
Abstract
Summary
Meetings to enhance shared decision-making, such as family group conferences, potentially contribute to enhancing meaningful involvement of families. Such meetings are also claimed by some to reduce the need for children to be in care, either by increasing support from family for parents or by identifying care from within the family network. This rapid realist review aims to develop an understanding of how meetings that facilitate shared decision-making between professionals and families might work to safely reduce the need for children to be in care. It identifies mechanisms that are thought to make a difference and contextual factors that influence the impact of identified mechanisms.
Findings
A comprehensive search of academic and gray literature identified 64 documents spanning seven types of shared decision-making meetings. Data from these papers were collected using an iterative process of juxtaposition, comparison, contrast, and combination with a developing program theory. Data from the literature was supplemented with consultation to ensure relevance to the UK setting. The review identified three key mechanisms that made shared decision-making meetings more likely to be effective in safely reducing children's entry to care: enabling participation and engagement; building trust and reducing shame; enabling participation in decision-making processes. It describes how these work before, during, and after meetings.
Applications
The findings help us understand the complicated research findings about the relationship between meetings and care entry and provide a theory about what is needed to make such meetings work that is of practical use for practice and future research
Introduction
The right for children, young people, and families to be involved in decision-making about their lives, and for plans to be focused on their individual needs, is widely accepted in social work literature and practice (Forrester, 2024; Diaz, 2020; Stabler et al., 2019), and is enshrined in legislation and statutory guidance in England (Department for Education, 2014). Social workers must involve children and their parents in all aspects of child protection planning (Department for Education, 2018). However, there is evidence that statutory meetings such as Child Protection conferences—multi-agencies meetings where key decisions are made—do not work well to include family members in decision-making (e.g., Dillon, 2021; Featherstone et al., 2018; Muench et al., 2017).
One way to achieve shared decision-making that has gained wide support is meetings—such as Family Group Conferencing (FGC)—which have the aim of families taking the lead on decision-making for their families. The idea is that, when families take the lead on developing plans for keeping their children safe, they will be able to draw on their knowledge and resources to come up with creative, viable solutions that can work in the individual family's circumstances (Barn & Das, 2016; Connolly & Masson, 2014).
These solutions can then in theory keep the child safely at home, rather than entering alternative care (Mitchell, 2020; Sen & Webb, 2019; Frost et al., 2014). However, there is mixed evidence as to whether this outcome is achieved with these meetings (Nurmatov et al., 2020; McGinn et al., 2020; Dijkstra et al., 2016). A large randomized controlled trial (RCT) in England found a positive effect of FGCs on care reduction (Taylor et al. 2023), but this has prompted substantial debate about the evaluation of FGCs (Morris et al. reported in Community Care, 2019). The issue of whether meetings such as FGCs might reduce the need for children to enter care, whether that is a legitimate outcome for evaluation and, indeed, whether FGCs can be evaluated against outcomes at all has been the object of substantial debate in the United Kingdom in recent years (Schout, 2022).
The review presented in this article seeks to contribute to the discussion about FGCs by developing a theory about how these meetings might work to reduce the need for children to enter care. Our hope is that the development of such a theory will help us to understand the mixed pattern of results in the evidence so far, that it will identify the conditions that make it possible for shared decision-making meetings to reduce the need for care and by doing so it will provide lessons for both delivery and evaluation of FGCs and similar meetings.
A key point made by critics of a focus on reducing care for evaluating FGCs is that inclusive and participatory meetings are a matter of good practice and appropriate processes (Schout, 2022). They are therefore akin to a fair trial or safeguards against indiscriminate stop and search powers, in that their value is that they respect rights to involvement and participation. Unfortunately, the evidence base in this area, while smaller than that for reducing care, is also mixed (Nurmatov et al., 2020). Three factors may explain these results. It is possible that shared decision-making meetings such as FGCs are less good at creating participation and involvement than we believe. It is also possible that we underestimate the involvement that takes place in other ways. We would expect, for instance, that good social workers try to involve family in a variety of different ways. Finally, the lack of impact may be due to the variation in the quality of delivery. The simplest explanation for this finding is that differences in quality of implementation and contextual factors may lead to meetings such as FGCs varying substantially in the impact they have.
Our review has findings that relate directly to this issue. By examining the literature and working with stakeholders we aim to develop a theory about what is required to deliver shared decision-making meetings well. The current literature provides a wealth of descriptions of how shared decision-making meetings should be delivered, and rich insights into the experiences of family members and professionals, the complexities of working with power dynamics, and other key issues involved in delivering meetings. This article seeks to do something somewhat different. It aims to synthesize the chains of causal explanations about how shared decision-making meetings might work well that are implicit or explicit within such research studies. In doing so it tries to articulate a theory about what needs to happen for meetings—FGCs and other meetings with similar aims—to work to reduce the need for children to be in care.
Aim of the review
The aim of this review is to articulate the key mechanisms through which shared decision-making meetings can work to help keep children safely out of care and at home. The review question was: How can shared decision-making meetings work in a child protection setting in the UK to safely reduce the number of children in care?
This article focuses specifically on adult involvement in these meetings as the involvement of children and young people differs somewhat, and is the focus of a separate but related review.
Methods
Design
A realist review is a theory-led systematic review that focuses not only on using the literature to evaluate what works but also asks for whom, under which circumstances, and in what way (Pawson et al., 2005). This form of systematic review emphasizes underlying “program theory” development and provides a theoretical framework that addresses the research question through mixed-method evidence from both secondary and primary sources. The integration of data from the literature and primary data from those involved in areas of an intervention or system aims to develop a refined theory of how an intervention might be expected to work, why, for whom, in what contexts, and to what extent. This is achieved through synthesizing data from interventions in a way that seeks to unpack causal mechanisms that relate to how complex programs work (or why they fail) in specific contexts and settings (Pawson et al., 2005). In social work, we work with human beings, and therefore the changes we seek to create are at some level within people. Mechanisms are therefore underlying and sometimes unobservable human responses (i.e., how someone thinks and feels) which are triggered by changes in context (Pawson, 2008). Contexts are moderators that enable or inhibit mechanisms to produce outcomes (see Kirsh et al., 2017 for a helpful glossary of realist terms).
