undertaken in the UK or other countries with a similar child protection system (e.g., Australia, Canada, or New Zealand). This included articles published in peer-reviewed journals and gray literature such as research and evaluation reports available online. Studies needed to be concerned with parents involved in repeat care proceedings and services supporting them, defined as being services set up to support birth parents whose children had been taken into care with the aim of preventing these parents from experiencing further child removals.
Exclusion criteria were papers on services to support birth parents who had lost children into care and/or and to support reunification where the aim of avoiding further care proceedings was not identifiable within the service design; papers involving care relating to recurrent medical conditions; business cases or needs assessments for setting up a recurrent care service; opinion pieces; and papers on reunification services or on parental needs/issues that put children “at risk” of care proceedings, since the context behind this literature review was avoiding the repeat or recurrence of care proceedings and child removals. This also resulted in the exclusion of papers on the FDAC (an alternative, problem-solving approach in cases where parental substance misuse is a key factor in the decision by a local authority to bring care proceedings) since although some of the parents involved may have experienced previous care proceedings, the service is not directly targeted at these parents and FDAC has a distinct identity as a court-based model (Figure 1).
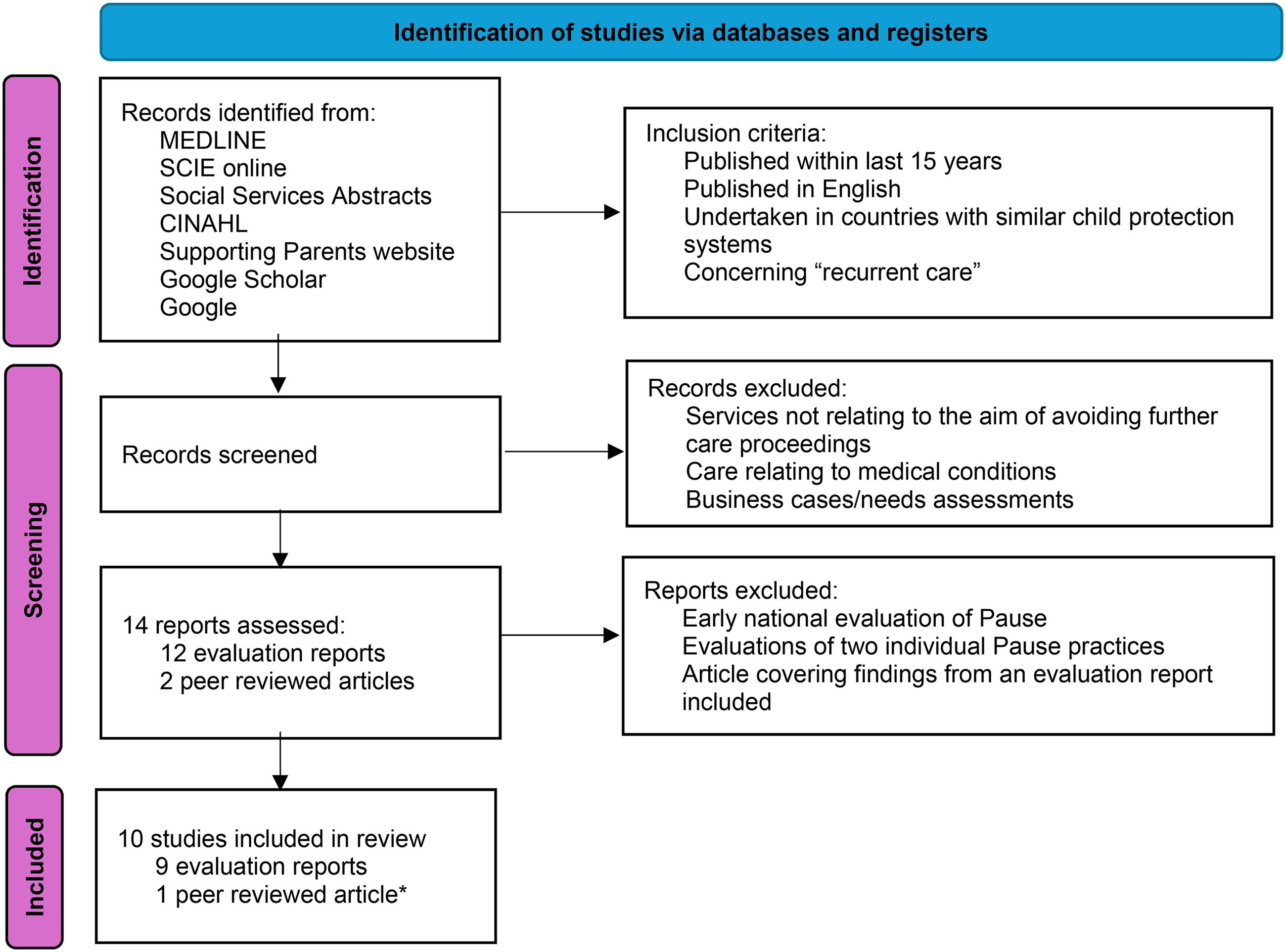
Identification of studies, including selection criteria. *Findings from the published evaluations of two of the three services reported on within the peer-reviewed article are included since the two evaluation reports contain significantly more detail than the article, but the evaluation report on the third service is not available online.
A total of 14 articles or reports were identified, with the majority using mixed methods approaches to evaluate services. All were from the UK and most were externally and independently conducted evaluations. Four studies were excluded: one was an early evaluation of Pause and two were evaluations of an individual Pause practice—only the national and final Pause evaluation in 2020 was included to avoid over-representing Pause findings. The fourth excluded article covered findings from the full evaluation report that was already included. It should be noted that findings from the published evaluations of two of the three services reported on by Cox et al. (2020) are included since the two evaluation reports contain significantly more detail than the article but the evaluation report on the third service is not available online.
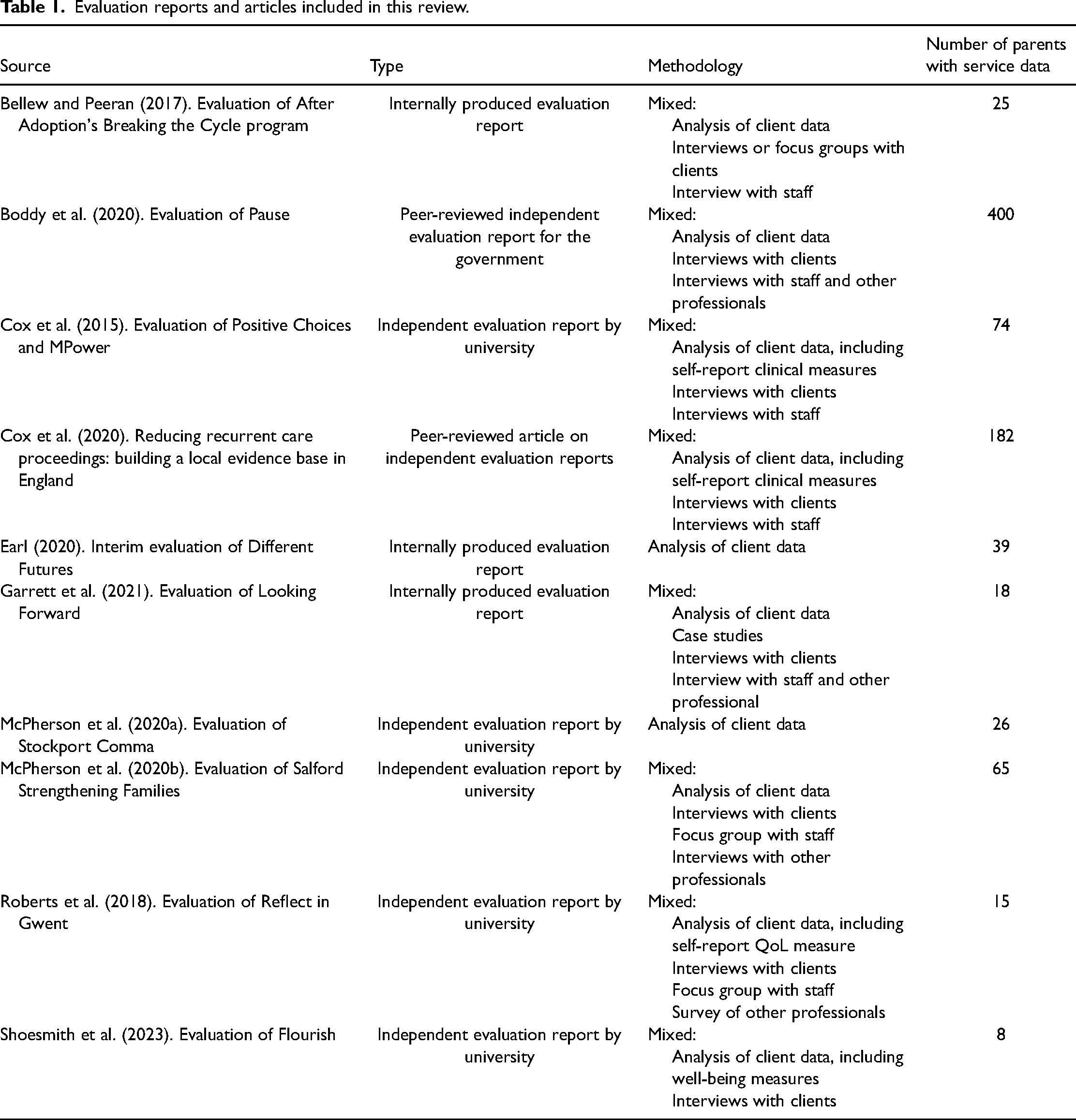
Of the 10 items included within this review, 1 was a peer-reviewed independent evaluation report for the government, 1 was a peer-reviewed article based on 3 independent evaluation reports by a university, 5 were independent evaluation reports by a university, and 3 were internally produced evaluation reports. Participants across the final 10 studies included represented 852 birth parents (almost entirely mothers: just 8 fathers were included) (Table 1).
