
Abstract
Summary
Limited information exists on the lived experiences and well-being of female social workers providing mental health services in northern Canada. Participatory narrative inquiry was utilized as a collaborative approach to gather stories from/with outsider female social worker mental health providers herein referred to as providers. Ten providers participated in this project through individual and group semistructured interviews in three phases. Transcribed interviews from each phase were analyzed through participatory narrative analysis to collaboratively generate themes, while ensuring the context of participant stories was maintained.
Findings
Collaborative participatory narrative analysis of participant stories revealed the following major themes: the work is complex and impactful including direct and/or indirect secondary trauma; safety and well-being supports are required; relationships are central to the work; and personal growth and understanding the trauma history of Indigenous peoples is crucial to carrying out northern trauma services.
Applications/conclusion
Providers believe that they need to feel safe and supported to protect their personal well-being and, in turn, to effectively carry out trauma services. However, current northern work environments lack networking, clinical supervision, and the safety supports required to meet the providers’ needs. Well-being support recommendations for providers included: adopt a strength-based attitude/outlook as well as an effective long-term relational team-based practice approach, improve networking through a “community of practice,” develop trauma-informed northern work-specific competencies and training, and advocate for safety improvements as well as governance agency provider supports.
Introduction
Northern Saskatchewan, Canada, is a large geographical area with almost 90% of people identifying as Indigenous (Statistics Canada, 2016). Many locations are accessible only by plane or winter ice roads; they also face challenges in establishing local resources, as well as accessing client supports outside of the community (Lavoie & Gervais, 2012). Previous research identified isolation as the most challenging barrier to northern work because providers often have limited access to clinical supervision and peer supports (Coholic & Blackford, 2003; O’Neill et al., 2013, 2016). Without readily available resources, providers must have the necessary skills to work independently carrying out northern services without supports (Assembly of First Nations, 2015). An isolated work environment with a high demand trauma caseload without adequate supports can negatively impact the well-being of providers, including increasing one's risk of emotional distress such as secondary trauma (O’Neill, 2010).
Well-being was based on wellness from an Indigenous perspective and defined as “a whole and healthy person expressed through a sense of balance of spirit, emotion, mind, and body” (Thunderbird Partnership Foundation, 2014, p. 5). Whereas, secondary trauma was described through the construct of secondary traumatic stress and defined as the distress experienced by a provider as a result of repeated indirect exposure to the traumatic stories of others (Figley, 1995). As such, participants were asked to describe the impact of their northern work in relation to the physical, emotional, spiritual, psychological, and relational aspects of life and work.
To begin to understand the well-being needs of northern Saskatchewan providers, it was imperative to recognize that individuals with lived experience hold the wisdom to understand and transform their work environment (Le Blanc & Schaufeli, 2008). Participants engaged in a collaborative, multiphase, participatory narrative inquiry (PNI) qualitative process to provide the in-depth data necessary to answer this project's research questions (Kurtz, 2014). Data was also analyzed through participatory narrative analysis to identify how northern trauma work impacted the well-being of providers and, in turn, make informed recommendations to improve the quality of their northern workplace environments (Riessman, 2008).
Well-being implications of northern trauma work
Providers carry out services in isolated northern Canada with populations experiencing high levels of trauma and describe the work as both exhilarating and heartbreaking (O’Neill et al., 2013). Trauma counseling involves listening to clients’ graphic stories (Bishop & Schmidt, 2011; Harrison & Westwood, 2009; Hensel et al., 2015; O’Neill, 2010) which can be emotionally and psychologically arduous, even for the most seasoned social worker (Bride, 2007). Providers who deal primarily with traumatized clients are more likely to experience secondary trauma (Bride, 2007; Pearlman & Mac Ian, 1995). Secondary traumatic stress can create cognitive shifts (increased distrust and anticipatory danger without the ability to protect oneself), as well as psychological distress (unpleasant or lack of feelings and increased startle response) which, consequently, can interfere with one's capacity to perform daily activities (Collins & Long, 2003a).
In light of the job demands and isolation, northern providers might be at increased risk of experiencing secondary traumatic stress symptoms such as a loss of compassion, sleep issues, hypervigilance, heightened distress, and an inability to adequately meet the needs of their clients (O’Neill, 2010). Secondary traumatic stress risk factors include working long hours, work stress, and insufficient coping strategies (Bishop & Schmidt, 2011; Pearlman & Mac Ian, 1995). There could also be issues of being a young inexperienced worker, unresolved personal trauma, or a high trauma caseload with the lack of accessible supports (Hensel et al., 2015). Overall, new providers most often experience culture shock and a lack of connection with/within northern communities (Cruikshank, 1990; Zapf, 1993), therefore being at the greatest risk of experiencing secondary traumatic stress (Devilly et al., 2009). Additionally, it was reported that secondary traumatic symptoms experienced by providers impacted the people closest to them (Breaux et al., 2008; Pearlman & Saakvitne, 1995; Stone, 2011; Westman & Bakker, 2008).
Providers reported that the job demands in northern communities occasionally take over their lives (O’Neill, 2010), including: high rates of complex trauma clients, limited supports/resources, insecure program funding, and high staff turnover (O’Neill et al., 2013). The inability to adequately balance northern trauma work demands with one's personal life was the most common reason provided for leaving their job or giving up any type of trauma work (Hensel et al., 2015; Kanno, 2010). In contrast, providers least negatively impacted by trauma work could detach themselves from their client's stories (Ludick, 2013) and focus on client resiliency (Morrissette & Naden, 1998). As such, providers require empathy boundaries, particularly when they share a trauma history resembling that of their clients (Ludick & Figley, 2016); however, emotional distance can undermine supportive/healing client relationships (Collins & Long, 2003a). Therefore, northern providers expressed a desire to utilize trauma-informed practice competencies that support the well-being of their clients, as well as their own, to strengthen their capacity to provide long-term service to and with communities (O’Neill et al., 2016).