It is important to understand the conditions that need to be in place for an intervention to have the intended effect, in certain populations or settings. This can produce evidence to inform decisions that need to be made in practice and policy by ensuring that the findings are relevant to the intended application. Prioritizing and refining the theory aims to articulate for policy-makers and practice leaders the essential elements of intervention necessary for it to work well, and what needs to be in place for these elements to operate (Pawson et al., 2005). It is also useful for understanding the patterns of outcomes found in research to provide a foundation for subsequent evaluative studies.
The Rapid Realist Review (RRR) methodology was chosen for two inter-related reasons: (1) there was a policy-identified need to understand “how” interventions might lead to a specific outcome, namely reducing the number of children in care; (2) there was an existing group of studies with rich theory focused data identified in the scoping review.
As well as from synthesizing the existing literature the RRR methodology allowed consultation with stakeholders to explore findings that may have come from different settings, or have limited evidence from the target setting. For example, Family Group Decision Making in the USA has been theorized to be an “on-going process of collaboration and empowerment” (Pennell & Burford, 2000, p.153) linked to a reduction in child protection events. However, it is important to explore whether contexts in the target setting might interact with these mechanisms differently, or whether different mechanisms entirely might be more relevant.
In reporting this review, RAMESES (Realist And MEta-narrative Evidence Syntheses: Evolving Standards) are followed (Wong et al., 2013).
Conduct of the review
Scoping the literature
A scoping review was conducted to identify clusters of evidence about what works to safely reduce the number of children in care (Stabler et al., 2022) (see supplementary file 1 for the search strategy). Studies were conducted by “system level mechanism”—that is, they were grouped not by named intervention—such as Family Group Conferencing—but by ways in which the interventions seemed to work—for example, a facilitated shared decision-making process. This led to nine clusters of studies illustrating possible ways in which the outcome of interest could be achieved (see Wood et al., 2022 for another RRR from this scoping review). One of these clusters of evidence-evaluated meetings that aimed to include families in decision-making to reduce the need for children to be in care.
Searches
The original set of 17 papers identified in the scoping review was used to develop an initial program theory of how shared decision-making meetings are thought to work to achieve the outcome of interest. This then formed a basis for specifying additional searches (conducted in October 2019). These papers also remained part of the overall synthesis.
Additional papers were identified through four search approaches. Firstly, the full results of the scoping review searches were screened again based on the criteria of the RRR. The results were searched using key intervention terms: family group decision-making; team decision-making; family group conferencing; sobriety treatment and recovery teams (START); family first; reunification program (n = 60 studies). Other studies that did not meet the scoping review criteria but had been tagged as of interest to theory development (n = 168 studies) were also included. Two supplementary searches were carried out to identify papers that might not have been picked up the in original scoping review searches: Citation tracking of studies included in the “shared decision-making meetings” cluster in the scoping review (n = 180 studies); and citation tracking of the Children's Social Care Innovation Programme publications that contained the key intervention terms listed in step 2 (n = 12 studies). This second approach to citation tracking was taken to include this particular group of gray literature reports identified as important and relevant by stakeholders.
After de-duplication, a total of 400 studies were included for screening.
Study selection
Studies from the scoping review cluster were automatically included. For additional papers, study selection was undertaken in three stages: (1) preliminary title and abstract screening (conducted by two researchers LS and COD), (2) full-text screening (by one researcher COD) (3) and agreement to include (by two researchers LS and COD). The researchers were guided by the inclusion/exclusion criteria which was broad enough to identify a wide range of material (an inclusive approach). Papers were included for the next stage if they focused on children in or on the edge of care and/or their families; described interventions that fit the description of “shared decision-making meetings” developed through the initial program theory; and were published in English.
In contrast to a systematic review, which judges the quality of the research according to the rigor of the design and methods, a realist review aims to examine whether it is fit for the purpose according to relevance to the program theory. The main question used to guide the appraisal of papers was “does it contribute to theory building and testing?” Studies were not excluded according to their design. Due to the “rapid” nature of this rapid realist review (RRR), the question of rigor was not applied to studies in the screening stage.
In total, 64 studies were included in the final review (17 from the initial scoping review cluster and 47 from additional searches) (see Figure 1).
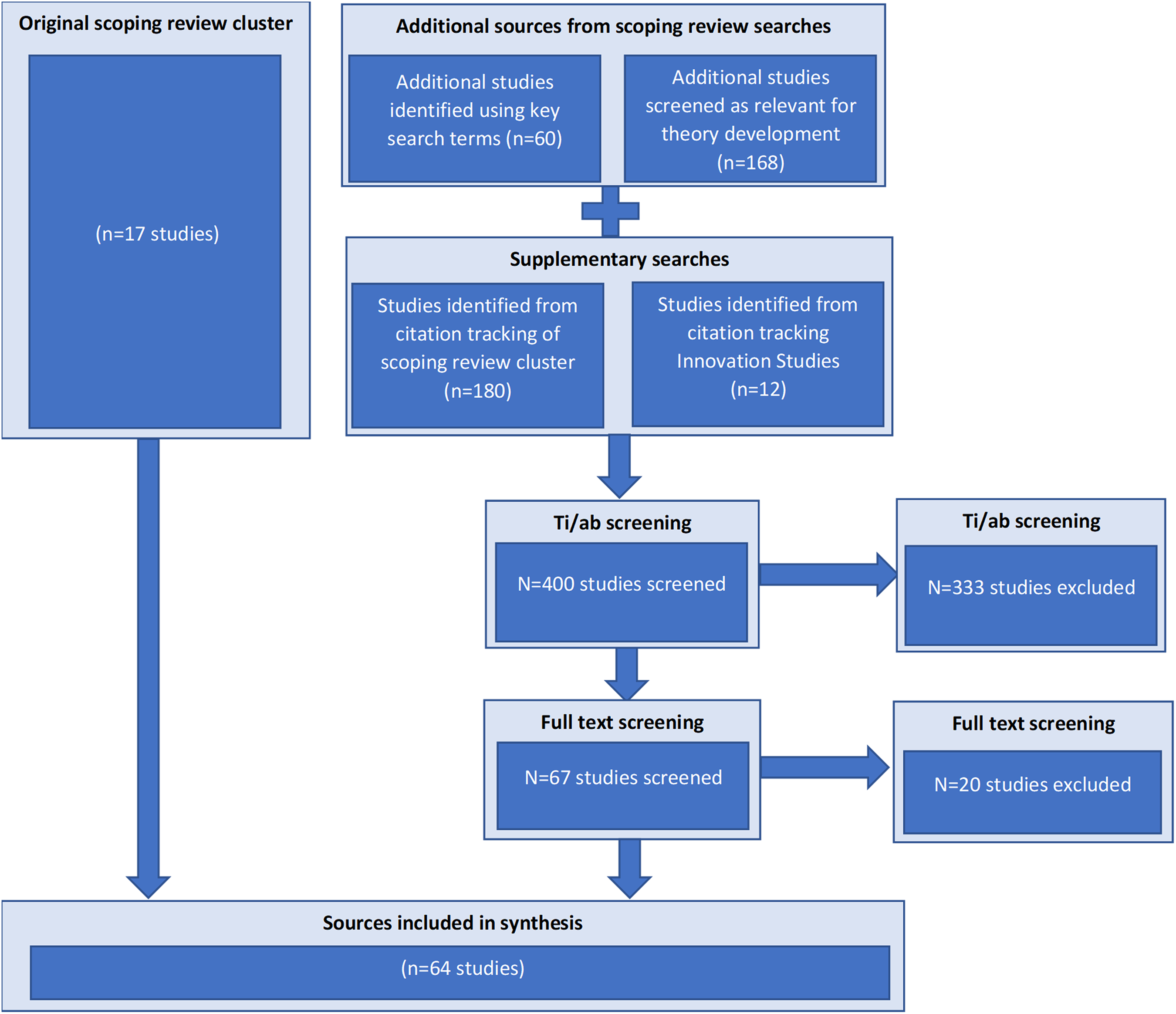
Diagram of rapid realist review searches and screening.