Evaluation reports and articles included in this review.
A thematic analysis approach (Braun & Clark, 2006) was used to code the outcomes identified within each study, with a meta-summary to synthesize the qualitative results based on Sandelowski and Barroso's (2003) first two techniques of extracting relevant findings from each report and reducing them into abstracted findings.
Overview of different interventions
The information on services covered within the literature identified is variable. The majority are single-site services (Pause and Reflect are the exceptions). They typically provide intensive interventions for a period of between 12 and 24 months as outreach services. The literature identified did not all provide full details of the offer from each service, but the core components almost certainly include those identified by Mason and Wilkinson (2021), which are trauma-informed care; relationship-based care; person-centered and client-led care; therapeutic and practical support; assertive and flexible outreach work; recognizing and acknowledging parents’ loss and grief; support to develop healthy relationships; and sexual and reproductive health support.
Evidence from Baxter et al.'s literature review (2024) of the effective components of recurrent care services reflects these core components. The review highlighted the importance of relationship-based practice and building a trusted relationship (with a non-judgmental approach) between practitioners and parents as well as offering flexible, holistic, and client-led services with a long period of support and a flexible end date. It identified that services need to be trauma-informed and recognize the unresolved loss, trauma, and complex grief experienced by recurrent care experienced mothers. Services should provide therapeutic, emotional and practical support, advocacy, continuity, and tenacity in engaging with parents.
Breaking the Cycle is run by the after-adoption charity After Adoption and is a trauma-informed program that is reflective and therapeutic in nature. It is delivered by two part-time social workers who provide one-to-one and group work support to birth mothers. The evaluation period was 2 years.
Comma is based within Stockport Family, part of Stockport Children's Trust, and offers mothers a flexible, bespoke, and client-driven package of support. It is delivered by two part-time members of staff, a specialist health visitor and a social worker. The evaluation period was 18 months.
Different Futures is run by the local authority and supports mothers and fathers intensively for 2 years with gradually reducing direct input and the option to access aftercare for an extra year.
Flourish is based within local authority children's social care services and was commissioned to run an 18-month trauma-informed pilot intervention based upon an outreach approach and systemic principles that emphasize the importance of supportive relationships. It is run by a team manager and two practitioners. The evaluation period was 18 months.
Looking Forward is jointly run by the local authority and a non-profit organization. It employs one practitioner (22.5 h/week) to deliver trauma-informed and relationship-based support, including practical and psychological/therapeutic support, to birth mothers. The service is available for up to 2 years, sometimes longer. The evaluation period was 12 months.
MPower is run by a charity and works with mothers and their partners where appropriate and was launched with a part-time senior practitioner/support worker and part-time service manager. It provides one-to-one client-led, flexible, and relationship-based support. The evaluation period was 12 months.
Pause is a national non-governmental organization with local services that deliver intensive trauma-informed relationship-based practice by an average of 3–4 practitioners in each area over an 18-month period. Activities include one-to-one key work, group activities, and “Next Steps” support for mothers who have completed the intervention. The evaluation was over 2 years, but included analysis of data for a longer time period.
Positive Choices is run by the local authority and works with mothers and their partners where appropriate and was started with two full-time practitioners and one part-time service manager. It provides one-to-one client-led, flexible, and relationship-based support. The evaluation period was 18 months.
Reflect is provided by the charity Barnado's with sites covering all local authority areas in Wales, although this evaluation identified is only for the site in Gwent. It offers support to mothers and their partners for a period of up to 2 years. The evaluation captured longitudinal data with the use of case files.
Strengthening Families is run by the local authority providing an intensive service for parents (mothers and fathers) delivered through home visiting, one-to-one sessions, and group work on a range of parenting courses. The team comprises a manager, two lead practitioners, four practitioners, and one dedicated midwife. Support is available for a maximum of 2 years or (for birth parents keeping their baby) until their child begins school. The evaluation used retrospective data on parents referred to the service between May 2014 and February 2017.