Practice competencies to support the well-being of northern providers
To work effectively in northern communities with high trauma caseloads and limited resources, providers must develop safe collaborative partnerships to protect their own well-being (McCormick, 2009). Although providers recognize that building trusting relationships is crucial to working within northern communities and reducing the isolation; they also understand that assuming dual roles can create challenges in following their professional Code of Ethics (Coholic & Blackford, 2003; Galambos et al., 2005; Graham et al., 2008; Hensel et al., 2015; O’Neill et al., 2016).
Relationships and trust are the foundation to working with, and learning from, Indigenous clients (Shepard et al., 2006). With high staff turnover by northern professionals, it is vital to develop community connections to better understand the strengths and needs of each community. Providers must obtain key contextual knowledge surrounding the history of forced assimilation of Indigenous peoples to understand the circumstances that have created trauma, systemic inequalities, and distrust of outsiders in northern communities in Canada (Stewart, 2009). Furthermore, this knowledge (or lack thereof) influences the type of therapeutic relationships that Canadian social workers can create with their clients, including the possibility of perpetuating power and racial inequities (Pierce & McKinnon, 2022).
Ermine (2007) argues that providers need to acknowledge the importance of creating ethical space to engage in these key conversations for learning and building relationships. Northern providers must also embrace a trauma-informed approach to counseling (Allan & Smylie, 2015; Assembly of First Nations, 2015; O’Neill et al., 2016) so that both clients and providers are supported (Substance Abuse and Mental Health Services Administration, 2011; Wieman, 2009). For example, Kiawenniserathe Benedict (2015) emphasized that “the healing journey and spirit of the helper is just as important as that of the one seeking help. In order to help in a good way with a good mind, helpers need to be cared for” (p. 18). In this context, O’Neill et al. (2016) recommended that northern providers utilize the following practice competencies to support their well-being and mitigate the risk of secondary trauma: “cultural competence, generalist practice, trauma-informed practice, finding ways to make full use of limited resources, and sustaining strategies” (p. 134).
Previous studies indicated that isolation and boundary challenges experienced by providers can be offset by clinical supervision, networking, debriefing, secondary trauma training, expanded client resources, and supportive family/friends (McSwain, 1997; O’Neill et al., 2016), as well as collaborating with an interdisciplinary team (Goodwin et al., 2016). Additionally, teams with supervisory oversight can help protect providers from secondary traumatic stress (Collins & Long, 2003b). As such, the well-being of providers is better supported within a team approach such as a “community of practice” (Wenger & Snyder, 2000), which is defined as “groups of people who share a concern or a passion for something they do and learn how to do it better as they interact regularly” (Wenger & Wenger, 2015, p. 1). Moreover, a “community of practice” would be advisable when working in northern Canada to support the needs of providers and the community by creating partnerships to enable social workers to share their knowledge and experiences, and to improve their capacity to provide services (Ceatha, 2018).
With a lack of information regarding the well-being of northern providers (Mental Health Commission of Canada, 2012) and in particular women in this role, it was important to examine their experiences to make evidence-informed recommendations that could support the well-being and psychological safety of providers (Mental Health Commission of Canada, 2013). This required an in-depth understanding of their lived experiences, along with their ability to cope with northern work demands (Ludick & Figley, 2016). More specifically, female outsider providers in northern Saskatchewan who travel to a community to work (e.g., are not a resident of that community) needed an opportunity to share crucial information so that others could better understand the implications of northern trauma work on well-being and, in-turn, identify needed supports for effective practice. This project was an opportunity to link this void in knowledge by answering the following research questions: How, through the lived experiences of female outsider providers working in northern Saskatchewan, can we better understand the impact of delivering trauma-informed services (e.g., secondary trauma), and how can we initiate opportunities to improve supports? How can sustainable supports be co-created with participants, including a “community of practice,” to protect/improve the well-being of providers working in northern Saskatchewan communities? How can we improve the quality of their work environments and, in turn, improve the quality of services for clients?
Method
Design
To support hearing the stories of female social workers experiences in northern Canada (Creswell, 2013) and to reflect and interpret those experiences (Kovach, 2009; Kurtz, 2014), data was collected using qualitative methods and PNI. Qualitative research allowed participants to build the necessary rapport and trust with the researcher to share their rich in-depth knowledge working in northern Canada as female social workers (Creswell, 2013). In order to create a safe trusting space for participants to share their experiences qualitatively, PNI was utilized (Kurtz, 2014). Cynthia Kurtz (2014) created PNI as a means to support participants in sharing their stories through a process of exploring and reflecting to gain a more in-depth understanding of their experiences and to make informed decisions for change. PNI merges participatory action research and narrative inquiry and is based on the premise that realities are relationally co-constructed (Colla & Kurtz, 2024; Kurtz, 2014). Furthermore, it is through this relational process between all participants including the researcher that knowledge is created (Burr, 1995). In PNI, participants take part in the research process to accurately reflect, interpret, and make meaningful recommendations for change (Kurtz, 2014, Riessman, 1993). PNI was used to co-create providers’ well-being stories by making sense of the context of their work experiences by engaging in a process of self-reflection and transformation utilizing the following principles: supporting participants to work collectively and creatively to make effective recommendations for change; connecting participants’ stories to their intended recipients (agencies and policy-makers); viewing participants as subject-matter experts regarding their own experiences; refraining from interfering with participants’ stories (e.g., removing emotions); supporting differences of opinions to generate innovative ideas; and adjusting the process to meet the needs of participants (Kurtz, 2014). Innovative elements of this project included participant engagement throughout the research process to gather their stories and generate meaningful practice recommendations (Kurtz, 2014), which included building a “community of practice” (Wenger & Wenger, 2015). By bringing people and their stories together, participants were able to develop innovative and collaborative methods for data collection and analysis and generate meaningful recommendations for change beyond what could have been generated individually (Hacker, 2013; Kurtz, 2014).
Gathering the lived experience of participants required a methodology built on a foundation that supported building strong relationships with participants. Stories are co-created (collaboratively generated) from the relationships developed between participants and the researcher, as well as between the participants. As such, participants’ realities (more specifically, their stories), are generated contextually through these relationships and shared experiences that include culture and history (Burr, 1995, 2015). Therefore, PNI was chosen because it specifically supported a relational-based method of gathering qualitative information to better understand the impact of working in northern Saskatchewan as an outsider female social worker, that could not be answered without a relational-based approach (Caruth, 2023; Kurtz, 2014).