Stakeholder consultation
Consultation data were collected through a group discussion and four individual discussions to ensure that the findings were relevant to the UK setting. Data collection focused on testing the developing program theory. Notes were taken by the researchers throughout these discussions. The group discussion was carried out face-to-face and individual discussions were carried out by one researcher either on the telephone (n = 1) or face-to-face (n = 3).
The group discussion took place with practitioners with experience of social work practice (n = 14) recruited from three local authorities in England which were in the process of adapting their approach to child protection conferences. The local authorities were experienced in delivering Family Group Conferencing alongside other types of social work meetings. Practitioners were consulted about the emerging program theory to gain their UK practice perspective on what felt right, what seemed different in their experience in UK practice, and what was missing. During the two-hour discussion, two researchers presented the initial program theory diagram to the whole group, before smaller groups discussed areas of interest to gain a deeper analytical depth.
Individual discussions were carried out with FGC practitioners (n = 3) from three local authorities in England with experience of delivering FGCs. Discussions focused on the key elements of FGCs, how FGCs worked alongside social work processes, and the differences between FGCs and professional-led meetings. An additional discussion took place with a social care academic (n = 1) with experience as a social worker and as an Independent Review Officer 1 , selected due to their area of research which had focused on family participation in child protection case conferences. The researchers first talked through the program theory, then asked specific questions focused on gaps within the program theory that the stakeholder(s) had direct experience of. Social work professionals were recruited through existing partnerships that the researchers had with local authorities. Professionals were invited to take part in an individual or group discussion.
Data extraction
Data from papers and notes taken during primary data collection by two researchers (LS and COD) were coded in nVivo using a coding tree focused on key realist concepts—program architecture, contexts, mechanisms outcomes, and intervention resources. The data were extracted into an Excel spreadsheet. The spreadsheet identified whether the extracted data were adding something new to the initial program theory that was developed from the scoping review. The extraction form asked if the data added nuance to an identified theme (e.g., communication was already a theme, but new data might emphasize strength-based communication), contrasting with an identified theme (e.g., trust was a theme, but data might highlight the role of skepticism in the assessment of risk) or reinforcing an identified theme (e.g., the reduction of stigma was a theme but data might highlight that this might be particularly important for issues around domestic violence). Each study was extracted by one researcher, and the extracts were checked by another researcher.
Analysis
In Excel, data extracts were re-formulated into explanatory accounts as if-then statements (See Figure 2; also see Pearson et al., 2015; Stabler et al., 2022) to capture theories related to how shared decision-making meeting interventions impact on care numbers. This was carried out collaboratively by two members of the research team (LS and COD) and discussed with the lead researcher (SB). Particular attention was paid to nuance in relation to 1) which parents, families, and children these meetings were most likely to work for and why, and 2) which circumstances shared decision-making meetings were most likely to work in and why.
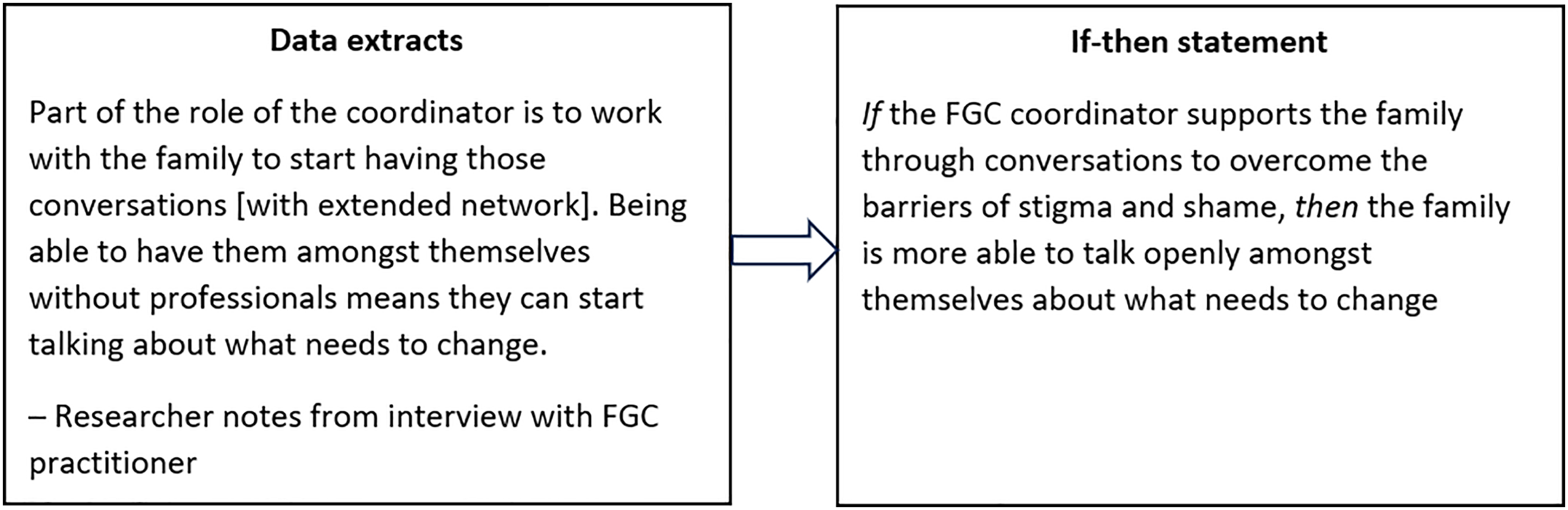
Example of refining extracted data to if-then statements: Theme “reducing shame.”