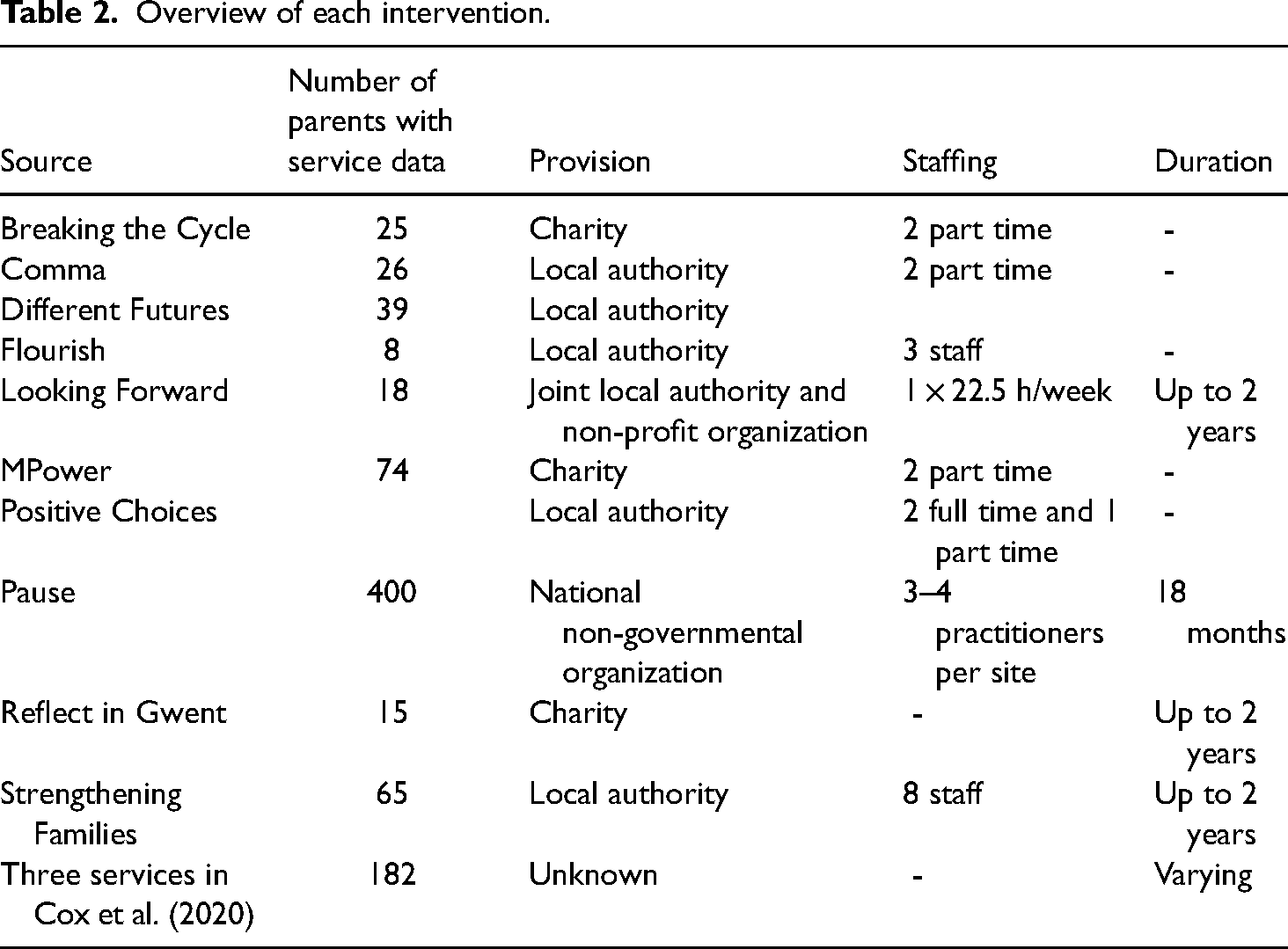
The three services within Cox et al.'s article (2020) were anonymized, so it is not possible to identify their funding. They all offer person-centered support and focus on the needs of individual parents. Two of the services work with mothers who are pregnant at referral as well as those who are not, and one service only accepts women who are not pregnant at referral, although it continues to work with them if they become pregnant. One service works intensively over the period of a year through one-to-one support, although this is flexible and dependent on individual need. One service has no maximum time limit to support mothers but has a “moving on” pathway for those who feel they are ready for a more “light touch” approach. One service provides post-proceedings support for a maximum of 2 years, increasing to 5 years in certain circumstances, and then continues to provide a reducing level of support for mothers who were pregnant at referral and who were able to keep their baby until the child starts primary school. The periods of evaluation differed by service from 2 years to 5 years (Table 2).
Overview of each intervention.
Results
Cost savings identified
Taking children into care represents high financial costs for local authorities, which include both one-off and ongoing costs. The one-off costs relate to care proceedings, which Boddy et al. (2020) estimated cost £44,300 per occurrence in 2018/19 prices. Annual placement costs are estimated to be £35,412 per child for foster care (Unit Cost Database, 2022). Not all children remain in care until they turn 18 as they may leave care to live with relatives or be adopted.
Boddy et al.'s national evaluation of Pause (2020) estimated that 14.1 fewer children below the age of 12 months entered local authority care, per year and per local authority. The outcome measure for this analysis was the rate of care entry per 10,000 children under 12 months of age from published data for the five Pause Round 1 areas and seven matched comparator local authorities (the latter had no known recurrent care service, similar backgrounds, and similar prior trends in infant care entry). This was to test the hypothesis that the Pause service had a cumulative effect on the rates of looked after children as women leaving the service are at a lower risk of subsequent child removals.
A cost-benefit analysis was undertaken, combining evidence on the costs associated with resourcing and delivering of Pause; estimates of the program's causal effects derived from the evaluation of its impact; and the unit costs of key outcomes associated with care proceedings, permanence, and placements. The study calculated that benefit-to-cost ratios (the savings per £1 of cost) were £4.50 over 4 years and £7.61 over 18 years. These savings exceed the UK HM Treasury (2018) thresholds for acceptability in value for money, which are normally a saving of £2 for every £1 spent. This is likely to be a significant under-estimate of the projected savings since it does not account for the benefits accrued from improved outcomes for the women participating that relate to reductions in high-cost service use, employment, or improved well-being as well as costs saved relating to children after the age of 18.
The delivery costs for the five Pause sites from 2016 to 2019 were estimated at £6.0 m, which is offset against the calculated savings of £8.9 m over 3 years in avoided care proceedings and £17.9 m over 4 years in avoided placement costs based on the reduction in the annual rate of removals, which would represent gross savings of £20.8 m. One note of caution is that since not all children remain in care until the age of 18—and for example, it takes an average of 2 years and 5 months for a child to be adopted (DfE, 2023)— the savings over 4 years may not be fully realized but would still be more than the Treasury's value for money acceptability thresholds.
A different methodology for calculating savings was used for a number of locally developed services that were evaluated by the research team at the University of Essex, but the results would appear to be not dissimilar to the savings ratios estimated for the Pause practices. These savings were based on Broadhurst et al.'s (2015) calculation that the probability of recurrence of care proceedings—without intervention—within 1–2 years of initial proceedings is 13.2%. The research team could therefore estimate the number of women engaging with each service who would be likely to experience an unplanned pregnancy and face recurrent care proceedings. Cost savings were then extrapolated based on the cost of “avoided” care proceedings and placements, although the avoided annual placement costs may not generate annual savings over all 18 years of each child's life. Calculations of avoided placements incorporated the Alrouh et al. (2022) findings that just 12.7% of parents appearing in recurrent care proceedings had an outcome where the child remained with their parents under supervision orders.
The three services evaluated by Cox et al. (2020), which worked with women to prevent pregnancies—but also worked with women who were pregnant at referral or who became pregnant during their engagement with the service—demonstrated that they could help to avoid removals. All children born to one of these women would have been at high risk of removal without any intervention, but of the 127 babies born during the evaluation period, three-quarters (96) remained with their parent or other family member while just a quarter (31) became looked after children or adopted. In addition, 12 children who had previously been removed were reunified with their mother during the period of their engagement with the service. Using the estimated costs of care proceedings and placement costs above would have resulted in estimated savings of £4.25 m from 96 avoided care proceedings and £3.8 m per year in 118 avoided annual placement costs. These estimated savings need to be offset by the cost of providing the services which was not available in the report but may be in line with Pause delivery costs of an average £300k per annum per practice (Boddy et al., 2020).
Additionally, Cox et al. (2020) suggested that recurrent care services are likely to generate further significant cost savings for the public sector through not exacerbating parental mental health difficulties, reducing substance misuse, and reducing the risk of poor outcomes for children in the future such as them becoming NEET (not in education, employment or training) and/or experiencing mental health difficulties themselves.
McPherson et al.'s evaluation of the Strengthening Families service (2020b) estimated that it had directly contributed to avoiding 118 children becoming looked after over the 5-year evaluation period. All of the mothers in the cohort were pregnant at referral, so on the assumption that they would all have gone through care proceedings when the baby was born, there were no cost savings due to avoided care proceedings. However, annual savings of £3.8 m would have accrued due to the avoidance of foster care placements. The estimated savings are approximately four times higher than the staffing costs of around £0.9 m over the evaluation period, i.e., around £4 per £1 spent.
The evaluation of Comma (McPherson et al., 2020a) estimated that the service had directly contributed to the avoidance of 3 sets of care proceedings for the 26 birth mothers engaging over the 18-month evaluation period. This would have generated one-off savings of approximately £97k in avoided care proceedings plus additional annual savings of up to £158k arising from the three children not becoming looked after. In addition, two looked after children were reunified with their mother generating savings of £105k per year through avoided foster care costs. Taking into account the staffing costs of around £61,500 during the evaluation period, total savings were estimated at approximately £5 per £1 spent.
The evaluations of MPower and Positive Choices (Cox et al., 2015) found that just 1 out of 66 birth mothers supported by these services was supported through a planned pregnancy and none of the remaining mothers became pregnant during the 18-month evaluation period. Without intervention, the researchers estimated that at least nine would have experienced an unplanned pregnancy and faced care proceedings. Again, using the estimated costs of care proceedings and placement costs mentioned above would have resulted in estimated savings of £400k from nine avoided care proceedings and £320k per year in nine avoided annual placement costs. These estimated savings need to be offset by the £169k cost of providing the services.