Collaboration began at the onset of this project by developing a Community Advisory Committee which was comprised of four key individuals (Provider, Social Work Professional Regulator Director, and two Associate Professors at First Nations University of Canada) who guided all aspects of the process. This included developing the research questions, identifying participants and the methods/methodology to be used, choosing the analytical tools, and reviewing/considering the recommendations that evolved from this project, including individual practice improvements (Canadian Institutes of Health Research, 2014). Figure 1 illustrates how participants and the Community Advisory Committee engaged in a cyclical, reciprocal, and iterative process to support the principles of PNI (Flick, 1998; Gehart et al., 2007; Hacker, 2013; Israel et al., 1998).
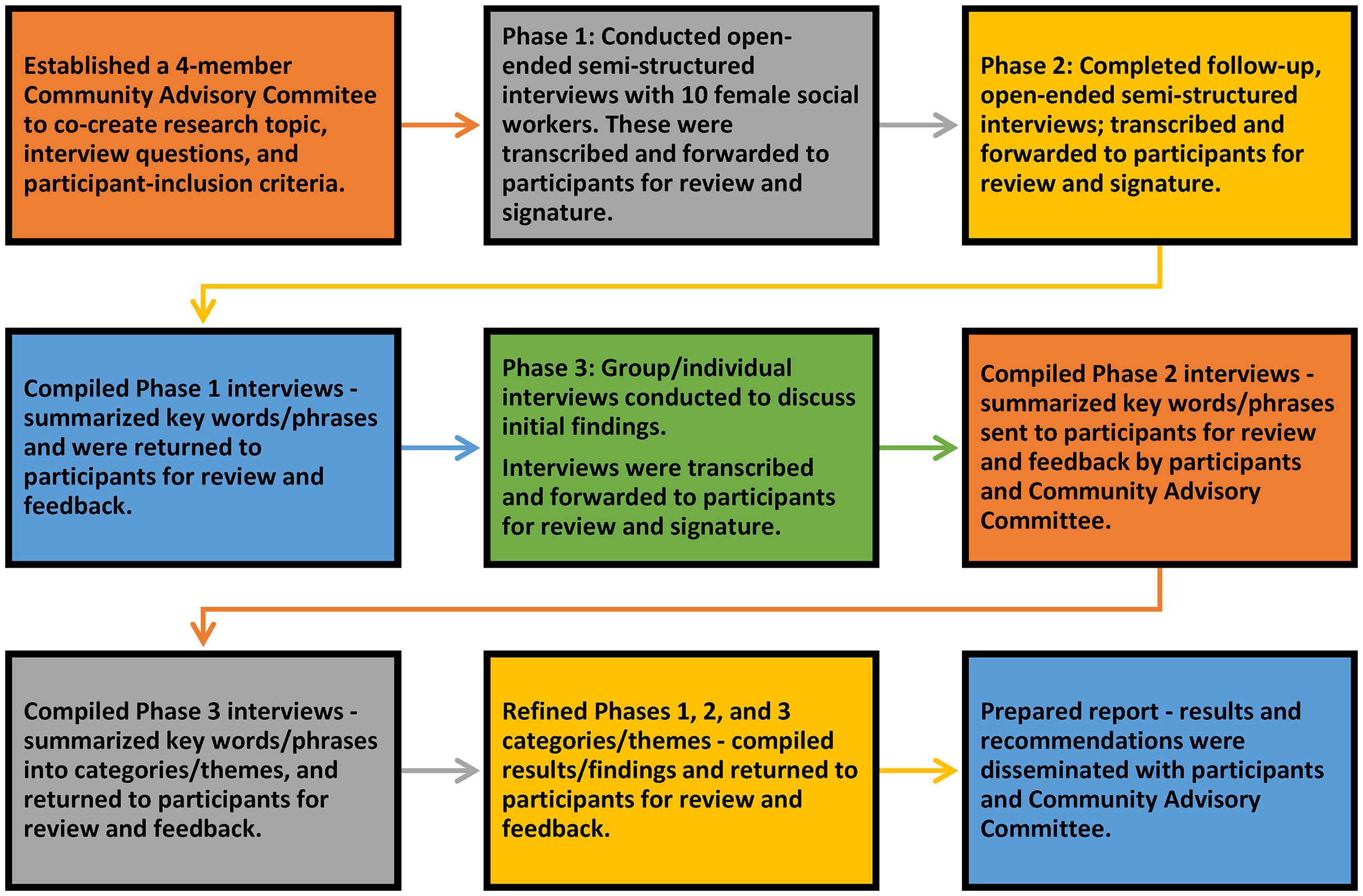
Research process summary.
Data collection took place as follows: (a) stories were generated collaboratively with participants through a series of three audiorecorded, semistructured open-ended interviews which included inviting participants to share the meaning of their experience in Phase 2; (b) audiorecorded interviews were transcribed by the researcher; (c) transcripts in each phase were deidentified (identifying information redacted), and then e-mailed to participants for review and feedback; (d) participants were asked to sign a Transcript Release Form in each of the phases once they deemed their transcript to be acceptable and accurate (following each interview); (e) a group gathering took place with four participants to review the compilation synthesis of participant quotes and paraphrased phrases of all transcribed Phase 1 interviews; (f) group participants also discussed commonly identified barriers and possible solutions to northern work, as well as their own strengths, self-care strategies, and recommendations to whom and where their stories should be conveyed; and (g) participants unable to attend the group gathering responded to the questions via a telephone interview or e-mail.