All if-then statements formed from stakeholder consultations and supplementary papers were compared and contrasted with the existing program theory (see supplementary file 2) to either add nuance or fill in a gap in the initial program theory. Data extracted were critically considered based on credibility (e.g., if only one source made a claim based on the author's own conclusions, and this contradicted every other source, it would likely not be included in the final program theory).
If-then statements were grouped into themes, related to either components of the intervention, mechanisms through which it worked, or moderators that affected whether it worked for certain families. Two reviewers (LS and COD) identified themes through separate coding and then discussion. Final themes were those groupings subjectively considered to best capture what was the most important in the evidence in relation to how shared decision-making meeting interventions work, for which families, and under which circumstances.
Synthesis
Each group of if-then statements was then brought together in a process of consolidation (Figure 3; see also Pearson et al., 2015, supplementary file 3) into a smaller number of richer and more nuanced larger consolidated explanatory accounts explaining how the intervention works, for whom, in which circumstances.
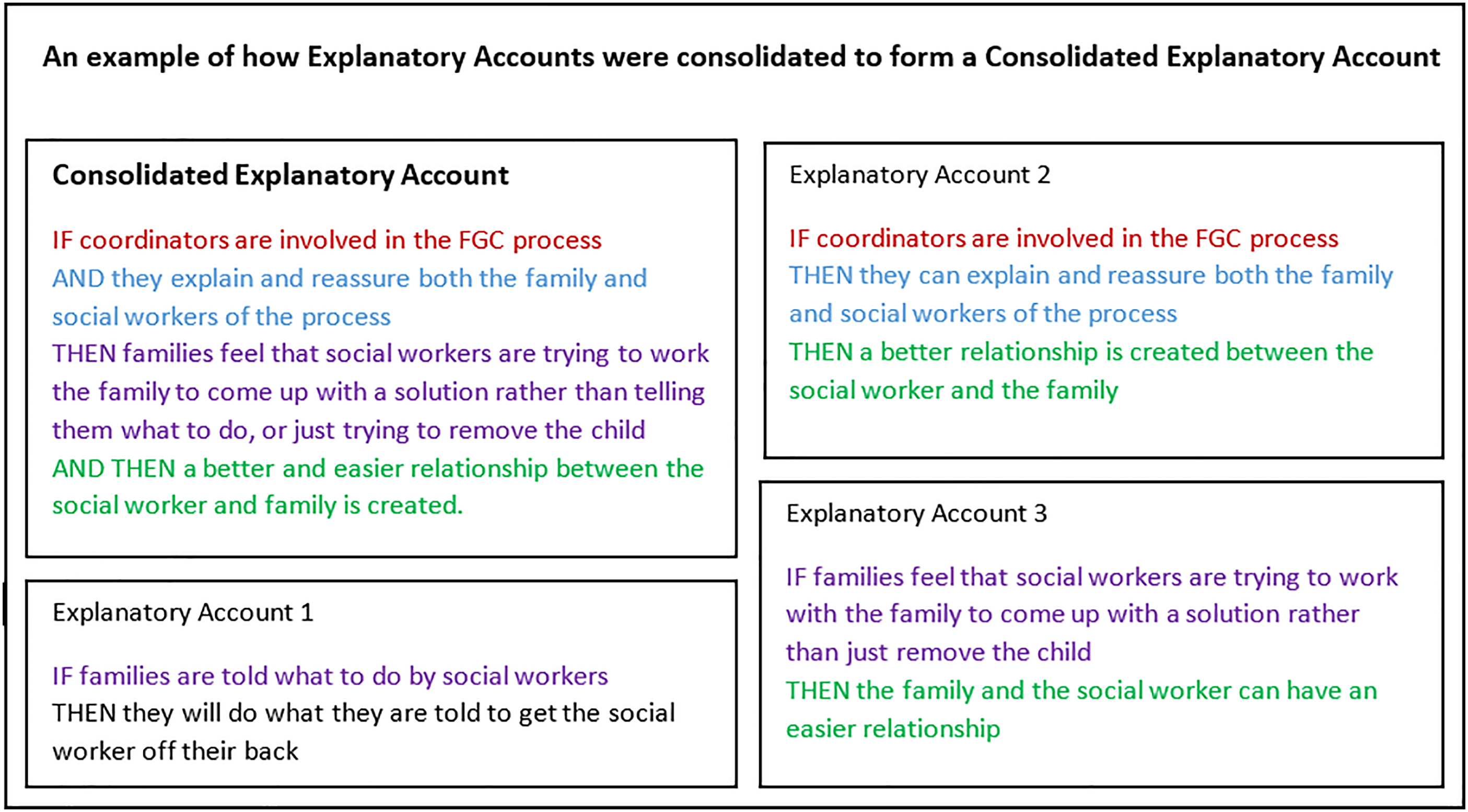
Consolidation process showing how IF THEN statements are brought together.
Evidence for each theory area was mapped out into a program theory diagram by three researchers (LS, COD, and SB). The conceptualization of mechanisms by Dalkin et al. (2015) was used to identify mechanisms through highlighting how resources, contexts, and reasoning interact to produce outcomes. (M (Resource) + C → M (Reasoning) = O) highlights that resources must be introduced into a pre-existing context, which in collaboration induces an individual's reasoning, leading to an outcome. (Dalkin et al., 2015, p. 2)
The resource therefore is the intervention architecture or components (e.g., preparation meetings), which are introduced into contexts (e.g., an environment where social workers have time to spend with families). These can interact to trigger a response—the reasoning of an individual (e.g., trust in the process)—which underpins whether or not the desired outcome is achieved.