Based on Broadhurst et al.'s (2015) calculation that 13.2% of mothers go through repeat care proceedings within 1 to 2 years, the Flourish service would have expected one of their eight clients to have experienced recurrent care proceedings. The evaluation found that one mother became pregnant and was supported to access early support, but that this child was removed from her care. None of the other mothers became pregnant.
The evaluation of the Breaking the Cycle service, although involving just 25 mothers, found that no birth mother had lost a subsequent child since engaging with the service and three of the mothers had retained children in their care (Bellew & Peeran, 2017).
The remaining three evaluations did not provide any estimates for cost savings achieved but did report on other outcomes and clinical benefits achieved.
Outcomes and clinical benefits identified for mothers
The 10 evaluations all provided data on a range of outcomes produced for birth parents as a result of the support and interventions which may have some implicit cost savings although these were not calculated in financial terms. A wide variety of outcomes were measured by different evaluations, with a lack of consistency in how they were measured and over what time period. Some of the data on outcomes was recorded by practitioners, and some was self-reported by clients so may be influenced by factors such as trust in the practitioner, social-desirability bias where the client wants to “look good” or under-reporting the severity of problems. However, some overall conclusions can be drawn from the data presented in each report (Table 3).
Studies recording reduced use of drugs and alcohol.
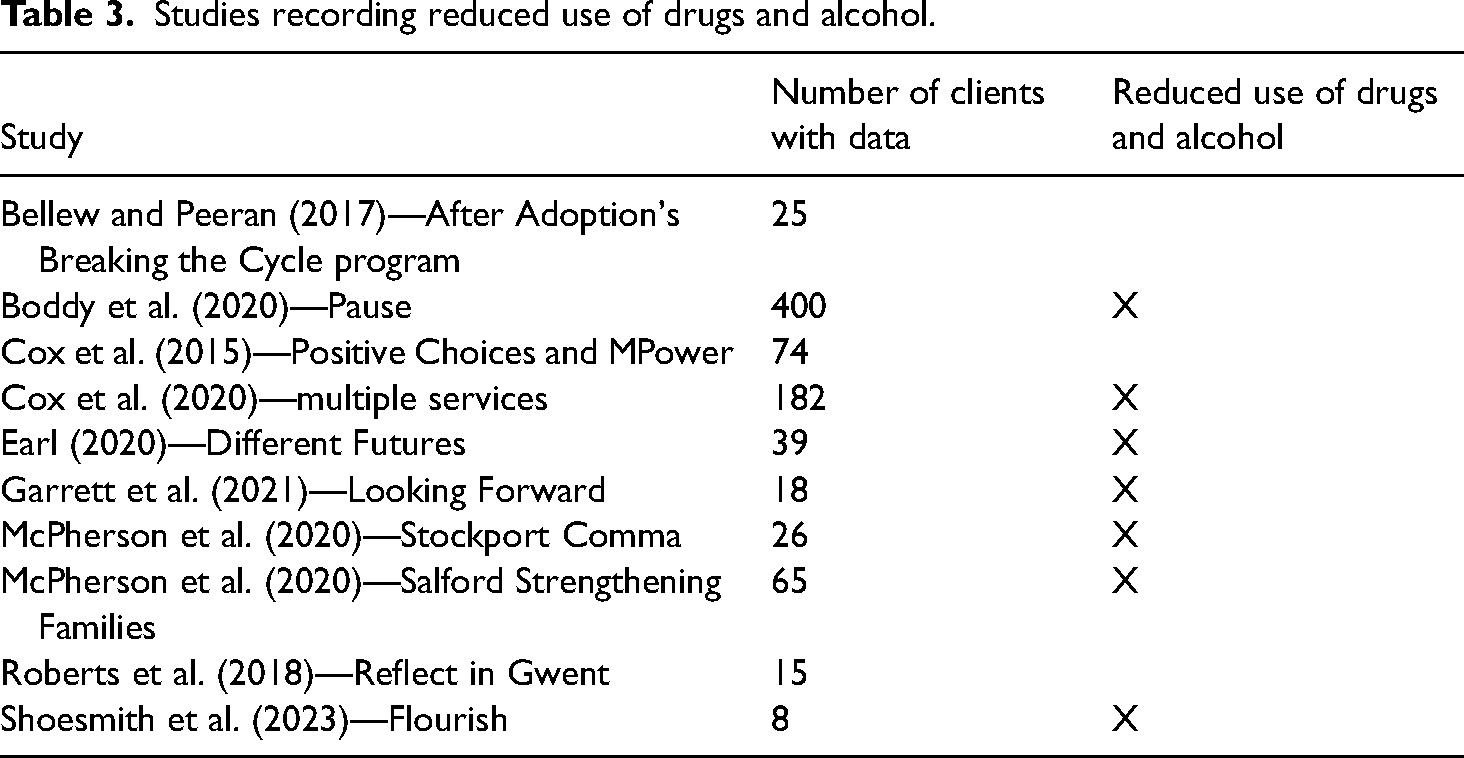
Seven of the nine evaluations recorded the reduced use of drugs and alcohol by birth parents since referral into the service, mostly based on practitioner reporting. Boddy et al.'s (2020) evaluation of Pause identified 23% of clients who reported a reduction in class A drug use (although 8% increased use) and 51% who reported reduced alcohol misuse (29% increased this). Boddy et al. (2020 suggested that the self-reported increases were very likely due to delayed disclosure to practitioners since trust took some time to establish. In Cox et al.'s evaluation of three services (2020), 22% of mothers revealed problems with drug use at referral, decreasing to 17% by the follow-up points, and 27% of mothers revealed alcohol issues, falling to 14% by the follow-up points. McPherson et al. (2020a) identified that while 28% of Comma's clients had problems with recreational drugs at referral and 21% had problems with alcohol, this fell to 7% and 14%, respectively, after 6 months. Drugs were a problem for 36% of Strengthening Families clients at referral but just 13% after 3 years while alcohol use was an issue for 29% at referral, down to 14% after 3 years (McPherson et al., 2020b). Shoesmith et al.'s evaluation of Flourish (2023) identified that while one mother (12.5%) stopped using substances and two mothers (25%) stopped misusing alcohol after 6 months working with the service, three (37.5%) were still using drugs, and one (12.5%) was still misusing alcohol. Two evaluations used the self-report Outcomes Star: Different Futures (Earl, 2020) found that 45% of clients maintained their score at the top for drug and alcohol use and 43% were progressing (13% had dropped back) while Looking Forward (Garrett et al., 2021) reported improvement from an average first score of 3.9/10 to an average last score of 4.5/10 (Table 4).
Studies recording improvements in mental health and well-being.