Participants
At the time of this project (August 2020, which was during the COVID pandemic), most Health Canada-approved providers in northern Saskatchewan were female social workers (Health Canada, 2020). With this key information, and after considerable discussions with the Community Advisory Committee, it was determined that because female social workers most often occupied the role of northern provider, their voices were needed to carry out this project. Therefore, a purposeful sampling strategy was utilized to recruit female social workers with comprehensive knowledge, and who lived with the phenomenon under examination (Patton, 1990). As such, collaborative engagement with the Community Advisory Committee resulted in the following inclusion criteria for participants in this project: (a) female social workers registered with the Saskatchewan Association of Social Workers and Health Canada approved; (b) individuals who had previously worked in a northern Saskatchewan First Nation community; and (c) those who traveled into a community to work (not a resident of that community). In addition, a small sample size was needed to support the building of safe trusting relationships over time, through multiple narrative interviews, with the goal of generating rich data (Rossman & Rallis, 2012).
This resulted in a purposeful sample of 10 female providers who had identified an interest in the project and agreed to provide in-depth narratives that could only be accomplished with a limited number of participants (Patton, 2015). Participants were invited to take part in this project until saturation was reached, meaning no new information was emerging from the participants (Smith & Osborn, 2003). All 10 participants possessed a Bachelor of Social Work degree; of these, seven of the 10 had also obtained a Master of Social Work degree. Most participants were non-Indigenous; two individuals identified as being Indigenous. Participants identified having 15 or more years of experience working in mental health, and 3 or more years experience working in northern communities. All participants indicated that they did not reside in, nor were they a member of the northern community where they provided counseling services.
Data analysis
Audiorecorded individual and group interviews were transcribed and then reviewed, revised, and signed off by each participant at each of the three phases. With this being a participatory project, participants were fully involved in the analysis of the data, which is consistent with the principles of PNI. Therefore, participatory narrative analysis was used because it supported a flexible process for participants’ narratives to be systematically brought together and collaboratively reviewed for common ideas/themes, while keeping the story connected (Kurtz, 2014, Riessman, 2008). The data analysis process was carried out as follows: (a) the researcher began by getting familiar with the transcribed data by coding (highlighting the statements, segments, and verbatim quotes that stood out within the transcripts from each phase (Gehart et al., 2007); (b) initial coding was compiled into a synthesis document from each phase which was then forwarded to participants for review, feedback, and approval thus beginning the iterative aspects for discussion and interpretation of the stories (Kurtz, 2014); (d) with feedback and approval from participants from each phase, the researcher generated initial themes which were then forwarded to participants for review, feedback, interpretation, and approval (Caulfield, 2022; De Fina & Georgakopoulou, 2012; Gehart et al., 2007; Riessman, 2008); and (e) participant feedback was then compiled and used to refine themes, name the themes, and clearly define/describe each of those themes with participants’ direct quotes (Braun & Clarke, 2006). Participatory narrative analysis within this PNI project was unique because it encouraged participants to fully engage in an authentic collaborative, sense-making data analysis process, which facilitated the interpretation of their well-being stories and to determine common themes of what was needed to support the well-being of outsider female social work providers in northern Saskatchewan, Canada (Kurtz, 2014).
Ethical considerations
A Certificate of Approval (Beh ID 851) was obtained prior to beginning this project. Participants were advised in writing and verbally at the onset of their first interview that their participation was voluntary, and they could withdraw at any time. Additionally, participants were informed that their data would be treated confidentially by the researcher but cautioned that confidentially among participants within the group could not be guaranteed. Because participants oversaw how their stories were told and the information contained in their transcripts, informed consent and transcript release forms required signatures. Furthermore, transcript release forms required participant signatures for each phase of the project. Finally, participants were given a list of supports available to discuss possible negative responses to any one of the interviews.
Results
Themes
The primary focus of the project was to work in partnership with providers by building trusting relationships to gather their well-being stories, gain an understanding of needed supports and, in turn, make recommendations to transform/improve their northern Saskatchewan work environment. Participants emphasized the following key themes specific to their well-being stories: understanding the colonial trauma history of Indigenous peoples is crucial for providers; personal growth and building trusting relationships is essential, particularly as an outside provider; northern work is complex and impactful including direct and/or indirect secondary trauma; and safety and well-being supports are required for providers to carry out effective northern trauma services. Figure 2 summarizes the polarities of the job (positive experiences versus barriers/roadblocks) with the discussion of resulting themes and categories following.