Scrutiny and analysis of this emerging program theory diagram, across each theory area, resulted in the identification of eight Mechanism (Resource) + Context → Mechanism (Reasoning) = Outcome configurations (M-C-M-Ocs). These were further mapped resulting in three key mechanisms that seemed most important for increasing the likelihood of the intervention working, alongside contexts in which these mechanisms may (or may not) be activated.
Results
Document characteristics
The majority of the 64 papers included in this review were from the USA, with others (in the order of number of included studies) from the UK, the Netherlands, Norway, New Zealand, Sweden, Canada, Germany, Australia, Sweden, and Republic of Ireland (one paper referred to both the UK and USA and one to Germany and New Zealand). The interventions covered were Family Group Conferencing (n = 33), Family Group Decision Making (n = 18), Family Involvement Meetings (n = 3), Team Decision Making (n = 2), Sobriety Treatment and Recovery Teams (n = 2), Family Group Meetings (n = 1), Family Welfare Conferencing (n = 1), Family Team Conferencing (n = 1), Family Preservation Services (n = 1), Family First (n = 1), Family Group Engagement (n = 1), Family Team Meetings (n = 1), one generic reunification program and one generic legal representation intervention (Table 1).
Included sources in the RRR.
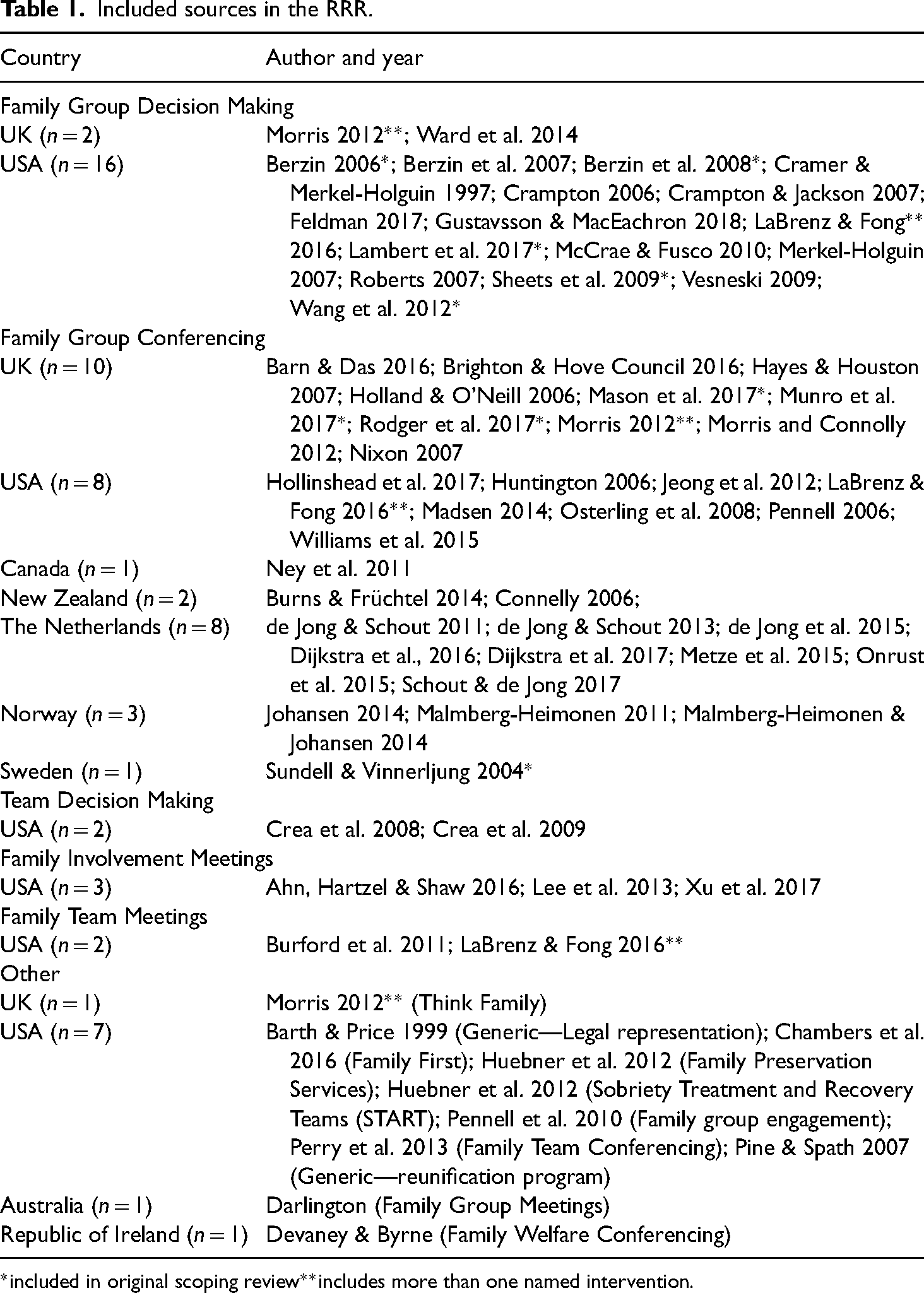
*included in original scoping review**includes more than one named intervention.
Program theory
This section presents the program theory developed in the review. Diagrams and tables illustrate how the meeting process takes place across three stages (before, during, and after the meeting), with each contingent on the success of the previous stages, and the role different participants play within the theory. Gaps indicate areas where there is limited data available to test this element of the theory.
Three key mechanisms through which shared decision-making meetings can safely reduce the number of children in care were prioritized and elaborated (Figure 4): (1) Collaboration and engagement; (2) Building trust and reducing shame; (3) Enabling participation in decision-making. These operate across the three stages of shared decision-making meetings: before, during, and after (see Figure 4) (Table 2).
