
Abstract
Summary
Competence is an essential part of any decision-making process. In child protection, it is challenged by the controversial nature of child removals and the vulnerable situations which children and parents experience therein. This article examines how and on what grounds social workers view parents and children to be competent to give their informed view in care order proceedings and what they do if doubts about competence arise. The analysis is based on 30 interviews with social workers in Finland.
Findings
The professional ethos and ethics of social work were embedded in the social workers’ descriptions of children’s and parents’ competence. The social workers were confident that the parents and children (of certain age) were competent to give their informed view about whether to consent to the care order proposal and the proposed substitute home. When they spoke about competence ascribed with hesitation, they described the vulnerability of service users, as well as their attitudes and withdrawal from contact. In the cases, social workers emphasized a strength-based view of children and parents and aimed to ‘talk more’ with them and to ‘give them more time’ to support their right to give an informed view.
Applications
Social vulnerability and competence should be explored reflectively in relation to decision-making in child protection. A better understanding of their interrelation makes social workers more competent to support the service users’ right to be included in decision-making. Critical awareness is needed to recognize when ‘more talk’ is not enough to realize children’s and parents’ rights.
Introduction
Self-determination is one of the iconic principles of professional social work (Furlong, 2003). The principle marks the autonomy of individuals and the individuals’ right to make their own decisions as key values in social work. This emphasis is found in both the traditional as well as the radical writings of social work (Furlong, 2003). However, self-determination is not the only concept to address the autonomy of individuals in social work. According to Furlong (2003), the early writings of social work used the term participation (as did Mary Richmond), and more recent writings in neoliberal environments may employ the term individual choice to address the rights of individuals in a somewhat similar way. The principle of self-determination is iconic but also idealistic and rests on Western values, as Furlong states: ‘being in charge of one’s life is a shibboleth in the western, developed world’ (Furlong, 2003, p. 185).
The fulfilment of individual autonomy in its full meaning is rather difficult in social work as the values and norms of society may conflict with the individuals concerned. Consequently, social work is also shaped by paternalism, which interferes with an individual’s freedom for his or her own good (Reamer, 1983). There are certain situations in which social workers are obliged by law to overstep the individual’s self-determination if specific criteria are met. These actions are typically called ‘coercive measures’.
Child protection is a field of practice in which a variety of coercive measures (e.g., child removals) takes place. It is a field of practice in which the autonomy of individuals is constantly contested not only due to the possible use of coercive measures but also due to the emotionally and morally complex nature of the issues dealt with. Child protection is an uncertain and untidy activity, fraught with complexities (Buckley, 2013), and children and parents involved are in a vulnerable position due to psychosocial problems in their family lives as well as due to the formal child protection proceedings. The consideration of the vulnerability of children and parents as a crucial element in decision-making may, on the one hand, be ‘problematizing, patronizing, and oppressive’ and, on the other hand, it may be autonomy-inspiring and resource-legitimating, as suggested by Brown (2011; see also Gupta et al., 2016). Consequently, vulnerability may be seen as a feature which narrows a person’s competence to take part in making decisions or as a feature which sets extra requirements for decision-making processes. In both cases, the parents’ and children’s competence to be involved in decision-making is assessed firsthand by social workers or other practitioners involved in front-line practice, and their assessment directs the intensity and forms of involvement in the decision-making processes.
Therefore, in this article, we focus on the social workers’ interpretations of children’s and parents’ competence. Competence is approached as part of informed consent, as will be described in the next section, and it will be explored empirically by analyzing social workers’ reflections on the decision-making processes in which a child has been removed from parental care and placed into public care. The study is located in Finland, where the decision-making process of care orders is divided into two types based on whether the parents and children consent or object to the proposal in a hearing organized by social workers. As a consent-based care order has the same legal implications as an objection-based one, it is essential that parents and children give ‘informed consent’ when they practice their right to self-determination. We ask: how and on what grounds do social workers view parents and children to be competent to give their informed view in care order decision-making? What do they do if they have doubts about competence? Our approach is explorative as very little research has been done regarding competence in child protection decision-making both in Finland and, to our knowledge, elsewhere. Although the Finnish context differs considerably from many European countries where the courts make care order decisions and informed consent does not matter in the same way (Burns et al., 2017), on a more general level, the aim of the article is to encourage a more practice-based analysis of interpretations of competence in front-line social work, including vulnerability as an issue to consider. The issues of competent service users are relevant to many fields of practice, for example, the voluntary removals of children (Burns et al., 2019).