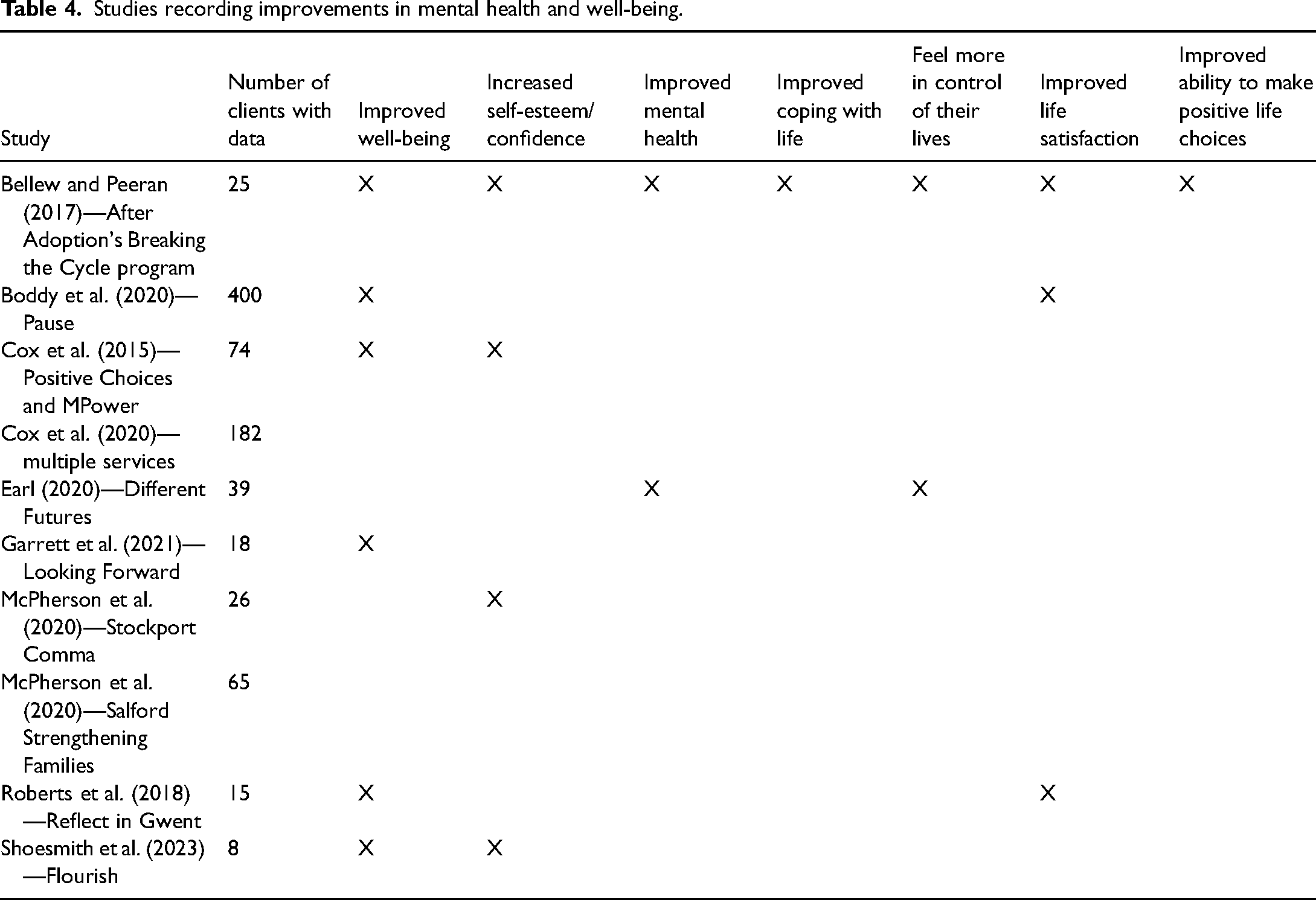
Six services reported improvements in parental well-being, four recorded increased self-esteem or confidence, three identified improvements in life satisfaction, and three reported an overall improvement in parents’ mental health. Bellew and Peeran's (2017) evaluation of Breaking the Cycle reported that clients showed improvements in self-reported well-being (including self-esteem, confidence, and mental health). Earl (2020) recorded that the percentage of clients of Different Futures who were “self-reliant” in mental health tripled between their first and last self-completed Outcomes Stars, but it was still low at 15% while Garrett et al. (2021) reported a slight increase for mental health and well-being from an average first score of 3.4/10 on the self-completed Outcomes Star to an average last score of 3.7/10. Pause monitoring data showed improvements in clients’ self-reported life satisfaction, but although the average score on the ONS life satisfaction questions at the endpoint was approaching the national norm for women of 7.69, it was still lower than 82% of the UK population (Boddy et al., 2020). Shoesmith et al. (2023) found some limited improvement for mothers on self-reported measures of well-being at individual levels, but most mothers’ well-being did not improve at the end point and their scores remained within clinical ranges which suggest an ongoing need for more intensive psychological support.
Two evaluations used validated self-report psychological measures, finding that psychological outcomes did not improve and that many of the mothers were still experiencing high clinical need in terms of their mental health. Questionnaire measures of maternal well-being in several evaluations have noted under-reporting of psychological symptoms at the start of intervention and increasing reporting of psychological symptoms as mothers engage more with practitioners and start to trust them, so it is possible that they understated the situation at the baseline point. Since there is likely to be under-reporting of symptoms and issues at baseline, clinically significant improvements would not necessarily be seen for all of the measures and some may even show deterioration. Either way, the findings across the studies suggest that mothers working with recurrent care services have a similar level of need as adults receiving support from formal mental health services which for many does not improve during the evaluation period, suggesting a significant unmet need for psychological care (Cox et al., 2020).
Two evaluations identified that parents reported feeling more in control of their lives, one that parents had improved coping with life and one that they had improved their ability to make positive life choices. Two reported improved physical health for parents (Table 5).
Studies recording improvements in housing and financial security.
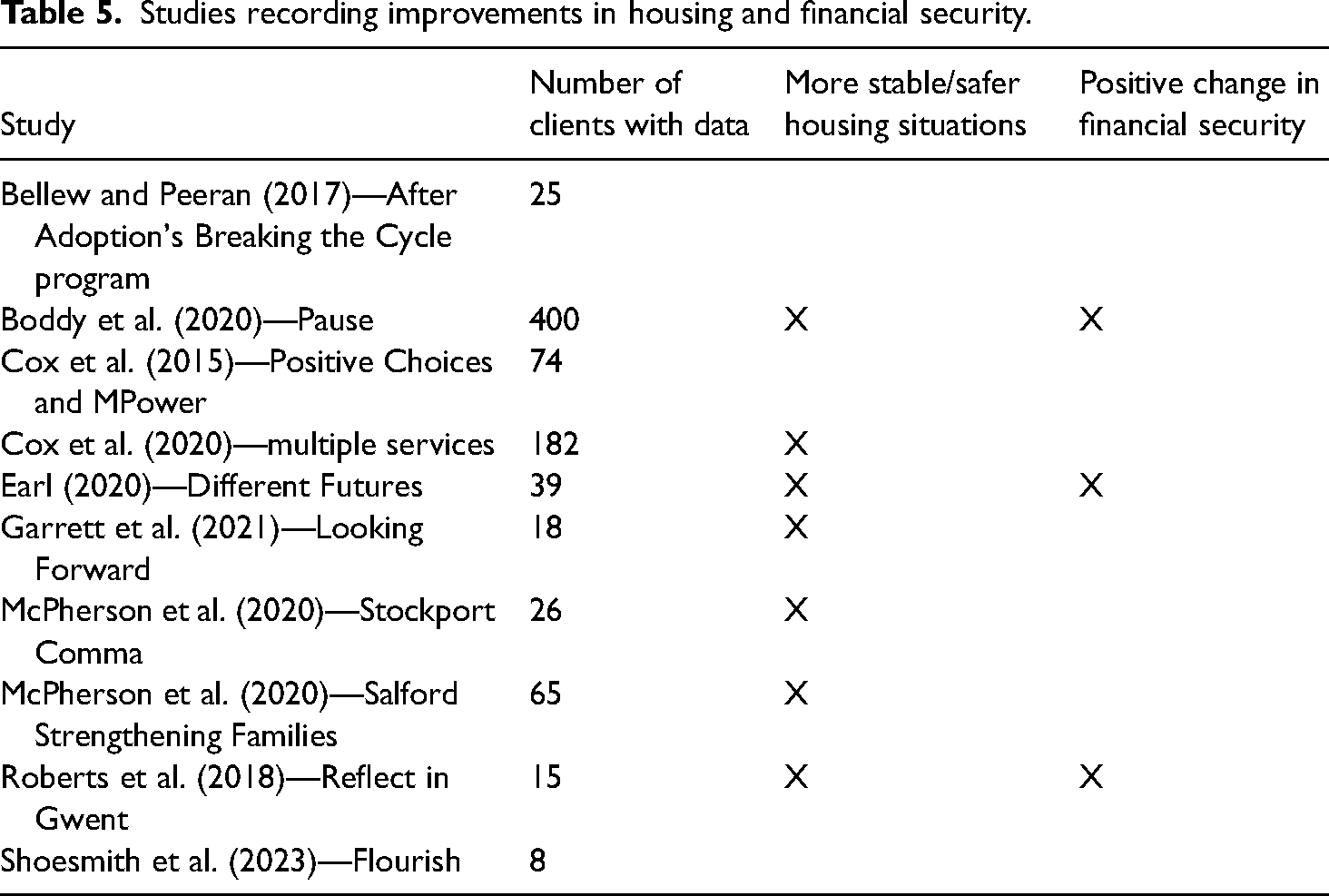
In seven of the evaluations, practitioners recorded that parents were in more stable or safer housing situations, including no longer being homeless. Thirty-eight percent of mothers working with Pause were in rent arrears at baseline, reducing to 28% at the endpoint, and the average value of rent arrears fell from £760 to £485, while the proportion who were in unstable accommodation or homeless fell from 22% to 13% (Boddy et al., 2020). For the three services evaluated by Cox et al. (2020), 16% of clients at referral had rent arrears or were homeless or at risk of eviction, but after engagement for at least 12 months, the proportion in stable accommodation increased from 74% to between 89% and 94%. Five percent of clients working with Comma were living in unstable housing at referral, but none were after 6 months (McPherson et al., 2020a). The two clients who were homeless at referral to Strengthening Families had rented accommodation after 3 years, and the two clients who were homeless after 3 years were living with family or in rented accommodation (McPherson et al., 2020b). The evaluation of Reflect identified progress for 33% of women in securing more stable housing (Roberts et al., 2018). Garrett et al. (2021) identified evidence that Looking Forward had helped to prevent the further deterioration of clients’ housing situations and also some improvements. Thirty-two percent of clients of Different Futures maintained their Outcomes Star score for managing tenancy and 61% were progressing (7% had dropped back) (Earl, 2020).