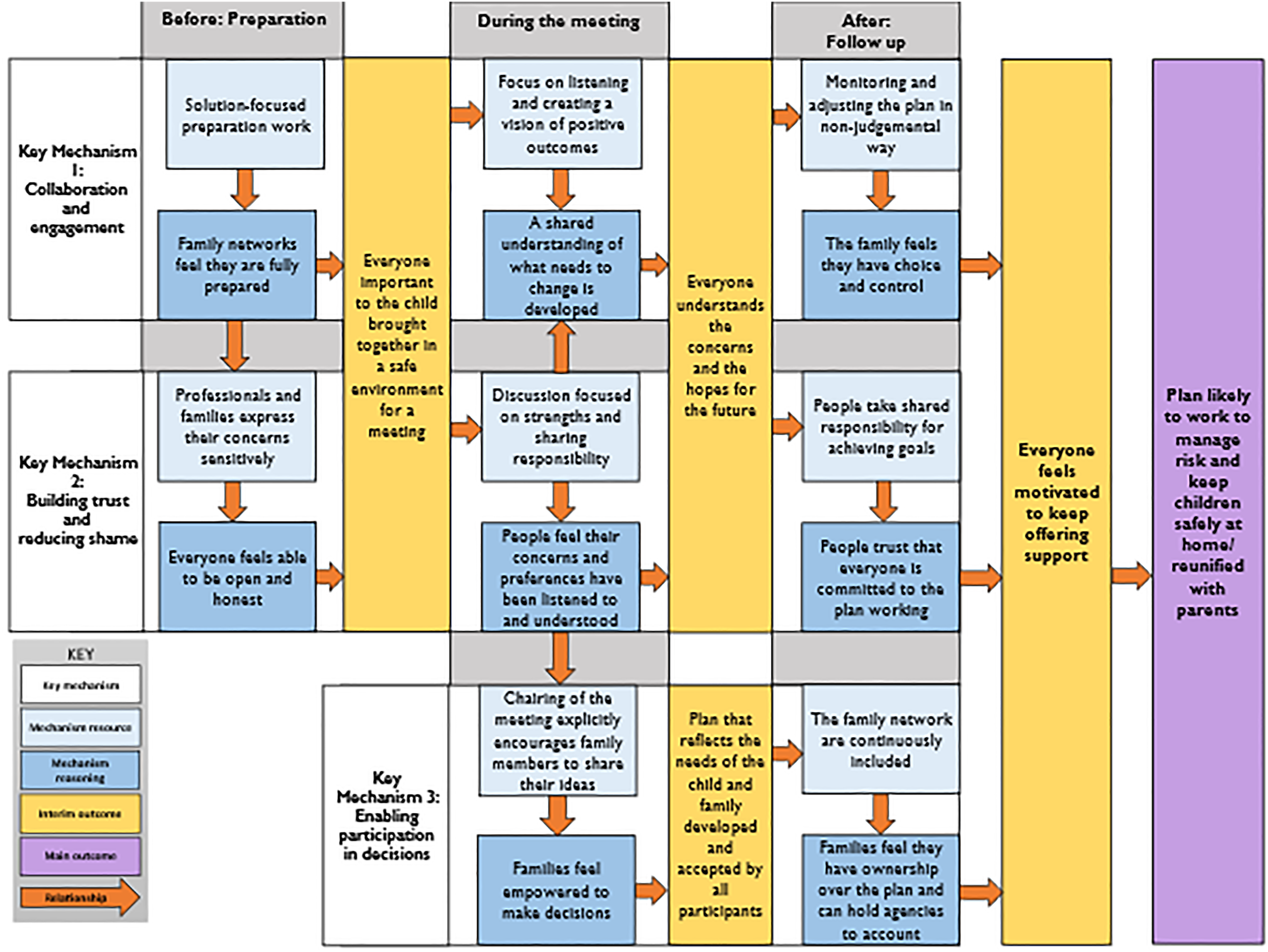
How the program theory suggests that shared decision-making meetings can help to keep children safely at home.
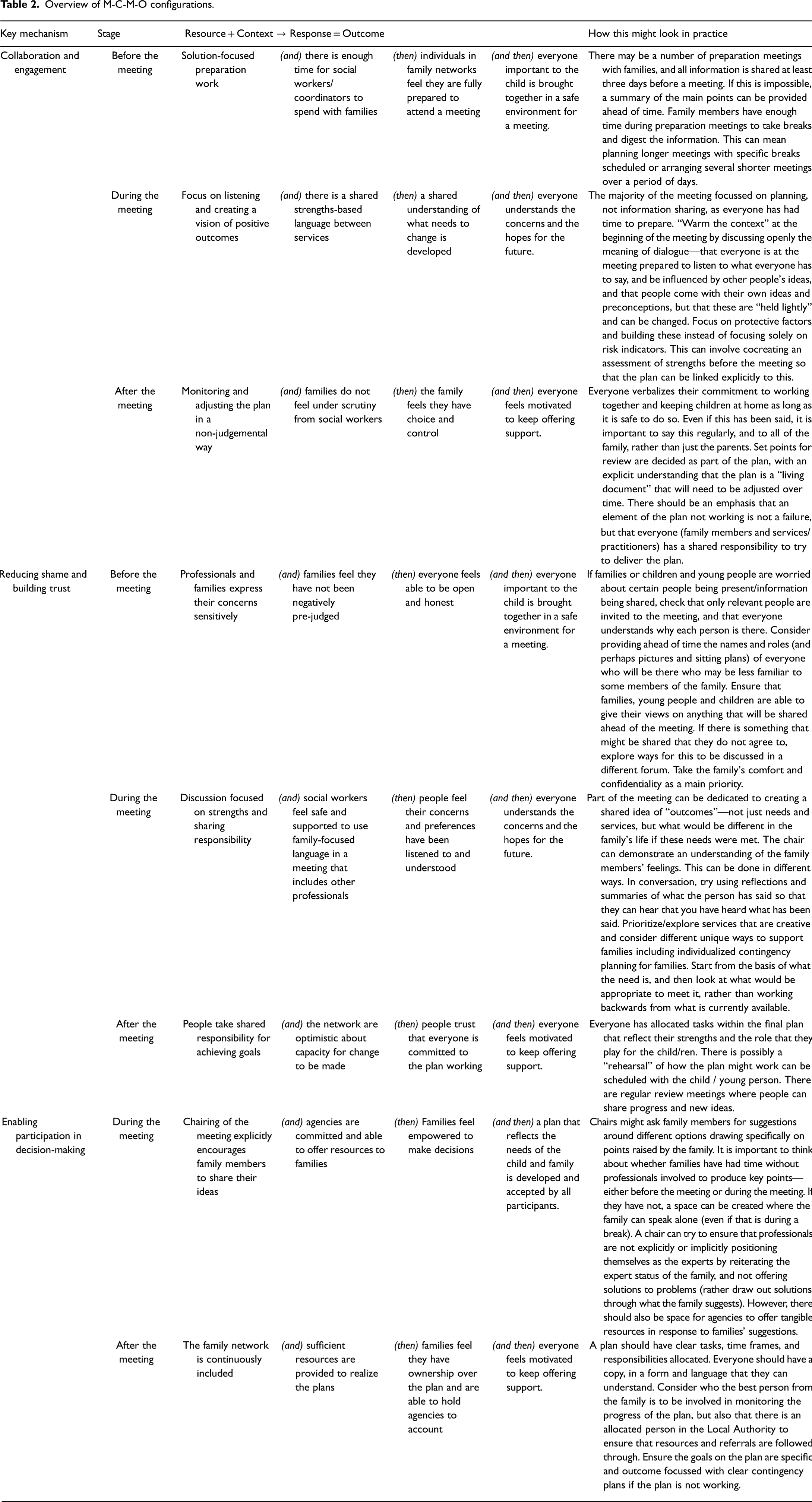
Overview of M-C-M-O configurations.