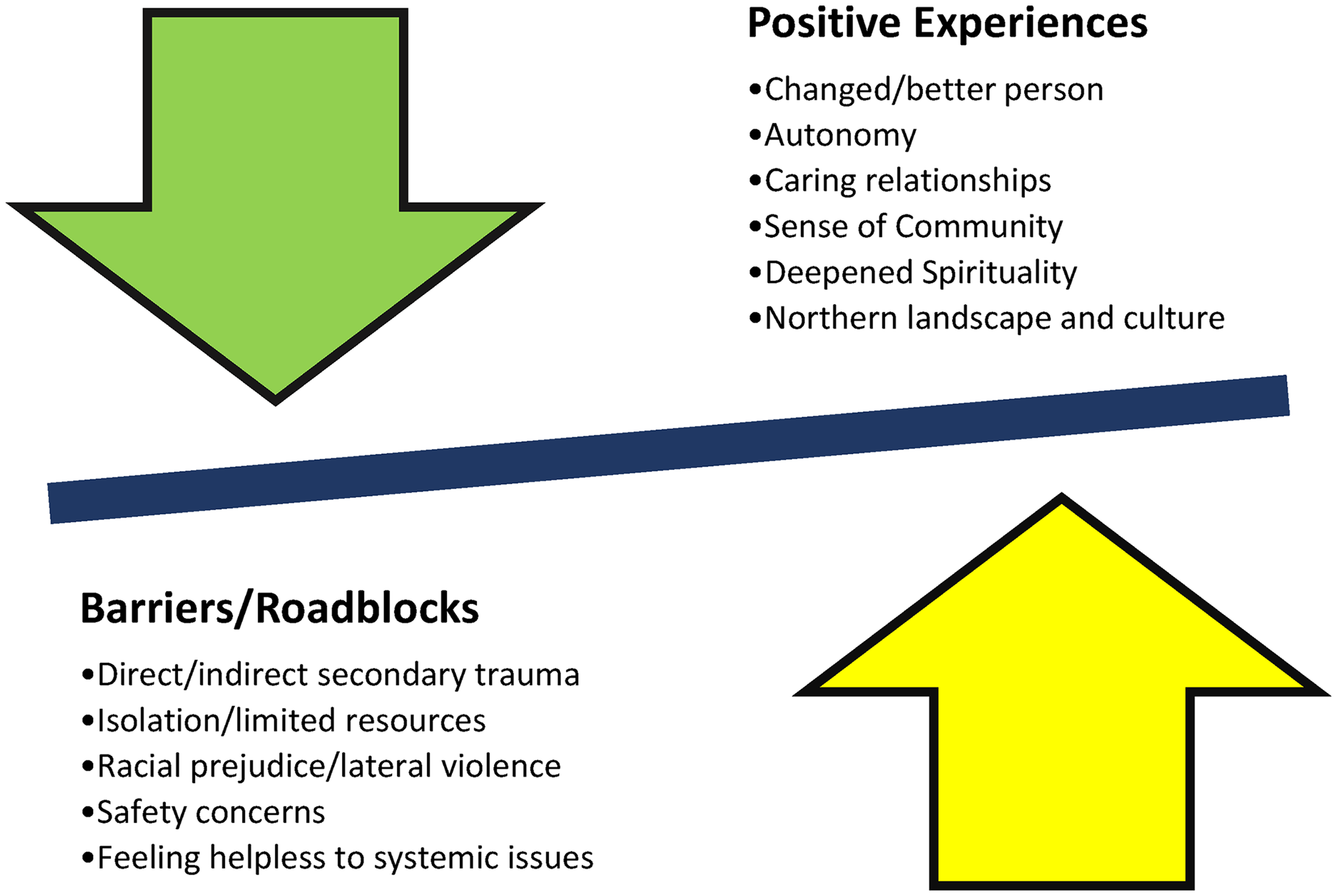
Positive job experiences—job barriers/roadblocks.
Understanding colonial trauma through critical self-reflection
Providers emphasized the importance of learning about the historical colonial trauma experienced by Indigenous peoples, as well as acknowledging and examining their own colonial history to provide services in northern communities. One mental health provider shared the following: Your eyes can’t be closed when people are right in front of you and telling their story. You can’t look the other way and think that this had nothing to do with me, and this has nothing to do with our history, and our government, and our churches, and our people. (Provider)
Providers indicated that they had no tolerance for racism and were confident to confront it. This included within their own families, even if it meant severing relationships with racist relatives. Participants reported that they had to acknowledge their role in colonization although this was difficult, especially when they are both the helper and the colonizer. For example, one provider stated, “Having to hold the reality of both experiences and acknowledge what it's like for the other person to be on the receiving end of being … seen as the oppressor. And how do you then get to be the helper?” (Provider). Another discussed having to recognize and be accountable for her own colonial history as a white settler. She described her feelings as follows: To acknowledge it … to sometimes feel the heaviness of it … of the sense of responsibility. Of some of the shame that's attached to it and should be attached to the history that we have in Canada. But I also feel a deep sense of hopefulness … we are moving in a better direction. But that there's so much to be done. (Provider)
Participants also discussed needing to understand the ongoing implications of systemic racism on their clients. Systems and agencies that were created to protect Indigenous peoples have unfortunately created further barriers and roadblocks for northern communities. A participant shared this very powerful story about food service policies that have been imposed on northern hospitals. There was this man who would go fishing every morning and would bring fresh fish for the patients. Then take them to the kitchen and it was local people cooking and, also caribou. People from the north—when they come down to the south—they don’t feel very well living on southern food. He was supplying those things … through his kindness and his efforts he was taking care of the patients of the hospital. Now a provincial health dietician comes and what happens? … Get rid of that. You can’t have that. You know what we ended up eating? What we call mystery meat. (Provider)
To understand and support the well-being of northern Indigenous clients, providers recognized the importance of understanding the colonial history and developing strong trusting relationships. In addition, all providers recognized the importance of building relationships within the communities in which they worked; to support their own well-being.
Relationships central to northern work
Participants discussed the need to build strong trusting relationships within northern communities to reduce isolation and forge alliances to execute the work. This included having someone within the community to reach out to when they needed support, or just someone to spend time with. One participant said, The human connection is so powerful … I feel very honored how I’ve been welcomed into the community and welcomed into people's stories, and that's honestly life-changing for me … It's probably the most rewarding work I’ve done. (Provider)
Participants reported that building trusting relationships within the community was the most important component of their job. They also acknowledged that building trusting relationships took time, patience, and understanding, particularly as an outsider. Providers who did not prioritize relationship-building felt more isolated. It was also important for providers to connect with their coworkers to reduce feeling isolated and generate local well-being supports, as described below by one participant: I think we need to take the initiative to really connect with the staff who are doing work up there and be cautious about coming off as judgmental, or that we have something to offer that they don’t. (Provider)
Although providers with time and patience were able to build strong trusting relationships within northern communities, it was critical that providers understood the implications of colonization on these relationships. Providers described an underlying tension working within northern communities as they struggled to build trust as a mainstream outsider, government-approved social worker, likely Caucasian—which could trigger historical colonial trauma.
Racial colonial tension
Providers were often subjected to stereotyping and racial prejudice in northern workplaces. They felt that the negative comments regarding outsiders and non-Indigenous providers in northern communities stemmed from a position of oppression and the effects of ongoing colonial trauma. In this context, participants emphasized the importance of engaging in self-reflection to process these comments by community members and to “not take everything personally” (Provider). Participants also provided illustrations of being bullied by staff, management, and community members which included inappropriate comments, a lack of inclusion, and disrespectful behavior. Participants reported feeling exhausted, overwhelmingly anxious, and burnt out due to having to deal with lateral violence. Providers also said that the lateral violence was from other providers and felt that new providers were most at risk of being bullied and not getting needed support from their coworkers. One participant said, “There's competition for these jobs … lack of working together as social workers … Staff from there … scrutinizing what I had done instead of supporting each other” (Provider).