Competence as part of informed consent
Child welfare systems differ in their ways of recognizing the status of competence, as well as self-determination, since decision-making systems, rationales, and practices differ considerably (Burns et al., 2017). The involvement of children and parents in decision-making is, however, a well-acknowledged principle and norm in legislation and policy, although it is not always easily implemented in the front-line practice of child protection (Berrick et al., 2015; Bijleveld et al., 2015; Bilson & White, 2005; Cashmore & Parkinson, 2007; Falch-Eriksen & Backe-Hansen, 2018; Leeson, 2007; Tisdall, 2015).The obstacles to involvement are often related to practitioners and their skills and methods. Questioning the competence of service users is not prominent in social work; instead partnerships between practitioners and service users are emphasized as an important characteristic of ‘good practice’ (see, e.g., Featherstone et al., 2014; Lonne et al., 2016; Thoburn et al., 1995). Children are an exception as the notion of maturity and the capacity related to it have been given special attention (Bijleveld et al., 2015).
The literature on informed consent is helpful in setting the conceptual context for competence. Competence is part of informed consent, by which service users practice their right to self-determination (Reamer, 1983, 1987). Only competent service users should give their informed consent to any decision concerning them (Reamer, 1987). In Reamer’s view, incompetence should not be presumed for any particular group of service users (such as children or ‘vulnerable people’). He suggests that instead of these fixed groups, one should consider that some groups may have a greater probability of incapacity. He also reminds practitioners that some service users’ competence may fluctuate: they may be capable of giving or withdrawing consent at some points and not at others. If a service user is determined not to be competent, Reamer asks social workers to be guided ‘by the principle of substituted or proxy judgement in which a surrogate attempts to replicate faithfully the decision that the incapacitated person would make if she or she were able to make a choice’ (Reamer, 1987, p. 426).
When addressing the definitions of competence, Reamer makes use of medical research and its approaches to competency. He refers to Appelbaum and Roth (1982) who state that practitioners must consider the ability of the person to make choices, comprehend factual issues, manipulate information rationally, and appreciate his or her current circumstances. In addition, the ability to retain information or the ability to test information is important (Reamer, 1987). These features of abilities are related to an autonomous individual (Ruhe et al., 2016, p. 515).
The notion of relational competence differs from the above skill-based view of competence. In this view, competence originates from social interactions and relationships: ‘capacity is not something that simply appears but something that develops through communication, explanation and interaction with others’ (Ruhe et al., 2016, p. 517). Competence may take a narrative form (Mahr, 2015). Therefore, one should not evaluate competence as a status or skill that one has but as a developing learning process wherein different parties—here children, parents, and practitioners and other narrators—all have an important role. Since competence can be promoted and learned, it is not an objective property that someone has but a socially learned ability and a social construction (De Clercq et al., 2017; Secker, 1999).
As child protection by its very nature is very much about relations, individual autonomy is typically viewed in their context; consequently, a relational view of competence is quite naturally embedded in child protection. Furthermore, social work is committed to empowerment through its professional ethos and ethics in decision-making (Lonne et al., 2016). Consequently, social workers aim to emphasize the existing capacities and competences of children and families, and to enhance them in the frame of ‘strength-based capacity-building’, instead of focusing on the lack of skills (e.g., O’Sullivan, 2011, pp. 50–61). This emphasis on strengths, for its part, may explain why there seems to be very little research on competence in the child welfare context.