Key mechanism 1: collaboration and engagement
Collaboration and engagement are built between the social worker and the family through preparation and power-sharing. If this collaborative work is carried out and engagement is built, then families may be more likely to remain engaged with services (both statutory and voluntary) in the future, which can support a safety plan. This key mechanism includes three M-C-M-Ocs:
How this might look in practice
There may be a number of preparation meetings with families, and all information is shared at least three days before a meeting. If this is impossible, a summary of main points can be provided ahead of time. Family members should have enough time during preparation meetings to take breaks and digest the information. This can mean planning longer meetings with specific breaks scheduled or arranging several shorter meetings over a period of days.
How this might look in practice
The majority of the meetings should be focused on planning and not information sharing, as everyone has had time to prepare. “Warming the context” at the beginning of the meeting could happen by discussing openly the meaning of the dialogue—that everyone is at the meeting prepared to listen to what everyone has to say, and be influenced by other people's ideas, and that people come with their own ideas and preconceptions, but that these are “held lightly” and can be changed. A focus on protective factors and building these instead of focusing solely on risk indicators can involve cocreating an assessment of strengths before the meeting so that the plan can be linked explicitly to this.
How this might look in practice
It is important that everyone verbalizes their commitment to working together and keeping children at home as long as it is safe to do so. Even if this has been said, it is important to say this regularly, and to all of the family, not just the parents. Set points for review should be decided as part of the plan, with an explicit understanding that the plan is a “living document” that will need to be adjusted over time. There should be an emphasis that an element of the plan not working is not a failure, but that everyone (family members and services/practitioners) has a shared responsibility to try to deliver the plan.
Key mechanism 2: reducing shame and building trust
Reducing shame and building trust is important to allow families to be open and make plans that consider all important factors and circumstances. This is the main intermediate outcome for these meetings. Even if a plan was not developed after this point, and regardless of whether children enter care, it is an improvement in the experience of family members compared to non-participative meetings. It is therefore an important outcome in its own right.
Shame is an important mechanism in the three stages of the meeting. Feeling shame around involvement with children's services can make families less willing to discuss or disclose this involvement to their family, friends, and neighbors or to invite them to a meeting. This key mechanism includes three M-C-M-Ocs:
How this might look in practice
If families or children and young people are worried about certain people being present/information being shared, the chair/coordinator might check that only relevant people are invited to the meeting, and that everyone understands why each person is there. Providing the names and roles (and perhaps pictures and seating plans) of everyone who will be there who may be less familiar to some members of the family could reduce anxiety. The family network, including young people and children, should have the opportunity to give their views on anything that will be shared ahead of the meeting. If there is something that might be shared that they do not agree to, ways for this to be discussed in a different forum could be explored. The family's comfort and confidentiality should be a main priority.
How this might look in practice
Part of the meeting can be dedicated to creating a shared idea of “outcomes”—not just needs and services, but what would be different in the family's life if these needs were met. The chair can demonstrate an understanding of the family members’ feelings. This can be done in different ways. In conversation, this could involve using reflections and summaries of what the person has said so that they can hear that everyone has heard what they have said and understanding can be checked. Planning might consider different unique ways to support families including individualized contingency planning. The conversation can start from the basis of what the need is, and then look at what would be appropriate to meet it, rather than working backwards from what is currently available.
How this might look in practice
Everyone can have allocated tasks within the final plan that reflect their strengths and the role that they play for the child/ren. Children can have their own allocated tasks too. There could be a “rehearsal” of how the plan might work which can be scheduled with the child/young person. There should be regular review meetings where people can share progress and new ideas.
Key mechanism 3: enabling participation in decision-making
Through the other two key mechanisms, participation in decision-making for families can be enabled during and after the meeting, which helps to ensure the plan is more likely to work. This is facilitated through the previous steps, ensuring that families are given the space, time, and correct information, with the right support to be able to make informed decisions, and that these decisions are supported and respected by professionals. Without work to collaborate and share power with the family, without trusting relationships, and where the family is feeling shame about the situation they are in, it is difficult for them to truly participate equally in decision-making. This key mechanism includes two M-C-M-Ocs:
How this might look in practice
Chairs might ask family members for suggestions around different options drawing specifically on points raised by the family. It is important to think about whether families have had time without professionals involved to produce key points—either before the meeting or during the meeting. If they have not, a space can be created where the family can speak alone (even if that is during a break)—this would be private family time in the FGC model. A chair can try to ensure that professionals are not explicitly or implicitly positioning themselves as the experts by reiterating the expert status of the family, and not offering solutions to problems (rather draw out solutions through what the family suggests). However, there should also be space for agencies to offer tangible resources in response to families’ suggestions.
The mechanisms help to create a shared understanding of risks, needs, and outcomes between everyone at the meeting. Everyone being able to have their say in a safe, supportive environment can lead to the development of a mutual understanding in the meeting of what is going on for the family. This is enabled by families having reached a point of being able to understand the concerns that agencies have, been supported to identify their own strengths and those of their network and felt comfortable asking for support without fear of blame. Through this, a shared understanding can be developed of what is necessary to keep the child safely at home.
Families who feel responsible, but not solely accountable for carrying out the plan may be more open with social workers and the network going forward. This can help to ensure that the situation that brought them to the point of involvement can be better managed in the future as the network will be more knowledgeable about the situation and what support is needed. This could reduce the re-entry of children into care. If parents are open to hearing what professionals have to say about their concerns and are able to accept the responsibility for their part, professionals may feel more confident in the willingness of parents to change to reduce and/or manage risks. There is a gap in the literature around how this works when the risks are from outside rather than inside the family.
