
Abstract
Summary
Local Area Coordination is an approach that emerged during the 1980s and 1990s to support individuals with learning disabilities in rural and metropolitan Western Australia. Offering direct family support, signposting and networking it aimed to improve access to services and promote social inclusion. It leveraged community resources and sought broader transformation through local collaborations and service redesign, as underpinned by a strengths-based philosophy. Scotland introduced a similar model of delivery from the early 2000s for learning disability support. Since 2010, a number of English and Welsh Local Authorities have introduced Local Area Coordination, and in doing so have expanded its support eligibility criteria to include those considered ‘vulnerable’ due to age, frailty, disability, mental health issues and housing precariousness.
Findings
This article provides the first review of developments in England and Wales. Drawing upon published evaluation studies it reflects on Local Area Coordination implementation; reviews the existing evidence base and challenges surrounding data collection; and discusses the competing logic of Local Area Coordination in its aim of supporting individual and community improvement of health outcomes and well-being, and of furthering local government civic engagement and participation.
Applications
This article points to the challenges and opportunities of implementing such a strength-, assets- and placed-based initiatives within Local Authority social service settings. Embedding Local Area Coordination within Local Authority settings requires skilled political and policy leadership. It balances emerging individual outcomes – health and well-being – with the civic mission (values, control and coproduction), and avoids one being subverted to the other.
Keywords
Local Area Coordination: The story so far
Local Area Coordination is an approach that emerged during the 1980s and 1990s to support individuals with learning disabilities in rural and metropolitan Western Australia (Bartnik & Chalmers, 2007). The approach later diffused to those with physical impairments and other subnational jurisdictions in Australia, including Queensland, New South Wales, Northern Territory and the Australian Capital Territory (NDA, 2015). Offering direct family support, signposting and networking it aimed to improve access to services and promote social inclusion. It leveraged community resources and sought broader transformation through local collaborations and service redesign, as underpinned by a strengths-based philosophy. Local Area Coordinators were identified within Australia’s reformed National Disability Insurance Scheme as the main point of contact (NDIS, 2019).
In 2000, a Scottish review of services to people with learning disabilities recommended the importation of Local Area Coordination and Local Authorities were encouraged, but not obliged, to implement the approach (Scottish Government, 2000; Stalker et al., 2008). By 2006, Scotland had 59 Coordinators in post across 25 Local Authorities (SCLD, 2010; Stalker et al., 2007). This number subsequently increased, and by 2009, 80 Coordinators were in post across 26 Local Authorities (SCLD, 2010).
Since 2010, a number of English and Welsh Local Authorities have introduced Local Area Coordination. This has occurred against a broader policy landscape including: the 2014 Care Act (focused around authorities’ duties for needs assessment); National Health Service (NHS) Five Year Forward (developed new models of care); the 2011 Localism Act (devolved decision-making to individuals and communities); the 2015 Well-being of Future Generations Act (Wales) (required public bodies to be more sustainable and long-term); and, inevitably, a prevailing climate of austerity. Most initiatives have the support of the National Local Area Coordination Network – a network and resource for the long-term development of Local Area Coordination in England and Wales.
The introduction of Local Area Coordination in England and Wales has entailed ‘policy morphing’ (Bainbridge, 2019) concerning the eligibility criteria for support. Support is not restricted to those with learning disabilities, but instead extends to include those considered ‘vulnerable’ due to age, frailty, disability, mental health issues and/or housing precariousness (NDA, 2015). In addition, support is available to all, regardless of whether an individual is known or unknown to existing services. Obvious continuities with the original Western Australian model however are identifiable. Support is provided on a locality basis (typically at a ward level of 10–12,000 people), is underpinned by principles of earlier intervention and strengths-based approaches, and entails the development of community-led resources at a neighbourhood level. There is focus on voice, empowerment and the building of stocks of community and social capital.
As argued in this article the two broad missions – of well-being and civic participation – are competing logics that run through Local Area Coordination (Besharov & Smith, 2014), with distinct implications for resourcing, organising, delivering and measuring success within Local Authority settings. These logics have their own distinct strengths, and Local Area Coordination portrays these as individual, community and system benefits, embracing a commitment to evidence-based outcomes and value-driven processes. The contribution of this article is to provide the first review of Local Area Coordination developments in England and Wales, and it addresses this within the theoretical framing of multiple logics. Drawing upon published studies it:
Reflects on the implementation of Local Area Coordination; Reviews the evidence base to date and the challenges surrounding data collection; Discusses a competing logic of Local Area Coordination in its aim of supporting individual and community improvement of health outcomes and well-being, and of furthering local government civic engagement and participation.