Giving consent in care order decision-making
The competence of parents and children becomes an important precondition for decision-making when they are required to express their views on matters which have a considerable impact on their lives. In voluntary child removals, the assumption is that ‘voluntariness’ means that parents and children (of certain ages) have given their consent to the removal. Voluntary removals are rather common in several European countries (Burns et al., 2017), yet studies on the decision-making processes of those removals are rare (Burns et al., 2019). In existing research, there are concerns about the authenticity of consent due to existing power relations in child protection and the ultimate possibility of the use of coercive measures (see, e.g., Alexius & Hollander, 2014; Burns et al., 2019; Leviner, 2017; Lynch & Boddy, 2017). The very notion of the competence of the consent giver is highly crucial for Finnish child protection as, in addition to ‘voluntary placements’, there are two types of care orders in which consent plays an important part (Child Welfare Act, 2007, section 40). Care orders differ from ‘voluntary placements’ (Child Welfare Act, 2007, section 37) in which the parents’ and children’s rights are not restricted in any way. A care order is the most intrusive decision in the Child Welfare Act regarding parents’ and children’s rights. The threshold for issuing care orders is high, and they should only be used as a last resort. When the care order has been implemented, the authorities look after the child in partnership with the parents. In a legal sense, the parents still have the right to decide about their child’s name, religion, and nationality, while the child is in care (Child Welfare Act, 2007, section 45).
Regarding the decision-making process of care orders, the legislation is built on the understanding that children and parents are competent to give their view in regard to consenting or objecting to a care order and, also, that social workers can legitimately use their authority to ask for and document their consent or objection. Consent given by children aged 12 years or older and by parents makes the municipal child welfare authority the decision-making authority (a consent-based care order): the decision to issue a care order and to make a placement is made by a social worker in a managerial position without any interference from the court. If any of the parties object to the care order proposal or the suggested placement, the decision-making authority is given to the administrative court (an objection-based care order). The view expressed by a child who is 12 years or older has the same legal bearing as the view of his or her parents. The legal implications of both types of care order are similar. The types differ only in regard to whether they are made only in the social work domain of the municipality or also in the legal domain of the court.
The preparations for a care order are complex, and they involve a variety of negotiations with children, parents, relatives, and other professionals. Before the preparatory process, the family may have been known to the social services for months, if not for years (Pekkarinen, 2016). The very final view on the care order and placement is heard in a formal hearing organized by social workers. The purpose of the hearing is that the persons in question have the right to express their opinion about the care order proposal and the proposed substitute home and that they have the right to have access to all the material which the public authorities have about their case (Pösö & Huhtanen, 2017). The outcome of the hearing is a documented view of consent or objection to the proposals.
The majority of care order decisions are made by social workers, suggesting that in most cases, ‘consent’ is given by the parties involved (Pösö & Huhtanen, 2017). This is very different from adversarial child welfare decision-making systems, with courts as the main decision-making bodies, as highlighted in several Anglo-American studies (e.g., Burns et al., 2017). The Finnish system also stands out from the other Nordic countries with its emphasis on child welfare professionals making the majority of the removal decisions (Hultman et al., 2018). The practice obviously gives a lot of power to social workers but also to parents and children (of certain ages): they are given the power to say that the child can be taken into public care without court involvement. We argue that it is important to acknowledge the many aspects of institutional power in regard to service users in these decisions (e.g., Leviner, 2017; Pösö et al., 2018), but we only focus on the issue of competence in this article. It is, after all, an essential precondition to expressing one’s view.
Following on from that, it is rather surprising that the Child Welfare Act does not provide any criteria for competence or instructions for the assessment thereof. The overall assumption is that parents and children of a certain age are competent to express their consent or objection. In certain situations, parents and children can be assigned guardians, according to legislation not included in the Child Welfare Act, to represent their rights in the proceedings because of incompetence. It is mainly only the Code of Professional Ethics for social workers which sets the frame for competence from the point of view of the self-determination of service users. The code does mention that the restriction of self-determination is possible but only when there are legal grounds, and it does not go into any details and avoids the issues of care order decision-making (“Arki, arvot ja etiikka,” 2017).