Practitioners in three studies reported a positive change in financial security for parents. Fifty-three percent of Pause clients were in debt at the baseline, falling slightly to 47% at the endpoint (Boddy et al., 2020). Of the 11 women working with Reflect who were experiencing debt problems or difficulties with budgeting at referral, just 3 (27%) were continuing to experience problems at case closure: 7 (64%) had been supported to set up repayment plans and were no longer increasing their debt while 3 (27%) had been supported through benefit tribunals with two decisions successfully challenged (Roberts et al., 2018). Sixteen percent of Different Futures clients maintained their Outcomes Star score for managing money and personal admin, and 68% were progressing while 16% had dropped back (Earl, 2020) (Table 6).
Studies recording changes in employment/education status.
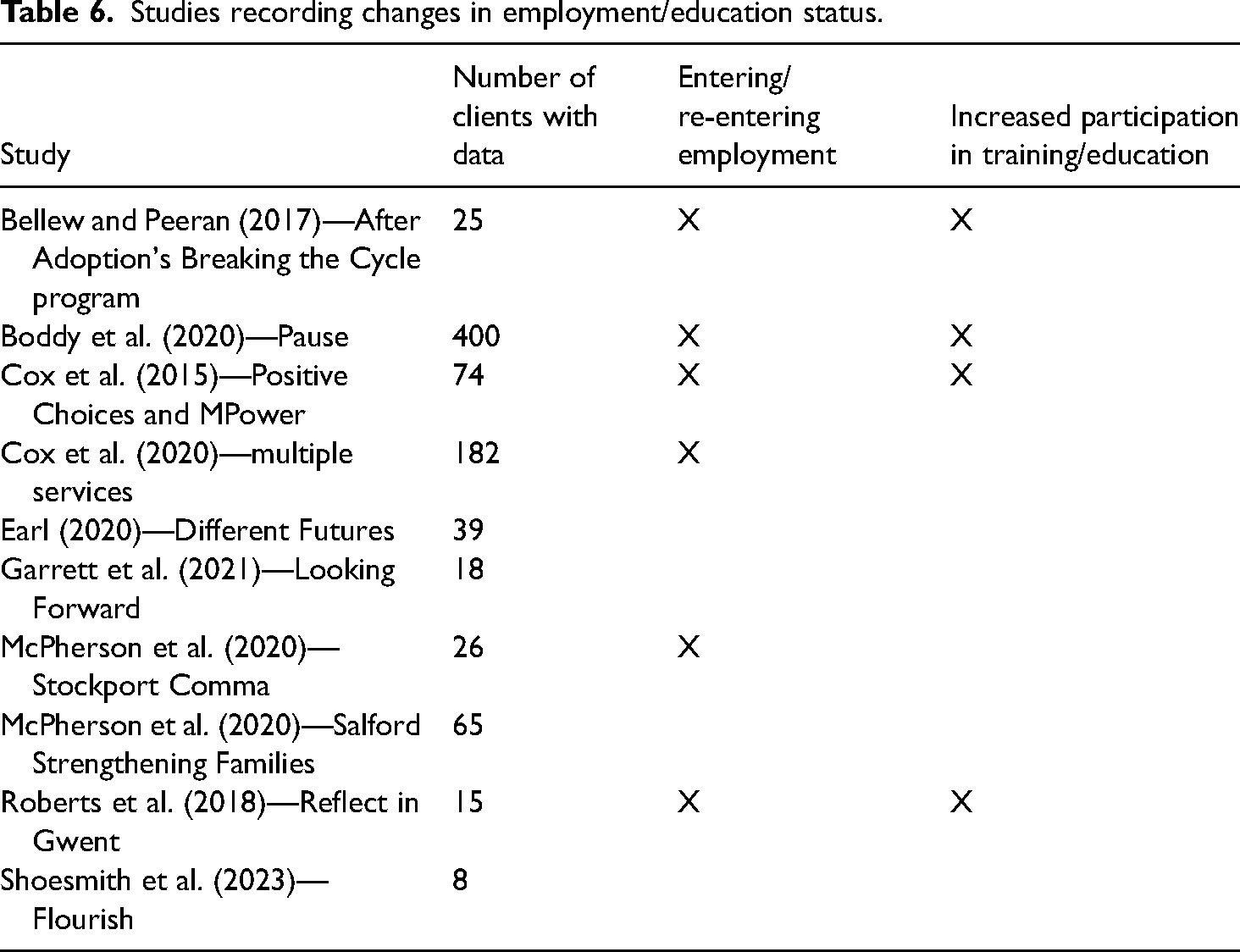
In six evaluations, practitioners reported that parents had entered/re-entered employment while four recorded parents’ increased participation in training or education. Twenty-four percent of the clients of Positive Choices and MPower had been able to find employment and 23% had accessed training (some had done both) (Cox et al., 2015). A fifth of mothers working with Breaking the Cycle had re-entered employment and a fifth had re-engaged with education (Bellew & Peeran, 2017). Thirty-three percent of women working with Pause were in employment at the endpoint, up from 21% at baseline (Boddy et al., 2020). Most mothers (89%) working in the three services evaluated by Cox et al. (2020) were either not working or unable to work at referral and this proportion fell slightly for two services. However, it rose slightly for one service, which may have been due to the large number mothers working with that service who had given birth and kept their babies. The proportion of clients working with Comma who were unable to work or were unemployed at referral fell from 44% at referral to 30% after 6 months (McPherson et al., 2020a). Five women (33%) working with Reflect were in education, employment, or volunteering by case closure, and a further 5 (33%) had taken positive steps towards this outcome (Roberts et al., 2018) (Table 7).
Studies recording access to other services/reductions in offending and domestic abuse.