Providers did not directly confront the issue of racial prejudice due to a lack of job security as contract workers; rather, they relied on community allies to advocate for them. Providers indicated that the lack of support, security and safety undermined their ability to do the work. All participants talked about needing to feel supported and safe to effectively deliver services in northern communities.
Secondary trauma
Providers discussed how working in northern communities and the complex trauma caseloads had changed their view of the world being safe and their need for access to well-being supports. One participant described it as an “ever-present threat to my own personal safety” (Provider), while another explained that she is now “always assessing for danger, always assessing for the possibility of threat” (Provider). Others talked about being more anxious about going out to carry out everyday activities and, in general, being worried that children are in danger.
Safety foundation to well-being
Providers felt that they needed to feel safe to carry out their work, with one participant expressing, “I think that we can’t do the work unless we’re safe. But we do the work even though we may not feel safe” (Provider). Participants were also asked to reflect on whether being a woman in the biological sense impacted their fears regarding safety. Participants felt that safety concerns might be different for men in this role, specific to “the difference around power differential and physical power … and women being objectified” (Provider). Providers indicated being a woman was a factor in being told not to walk around the community and instead to use indoor exercise equipment.
Participants indicated barriers to safety, included not being kept informed of issues that directly impacted them such as boil water advisories, forest fires, or a threat of violence. One provider described the following incident, “A fellow threatened to … shoot us all … nobody told me. Everybody left the building, and I came back after lunch and went oh that's weird—where is everyone?” (Provider). Participants also stated that no one checked on them or provided them with access to debriefing support following traumatic situations. Furthermore, providers were expected to lead/facilitate crisis debriefings even though they had been a direct victim of the traumatic experience.
Further undermining providers’ sense of safety was a lack of access to secure accommodations in the communities. Providers explained that they needed adequate sleep due to the job demands. What is required is “a stable residence to be able to disengage and be surrounded by comfort” (Provider). Providers often did not know who they were staying with, resulting in heightened anxiety. One participant also described how a break-in at her housing unit had impacted her sense of safety. Sitting up with my back against the door because people had broken into my unit and trashed the place … and I’m supposed to sleep in this mess and then go start work the next morning. (Provider)
Northern work complexities
Participants said that there was much planning and preparation required to get ready to travel into northern communities, particularly if you were flying in. As such, providers recounted not having adequate information regarding what they needed when arriving at a community for the first time. The process of getting ready to travel into the community never seemed to get easier, “It's the complexity of packing up … bring my own food … and then you go to work and there's endless chaos with what's going on” (Provider).
An additional complexity described by providers was the need to be aware of political and systemic issues that negatively impact northern communities. Maneuvering systemic concerns was both overwhelming and exhausting for providers. One participant shared the following: What wears me down is the organizational stuff … The injustice … people at the top making decisions for people that they don’t have any idea what their lives are like. That's been heaviest on me my whole career … now I’m not fighting that fight as much as I used to. I’m putting more attention just on what I can do, and doing that to the best of my ability. (Provider)
Many participants described feeling powerless in their capacity to influence change in broader systems that undermine access to effective support services to northern communities. With one participant describing, “I’m completely helpless. I plant seeds whenever I can with whoever I can about stuff. But you’re mostly voiceless in that” (Provider). While other participants discussed jurisdictional barriers that further undermine providers’ capacity to deliver effective services. One participant said, Power and control issues that go on really do bother me … Everybody's so territorial and if we could just work together … it would be so much better for people involved … makes me angry … I have to learn how to deal with that because I can’t change the political scene. (Provider)
Providers reported being so busy with the complex demands of the job, that paying attention to the systemic challenges was too much to deal with. As social workers, participants have received training on systemic challenges that have been imposed on Indigenous peoples in Canada. In addition, social workers in Canada must adhere to the Canadian Association of Social Workers (CASW) Code of Ethics, which promotes “social fairness and the equitable distribution of resources, and must act to reduce barriers and expand choice for all persons, with special regard for those who are marginalized, disadvantaged, vulnerable, and/or have exceptional needs” (CASW, 2005, p. 5). Therefore, feeling powerless puts them at odds with the principles of ethical practice. Although there are roadblocks in providers’ capacity to practice and follow their Code of Ethics, they also discussed their own personal growth gained through their northern work.
Personal growth
Participants were asked, “What has been the positive aspects of this work?.” Participants described now seeing the beauty/resiliency of their clients and needing to be “a peaceful presence (instead of trying) to solve all their problems … very much strength-based” (Provider). Providers also indicated they felt more autonomy or control over their work and are now a better person. Another described the landscape, nature, trees, culture, and history of the north as being “extraordinary” (Provider).
Everyone described a spiritual awakening or strengthening, which enhanced their capacity to work in northern communities, with one participant saying, “Being able to bring that conversation (about the client's spirituality) into the clinician's space … and if we don’t, we’re leaving a very important part of their healing at the door of the therapist's office” (Provider). Spiritual growth was also described as witnessing beautiful moments that sometimes emerged from a tragedy in the community, They had a wake and funeral in their gymnasium … The most beautiful thing I saw … the way everything is set up. They had her casket, and it was just beautiful all around … the flowers and the pictures and everything. There were a lot of people and there was a large circle, and everybody … waiting to go and visit her casket. As they moved around and there was a drumbeat, a butterfly came in and it flew over her casket, and then it went to the circle that was coming around, and it flew, and it touched on every person in that circle and then it flew out. Nobody said a word, but everybody saw it (began to cry). It's amazing to experience some of the things that I’ve experienced. (Provider)
Most participants claimed that working in northern Indigenous communities had also awakened their family's moral conscience and an early awareness of social issues. Other participants said their families learned about the north and the culture through pictures of the landscape and activities.