Local Area Coordination: Strengths-based, place-based, asset-based working
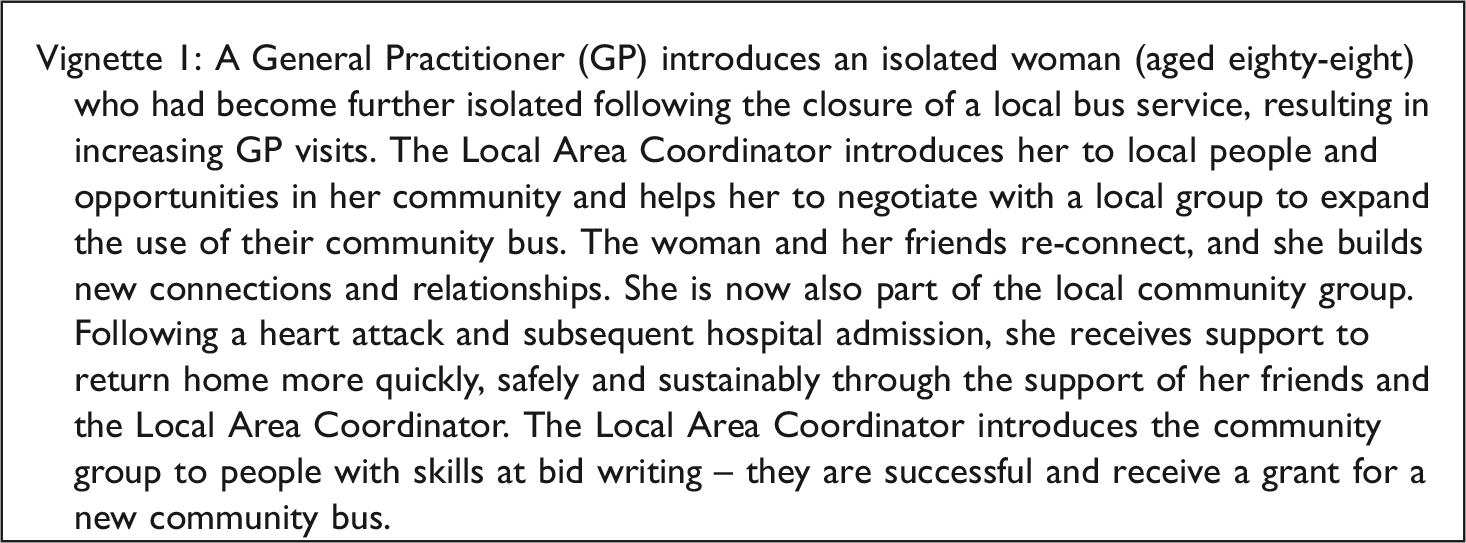
Local Area Coordinators ‘walk alongside’ individuals in communities to help them pursue their vision of a ‘good life’ and shape individual solutions, beginning with a joint conversation to identify their aspirations and their plans for getting there. There is no formal referral mechanism and local residents can contact their Local Area Coordinator directly, or be introduced by friends, family, neighbours, statutory services or community organisations. Local Area Coordinators seek practical, non-service solutions to issues and problems wherever possible. They help to build supportive relationships and networks; facilitate access to and navigation of services; and provide relevant, and timely, information. Moreover, Coordinators draw upon community resources (including individuals, families, communities and services), identify gaps in community opportunities and advance local partnerships with private, community and third sector organisations.
Local Area Coordinators offer support at three levels:
Level 1 entails focused interactions that involve signposting and the provision of information Level 2 involves a longer-term relationship. The optimal caseload for Level 2 engagements is 50–60 people per Local Area Coordinator Community Level support is offered to existing and nascent community organisations (for example, around funding opportunities and support networks).
Local Area Coordinators are typically located in Public Health, Housing, or Adult Social Care line management structures but do not provide services directly themselves. Support is not time limited but seeks to avoid dependency, and is also tailored within each relationship. Thus, While guided by a vision, principles and values that are integral to the quality and focus of [Local Area Coordination-type] processes, the shape of the individual [Local Area Coordination-type] service is deliberately unprescribed, with few ‘off-the-shelf’ products, in order to allow the effective response to changing individual needs. (Bennett & Bijoux Ltd, 2009, p. 11)
Strengths-based practice stemming from the joint conversation, shared agreements and planning provides goal orientation; assesses strengths; incorporates individuals, associations, groups and organisations as resources; and offers meaningful relationships, real choice and informed decisions (Rapp et al., 2005). People from socially disadvantaged groups are habitually described as hard to reach or seldom heard. These terms are used inconsistently and interchangeably to describe inter alia, disabled people, older people, people from BAME groups and those who identify as homeless. Yet, many commentators argue that using these umbrella terms to describe groups implies a homogeneity within groups that does not exist (Brackertz, 2007; Freimuth & Mettger, 1990). Adoption of these terms also risks stigmatisation and locating the problem within the group itself, instead of how groups are perceived and involved (County Council of The City and County of Cardiff, 2009). The emerging vocabulary of Local Area Coordination (for example, introductions, connections, walking alongside and good life) actively avoids loaded and potentially pejorative language, and in doing so emphasises empowerment, resilience and membership. Indeed, individuals are understood to be citizens and community members, not clients or service-users.
As a place-based approach, Local Area Coordination addresses challenges of individuals and families at a local level, usually involving a focus on community building. The approach aims at systems change, and a reconfiguration of relationships between the state, citizens, private enterprise and the third sector – with collaborations addressing causes of community problems (Taylor et al., 2017). For individuals and families, Local Area Coordination aims to support people to find non-service solutions and reduce reliance on services, with supportive relationships, improved health and well-being, and contribution and confidence all understood to be key. At the community level, it seeks stronger and better-resourced communities. At the system level, it targets prevention, the building of social capital, enhanced support and services, and consolidated partnerships and joint working between and across statutory and non-statutory organisations (see Glasby et al., 2013). Place-based approaches acknowledge that both place and social networks shape peoples’ well-being (Glasgow Centre for Population Health, 2012; Melbourne Centre for Community Child Health, 2011). As Gamsu and Rippon (2018) note, in recent years, England and Wales have witnessed a move towards a relational model, whereby local government is a ‘place shaper’ rather than purely a provider of services. There is growing emphasis in local government to shift towards a participatory civic engagement model wherein local people are represented, and involved in, local decision-making related to community assets, welfare and care provision (Cottam, 2014). Largely, this has been set in the context of the Localism Act 2011 and, more recently, interpretations on civic life via independent bodies (see Civil Society Futures, 2018). The opportunities and implications for Local Area Coordination in this context are significant. Local Area Coordination hinges on practitioners getting to know and building positive, trusting relationships with individuals, families and communities, whilst also being aware of community resources and their current and future potential.