The research design: The method and data
This article examines how, and on what grounds, social workers describe parents and children to be competent (or incompetent) to give their informed view in the care order preparatory process. The article is based on 30 interviews with social workers in three municipal child protection agencies. The interviews were tailored to address the care order preparations as narratives of the social workers. Narratives and storytelling can be seen as a form of engagement of the listener (the researchers in this case) with the experiences of the narrator (the social workers in this case; Riessman, 2008). This is why we asked the social workers to narrate, in their own words, a recent care order preparatory process resulting in a hearing. The instruction was to choose a case which was informative about both consent and objection in care order decision-making. After the narrative description, at the end of the interview, we asked questions about informed consent in order to introduce a new layer to the narrative, including the question: ‘In your view, were the parents and the child competent to express their consent/objection concerning the care order and the placement in substitute care in the case you just told me about?’
Although the analysis focuses on the answers to that particular question, we read the fully transcribed interviews carefully to get a sense of the whole interview. The parts of the interviews that included descriptions about competence were separated and the analysis focused on them. These episodes of competence descriptions were approached as constitutive descriptions of competence: competence was ‘talked into being’ (Gubrium & Holstein, 1997, pp. 132–134). The main way of talking about competence was evident: every relevant party was talked of as being competent in every narrated case. We moved on to analyze the descriptions of competence in more detail and realized that these descriptions fell into two main categories: full competence (without any doubts) and hesitations about competence. The second category includes descriptions which were to some extent shadowed by doubt as the social workers mentioned cracks in the service user’s competence.
These two categories were further analyzed by focusing on the thematic descriptive patterns employed by the social workers when talking about competence. We identified recurring themes about how competence is constituted, what causes hesitation and how the social workers act if there are any doubts about competence. The findings are presented under two main headings—full competence and hesitations about competence—and the descriptive patterns are presented under these headings as well. The analysis was done by two researchers to allow for the elaboration of the thematic categories.
The interviews were carried out as part of a larger project in which consent and objection were studied and other material, such as case files and recordings of hearings, was collected. The study was ethically reviewed by Tampere University, and the municipalities gave their research permission for interviews and other types of data gathering. Social workers (29) took part in the interviews on a voluntary basis, and they picked the case based on their own interests with the result of 30 stories. Three social workers narrated two stories each, and two cases were told jointly by two social workers as they had been working intensely on those cases. Many of them explained that they wanted to tell a story about a case which had been quite unique in their professional careers. The majority of the social workers were very experienced in child protection: 16 of them had worked in child protection for more than five years and had been involved in more than 10 care order preparations. Five social workers had experience of less than five years and they all lacked the full qualifications to act as social workers.
Findings
Every parent and child were viewed as competent
The data include 30 stories about the preparatory processes of the care orders of 33 children: 21 consent-based care orders and 9 objection-based care orders. The care order preparations had lasted for 2.2 months on average; a typical starting point for the preparations was an emergency placement. The families and children were typically already known to the child protection agencies much before then. The reasons for the care order preparations related to the misuse of alcohol or drugs, mental health issues, and children’s norm-breaking behavior. Eighteen cases include both parents (shared custody of the child), 11 cases only either the mother (7) or the father (4) with sole custody and 1 case includes a relative with custodial rights. In all the cases, the social workers described the parents and children over 12 years (18 children belonged to this group) as being competent to give their informed view on the care order proposal and suggested placement. This assessment was based on their professional view.