Recommendations for well-being
Collective stories from providers supported a process of self-validation, transformation, and healing. Furthermore, normalization and empowerment occurred after telling and reading providers’ stories, When I first read through it (collective stories), I cried … my thoughts were, this job we do is so big. It's so big emotionally, spiritually and intellectually … and we go into these communities just so vulnerable … There was a lot of things that I don’t think I even talked about that I’ve just pushed them down, forgotten them. Hopefully I’ve dealt with them and let them go, but there was a lot of trigger memories coming up as I read … other people's stories … It strikes me … we’re all going into these different communities separately but we’re having such similar experiences. (Provider)
Providers were able to work collaboratively through their shared stories to make recommendations for changes. With one participant saying, “When we start to share, things can happen” (Provider). Participants want to work collectively to develop a “community of practice,” and to collaborate with the Community Advisory Committee to take these recommendations forward to the agencies and policymakers who are empowered to improve the quality of their work environments. Participants wanted more than just a discussion about northern workplace well-being supports and acknowledged that change could take place only with group collaboration. An overall theme and recommendation of needing to feel safe permeated all aspects of providers’ stories and that solutions need to be collaboratively generated. For example, one provider said, “It has to be a concerted group effort for safety … to pool those experiences and then present them somewhere. But not just suggestions for change” (Provider). While another said, There is a certain level of vulnerability in doing this … We are seen as weak if we seek out our own supports and say we need help … We need to do our own self-help … need to normalize the way therapists are feeling … We need to support each other. (Provider)
As such, providers recommended the following solutions to the identified roadblocks to carrying out their work: collective wellness supports, commonly identified strengths of providers, and self-care/healing strategies.
Governance agency supports
Providers want a process to meet on a regular basis and to have access to support, as well as improved screening and training of providers. Participants were concerned that new providers are overwhelmed, and that they have less support than past providers. For example, the government agency in charge of approving providers no longer brings them together in a group setting. Participants made the following suggestions, “Providers need to be offered coverage for their own therapy when exposed to trauma” (Provider). While another said “Once a year, they (government agency) should get them (providers) together and do cultural training … Do a 1-day session around culture shock. Where to go for help” (Provider).
Strength-based attitude/outlook
Providers talked about giving themselves permission to recognize their own worth and needing to acknowledge that their work does make a difference to the lives of people in the north. If a therapist doesn't believe they are making a difference, then they are not in the right place. Anger against the system is okay, but it isn't helpful if you don't use it as a catalyst for working for social justice and systemic change … I believe in planting seeds, and in supporting communities to identify challenges, and to face those challenges in their own way. In time, with consistent support, positive changes become evident despite the systemic challenges. (Provider)
Teamwork needed
All participants in this project expressed a desire to work collectively. Providers want a support network for themselves and, in particular, for new providers. They need access to a team of colleagues and agencies inclusive of a crisis management team to facilitate working together at the community level. For example, one participant commented, “I really miss having a team of other therapists around me that I could talk to” (Provider). Participants chatted about using innovative ways to connect with colleagues such as a private Facebook page for providers, along with a “community of practice.” One participant said, “A community of practice could be a collective voice … Bringing more education and workshops—more of the teamwork approach” (Provider). They said that the well-being of providers could be more effectively supported by having access to a network of northern providers.
They want these improvements because “making it better means things have to change … losing well-trained therapists because things are not changing” (Provider). Participants said improved supports and expanded capacity for self-care also includes more information about the needs of the northern community they will be serving and access to a knowledgeable mental health supervisor. As well, “Professionals need to be more collaborative and refrain from being competitive or defensive, as this creates an unhealthy working environment and can be counter-productive for community members” (Provider).
Long-term relational-based approach
Providers often found themselves engaging in crisis support which they described as ineffective and “just putting out fires” (Provider). All participants conveyed the message that longer-term work within communities was much more effective, as it created the necessary time and space for trusting/caring relationships to develop. For example, one provider declared, “I’m just doing … as best as I can—I do it with love and care in my heart” (Provider). Northern communities struggle to secure long-term experienced providers who are committed and willing to develop relationships with clients and the community to effectively carry out the work. Understanding that patience and effort were required was crucial for providers to avoid feeling further isolated in their northern work. For example, one participant described how she created opportunities to sincerely connect with the community. Being able to celebrate and grieve with the people and being out in the open. Going out to the … store to buy groceries … going to a kindergarten graduation … a funeral or going to a wake and sitting and praying with the people … they notice … going to church on Sunday with them … I really do believe that they knew that I loved them and that I made time for them, and that they mattered at the end of every session. (Provider)
Northern practice specific training
Participants were concerned that providers with little or no trauma work experience who are not equipped to work with people impacted by trauma are being hired in northern communities. One participant noted, “We just throw a lot of therapists into the community, and they don’t know the people. The community does not know them” (Provider). One provider brought up the need for improved screening for northern providers, as follows, “We should be … evaluated every 3–6 months. Approval agency needs to be stricter in their credentials and experience needed” (Provider).
Some participants felt that northern providers should possess a minimum of a Master's degree and clinical experience, while others stressed that providers require specific university level education and direct work experience that includes trauma-informed counseling, case management, as well as proposal and report writing to sufficiently prepare them for northern practice. Furthermore, participants pointed out that experienced providers should be asked to provide input into this training. In addition, seasoned providers and northern community members could play a vital role in mentoring new providers. One participant suggested the following: Getting connected with a local family for orientation to the (northern) community. Making sure there is a person to greet us when we arrive and give us instructions on what's going on. (Provider)
The well-being stories, lessons learned, and recommendations were a culmination of the participatory process in this project. As such, participants were able to share ideas about what they require for improved supports in their northern work environments.
Discussion
Providers viewed their experiences as “hard-learned lessons” (Provider) and talked about how working in northern communities had changed their worldview. For example, participants reported being more cautious and now perceiving the world as unsafe, particularly for children because of the indirect/secondary trauma of their client stories or directly experiencing a traumatic event in their northern work. Although all providers talked about hearing many tragic stories from their clients, they also described a spiritual awakening because of their northern community work, mostly absent from previous research in this area (Bishop & Schmidt, 2011; Coholic & Blackford, 2003; O’Neill et al., 2013, 2016). In addition, providers reported being transformed due to their work, which included broadening their understanding of colonization and acknowledging their own colonial history. Providers expressed the need to engage in a process of critical self-reflection regarding their personal values and cultural principles (Moss et al., 2012). Moreover, participants were now more aware of racism in the world and would not tolerate this behavior within their own families or friendships. Although providers felt helpless to change structural inequalities, which is a key principle of the Social Work—Code of Ethics (CASW, 2005, 2024), they were committed to focusing their time and energy to facilitate client support.