Local Area Coordination sits within asset-based initiatives that include Shared Lives schemes, community circles, community enterprise development, asset-based community development, time banks, peer support, community navigators and social prescribing (SCIE, 2015; also see Bickerdike et al., 2017; Seyfang, 2004; Whiting et al., 2012). It is also located in a wider family of community centred approaches proposed by South et al. (2019). Typically, examples of asset-based working are place-based, focused on/within a particular community or neighbourhood. It is a moot point – and one we return to later in discussion – how delivery of Local Area Coordination as a place-based activity sits alongside support by the Better Care Fund 1 and a broader NHS England Prevention Agenda.
Implementation
The first part of our analysis reflects on the implementation of Local Area Coordination in England and Wales, drawing on the published studies and reports (see bibliography) and utilising the 10-point implementation framework outlined by Hudson (2011) (Figure 1).
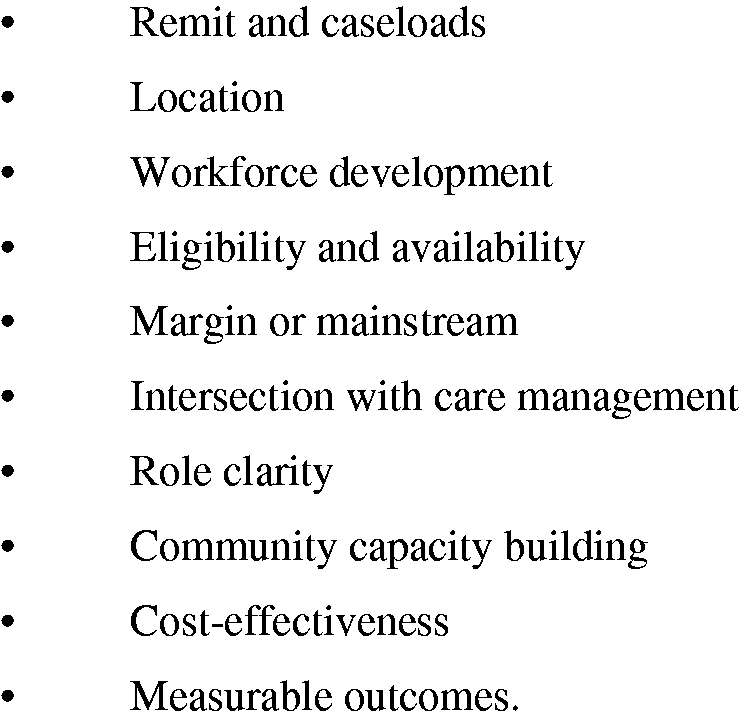
Implementing Local Area Coordination: 10 key issues. Source: Hudson (2011, p. 93).
Location
Local Area Coordination is delivered at ward level within Local Authority settings. A common trajectory has been for the establishment of a small number of Local Area Coordinator posts in priority wards, and for subsequent expansion of posts when funding is secured and benefits/learning from early implementation are acknowledged. Some Local Authorities have blanket Local Area Coordination coverage across all wards (for example Derby City, where Local Area Coordination has a longer history), whilst partial coverage exists in others (for example, York, where Local Area Coordination is a more recent development). Some areas badged the introduction of Local Area Coordination as a ‘pilot’ (for instance, Middlesbrough and Waltham Forrest). Other Local Authorities such as York have avoided such terminology.
(ii) Remit and caseloads
The remit of Local Area Coordination in England and Wales includes adults, children and families. The approach works with all population groups, although there are differences in what this looks like on the ground. For example, the Isle of Wight service worked with people mostly of working age; whilst in Waltham Forest focus tended towards older people and those who were socially isolated. Although early implementation of Local Area Coordination in England and Wales (for example, Middlesbrough) focused on groups deemed to be ‘vulnerable’, programmes more recently have avoided such labelling. Broadly, there is a consistent focus on Level 1, Level 2 and Community Level Support, and an expectation that Level 2 caseloads will be approximately 50–60 people. A recurring comment within evaluation reports (see for example, Lunt & Bainbridge, 2019; M E L Research, 2016) is that Local Area Coordination is working true to its aims and approach.
(iii) Workforce development
Local Area Coordinators are from a broad range of professional backgrounds (including probation, mental health, adult social care, children and family) and settings (both statutory and non-statutory). The emphasis has been on appointee familiarity with the Local Authority and, where possible, the particular ward setting. Local Authorities including Thurrock, York and Waltham Forest have utilised citizen-led panels for recruitment, with community priorities at the forefront of appointment and Community Champions acting as interviewers.
(iv) Eligibility and availability
To be eligible for Local Area Coordination support a person must reside within a specific ward. Cross-ward ‘introductions’ are made as necessary, and signposting to Authority-wide agents (such as Community Facilitators) occurs when individuals are not eligible to engage with a Coordinator due to their home address falling out-of-area. Local Area Coordinators provide a number of dedicated drop-in sessions in locations across their ward. Coordinators are typically available Monday to Friday, and most positions are full-time. Emphasis is on direct engagement rather than on administration and paperwork. Emerging evidence suggests that the workload of Coordinators can be heavy and demanding, particularly as their caseload grows and they attend community meetings and events that are held in the evening (see for example, Lunt & Bainbridge, 2019). Some studies (see for example, M E L Research, 2016) have concluded that Local Area Coordination has been successful in avoiding beneficiary over-reliance on Local Area Coordination as ‘another service’. Thus, Coordinators were working with beneficiaries to build their own capacity and resilience and Coordinators were clear about their remit and focus.