Most descriptions of competence did not include any doubts, as demonstrated in the second column of Table 1. The table also lists the descriptions that included some doubt, showing whether the doubt related to the mother, father, or the child and whether the cases resulted in consent. There are no systematic differences in the social workers’ views on competence based on whether the parents or children consented or objected. Table 1 demonstrates that hesitation occurred when speaking about any party, yet mothers’ competences received slightly more doubts than other parties’. It also presents the number of absent views, that is, when the mother or father withdrew from any contact with the agency.
The patterns of competence descriptions in social workers’ interviews (n = 30).
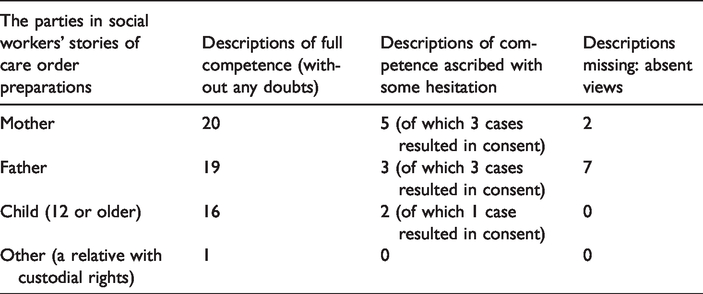
In the following two sections, the descriptive patterns of full competence and competence ascribed with some hesitation are presented. They both include several dimensions which are presented under subheadings. When no doubts about competence were expressed (full competence), the social workers referred to the rationality and understanding that the service users had gained using the services, as well as the relations between themselves and the family members. When doubts occurred, they were talked about in relation to the vulnerabilities of the parents and children, attitudes influencing rationality and the lack of contact between the agency and the parents or children. These doubts, as well as the social workers’ ways to overcome these doubts, are described in detail in the following.
Full competence (without any doubt)
A rational child and parent
When social workers talked about competence, they described it as being a feature of rationality and reasoning which the parents and children demonstrated. Being rational meant that parents and children understood the different aspects of the care order and placement in substitute care. Understanding was talked about as being the key element in rational decision-making; rational children and parents asked questions and verified issues which were unclear to them, and they did not let emotions take over their rational understanding. The rationality of the individuals was further linked with the stability of opinions: the children and parents did not change their opinion from one day to another.
Although the descriptions of rational individuals did not treat children and adults differently, children’s competence was, on the whole, typically highlighted by describing them as being ‘mature, smart, brainy, active and reflective’. Such children were described as ‘almost like adults’ or ‘more mature than children of that age usually are’, that is they were taken to be competent to give their informed view.
Competence acquired as a service user
Full competence was described by social workers as something which children and parents acquired during their time involved with child protection services. In other words, the service user experience plays an important part in gaining competence. Many children had long-lasting experiences of the child protection system, and in some cases, their siblings had been taken into care, which was mentioned as support for their competence. The following extract demonstrates how a young person’s competence was described as being supported by their previous experiences in child protection: I think that this young person, he already had experience of placements. He already knew what it means. I wasn’t left with the impression that he wouldn’t understand what this means on a practical level. (26)
Similar kinds of descriptions were also given about the parents’ previous experiences and their impact on their competence.
Competence supported by relations
Full competence was described by social workers as a relational process between themselves, the children and the parents. When they knew each other, there had been time to ask questions and discuss a variety of issues. A common history meant that there was time to build up a relationship of trust and get to know each other, which made it possible for the children and parents to go through the proposal several times and understand what they were about to make a decision about.
The mutual history also gave the social workers the confidence to assess the competence in unexpected situations. An example of this is a situation where a parent’s capacity to talk and think was clearly weakened due to a life-threatening tumor. A long-term relationship with the parent gave the social worker enough perspective to determine that the parent was consistent in his views and wishes based on what he had previously expressed: He might not necessarily have been able to [give his view], because of his illness, but because we’d known him for such a long time, we knew that he’s very systematically had the same thoughts about things; so I think that, we’re pretty, I’m pretty confident in thinking that he’s been able to assess the matter, and he had the competence and we had the right view about it. (22)
In this extract, the social worker sees that the father’s competence was somehow threatened by his illness, but knowing the father and his views and wishes for a long time supported the social worker’s view of him having full competence.