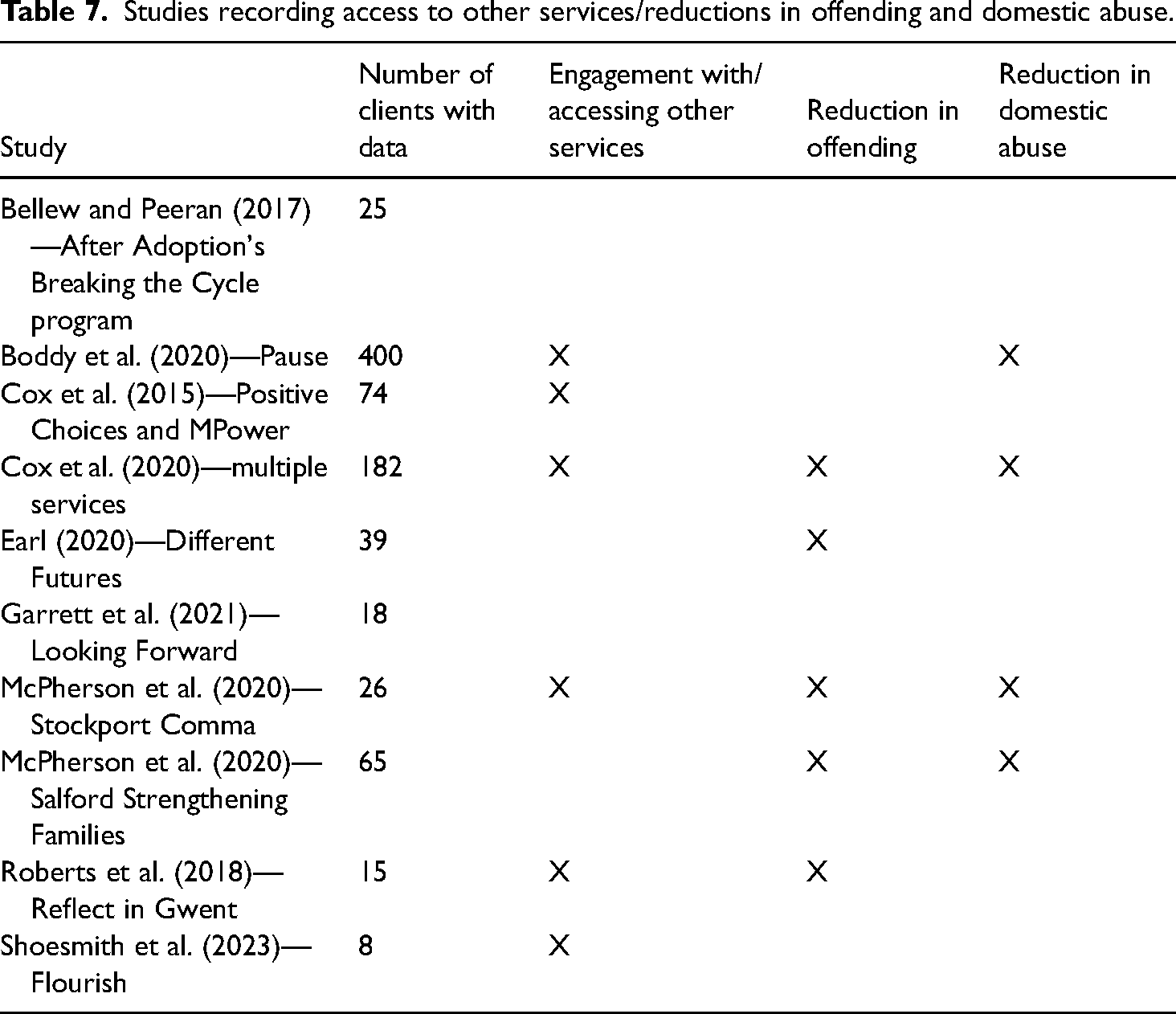
Practitioners in six evaluations reported that parents were engaging with or accessing other services as a result of the support received: this included mental health services, substance abuse services, sexual health services, and GPs. Five recorded a reduction in offending and/or that parents were no longer under the probation service. Between 11% and 22% of clients were on probation at referral, or involved with probation services, but none were at the follow-up points for the services evaluated by Cox et al. (2020) and McPherson et al. (2020a and 2020b). At case closure, engagement with probation was ongoing for three women working with Reflect and no further convictions, charges, or convictions had been recorded (Roberts et al. 2018). Sixty-eight percent of Different Futures clients maintained their Outcomes Star score at the top for offending and 26% were progressing, but 3% had dropped back (Earl, 2020).
Practitioners in four evaluations recorded significant reductions in the number of parents experiencing domestic abuse. Boddy et al.'s evaluation of Pause (2020) identified that the proportion of women reporting that their current partner hurt or threatened them fell from 35% at baseline to 17% at the endpoint. While 67% of mothers working with the three services evaluated by Cox et al. (2020) at referral reported partner abuse within the previous year, this decreased to around a third at the final follow-up points. At referral, 53% of mothers working with Comma reported partner abuse within the last year, falling to 25% after six months (McPherson et al. 2020a) while 57% of clients working with Strengthening Families identified partner abuse at referral, decreasing to 20% of clients after 3 years (McPherson et al., 2020b) (Table 8).
Studies recording other outcomes.
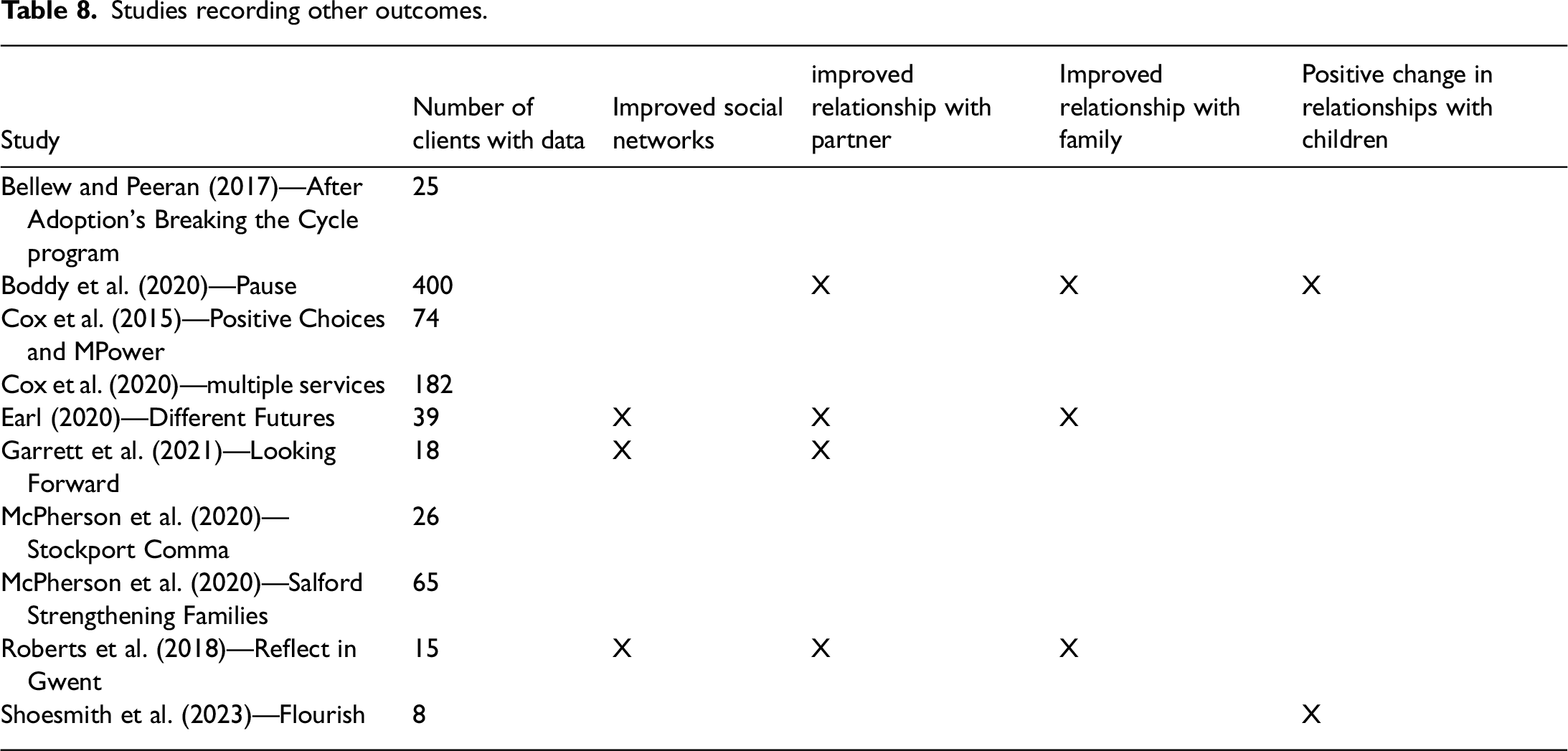
Practitioners in four evaluations stated that relationships with partners had improved and in three that relationships with family had improved, while three evaluations recorded improved social networks and one a greater engagement with community activities. Practitioners in two recorded a positive change in the mothers’ relationships with their children.