2
(v) Margin or mainstream
Those receiving support include those who (a) are new to local services; (b) have existing, and sometimes longstanding, service histories and (c) have become disconnected from services. Cases range from straightforward provision of information and signposting to highly complex interventions, involving whole-family (and extended family) multi-agency intensive support over many months. Within the Local Authority, those establishing Local Area Coordination intend it to operate amongst the range of services and support available to citizens, and to gain acceptance over time from Local Authority colleagues, health professionals and those within community settings (e.g. Lunt & Bainbridge, 2019).
(vi) Intersection with care management
There was no evidence of Local Area Coordinators undertaking formal care management needs assessment. There is an aspiration, however, that Local Area Coordination will reduce the demands on formal care services and develop preventative and early intervention responses. The link of Local Area Coordination with care management is therefore strategic and financial. The Better Care Fund supports the provision of Local Area Coordination in areas such as Leicestershire and York, and Local Area Coordination is integral to joint working by the Local Authority and Clinical Commissioning Group (see for example, the Better Care Together initiative in Waltham Forest).
(vii) Role clarity
The introduction of Local Area Coordination has seen fidelity to the core principles distinctive of the role. In Leicestershire for example, Local Area Coordination was judged by independent evaluators to have retained its point-of-difference compared to the business-as-usual of traditional services approaches (see M E L Research, 2016). This is a consistent message from a number of evaluations, with relatively little divergence in roles and expectations. Such role clarity stands in contrast to the earlier rollout of Local Area Coordination for those with learning disabilities across Scotland (Stalker et al., 2007) and later, Northern Ireland. Indeed, Vincent (2010) concludes that in these countries implementation was a ‘bolt on’, whereby the addition of components was a compromise with existing services. Across England and Wales there is a process of professional and client familiarisation with the role being developed, and inevitably some perception of intra-professional boundary transgression and unbridled autonomy in work practices.
Notwithstanding fidelity to the model, there is emerging flexibility in how Local Area Coordination is shaping working practices on the ground. Some Local Authorities have sought to eliminate the distinction between Level 1 and Level 2 activity; others have introduced Senior Local Area Coordinators to provide a clearer structure of management and supervision (e.g. Derby City and City of York). The challenge for Local Area Coordination-type processes is to preserve core programme values and programme fidelity whilst simultaneously stimulating progress and avoiding ossification. Thus, Local Area Coordination-type processes have been argued to be a ‘solid framework’ when implemented wholescale and which can be both preserved and enhanced through review, reflexivity and ongoing learning (Bartnik & Chalmers, 2007; also see Chenoweth & Stehlik, 2002). 3 The key argument is that Local Area Coordination models utilise similar frameworks, principles and vision, linked to independence, competency, control, choice and quality of life (NDA, 2015). When a Local Authority adopts the Local Area Coordination model, a national network offers support to ensure fidelity.
The emerging evidence base
This section explores the evidence base for Local Area Coordination and the challenges that programme advocates face (Table 1 details the studies published for England and Wales and their methods and data). In Australia, the approach for learning disabilities has been commended for its capacity to strengthen individuals, families, carers and communities; develop partnerships and support services; and provide good quality, cost-effective interventions with high citizen satisfaction (Bartnik & Chalmers, 2007; Chadbourne, 2003; Vincent, 2010). Australian evidence for individuals with learning disabilities is robust and well cited with several major evaluations since 1993 (both internal and external), and although space does not permit a full presentation of findings, there are noteworthy landmarks. Chadbourne (2003) examined the findings and methods of 17 reports and concludes they portray Local Area Coordination as a success story and previous positive evaluations can be regarded as ‘continuous, enduring, long term and consistent over time’ (p. 1). The Disability Services Commission review of Local Area Coordination in Western Australia commissioned a number of studies including a comprehensive programme overview, analysis of current delivery and costs, and a value-for-money analysis. It concluded that according to measures of consumer and family/carer satisfaction, consumer outcomes, service coverage and cost effectiveness, Local Area Coordination was a highly successful programme over an extended period of time (Disability Services Commission, 2003, p. v–vi), although also identifying the need to re-focus the programme around values, core functions and quality processes. The 2011 Productivity Commission Inquiry review of disability services identified the ‘critical role’ Local Area Coordinators would play in the future operation of the National Disability Insurance Scheme (Australian Government, 2011, p. 413).
Scottish evidence gathered over an 11-month period identified that Local Area Coordinators were highly valued by individuals, their families and other agencies (Stalker et al., 2007). Generally, the study reported that individuals had improved access to services, support and information through contact with their Local Area Coordinator. There were some instances of enhanced inter-agency cooperation, and examples of networks growth and consolidation amongst families, services and the local community.
Studies published for England and Wales and their methods and data.