Competence ascribed with some hesitation
The vulnerabilities of children and parents
Service users’ cognitive constraints, mental health issues, or use of drugs and alcohol caused social workers to hesitate when ascribing competence. For example, one social worker recognized that a parent showed some signs of learning difficulties which was reflected in the care order preparations. Although there was hesitation, the social worker did not conclude that the parent was incompetent. In another case, a teenager’s use of drugs caused hesitation, described in the following extract emphasizing the likely physical implications of the drugs. The age of the child—16 years—was presented as an argument for competence, and the impacts of the drugs were described in a detailed biological manner that is not very typical for social work. Well, in terms of her age she’s of course already old enough that she’s certainly been in some way aware all the time of what is going on. But how should I put this? I think that she’s already drifted into drug abuse in a way that – or a certain kind of mechanism in her head – or addiction – I can’t make an exact diagnosis, but it drives her a lot in this matter; so, in that way, the question of whether she is able to understand why we’re trying to restrict her – I don’t really see it. But so she’s already used . . really many different things, and intravenously for some periods of a week or even two, so now I don’t – I think that it has affected her in some way. (28)
When the impact of vulnerabilities on competence was talked about, the social workers also talked about their ways to support parents and children with those challenges. When in doubt, more time was given to the parents and children to understand the process and to form their views on the proposals. Giving more time typically meant more talking: hesitation about ascribing competence was overcome by working more closely with the parent or the child. Special attention was given to the vocabulary, and simple words were used to make the process understandable. The social workers proceeded slowly in order to make sure that the children and parents knew what they were doing, and the parents and children were given repeated opportunities to ask questions. This was a way to guarantee that the children and parents were competent to give their views. This is demonstrated in the next example, where a social worker talks about parents with learning difficulties: We went through it so many times so that I could be certain myself when I prepared for the matter that they were definitely aware of what they were getting into regarding the decision. (23)
This kind of work required mutual willingness to meet and discuss the matter during the process. The work was very much about working on relations and supporting the existing strengths that could be found in the complex circumstances of the people involved.
Attitudes influencing competence
If consent was given or denied very easily or if the view of the parent did not recognize the child’s needs, doubts arose. If the parents were ready to give up the majority of their parental rights ‘too easily’ or if they withdrew from the process and did not oppose the care order in any way, this puzzled the social workers and gave them reason to question the parents’ competence.
Sometimes, the overall difficulties of the parents were so overwhelming that the parents used the meetings with the social workers to talk about their own situation after the care order. A parent might be more concerned about the smaller amount of housing benefit she would be eligible for when the child no longer lived at home than the care order itself. This selfish or immature way of thinking caused hesitation among social workers and made them wonder about the parents’ competence. It raised concerns about how to provide the relevant information so that different parties could understand their role in the proceedings: And the father’s take on this matter has been somehow really … well, from my perspective, light; so I’ve been wondering, for example, whether the father can see from the child’s perspective what kind of an experience it is. (12)
Likewise, doubt about the child’s competence to give his or her view was expressed in a situation in which the child ‘too eagerly’—as seen from the social worker’s point of view—requested to be taken into care. In one case, the social workers wondered if a 14-year-old adolescent was really able to understand what being in care on a long-term basis meant and how realistic her expectations about the placement in substitute care were.
When the social workers talked about attitudes in relation to competence, they also spoke about their own ways of working with those attitudes: they tried to ‘talk more’ with the parents and children.
A lack of contact and challenges in the assessment of competence
In cases where there was little contact between the social worker, parents, and children, the social workers described some hesitation about assessing competence. The lack of contact took many forms. The parents might not turn up to meetings to which they were invited. The exchange of information could be limited to a few text messages. Some parents were out of reach for long periods of time. In some cases, the children remained quiet and did not express their thoughts to the social worker. Sometimes, the social workers met the parents and children for the first time just before, or even during, the administrative hearing. This could be because of staff turnover or the family’s withdrawal from earlier meetings.