Discussion
An innovation in this review is the synthesis of national and international literature with primary data from stakeholders with lived experience and practice knowledge. The integration of these forms of data allows for a contextually relevant and nuanced understanding of how these meetings might, or might not, work in the UK social work context.
The theory identified three key mechanisms that enable shared decision-making meetings to work. These were:
Engaging family members and developing collaboration Building trust and reducing shame Enhancing participation in decisions
Each of these mechanisms had multiple components, as discussed in detail above. Crucially, to work they need to be present not just in the meeting, but also before and after it. In consultation about the potential of these meetings within the UK child welfare system, and in particular where there are serious concerns about the safety of children, it was clear that while working in this way might be desirable, it is also necessary to understand how this links with other practice and oversight. Moreover, some of what the intervention aims to address, such as mistrust between practitioners and families, can be deep-seated and have developed based on prior experiences, and wider cultural conditions related to social work intervention with families.
FGCs and similar meetings are complicated interventions to deliver, highly reliant on the skills of coordinators and the relationships built between individuals. They need to be delivered with a high degree of quality, but that alone is not enough. It seems likely that they only work if the practice before and after is consistent with the principles and practices of the meeting. This involves not just those delivering the intervention in this way, but also other practitioners involved with the family, both within social care professions and other agencies. In other words, introducing shared decision-making meetings into a system that is not focused on family participation is unlikely to work.
This has implications for research, practice, and policy. For research, our model helps explain the high level of variability in findings about FGCs in particular. The quality of FGCs is an important feature of effective delivery, but so is the context within which they are delivered. FGCs are complicated interventions with multiple mechanisms, and therefore delivering them well is difficult. They also only work within a broader context that needs to be supportive of them. It is likely that this complexity is what makes the evidence for FGCs so varied and apparently contradictory: it is likely that what is actually being evaluated varies enormously between studies.
That is why specific guidance for evaluating complex interventions has been developed (Skivington et al., 2021). This guidance emphasizes the importance of the development of strong theories and deep understanding of interventions prior to their evaluation. It is possible that the issue in social work is not that we should not use RCTs to evaluate FGCs, but that we have not done the painstaking work of theory development and empirical refinement that is required to ensure consistent delivery prior to evaluation. We hope that this review makes a contribution to such an endeavor.
These are not just research issues. The same considerations apply to the implementation of shared decision-making meetings in any setting. These are not a simple intervention that can be commissioned and delivered. In the same way that researchers may be prematurely rushing to evaluation, it also seems likely that many policy makers may be prematurely rushing to implement FGCs without considering how they fit into the overall approach to practice within the local authority. Without this, the meetings themselves will struggle to fit within current systems and may fail to bring any sustainable change.
We hope that the theoretical model developed in this article may be helpful for both researchers and those with responsibility for FGCs by outlining the key components necessary to deliver an FGC well. The challenge is to ensure the combination of high-quality delivery and a wider system change that maximizes the potential to involve family members in key decisions about their lives.
Limitations
The main limitation of the rapid approach is a lack of time and resource constraining wider consultation. widely. This review was part of a fast-paced program of research designed to inform the development of primary research as well as summarizing existing evidence. Although we consulted with practitioners and care-experienced young people, we were unable to consult with parents or wider family members who had experience of social care meetings. Evaluations that included qualitative data from families were included, which in some way addresses this gap.
The decision to include studies based on a key mechanism (shared decision-making) rather than a named intervention meant the inclusion of diverse literature. This enabled the development of a more comprehensive theory but limited the ability to draw conclusions about how different types of meetings operate. A related limitation is that interventions that have been subject to more evaluation have more papers included and any that have not been evaluated would not have been included. It would however be difficult to identify papers in this latter category while still maintaining a focus on the main outcomes (reducing the need for children to enter care or improving reunification).
Few studies focused on implementation, meaning an analysis of factors impacting on implementation was limited. This evidence base could develop if there was more clarity around what the meetings are, what they are not, and how those implementing them or evaluating implementation can know about how well they are being delivered.
A final limitation is that, while we acknowledge shared decision-making meetings must be seen in the context of a whole system, theorizing this was beyond the scope of the review. However, we hope the theory makes clear how the meetings, and the participants within them, are part of a system, rather than independent interventions.
Conclusion
If we are committed to including children and families in decision-making about their own lives, then it is necessary to change the relationship between social work and families. FGCs and similar meetings may have a part to play in creating this change. However, this is not a simple undertaking. These meetings require a high degree of skilled practice to ensure parents and others are treated in ways that reduce shame and stigma, promote inclusion, and create genuine involvement in decision-making. It is also clear that this process is not just one that happens within the meeting, it requires preparation before the meeting and it needs to be followed through afterwards. This highlights the fact that any approach to sharing decision-making with families is unlikely to work well in a system that does not share similar values. This is demonstrated with FGCs—they seem to work particularly well when they are part of whole system reforms that put listening to and involving families at the heart of good practice (Mason et al. 2017). It is perhaps most appropriate, therefore, to think about FGCs as one of the ways we need to involve families more that can be part of the whole system change, rather than a specific intervention that may reduce the need for children to be in care.
Supplemental Material
sj-docx-1-jsw-10.1177_14680173241258891 - Supplemental material for How might shared decision-making meetings reduce the need for children to be in care? A rapid realist review
Supplemental material, sj-docx-1-jsw-10.1177_14680173241258891 for How might shared decision-making meetings reduce the need for children to be in care? A rapid realist review by Lorna Stabler, Chloe O'Donnell, Donald Forrester, Clive Diaz, Simone Willis and Sarah Brand in Journal of Social Work
Footnotes
Ethical approval
Ethical approval was not sought for this study as it was a review that did not include collecting primary research from participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The review was supported by funding from the Department for Education, England, UK (grant number 41070002828; 16.10.2017). The CASCADE Partnership received infrastructure funding from the Welsh Government, through Health and Care Research Wales.
Declarations of conflict of interests
The authors confirm that they have no conflict of interest with respect to the material submitted in this article.
Authors contributions
All authors contributed to developing of the manuscript. LS, COD, and SW conducted literature searches and screening. LS and COD carried out the synthesis of the data, with oversight and training from SB. LS wrote the final manuscript with input from the co-authors. DF and CD proofread and contributed to the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.