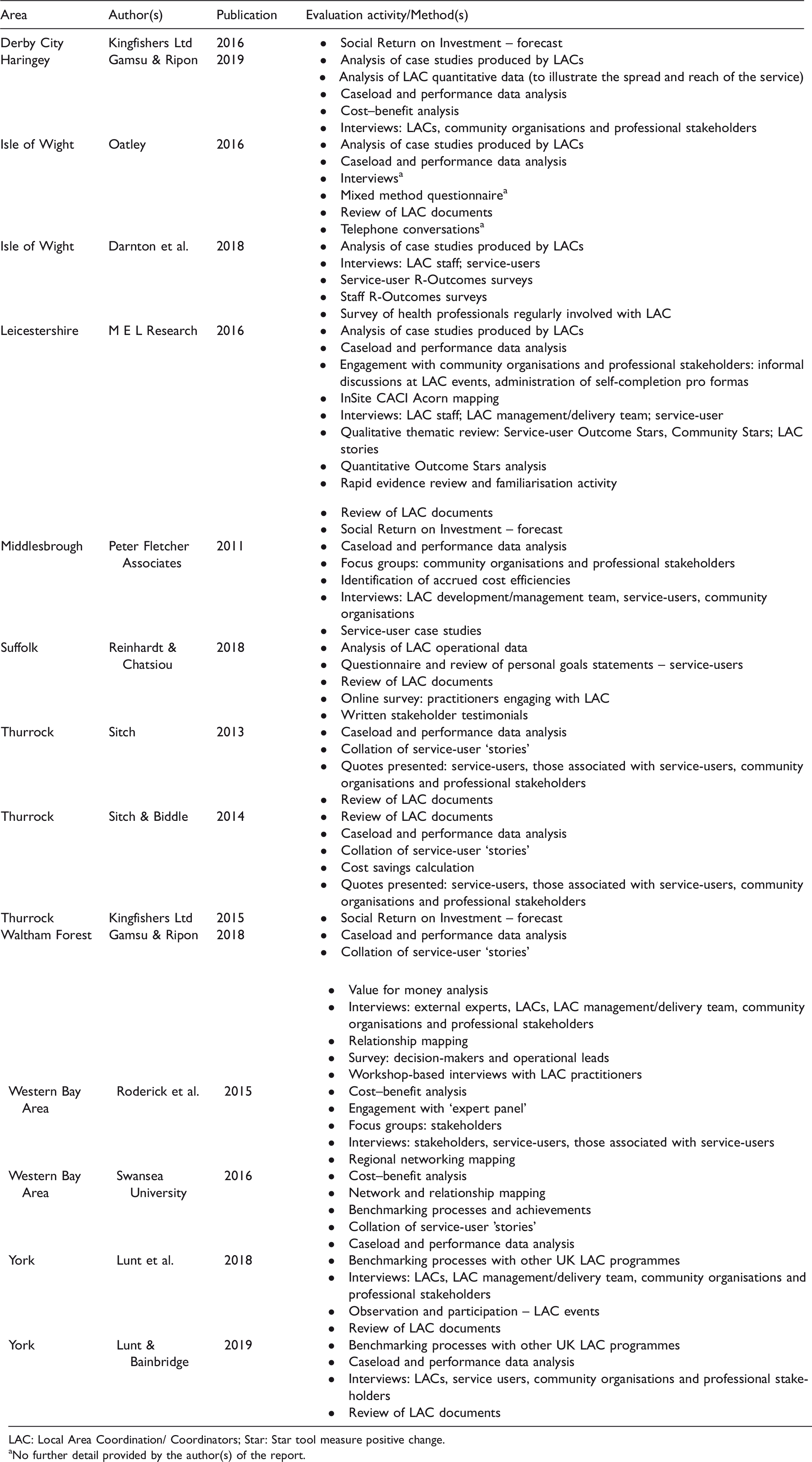
LAC: Local Area Coordination/ Coordinators; Star: Star tool measure positive change.
aNo further detail provided by the author(s) of the report.
Middlesbrough was the first English jurisdiction to ‘pilot’ Local Area Coordination. Ten months post-launch the city’s Coordinators were working with 44 individuals and families who were categorised as ‘vulnerable’ due to physical, intellectual, cognitive, sensory, mental health, age and/or sustained assistance needs. The pilot evaluation (see Peter Fletcher Associates, 2011) reported positive individual outcomes and benefits to agencies. However, there was little evidence to support Local Area Coordinators enhancing social inclusion and community capacity. The evaluators also reported that medium and longer-term outcomes were difficult to evidence given the pilot nature of the intervention.
Thurrock completed two internal Local Area Coordinator evaluations 4 and 14 months’ post-launch (see Sitch, 2013; Sitch & Biddle, 2014). The latter evaluation focused on the support that Coordinators had provided to 256 people of all ages who could otherwise require social service funded intervention. The largest user groups were older people (31%) and people with mental health issues (27%). The evaluation found reductions in referrals and visits to GPs, accident and emergency, adult care, mental health and safeguarding services. In addition, the evaluators noted that some housing evictions had been avoided as a consequence of Coordinator activity. Evaluation of Western Bays Local Area Coordination and Local Community Coordination (LCC) roles 4 included indicative cases scaled up to provide emerging and anticipated outcomes (see Swansea University, 2016). Network Analysis suggested that the introduction of Local Area Coordination had stimulated the building of strong and enduring personal networks.
Two studies of Local Area Coordination in the Isle of Wight are complete. The first was a formative evaluation of recruitment, induction and implementation, and included intervention logic (strategic, system and operational benefits) (see Oatley, 2016). The second, published two years later (see Darnton et al., 2018), identified qualitative and quantitative self-reported outcomes for 85 individuals across the domains of health, personal well-being and experience of using services. Whilst the evaluators found it difficult to monitor long-term outcomes and identify benefits for the wider system, they were able to capture impact in relation to Local Area Coordination staff perceiving improvements for community well-being, quality of care, engagement with healthcare staff, and utilisation of healthcare resources, and stakeholders welcoming the longer-term focus of Coordinators’ work (Darnton et al., 2018, pp. 13–14).
A Leicestershire study (see M E L Research, 2016) included qualitative and quantitative analysis of a sample of Local Area Coordination Outcome Stars, 5 with views gathered from those supported by Local Area Coordination as well as community and agency partners. Findings suggested that of the 520 Outcome Stars completed, measurable outcomes were achieved to a good extent for individuals with respect to quality of life, mental health and well-being, community contacts, reduced social isolation, earlier positive preventative action, greater control, support with debt/finance issues and entry into training/employment/volunteering (M E L Research, 2016, p. 3). However, there was less evidence of progress within health and social care integration, fewer community outcomes, and the evaluators suggested that community impact could take between 5 and 10 years to mature.