Participants valued building relationships to understand the workings of the community and to fit in as an outsider, while managing high-trauma caseloads without adequate support/resources. Although relationships developed slowly and a certain degree of tension occurred, they were strong, and a genuine authentic trusting space was created. Providers needed to acknowledge their race, culture, and privilege to create a safe authentic trusting space to support discussion, as described by one participant. I have white skin and am perceived to have had White privilege. I’m consciously aware of that in the process (counseling session). Lots of times, I will invite that as part of the process. So, what's it like to sit with me as a White woman? Sometimes, there’ll be some projection of anger … some acknowledgment … around trust or respect as I bear witness to their story. That's kind of having to hold the reality of two worlds … Being conscious of the fact that I do come from what is perceived as white privilege … and as a society, we weren’t subjected to oppression. (Provider)
Strengths and challenges
The collaborative process inherent to PNI provided many advantages. Firstly, the process and results were meaningful to participants and the project was co-created (Kurtz, 2014). Facilitating three narrative interviews with participants over the course of 10 months supported the development of trust. Trusting relationships needed time and commitment to develop; however, the benefits of these strong connections were key to the success of this participatory project (Kurtz, 2014). As such, providers were willing to share their stories with depth and reflection that may not have been possible with another method. Secondly, the audiorecorded interviews were facilitated and transcribed by the researcher in this project. Although this required a substantial amount of time and effort, it allowed the researcher to become very familiar with the data. Thirdly, participants oversaw how their story was told, which included reviewing their transcripts; once they decided it was an accurate reflection of their story, they signed a Transcript Release Form. Lastly, although participants were offered opportunities to take part in all aspects of this project, not everyone was willing or able to do so.
Although there were challenges in this study, trusting relationships were successfully developed over time to gather the data needed for participants to answer project-specific questions. This project was also an opportunity for participants to create a space for healing and transformation, similar to that of narrative therapy, in that problems are assessed to generate a different story to be told moving forward (Morgan, 2000). As such, participants were supported with co-creating their story to understand the impact of the work and what is/was needed to support their well-being, including the development of a “community of practice” in the future.
Limitations of the study
This project also had limitations. For instance, although participant feedback confirmed the overall results reflected their experiences, the sample size was small potentially limiting the transferrability (generalizability) of results (Pinnegar & Daynes, 2007). Potential bias could have also occurred through the small sample of providers that chose to participate in the study. As such, potential biases were acknowledged during the collaborative iterative process between researcher and participants (Gehart et al., 2007). The sampling of participants in this study was therefore purposeful and participatory so that the process, results, and recommendations were meaningful to individuals who took part in the project. Also, the small sample size was arguably necessary to gather thick data.
An additional limitation regarding sampling was the absence of male providers taking part in the study. One of the recommendations going forward is to have male providers take part in a future study. An additional limitation was the complexity of relationships within a participatory project, and the inherent vulnerability of participants taking part in a group gathering (Kurtz, 2014; Mayan & Daum, 2016). To create a safe space at the gathering required discussions with participants prior to the group meeting and reviewing confidentiality with the group at the onset of the meeting. Creating safety included supporting participant engagement, generating a welcoming space, acknowledging participants’ strengths, and nurturing self-reflection (Tetui et al., 2018, NP).
Conclusions, recommendations, and reflections
As a result of this PNI project, participants were able to share their well-being stories about northern Canada Indigenous community work for the first time, as well as how to better understand needed supports. Providers, in turn, want to build, “connections to others going north to do this work so that we together can … serve the communities in a consistent way” (Provider).
Through participants’ experiences and lessons learned, they collectively generated the following list of recommendations, which were co-created to support the well-being of providers working in northern communities: adopt a team approach; address safety concerns; improve management/provider relationships; develop a trauma-informed training curriculum specific to northern Saskatchewan community work; make improvements to the provider approval process and hiring guidelines; and expand access to professional supports, including a “community of practice.” Furthermore, the co-created recommendations generated by participants need to be taken beyond the scope of this project to fulfill the creation of well-being supports for northern providers. As a result, this could help to attract and retain experienced providers, thereby improving the quality of services to facilitate healing for and with northern Saskatchewan communities. As summarized by one participant, “It has to be a concerted group effort for safety-sake. And to pool those experiences and then present them somewhere … for change” (Provider).
Outsider, female social worker providers loved the work, the people, the clients, and the northern communities in which they worked; but, at the same time, they heard shocking and disturbing trauma stories from their clients that had secondary trauma implications. Moreover, the complex and ever-present managerial and political complexities, as well as isolation and lack of services, created environments conducive to burnout. Since the completion of this project, participants’ stories and their co-created recommendations are now reaching the attention of agencies contracting northern providers. As such, resources including a “community of practice” have been implemented to support the well-being needs of northern providers and to improve services for and with clients and communities.
Footnotes
Ethical Approval
Ethical approval for this project was given by the University of Saskatchewan's Behavioural Research Ethics Board (Beh ID 851).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Saskatchewan Centre for Patient Orientation Research Trainee Award—CIHR Funding (2018–2020). PhD Student Research Stipend, University of Saskatchewan; Office of the Vice Dean of Research (2016–2018). This research project was funded by the Saskatchewan Centre for Patient Orientation Research Trainee Award – CIHR Funding and PhD Student Research Stipend, University of Saskatchewan; Office of the Vice Dean of Research (no reference numbers).
Declarations of Conflict of Interests
The authors declare that there is no Conflicts of interest.
Acknowledgements
The authors acknowledge the following for their contributions to this article: the mental health providers who shared their powerful narratives. The authors wish to convey their gratitude to the mental health providers who shared their powerful narratives.