The following extract highlights the doubts arising when the social worker did not know the parents well from before and encountered them, in a meeting, in such a state that she thought they might be influenced by drugs. She assumed that the parents had ‘basic competence’, as she put it, and that they were persons who were able to make independent choices. Nevertheless, her own competence to assess their competence was mentioned as well. What she tried to do in order to overcome her doubts was to ‘talk with them’. Well, I thought that they had some kind of a basic competence at least. So in that sense I thought that they were competent. I won’t take a stance on whether they were competent in that instance, nor can I even judge whether they necessarily were . .; they didn’t seem disoriented in a way that would’ve suggested that they were inebriated in that way, but maybe they were possibly under the influence of some medicine or drug to some extent? But I thought that, in any case, they were in such a state that we managed to have that kind of a discussion with them and, based on that, they could express their opinion. They were fully competent people in that sense. (25)
There were several challenges in the situation that had to be overcome. The lack of previous contact meant that this one meeting was loaded with a lot of information and, despite that, the parents had to give their view on the care order. The social worker trusted that the parents’ basic competence enabled them to overcome the possible constraints and to understand the provided information and to express their informed view. However, despite these doubts, she did not invite any external assessment of the parents’ competence.
Discussion
We have seen above that the social workers, in general, were confident in their narratives that the parents and children (12 years or older) were competent to give their informed view about whether to consent to or object to the care order proposal and the proposed substitute home. They spoke about competence as a feature of the individuals, emphasizing rationality in particular, and also as a relational and narrative feature. There were no direct references to any particular theory of competence (e.g., Gupta et al., 2016) or ways to assess competence (e.g., Alexius & Hollander, 2014); yet descriptive patterns were widely shared across the stories. Most evidently, the social work ethos and ethics and the related view of human competence, autonomy, and self-determination (see, e.g., Lonne et al., 2016) were embedded in the social workers’ descriptions of competence.
Unlike the common presumption that children’s capacities are not yet fully developed and that they may lack the competence to take responsibility (Lansdown, 2005, p. xiii), social workers described children as being competent at the age when their views of consent or objection should be included in the preparatory process. The children’s competence was respected, as they were described as being ‘very competent’ to give their view. Especially children’s previous experiences of child protection were seen as supporting their competence to be involved.
When hesitation about ascribing competence was talked about, it was related to the vulnerabilities of the people involved and the circumstances they lived in. The vulnerabilities were of a social, psychological, and relational nature, although related medical vulnerabilities (e.g., the heavy use of drugs and possible learning difficulties) were not absent either. The descriptions of hesitation did not fall into any binary understanding of vulnerability and capacities, but the social workers rather acknowledged vulnerability-related competences as being on a spectrum which changes contextually and situationally (Clough, 2017). The notion of vulnerability is politically, socially, and morally contested (Brown, 2011, 2014; Virokannas et al., 2018), and it may lead to responses that problematize autonomy and that are patronizing and oppressive (Brown, 2011; Gupta et al., 2016; Reamer, 1983) as we mentioned earlier. In this analysis, differently to those concerns, the social workers emphasized a strength-based view of the children and parents: the social workers wanted to ‘talk more’ and ‘give more time’ if they hesitated to ascribe (full) competence in order to support the children’s and parents’ autonomy to give their view. Thereby, they aimed to support the parents’ and children’s understanding of the care order and placement, which goes further than just supporting them in expressing either their consent or objection: the understanding is meant to support them in coming to terms with the psychosocial and emotional layers of care orders.