In Waltham Forest, evaluators interviewed four Coordinators to explore fidelity to the Local Area Coordination model and to understand better performance and its measurement (see Gamsu & Rippon, 2018). It concluded that Local Area Coordination was located within a wider system of action for local neighbourhoods, dealing with immediate issues within the care and health system, but more strategically contributing to an emerging new settlement with local communities that fostered civic engagement and participation in community life.
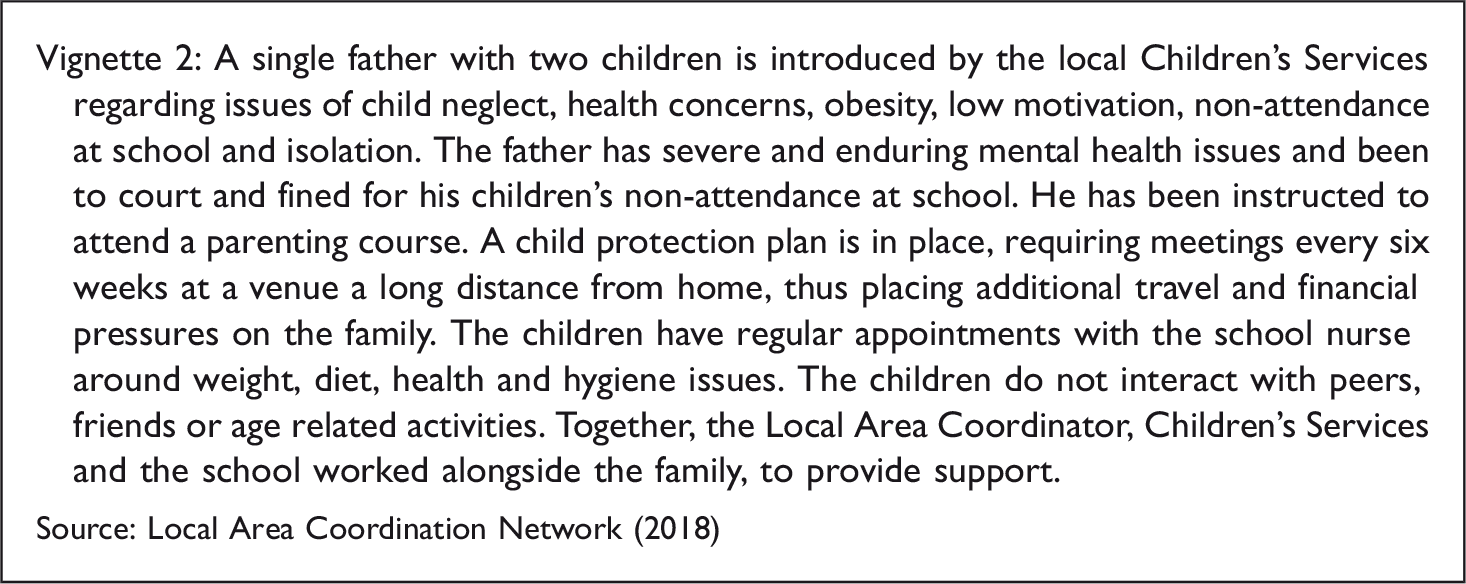
A process evaluation and an early outcome evaluation were conducted for York (see Lunt & Bainbridge, 2019; Lunt et al., 2018). Drawing on performance data, programme materials and qualitative interviews with project staff/those supported by the initiative, evaluators found that real change was achieved as a direct consequence of Coordinator support. This included preventative interventions, for instance, an older resident received support from their Coordinator to strengthen their independent living arrangements via applying for mobility aids and carers support. There were also cases where support helped families navigate highly complex and challenging circumstances. As an example, one of the Coordinators helped a single mother who had returned from a domestic violence refuge to find school placements for her two children. Following issues around low school attendance, the Coordinator subsequently worked with the mother to address her health and financial issues, and to facilitate her children’s participation in school and recreational activities. The evaluators also found that both community residents and stakeholders welcomed the long-term focus of the Coordinators, and that their ability to build strong relationships across their wards was highly valued.
The Haringey formative evaluation of two Local Area Coordinators (Gamsu & Rippon, 2019) identified positive signs of impacts and included personal narratives (case studies) that outlined what were complex issues in people’s lives. It also noted LAC activity that is supporting, promoting and developing community and neighbourhood-based resources. Such support of local people promotes social connection and is a contribution towards community asset development. In estimating financial benefits of Local Area Coordination, the study examined both the Social Return on Investment (SROI) model widely utilised (e.g. Swansea University, 2016), and a case conference scenario workshop with Local Authority and NHS professionals.
(viii) Individual and community outcomes
Local Area Coordination studies have been undertaken relatively soon after implementation and are thus formative and early outcomes-focused. Typically small scale, they emphasise satisfaction and provide narratives of support delivered for individuals and families. This is understandable given that (a) initial implementation of Local Area Coordination is itself often small scale and (b) commissioners and local supporters are looking to ‘build the case’ for (additional) funding and/or to learn as they build. Inevitably, most evaluations provide snap-shots of activity, and coverage of outcomes is weak with regard to community and services/system change.
(ix) Cost effectiveness (and SROI)
A number of studies have utilised SROI – a framework for measuring and accounting for social value or social impacts of activity. A Thurrock SROI study forecast that for every £1 invested, between £3.50 and up to £4 of social value is generated (see Kingfishers Ltd, 2015). A Leicestershire SROI suggested £4.10 in accumulated benefit for every £1 spent (see M E L Research, 2016), whilst a Derby City study identified £4 return for every £1 invested (see Kingfishers Ltd, 2016). For Swansea, the financial benefits ratio was 3:1 (Swansea University, 2016). Questions emerge however about the generalisability and meaningfulness of SROI calculations, particularly as the definitions employed to describe issues (such as depression) are not employed consistently (Gamsu & Rippon, 2018).