Outcomes for children
None of the evaluations monitored outcomes for children, other than their safeguarding status (i.e., being in the care of local authorities vs. being in the care of the birth parents). However, Boddy et al. (2020) in their evaluation of Pause argued that there are likely to be benefits for children also, given that mothers and professionals consistently reported better relationships with children within diverse placement and permanency arrangements.
The evaluation of Strengthening Families (McPherson et al., 2020b) tracked children who had reached school age in terms of their level of development when they started school. The number of children is very small (just 4), so caution must be used when analyzing the data, but it appears as though the children of parents supported by the service performed better than other looked after children within the same local authority in terms of a Good Level of Development by age 5 (Early Years Foundation Stage data reported to Ofsted).
Discussion
Overall rates of children in care in England have increased significantly in the last 22 years, from 59 per 10,000 children in 2001/02 to 78 per 10,000 in 2022/23 (Department for Education, 2023), as have the costs of looking after them.
The evaluations identified employed different methodologies, parameters, and assumptions to estimate the cost savings generated for public services, and some did not undertake extensive financial assessments. This means that some caution should be taken in directly comparing the estimated cost savings for each service. However, we believe that overall, there is sufficient evidence to state that services supporting recurrent care experienced parents do offer value for money and do generate cost savings.
We believe, based on the evidence presented by this literature review, that funding services to support birth mothers (and fathers) who have had one or more children removed from their care would reduce the number of looked after children and lead to substantial long-term savings for the public sector, which in the UK is principally local authorities. The cost of providing these recurrent care services would be considerably less than the savings generated in avoiding care proceedings and child placements. This should be welcomed given the current pressures generally on public services and specifically on local government budgets.
Boddy et al. (2020) in their evaluation of the Pause model, argued that: The findings provide convincing moral and fiscal arguments for the development nationally of trauma-informed relationship-based support for women who have had a child removed, to prevent risk of recurrence (especially for young women) following the first removal of a child.
The estimated cost savings generated by recurrent care services focused on avoided costs from children being looked after by local authorities and did not attempt to estimate the impact on wider public sector services, such as probation or domestic violence services. However, one of the outcomes identified for clients was a more appropriate or reduced use of services which clearly would have implications for cost savings across the whole system.
We would also argue that the evidence available from the published evaluations demonstrates the effectiveness and value of support for parents who are at risk of recurrent child removal.
Previous research has identified that recurrent care experienced mothers have multiple and interconnected issues, including physical and sexual abuse in childhood (Broadhurst & Mason, 2020). As adults, between 21% and 36% had problems with drug use or alcohol or both; 35% to 67% had experienced domestic abuse; 47% to 62% had identified mental health issues at referral; and between 11% and 22% were on probation or involved with probation services (Boddy et al., 2020; Cox et al., 2020; Garrett et al., 2021; McPherson et al. 2020a; McPherson et al., 2020b). Community services supporting these issues typically have long waiting times for access and operate as separate entities, making it difficult for clients with multiple issues to be treated holistically. The evidence shows that support from recurrent care services has enabled significant improvements in outcomes for their clients in these areas.
There are still a number of gaps and outstanding needs, particularly psychological needs. More targeted psychological support is required once mothers have been enabled to meet their basic needs and re-establish trust with professionals. Some may need more in the way of long-term psychological treatments and this group of women could be left out of plans to address inequalities in women's health if their mental health needs are ignored (Cox et al., 2020; Shoesmith et al., 2023).
Recurrent care services provide extremely valuable support to these parents, helping them to move into education, training, or work and to deal with difficult personal issues or domestic situations. Boddy et al.'s evaluation of Pause (2020) identified consistent evidence of positive changes for mothers that continued or even emerged post-intervention. However, life continued to be complex and challenging for many mothers, with implications for the program's provision of a foundation for long-term change.
The support from recurrent care services can establish positive changes in birth parents’ lives with the corresponding financial benefits achieved through reductions in the number of babies entering into care. The significant cost savings for the public sector more than offset the cost of providing services.
More needs to be done to promote the funding of services so that all recurrent care experienced parents are offered support. This includes not just national policy-driven services but also those which are designed and driven locally to adapt to local needs and population characteristics. The Women's Health Strategy for England (Department of Health & Social Care, 2022) acknowledges the significant disparities and inequalities in health faced by women and aims to address the huge inequality across health that women face. One of its 10-year ambitions is “preventing the onset of mental health conditions wherever possible, addressing disparities in outcomes, and ensuring equitable and timely access to specialist support for those who are struggling with their mental health. Our plans must take account of differential experiences of women if we are to successfully reduce disparities in mental health outcomes.” Another aim of the Strategy is to improve awareness of the effects of alcohol misuse on women's mental health.
Services should also be available in every local authority area in the country. If regional or national funding, such as for the Reflect service in Wales, is not provided then local authorities themselves should seriously consider doing so themselves to benefit from the substantial savings they can achieve. Can local government and the state really afford to ignore the complex needs of these parents and continue to allow the “revolving door” into repeat care proceedings?
Limitations of the study
There are a limited number of evaluations to draw evidence from in light of the 73 recurrent care services known to be offered in England, so that the findings presented here may not be fully representative, although the inclusion of Pause and a number of university-led studies should indicate some reliability. Additionally, none of the identified evaluations were from outside of the UK.
The evaluations have focused on outcomes mainly for mothers, with very few fathers included within the data presented. However, outcomes specifically for fathers (whether the father of the mother's children or not) should be considered when evaluating these services. While some services now work with fathers in their own right, whether or not the mother is engaging with the service (Mason & Wilkinson, 2021), no evaluations of support for recurrent care experienced fathers (who often have similar vulnerabilities and traumatic life histories as mothers) were identified.
Different evaluations have utilized different methods, parameters, and assumptions to estimate the cost savings for the public sector, which means that there is a risk of making inappropriate comparisons between studies.
Implications for further research
Most of the services evaluated have few members of staff and limited funding, so it was difficult for them to commission (and fund) an independent and external evaluation. A few were able to undertake an internally run evaluation. However, the majority of recurrent care services in the country are unable to fund an independent evaluation. A future research program to evaluate more services with a consistent methodology, perhaps through the Supporting Parents Community of Practice, would be beneficial.
The evaluations have focused principally on outcomes for mothers, and outcomes for fathers are not available. Outcomes for children have also not been effectively measured by any of the identified evaluations, although we could hypothesize benefits for them given the reporting of improved relationships. Future research should examine the long-term impact on children who remain with parents supported by recurrent care services and measure outcomes for fathers.
Conclusion
This is the first-ever review of the effectiveness of different services in the UK to support recurrent care experienced parents, in terms of the outcomes produced and potential cost savings for local government and state welfare budgets. The evidence shows that these services can generate cost savings of somewhere between £4 and £5 for every £1 spent through avoiding care proceedings and placements of children taken into care, although some caution must be used here due to the different methodologies employed within the identified literature. In addition, the parents working with these services achieve a range of positive outcomes including improved mental health (although more specialist psychological and mental health support still needs to be provided from many of these families), reduced substance misuse, less domestic abuse, employment, and more stable housing situations. This raises significant questions about why so many local authorities do not fund recurrent care services, especially in light of the budgetary pressures they are under for the reasons covered earlier.
Footnotes
Ethical approval
Ethical approval was not needed for this literature review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflict of interests
The Authors declare that there is no conflict of interest.
Data availability
All studies included within this review are available online.