There is obviously a high threshold for questioning children’s and parents’ competence in child welfare. According to Secker (1999), there is a danger if people who actually are incompetent are labeled competent: they may not be given the necessary protection of their interests and be forced to act in a similar way as competent service users. These selective data do not give any access to processes in which parents or children were deemed incompetent, for example, due to acute mental illness. Unfortunately, there is no information available to cast light on the frequency of such cases in Finnish child protection. One should ask whether ‘more talking’ and ‘more time’ are enough in all situations and whether children and parents would profit from other forms of support or advocacy in order to give their informed view.
Social workers carrying out the preparatory processes should themselves be competent to work with different types of people in vulnerable situations and to estimate when their own assessment of competence is not enough and when parents and children need external support such as support persons. Parents and children are dependent on social workers’ and their readiness to share more time with them. The stories of the social workers highlight clear ambition to support the parents and children in practicing their right to self-determination. However, they also imply that the social workers may change during the preparatory processes and that some of the social workers are not formally qualified to carry out the processes. These hints echo the shortcomings of the Finnish child protection system where there is a high turnover of staff, and the caseloads are so high that the standards for good professional practice are not always met (Mänttäri-van der Kuip, 2016). There is a risk that children and parents in vulnerable situations lack adequate support when they are asked to give their view on care orders. The risk is not eliminated by leaving social workers on their own, leaning mainly on professional ethics and professional ethos without any policy and practice guidelines.
Although it is a small detail in this study, parents’ absent views in the social workers’ descriptions should also be acknowledged. Parents may withdraw from contact with the child protection agency for a variety of reasons. Some may have left the country, some may not be traceable and others may feel powerless to the extent that they do not want to be involved: they are ‘hard to engage’ and ‘hard to help’ (Thoburn, 2010). It is impossible to know whether parents in these cases practice their right to self-determination or whether they have been excluded from a position of self-determination.
Limitations of the study
The data used for the analysis are limited and selective. Competence is a complex issue, and the questions at the end of the narratives of the preparatory processes may only address some elements of this issue. As the social workers were asked to narrate a case story of their own choice, the data are not representative of the whole child welfare practice. The selection of stories made by the interviewees did not, for example, include any cases in which the issues of competence were investigated by external bodies. The question about competence also surprised the interviewees. The uncommonness meant that both the interviewees and the interviewers occasionally had difficulties in phrasing the subject. We were told once that we used the wrong term, and it was not possible to understand the question. The answers were often short and declaratory but also pondered on the different aspects of competence. Nevertheless, we argue that there is a lesson to be learned about the vagueness and uncommonness of the notion of competence in (Finnish) child protection and hope to demonstrate this clearly at the end of the article.
There are disputes in the literature regarding the concepts of ‘capacity’ and ‘competence’ (see, e.g., De Clercq et al., 2017). We mainly use the latter concept.
Conclusions
The professional ethos and ethics of social work are embedded in the social workers’ descriptions of the children’s and parents’ competence to give their informed view about a care order proposal. Consequently, the possible cracks in competence are approached from the point of view of support given by ‘talking more’. Indeed, a high respect for self-determination is highlighted by this analysis. However, the study also highlights how the social workers negotiated the people’s competences in relation to their vulnerabilities and how these complex practices rest on social workers’ own competence to make assessments.
The principle of self-determination is not free from culture (Furlong, 2003). Likewise, the notions of competence, vulnerabilities, consent, and objection may have very context-bound meanings and practices in child protection. Regardless of the contexts, these principles and notions are included, in one way or another, in the range of coercive and non-coercive measures available in child protection. Following on from that, it is highly surprising how little attention has so far been given to social vulnerability and its impact on the spectrum of competences and how social workers can best support the rights of service users. This is a challenge for social work research, practice, and ethics which can make use of the medical or legal understanding of competence or incompetence only to a certain point. Therefore, a more nuanced exploration of social vulnerability and its impact on competences is needed to support the rights of people in difficult and vulnerable situations.
Footnotes
Ethics
The study was ethically reviewed by Tampere University (number 1/2018) and the municipalities gave their research permission for interviews and other types of data gathering.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the Academy of Finland (decision 308 402).