Diverted costs and savings have been another area of focus. A Derby City study identified £800k of diverted costs in the first year of Local Area Coordination implementation (Kingfishers Ltd, 2016). Moreover, a Leicestershire study estimated that 53 critical incidents had been avoided as the result of Coordinator support, producing savings to the public purse of between £200,000 and £330,000 per non-incident (see M E L Research, 2016).
A focus on cost savings and deferral is driven by the context of austerity and shrinking public services and the provenance of funding, including that provided by the Better Care Fund. There is some tension between the assets-based and community model of Local Area Coordination and the sharper clinical edge of the Better Care Fund. The Better Care Fund Metrics (for example, a reduction in people seeking residential care) does not easily dovetail with Local Area Coordination processes and timelines. As one evaluation concludes: … it is less plausible for [Local Area Coordination] to have an impact on the [Better Care Fund] metrics in the longer-term. However, the broad approach here is fundamentally about the re-direction of public investment away from treatment and towards prevention; the evaluation has gathered positive evidence of the impact of [Local Area Coordination] in contributing to this agenda. (M E L Research, 2016, p. 4) (x) Measurable outcomes
There are challenges in evaluating asset-based work and initiatives that develop ‘at the speed of trust’ (see Richards & Davies, 2018). As Darnton et al. (2018) note, Coordinators perceived that their work was more likely to improve an individual’s social well-being rather than reduce the likelihood of in-patient admission. Becoming overly focussed on the latter, however, could miss a great deal of the benefit of Local Area Coordination activity (Darnton et al., 2018).
Precise measures of impact are still to be agreed. Reflections on place-based work conclude that understanding an area and building relationships takes time, that working at different levels to link the local with the wider system is important and that building effective relationships with partners as well as being aware of existing local relationships is critical (Taylor et al., 2017).
There are familiar methodological challenges of assessing distance travelled for individuals (e.g. intermediate outcomes and qualitative measures) who have engaged with Local Area Coordination support, including establishing a baseline. As highlighted, some studies have begun to explore quantitative outcomes and changes over time. In doing so, they have nevertheless acknowledged that a tension exists between securing a baseline measurement and ensuring that the trusting relationship between a Coordinator and the person that they are supporting is not impaired by processes of evaluation.
Discussion
The review of Local Area Coordination within England and Wales identifies implementation approaches and lessons. Broadly, there is a consistent focus on Level 1, Level 2 and Community Level Support, and an expectation that Level 2 caseloads will be approximately 50–60 people. A recurring theme within evaluation reports is that Local Area Coordination is working true to its aims and approach. Here, the support of the overarching Local Area Coordination Network reinforces the core principles and ways of working. Alongside such core principles distinctive of the role there is also emerging flexibility in how Local Area Coordination is shaping working practices on the ground. This is in contrast with Scottish experience of Local Area Coordination (Stalker et al., 2007), where researchers identified wide variation in organisational arrangements, access to Local Area Coordinators, and differences in the size of area LACs cover and the total and target populations. There was also unease at the erosion of principles and approaches core to the Australian model within the implementation. For example, there was lack of time for community mapping and networking and relatively little time spent on community capacity building (Stalker et al., 2007).
Poignantly, satisfaction expressed by Local Area Coordinators in Scotland was shaped by the structural location of their post, and managerial support and understanding of the role. Many respondents spoke of the necessity of a broader debate around how aspects of Local Area Coordination fitted within the structural and political context of Scotland, as distinct from that of Australia (Stalker et al., 2007).
It is our contention that Local Authorities are facing longstanding and competing demands as intensified by ageing and austerity, and these demands manifest within Local Area Coordination approaches. Indeed, a plurality of demands in the wider environment of Local Authorities (including value for money, stronger evidence, improved well-being, greater voice, developing trust) gives rise to two distinct logics that are incorporated into ways of organising and delivering services and initiatives that we have reported.
On the one hand, there is a preventative and well-being focused agenda, coalescing around individual and community-level outcomes. Robust well-being frameworks signal opportunities to collect individual data – satisfaction, distance travelled and emerging outcomes – around a range of health and social dimensions. There is certainly a lively debate about the precise selection and nesting of outcome measures including the EQ-5D (3L) scale, Outcome Star measures and Patient Activation Measures, and ensuing technical, methodological and conceptual quandaries (Darnton et al., 2018; M E L Research, 2016). It has been noted how the lack of well-designed outcome evaluations of place-based initiatives work to limit the extent to which firm conclusions about effectiveness are possible (Melbourne Centre for Community Child Health, 2011). Local Area Coordination finds itself enmeshed in these debates and seeks to produce such evidence around individuals and families, as well as increasingly complex and longer-term changes at the community level and system level. On the other hand, Local Area Coordination has a civic mission focused on place, partnership and voice.
These broad missions – of well-being and civic participation – are competing logics seen as socially constructed and enduring assumptions and practices (Besharov & Smith, 2014), with distinct implications for resourcing, organising, delivering and measuring success within Local Authority settings. Both logics have enduring appeal and their own distinct strengths, and Local Area Coordination portrays these as individual, community and system benefits, embracing a commitment to evidence-based outcomes and value-driven processes. Capturing emerging individual outcomes – health and well-being – is encouraged not least by initiatives funded through health and social care resources.
Conversely, the civic mission (values, control and coproduction) of Local Area Coordination cannot be ‘cashed’ – literally or metaphorically – in terms of measurable health outcomes. Any new settlement for civic engagement, participation, localism and place-based developments does not easily calibrate with individual and community-level outcomes. Such tensions are played-out in the advocacy, resourcing and delivery of Local Area Coordination. For example, a major commitment of Local Area Coordination is for those people, who are on the margins in neighbourhoods and communities, to be better included and engaged. Such commitments advance tactically under the groundcover of health and well-being outcomes without measures encapsulating such values. This tension of health/well-being outcomes and the civic/participatory mission is fully evident within the development of cost-effectiveness and SROI studies. Our experience and understanding from published evaluations being that SROI is more often located in cost savings for sectors such as the NHS and Adult Social Care. We recognise that modelling SROI in community approaches is in its infancy and given the longitudinal nature of change through such initiatives it is not without its challenges, least of all in deciding where the savings are cashable in the system or may be shunted onto other sectors within the system.
These competing logics are irreducible to one side or the other; both are constituents of Local Area Coordination appeal and support. Should robust research designs, extensive data collection and longer timelines produce unfavourable empirical results, such evidence would not displace the civic appeal of Local Area Coordination. These logics are a more enduring tension – a tension to be managed and that has implications for organisational and institutional settings concerning how Local Area Coordination is sustained (Besharov & Smith, 2014). They include how Local Authority political and policy leadership shape competing logics within settings. Day-to-day processes, including the hiring and socialisation of professionals and their expectations, and the ties amongst members in network organisation, all contribute to how tensions are manifest and managed. These logics change over time and place as ‘nested and intertwined factors at multiple levels of analysis’ (Besharov & Smith, 2014, p. 376), and are differentially experienced on the ground (urban and rural; change over time; and at varying organisational levels in a Local Authority).
Limitations of study
The article is a review of published evaluation studies, SROI and cost analyses of Local Area Coordination. It examines the implementation of Local Area Coordination across England and Wales, drawing upon the full range of available studies. The authors draw upon the published findings of their own empirical studies of Local Area Coordination (Gamsu & Rippon, 2018; Lunt & Bainbridge, 2019; Lunt et al., 2018) and other completed studies.
Conclusion
Our review of Local Area Coordination identifies recurring messages: both that ‘early evaluation of some programmes has found positive outcomes’, and there is fidelity to process and commitment to citizenship. The emerging evidence around individual and family-level outcomes are laudable achievements and will go some way to Local Area Coordination gaining stakeholder acceptance, including amongst commissioners and funders. In the evidence presented around the first logic, the focus is on individuals and families, rather than communities or broader system transformation. In aspiring to wider system change and greater prevention focus, caution must be taken in reading Local Area Coordination as any ‘new script for social care’ (Daly & Westwood, 2018). There is as yet more limited community-level evidence, including how activities help build social capital. A greater emphasis on capacity building and the consolidation of partnerships and relationship with other services, communities and third sector organisations will take time to emerge and capture. The second logic, coalescing around place, partnership and voice, is much less amenable to measurement and evaluation design. Successful implementation is skilfully managing these competing logics of Local Area Coordination, and resisting subverting one to the other, either through side-lining or hard-wiring an evidence-based paradigm or elevating outcomes over process.
Evaluation and SROI reports
Kingfishers Ltd. (2016). Social value of Local Area Coordination in Derby: A forecast social return on investment. Analysis for Derby City Council Summary Report.
Gamsu, M., & Rippon, S. (2019). “Making Haringey a better place . . . where everyone can thrive” Haringey Local Area Coordination Programme – A formative evaluation of implementation. Leeds Beckett University.
Darnton, P., Sladen, J., Liles, A., Sibley, A., Anstee, S., Brooks, C., & Benson, T. (2018). Independent Evaluation of Local Area Coordination on the Isle of Wight. Wessex AHSN. Oatley, C. (2016). Local Area Coordination: Formative evaluation: Understanding the praxis and impact of the Local Area Coordination approach on the Isle of Wight.
M E L Research. (2016). Evaluation of Leicestershire Local Area Coordination.
Peter Fletcher Associates. (2011). Evaluation of Local Area Coordination in Middlesbrough.
Reinhardt, G.Y., & Chatsiou, K. (2018). Evaluation: Local Area Coordination in Suffolk Programme. Suffolk County Council/University of Essex.
Kingfishers Ltd. (2015). The Social Value of Local Area Coordination in Thurrock. A forecast Social Return on Investment Analysis for Adult Social Care. Thurrock Council, Summary Report. Sitch, T. (2013). Local Area Coordination. First four months evaluation report. Thurrock Council. Sitch, T., & Biddle, J. (2014). Local Area Coordination: Fourteen month evaluation report. Thurrock Council.
Gamsu, M., & Rippon, S. (2018). Local Area Co-ordination in Waltham Forest. A formative evaluation. Leeds Beckett University.
Roderick, S., Davies, G., Daniels, J., & Gregory, J. (2015). Formative evaluation report 2015. Local Area Coordination in the Western Bay Area: Initiation review. Pilot Site Study: Swansea. Swansea University. Swansea University. (2016). Local community initiatives in Western Bay. Formative Evaluation Summary Report, Swansea University.
Lunt, N., & Bainbridge, L. (2019). Local Area Coordination: Summative evaluation. University of York. Lunt, N., Bainbridge, L., & Tibocha Nino, A. (2018). Local Area Coordination: Process evaluation. University of York.
Footnotes
Acknowledgements
Simon Rippon is also affiliated with Leeds Beckett University, Leeds, UK.
Ethics
None applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of York Economic and Social Research Council Impact Acceleration Account, Co-Production Call.
Acknowledgements
Thanks to Journal of Social Work anonymous reviewers for their very helpful and supportive comments on an earlier draft of this article. An earlier version of this article was presented to the Local Area Coordination research network seminar, York, October 2018. We thank all participants for their valuble feedback.